
Maternal Handwashing with Soap Practices and Associated Risk Factors in Nepal: A Systematic Review

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Criteria Selection
2.2. Data Extraction, Analysis and Quality Assessment
3. Results
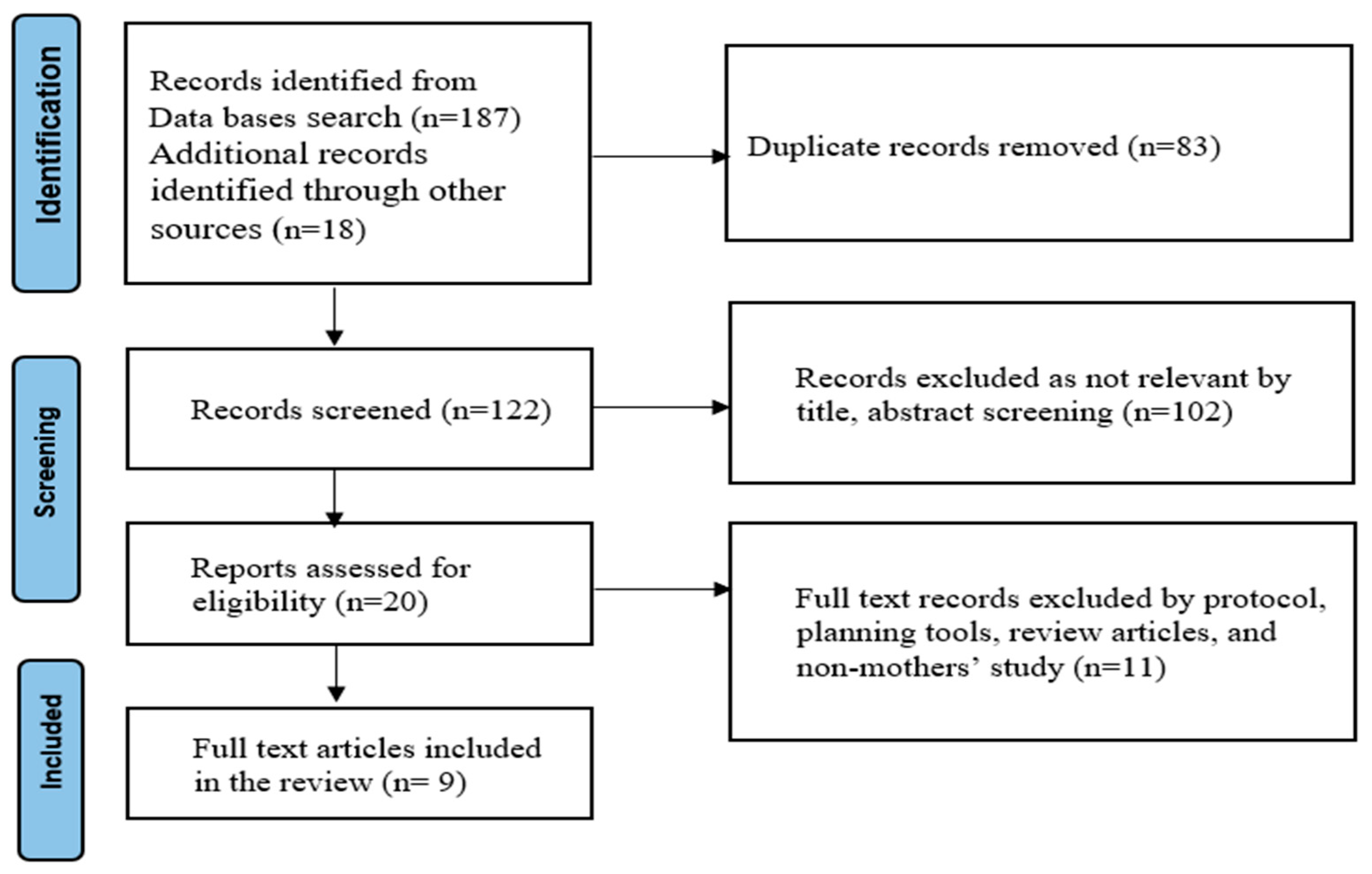
3.1. Study Flow and Characteristics of Included Studies
3.2. Rates of Household Handwashing with Soap by Mothers in Nepal
3.3. Factors Associated with Maternal Handwashing in Nepal
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Curtis, V.; Cairncross, S. Effect of washing hands with soap on diarrhoea risk in the community: A systematic review. Lancet Infect. Dis. 2003, 3, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Curtis, V.A.; Danquah, L.O.; Aunger, R.V. Planned, motivated and habitual hygiene behaviour: An eleven-country review. Health Educ. Res. 2009, 24, 655–673. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Loughnan, L.; Luyendijk, R.; Hernandez, O.; Weinger, M.; Arnold, F.; Ram, P.K. Handwashing in 51 countries: Analysis of proxy measures of handwashing behavior in multiple indicator cluster surveys and demographic and health surveys, 2010–2013. Am. J. Trop. Med. Hyg. 2017, 97, 447. [Google Scholar] [CrossRef] [PubMed]
- Aiello, A.E.; Coulborn, R.M.; Perez, V.; Larson, E.L. Effect of hand hygiene on infectious disease risk in the community setting: A meta-analysis. Am. J. Public Health 2008, 98, 1372–1381. [Google Scholar] [CrossRef] [PubMed]
- Luby, S.P.; Agboatwalla, M.; Feikin, D.R.; Painter, J.; Billhimer, W.; Altaf, A.; Hoekstra, R.M. Effect of handwashing on child health: A randomised controlled trial. Lancet 2005, 366, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Ross, I.; Bick, S.; Ayieko, P.; Dreibelbis, R.; Wolf, J.; Freeman, M.C.; Allen, E.; Brauer, M.; Cumming, O. Effectiveness of handwashing with soap for preventing acute respiratory infections in low-income and middle-income countries: A systematic review and meta-analysis. Lancet 2023, 401, 1681–1690. [Google Scholar] [CrossRef]
- Brauer, M.; Zhao, J.T.; Bennitt, F.B.; Stanaway, J.D. Global access to handwashing: Implications for COVID-19 control in low-income countries. Environ. Health Perspect. 2020, 128, 057005. [Google Scholar] [CrossRef]
- Hannah, D.M.; Lynch, I.; Mao, F.; Miller, J.D.; Young, S.L.; Krause, S. Water and sanitation for all in a pandemic. Nat. Sustain. 2020, 3, 773–775. [Google Scholar] [CrossRef]
- Amegah, A.K. Improving handwashing habits and household air quality in Africa after COVID-19. Lancet Glob. Health 2020, 8, e1110–e1111. [Google Scholar] [CrossRef]
- Beale, S.; Johnson, A.M.; Zambon, M.; Flu Watch Group; Hayward, A.C.; Fragaszy, E.B. Hand hygiene practices and the risk of human coronavirus infections in a UK community cohort. Wellcome Open Res. 2021, 5, 98. [Google Scholar] [CrossRef]
- Horga, N.G.; Cirnatu, D.; Kundnani, N.R.; Ciurariu, E.; Parvu, S.; Ignea, A.L.; Borza, C.; Sharma, A.; Morariu, S. Evaluation of non-pharmacological measures implemented in the management of the COVID-19 pandemic in Romania. Healthcare 2022, 10, 1756. [Google Scholar] [CrossRef] [PubMed]
- Biran, A.; Rabie, T.; Schmidt, W.; Juvekar, S.; Hirve, S.; Curtis, V. Comparing the performance of indicators of hand-washing practices in rural Indian households. Trop. Med. Int. Health 2008, 13, 278–285. [Google Scholar] [CrossRef] [PubMed]
- National Planning Commission. Sustainable Development Goals, Status and Roadmap 2016–2030; Government of Nepal, National Planning Commission: Kathmandu, Nepal, 2015.
- Hutton, G.; Chase, C. The knowledge base for achieving the sustainable development goal targets on water supply, sanitation and hygiene. Int. J. Environ. Res. Public Health 2016, 13, 536. [Google Scholar] [CrossRef] [PubMed]
- Aunger, R.; Schmidt, W.P.; Ranpura, A.; Coombes, Y.; Maina, P.M.; Matiko, C.N.; Curtis, V. Three kinds of psychological determinants for hand-washing behaviour in Kenya. Soc. Sci. Med. 2010, 70, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, W.P.; Aunger, R.; Coombes, Y.; Maina, P.M.; Matiko, C.N.; Biran, A.; Curtis, V. Determinants of handwashing practices in Kenya: The role of media exposure, poverty and infrastructure. Trop. Med. Int. Health 2009, 14, 1534–1541. [Google Scholar] [CrossRef] [PubMed]
- Seward, N.; Prost, A.; Copas, A.; Corbin, M.; Li, L.; Colbourn, T.; Osrin, D.; Neuman, M.; Azad, K.; Kuddus, A.; et al. Using observational data to estimate the effect of hand washing and clean delivery kit use by birth attendants on maternal deaths after home deliveries in rural Bangladesh, India and Nepal. PLoS ONE 2015, 10, e0136152. [Google Scholar] [CrossRef]
- Langford, R.; Lunn, P.; Brick, C.P. Hand-washing, subclinical infections, and growth: A longitudinal evaluation of an intervention in Nepali slums. Am. J. Hum. Biol. 2011, 23, 621–629. [Google Scholar] [CrossRef]
- Rabbi, S.E.; Dey, N.C. Exploring the gap between hand washing knowledge and practices in Bangladesh: A cross-sectional comparative study. BMC Public Health 2013, 13, 1–7. [Google Scholar] [CrossRef]
- Zhang, C.; Mosa, A.J.; Hayward, A.S.; Matthews, S.A. Promoting clean hands among children in Uganda: A school-based intervention using ‘tippy-taps’. Public Health 2013, 127, 586. [Google Scholar] [CrossRef]
- Gammon, J.; Hunt, J. The neglected element of hand hygiene-significance of hand drying, efficiency of different methods and clinical implication: A review. J. Infect. Prev. 2019, 20, 66–74. [Google Scholar] [CrossRef]
- Budhathoki, C.B. Water supply, sanitation and hygiene situation in Nepal: A review. J. Health Promot. 2019, 7, 65–76. [Google Scholar] [CrossRef]
- White, S.; Thorseth, A.H.; Dreibelbis, R.; Curtis, V. The determinants of handwashing behaviour in domestic settings: An integrative systematic review. Int. J. Hyg. Environ. Health 2020, 227, 113512. [Google Scholar] [CrossRef] [PubMed]
- Luby, S.P.; Agboatwalla, M.; Painter, J.; Altaf, A.; Billhimer, W.L.; Hoekstra, R.M. Effect of intensive handwashing promotion on childhood diarrhea in high-risk communities in Pakistan: A randomized controlled trial. JAMA 2004, 291, 2547–2554. [Google Scholar] [CrossRef] [PubMed]
- Freiburger, M.A. Mothers as Children’s “First and Best Teachers”: An Institutional Ethnography. Ph.D. Dissertation, University of Kansas, Lawrence, KS, USA, 2010. [Google Scholar]
- Lam, W.; Fowler, C.; Dawson, A. The approaches Hong Kong Chinese mothers adopt to teach their preschool children to prevent influenza: A multiple case study at household level. BMC Nurs. 2016, 15, 51. [Google Scholar] [CrossRef] [PubMed]
- Rhee, V.; Mullany, L.C.; Khatry, S.K.; Katz, J.; LeClerq, S.C.; Darmstadt, G.L.; Tielsch, J.M. Maternal and birth attendant hand washing and neonatal mortality in southern Nepal. Arch. Pediatr. Adolesc. Med. 2008, 162, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Mitlin, D. Equity and gender. In Pathfinder Report; Sanitation and Hygiene Applied Research for Equity (SHARE); Water Aid/Macro Betti: India, 2011; Available online: https://www.susana.org/en/community/partners/list/details/1561# (accessed on 30 October 2023).
- Central Bureau of Statistics. Nepal Multiple Indicator Cluster Survey (MICS) 2014, Final Report; National Planning Commission, Central Bureau Statistics (CBS), UNICEF: Kathmandu, Nepal, 2014.
- Gautam, O.P.; Schmidt, W.P.; Cairncross, S.; Cavill, S.; Curtis, V. Trial of a novel intervention to improve multiple food hygiene behaviors in Nepal. Am. J. Trop. Med. Hyg. 2017, 96, 1415. [Google Scholar] [CrossRef]
- McMichael, C.; Robinson, P. Drivers of sustained hygiene behaviour change: A case study from mid-western Nepal. Soc. Sci. Med. 2016, 163, 28–36. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Bull. World Health Organ. 2007, 85, 867–872. [Google Scholar] [CrossRef]
- Dhital, S.R.; Chojenta, C.; Evans, T.J.; Acharya, T.D.; Loxton, D. Prevalence and Correlates of Water, Sanitation, and Hygiene (WASH) and Spatial Distribution of Unimproved WASH in Nepal. Int. J. Environ. Res. Public Health 2022, 19, 3507. [Google Scholar] [CrossRef]
- Sekh, N.; Shekh, R.; Kaphle, K.; Ansari, I.A. Handwashing Habits before Pandemic COVID-19 in the Chitwan District of Nepal and Implication for COVID-19 Control. Open J. Soc. Sci. 2022, 10, 471–478. [Google Scholar] [CrossRef]
- Kafle, S.; Pradhan, B. Situation of water, sanitation and hygiene and diarrhoeal disease after open defecation free declaration and associated factors of Makwanpur District, Nepal. J. Nepal Health Res. Counc. 2018, 16, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Langford, R.; Panter-Brick, C. A health equity critique of social marketing: Where interventions have impact but insufficient reach. Soc. Sci. Med. 2013, 83, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Osrin, D.; Tumbahangphe, K.M.; Shrestha, D.; Mesko, N.; Shrestha, B.P.; Manandhar, M.K.; Standing, H.; Manandhar, D.S.; Anthony, M.D. Cross sectional, community-based study of care of newborn infants in Nepal. BMJ 2002, 325, 1063. [Google Scholar] [CrossRef] [PubMed]
- Kandel, P.; Kunwar, R.; Lamichhane, P.; Karki, S. Extent of fecal contamination of household drinking water in Nepal: Further analysis of Nepal Multiple Indicator Cluster Survey 2014. Am. J. Trop. Med. Hyg. 2017, 96, 446. [Google Scholar] [CrossRef]
- Miller, L.C.; Joshi, N.; Lohani, M.; Rogers, B.; Mahato, S.; Ghosh, S.; Webb, P. Women’s education level amplifies the effects of a livelihoods-based intervention on household wealth, child diet, and child growth in rural Nepal. Int. J. Equity Health 2017, 16, 183. [Google Scholar] [CrossRef] [PubMed]
- Aihara, Y.; Shrestha, S.; Sharma, J. Household water insecurity, depression and quality of life among postnatal women living in urban Nepal. J. Water Health 2016, 14, 317–324. [Google Scholar] [CrossRef]
- McCarthy Ribbens, J.; Edwards, R. Key Concepts in Family Studies; Sage: London, UK, 2011. [Google Scholar]
- Ministry of Health and Population. Nepal Demographic and Health Survey; MOHP, New Era and Inner City Fund International: Kathmandu, Nepal, 2016.
- Ministry of Health and Population. Nepal Demographic and Health Survey; MOHP, New Era and Inner City Fund International: Kathmandu, Nepal, 2022.
- Suen, L.K.; Rana, T. Knowledge level and hand hygiene practice of Nepalese immigrants and their host country population: A comparative study. Int. J. Environ. Res. Public Health 2020, 17, 4019. [Google Scholar] [CrossRef]
- Rajbhandari, A.K.; Sagtani, R.A.; Baral, K.P. Hand hygiene compliance among rural healthcare workers of Nepal. J. Patan Acad. Health Sci. 2018, 5, 90–95. [Google Scholar] [CrossRef]
- Song, I.H.; Kim, S.A.; Park, W.S. Family factors associated with children’s handwashing hygiene behavior. J. Child Health Care 2013, 17, 164–173. [Google Scholar] [CrossRef]
- Nguyen, N.K.; Gurung, H. Barriers and Facilitators to Hygienic Use and Maintenance of Latrines and Handwashing with Soap in Sarlahi, Mahottari, Siraha and Saptari Districts of the Terai, Nepal; Formative Research WASH Nepal, Netherland: SNV Smart Development Work; 2015; pp. 1–50. Available online: https://sanitationlearninghub.org/resource/barriers-and-facilitators-to-hygienic-use-and-maintenance-of-latrines-and-handwashing-with-soap-in-sarlahi-mahottari-siraha-and-saptari-districts-of-the-terai-nepal/ (accessed on 30 October 2023).
- Ghimire, M.; Pradhan, Y.V.; Maskey, M.K. Community-based interventions for diarrhoeal diseases and acute respiratory infections in Nepal. Bull. World Health Organ. 2010, 88, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Green, L.W. Health Program Planning: An Educational and Ecological Approach, 4th ed.; McGraw Hill: New York, NY, USA, 2005. [Google Scholar]
- Koirala Dhital, M.; Dhital, S.R.; Kc, B.B.; Owens, V.; Khadka, H.R.; Gyawali, P. Successful health promotion, its challenges and the way forward in Nepal. Glob. Health Promot. 2023, 30, 68–71. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| First Author, Year | Study Design | Sample Size | Study Periods | Main Findings |
|---|---|---|---|---|
| Dhital, S.R., 2023 [34] | Cross sectional | 11,040 | 1 year | The availability of soap and water was 47%. |
| Sekh, N., 2022 [35] | Cross sectional | 40 | 1 month | Mean handwashing with soap rate by household mothers was 28% and 34%, respectively in Shakti Khor and Tandi Municipality of Chitwan Nepal. The handwashing rate was higher after defecation than before taking meals. |
| Kafle, S., 2018 [36] | Cross-sectional | 178 | Not specified | Mothers washed their hands with soap by 43% during the critical moments. |
| Gautam, O.P., 2017 [30] | RCT | 239 | 3 months | Handwashing at home before feeding the child and eating increased from 5% to 67% after the health promotion food hygiene campaign. |
| Langford, R., 2013 [37] | RCT | 88 | 6 months | Approximately 21% of mothers washed their hands with soap after defaecation and 14% after cleaning baby’s bottom. No data were obtained about handwashing during/before cooking or feeding the child in non-intervention group. Intervention groups (baseline and post-intervention) showed that mothers washed their hands after defaecation (96% and 100%), after cleaning baby’s bottom (82% and 100%), before cooking (12% and 71%), before feeding children (26% and 62%) and before eating (14% and 60%), respectively. |
| Rhee, V., 2008 [27] | Cohort study | 23,662 | 40 months | Prevalence of maternal handwashing with soap before handling their infants was 15%. |
| Osrin, D., 2002 [38] | Cross-sectional | 5411 | Not specified | Approximately 50% of mothers who attended a birth had washed their hands with soap. |
| First Author, Year | Study Design | Sample Size | Study Periods | Main Findings |
|---|---|---|---|---|
| Dhital, S.R., 2023 [34] | Cross sectional | 11,040 | 1 year | The handwashing with soap is influenced by education, wealth and ecology. |
| Kafle, S., 2018 [36] | Cross-sectional | 178 | Not specified | Access to an improved water source, sanitary toilets, and the availability of soap for handwashing are key determinants of handwashing indicators. |
| Kandel, P., 2017 [39] | Cross sectional | 1421 | Not specified | Availability of soap, water and a fixed place for handwashing was significantly associated with lower rates of faecal contamination in water sources. |
| Gautam, O.P., 2017 [30] | RCT | 239 | 3 months | A comprehensive health promotion intervention involving mothers’ participation and motivation factors has facilitated handwashing. |
| Miller, L.C., 2017 [40] | RCT | 1011 | 48 months | Mothers used soap and had more water access at home than fathers, and the participatory Community Development program effectively improved household hygiene. |
| Langford, R., 2013 [37] | RCT | 88 | 6 months | Culture and belief determine to have a handwashing with soap by mothers at households. |
| Rhee, V., 2008 [27] | Cohort study | 23,662 | 40 months | Maternal handwashing with soap was associated with significantly lower rates of neonatal mortality. |
| Osrin, D., 2002 [38] | Cross-sectional | 5411 | Not specified | The level of knowledge is the most influential factor affecting handwashing with soap among household mothers. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dhital, S.R.; Chojenta, C.; Bagade, T.; Loxton, D. Maternal Handwashing with Soap Practices and Associated Risk Factors in Nepal: A Systematic Review. Hygiene 2024, 4, 14-22. https://doi.org/10.3390/hygiene4010002
Dhital SR, Chojenta C, Bagade T, Loxton D. Maternal Handwashing with Soap Practices and Associated Risk Factors in Nepal: A Systematic Review. Hygiene. 2024; 4(1):14-22. https://doi.org/10.3390/hygiene4010002
Chicago/Turabian StyleDhital, Shalik Ram, Catherine Chojenta, Tanmay Bagade, and Deborah Loxton. 2024. "Maternal Handwashing with Soap Practices and Associated Risk Factors in Nepal: A Systematic Review" Hygiene 4, no. 1: 14-22. https://doi.org/10.3390/hygiene4010002