
A Cross-Over Randomized Controlled Clinical Trial for Evaluation of Two Hygiene Protocols on Microbial Load, Tissue Health, and Opinion of Ocular Prosthesis Wearers
 , , , and
, , , and
Abstract
:1. Introduction
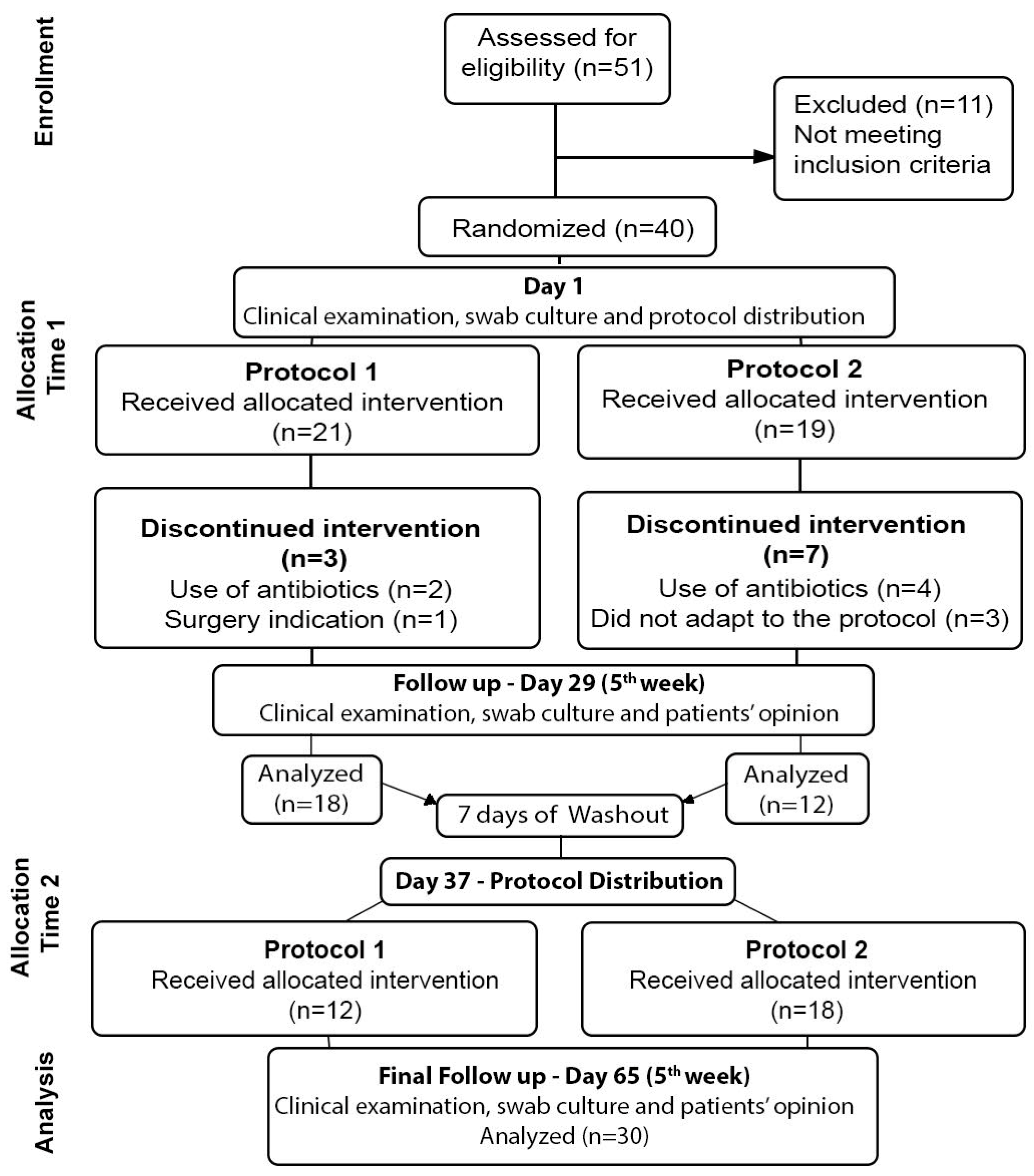
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amornvit, P.; Rokaya, D.; Shrestha, B.; Srithavaj, T. Prosthetic rehabilitation of an ocular defect with post-enucleation socket syndrome: A case report. Saudi Dent. J. 2014, 26, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Pine, K.R.; Sloan, B.H.; Jacobs, R.J. A proposed model of the response of the anophthalmic socket to prosthetic eye wear and its application to the management of mucoid discharge. Med. Hypotheses 2013, 81, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Pine, K.; Sloan, B.; Stewart, J.; Jacobs, R. The response of the anophthalmic socket to prosthetic eye wear. Clin. Exp. Optom. 2013, 96, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Bohman, E.; Roed Rassmusen, M.L.; Kopp, E.D. Pain and discomfort in the anophthalmic socket. Curr. Opin. Ophthalmol. 2014, 25, 455–460. [Google Scholar] [CrossRef]
- Rokohl, A.C.; Trester, M.; Guo, Y.; Kopecky, A.; Lin, M.; Kratky, V.; Heindl, L.M. Socket discomfort in anophthalmic patients—Reasons and therapy options. Ann. Eye Sci. 2020, 5, 36–42. [Google Scholar] [CrossRef]
- Raizada, K.; Rani, D. Ocular prosthesis. Contact Lens Anterior Eye 2007, 30, 152–162. [Google Scholar] [CrossRef]
- Patel, V.; Allen, D.; Morley, A.; Frcophth, R. Features and management of an acute allergic response to acrylic ocular prostheses. Orbit 2009, 28, 339–341. [Google Scholar] [CrossRef]
- Litwin, A.S.; Worrell, E.; Roos, J.C.P.; Edwards, B.; Malhotra, R. Can we improve the tolerance of an ocular prosthesis by enhancing its surface finish? Ophthalmic Plast. Reconstr. Surg. 2018, 34, 130–135. [Google Scholar] [CrossRef]
- Baino, F.; Perero, S.; Ferraris, S.; Miola, M.; Balagna, C.; Verné, E.; Vitale-Brovarone, C.; Coggiola, A.; Dolcino, D.; Ferraris, M. Biomaterials for orbital implants and ocular prostheses: Overview and future prospects. Acta Biomater. 2014, 10, 1064–1087. [Google Scholar] [CrossRef]
- Srinivasan, B.; Jakobiec, F.; Iwamoto, T.; DeVoe, A. Giant papillary conjunctivitis with ocular prostheses. Arch. Ophthalmol. 1979, 97, 892–895. [Google Scholar] [CrossRef]
- Kashkouli, M.B.; Zolfaghari, R.; Es’haghi, A.; Amirsardari, A.; Abtahi, M.B.; Karimi, N.; Alemzadeh, A.; Aghamirsalim, M. Tear film lacrimal drainage system, and eyelid findings in subjects with anophthalmic socket discharge. Am. J. Ophthalmol. 2016, 165, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Pine, N.S.; de Terte, I.; Pine, K.R. An investigation into discharge, visual perception, and appearance concerns of prosthetic eye wearers. Orbit 2017, 36, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Rokohl, A.; Trester, M.; Naderi, P.; Loreck, N.; Zwingelberg, S.; Bucher, F.; Pine, K.R.; Heindl, L.M. Dry anophthalmic socket syndrome—Morphological alterations in meibomian glands. Eye 2021, 35, 3358–3366. [Google Scholar] [CrossRef]
- Shapira, Y.; Worrell, E.; Ullrich, K.; Litwin, A.; Malhotra, R. UK National Artificial Eye Questionnaire study: Comparisons between cosmetic shell and artificial eye users. Part 1: Demographics, comfort and satisfaction. Br. J. Ophthalmol. 2021, 105, 1346–1351. [Google Scholar] [CrossRef] [PubMed]
- Volpe, G.; De Piano, M.; Mazzone, G.; Micera, A.; Bonini, S.; Modugno, A.C. Should we care about the ocular surface in the anophthalmic patient? Eur. J. Ophthalmol. 2022, 32, 1924–1933. [Google Scholar] [CrossRef]
- Pine, K.; Sloan, B.; Jacobs, R.J. Deposit buildup on prosthetic eyes and implications for conjunctival inflammation and mucoid discharge. Clin. Ophthalmol. 2012, 6, 1755–1762. [Google Scholar] [CrossRef]
- Pine, K.R.; Sloan, B.; Han, K.Y.; Swift, S.; Jacobs, R.J. Deposit buildup on prosthetic eye material (in vitro) and its effect on surface wettability. Clin. Ophthalmol. 2013, 7, 313–319. [Google Scholar] [CrossRef]
- Parr, G.R.; Goldman, B.M.; Rahn, A.O. Post insertion care of the ocular prosthesis. J. Prosthet. Dent. 1983, 49, 220–224. [Google Scholar] [CrossRef]
- McMonnies, C.W. Hand hygiene prior to contact lens handling is problematical. Contact Lens Anterior Eye 2012, 35, 65–70. [Google Scholar] [CrossRef]
- Rokohl, A.C.; Adler, W.; Koch, K.R.; Mor, J.M.; Jia, R.; Trester, M.; Pine, N.S.; Pine, K.R.; Heindl, L.M. Cryolite glass prosthetic eyes-the response of the anophthalmic socket. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 2015–2023. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, M.J.; Choung, H.K.; Kim, N.J.; Hwang, S.W.; Sung, M.S.; Khwarg, S.I. Conjunctival cytologic features in anophthalmic patients wearing an ocular prosthesis. Ophthalmic Plast. Reconstr. Surg. 2008, 24, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Osborn, K.L.; Hetller, D. A survey of recommendations on the care of ocular prostheses. Optometry 2010, 81, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Bonaque-González, S.; Amigó, A.; Rodríguez-Luna, C. Recommendations for post-adaption care of an ocular prosthesis: A review. Contact Lens Anterior Eye 2015, 38, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Mourits, D.; Hartong, D.; Buddin, A.E.; Bosscha, M.I.; Tan, H.S.; Moll, A.C. Discharge and infection in retinoblastoma post-enucleation sockets. Clin. Ophthalmol. 2017, 11, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Hatamleh, M.; Abbariki, M.; Alqudah, N.; Cook, A. Survey of ocular prosthetics rehabilitation in the United Kingdom, part 1: Anophthalmic patients’ aetiology, opinions, and attitudes. J. Craniofac. Surg. 2017, 28, 1293–1296. [Google Scholar] [CrossRef]
- Paranhos, R.M.Z.F.; Batalhão, C.H.; Semprini, M.; Regalo, S.C.H.; Ito, I.Y.; Mattos, M.G.C. Evaluation of ocular prosthesis biofilm and anophthalmic cavity contamination after use of three cleansing solutions. J. Appl. Oral Sci. 2007, 15, 33–38. [Google Scholar] [CrossRef]
- Behlau, I.; Gilmore, M.S. Microbial biofilms in ophthalmology and infectious disease. Arch. Ophthalmol. 2008, 126, 1572–1581. [Google Scholar] [CrossRef]
- Penitente, P.A.; Da Silva, E.V.F.; Goiato, M.C.; Maniçoba, L.L.P.; Brito, V.G.B.; Túrcio, K.H.L.; Rodrigues, A.S.; Nagay, B.E.; Dos Santos, D.M. The Inflammation Level and a Microbiological Analysis of the Anophthalmic Cavities of Unilateral Ocular Prosthesis Users: A Blind, Randomized Observational Study. Antibiotics 2022, 11, 1486. [Google Scholar] [CrossRef]
- Toribio, A.; Marrodán, T.; Fernández-Natal, I.; Martínez-Blanco, H.; Rodríguez-Aparicio, L.; Ferrero, M.A. Study of conjunctival flora in anophthalmic patients: Influence on the comfort of the socket. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 1669–1679. [Google Scholar] [CrossRef]
- Guiotti, A.M.; Da Silva, E.V.F.; Catanoze, I.; De Carvalho, K.; Malavazi, E.M.; Goiato, M.C.; Dos Santos, D.M.; De Almeida, M.T. Microbiological analysis of conjunctival secretion in anophthalmic cavity, contralateral eye and ocular prosthesis of patients with maxillofacial abnormalities. Lett. Appl. Microbiol. 2018, 66, 104–109. [Google Scholar] [CrossRef]
- Vasquez, R.J.; Linberg, J.V. The anophthalmic socket and the prosthetic eye. A clinical and bacteriologic study. Ophthalmic Plast. Reconstr. Surg. 1989, 5, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.T.; Pirbhai, A.; Franzco, D.S. Bacterial biofilms associated with ocular prostheses. Clin. Exp. Ophthalmol. 2015, 43, 602–603. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, J.; Vomero, M.; do Nascimento, C.; Watanabe, E.; Paranhos, H.F.O.; Coto, N.P.; Dias, R.B.; Oliveira, V.C.D.; Silva-Lovato, C.H. Genomic identification of microbial species adhering to maxillofacial prostheses and susceptibility to different hygiene protocols. Biofouling 2018, 34, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Byrd, A.L.; Belkaid, Y.; Segre, J.A. The human skin microbiome. Nat. Rev. Microbiol. 2018, 16, 143–155. [Google Scholar] [CrossRef]
- Sullivan, K.M.; Dean, A.; Soe, M.M. OpenEpi: A web-based epidemiologic and statistical calculator for public health. Public Health Rep. 2009, 124, 471–474. [Google Scholar] [CrossRef]
- Pine, K.; Sloan, B.; Jacobs, R. The development of measurement tools for prosthetic eye research. Clin. Exp. Optom. 2013, 96, 32–38. [Google Scholar] [CrossRef]
- Agência Nacional de Vigilância do Brasil. Farmacopeia Brasileira, 5th ed.; Fiocruz: Rio de Janeiro, Brazil, 2010; Volume 1, pp. 273–275. [Google Scholar]
- Alkhaldi, S.A.; Allam, K.H.; Radwan, M.A.; Sweeney, L.E.; Alshammeri, S. Estimates of dry eye disease in Saudi Arabia based on a short questionnaire of prevalence, symptoms and risk factors: The Twaiq Mountain Eye Study I. Contact Lens Anterior Eye 2023, 46, 101770. [Google Scholar] [CrossRef]
- Meduri, A.; Frisina, R.; Rechichi, M.; Oliverio, G.W. Prevalence of Meibomian Gland Dysfunction and Its Effect on Quality of Life and Ocular Discomfort in Patients with Prosthetic Eyes. Prosthesis 2020, 2, 91–99. [Google Scholar] [CrossRef]
- Pine, K.R.; Sloan, B.H.; Jacobs, R.J. Socket Complications: Complications of Prosthesis Retention. In Clinical Ocular Prosthetics; Springer International Publishing: Berlin, Germany, 2015; pp. 180–186. [Google Scholar]
- Aryasit, O.; Uthairat, Y.; Singha, P.; Horatanaruang, O. Efficacy of baby shampoo and commercial eyelid cleanser in patients with meibomian gland dysfunction. Medicine 2020, 99, e20155. [Google Scholar] [CrossRef]
- Ko, J.S.; Seo, Y.; Chae, M.K.; Jang, S.Y.; Yoon, J.S. Effect of topical loteprednol etabonate with lid hygiene on tear cytokines and meibomian gland dysfunction in prosthetic eye wearers. Eye 2018, 32, 439–445. [Google Scholar] [CrossRef]
- Moreno, A.; Goiato, M.C.; dos Santos, D.M.; Haddad, M.F.; Pesqueira, A.A.; Bannwart, L.C. Influence of different disinfecting solutions on the color change of artificial irises used in ocular prostheses. Color Res. Appl. 2014, 39, 56. [Google Scholar] [CrossRef]


{kind=link}
| Questions—Choose a Number from 0 to 10 that Best Describes Your Opinion for Each of the Questions Below |
|---|
1. Did you feel comfortable after cleaning the ocular prosthesis?  2. Did you feel the ocular prosthesis and cavity being clean after cleaning?  3. Do you think the product cleaned your ocular prosthesis? 4. Do you think the product smells pleasant?  5. Do you think the product smell interfered with your comfort after cleaning?  6. Do you think a minute for cleaning is an adequate time?  7. Do you think the product was completely eliminated after rinsing it off with running water?  8. Do you think it is good to clean the prosthesis once a day/week?  |
| Gender | Origin | ||||
|---|---|---|---|---|---|
| Male | 14 (46) | Ribeirão Preto | 8 (27) | ||
| Female | 16 (54) | Nearby Cities | 22 (73) | ||
| Age | |||||
| 18–39 | 5 (17) | 50–59 | 6 (20) | ||
| 40–49 | 8 (27) | 60+ | 11 (36) | ||
| Time of loss | Cause of Eye Loss | ||||
| 0 to 10 | 9 (30) | Pathology | 14 (47) | ||
| 11 to 30 | 10 (33) | Trauma | 14 (47) | ||
| 31+ | 11 (37) | Congenital | 2 (6) | ||
| Prosthesis type | Eye drop use | ||||
| Industrialized | 63 (19) | Yes | 9 (30) | ||
| Customized | 37 (11) | None | 21 (70) | ||
| Patient referral | Surgery | ||||
| Hospital | 24 (80) | Enucleation | 16 (53) | ||
| Internet | 3 (10) | Evisceration | 13 (44) | ||
| Directly | 2 (7) | None | 1 (3) | ||
| UHS * | 1 (3) | ||||
| Frequency of prosthesis cleaning (Baseline) | Cleaning agent (Baseline) | ||||
| Non reported | 7 (23) | Neutral soap | 7 (24) | Baby shampoo (BS) | 3 (10) |
| Daily (1 to 5 times a day) | 14 (47) | Common soap (CS) | 6 (20) | BS and saline | 1 (3) |
| Weekly (1 to 2 times a week) | 6 (20) | CS and saline | 2 (6) | Saline only | 2 (6) |
| Monthly (1 to 2 times a month) | 3 (10) | CS and boric acid | 1 (3) | Water only | 8 (27) |
| Microorganisms | Ocular Prosthesis | p | Socket | p | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline | DPt | WPt | Baseline | DPt | WPt | |||
| Total aerobes | 3.84 ± 1.52 | 3.37 ± 1.49 | 3.67 ± 1.29 | 0.119 * | 3.6 ± 1.02 | 3.35 ± 1.10 | 3.5 ± 1.28 | 0.328 * |
| Gram-negatives | 1.24 ± 1.96 | 1.14 ± 1.77 | 1.25 ± 1.64 | 0.677 ** | 1.06 ± 1.42 | .95 ± 1.6 | 1.03 ± 1.56 | 0.511 ** |
| Staphylococcus spp. | 2.73 ± 1.57 | 2.05 ± 1.90 | 2.42 ± 1.43 | 0.132 ** | 2.54 ± 1.50 | 2.34 ± 1.38 | 1.92 ± 1.47 | 0.134 ** |
| Candida spp. | 0.24 ± 0.66 | 0.21 ± 0.65 | 0.07 ± 0.39 | 0.12 ** | 0.27 ± 0.73 | 0.16 ± 0.51 | 0.07 ± 0.39 | 0.130 ** |
| Baseline | DPt | WPt | ||
|---|---|---|---|---|
| Inflammation | Absent | 18 (60) | 24 (80) | 25 (83) |
| Present | 12 (40) | 6 (20) | 5 (17) | |
| p = 0.005 * | a | b | b | |
| Eyelid edema | Absent | 20 (67) | 26 (87) | 25 (83) |
| Present | 10 (33) | 4 (13) | 5 (17) | |
| p = 0.021 | a | b | a, b | |
| Discharge | Absent | 7 (23) | 16 (53) | 19 (63) |
| Present | 17 (57) | 13 (44) | 7 (23) | |
| Abundant | 6 (20) | 1 (3) | 4 (14) | |
| p < 0.001 ** | a | b | b | |
| Crusting | Absent | 22 (73) | 29 (97) | 27 (90) |
| Present | 8 (27) | 1 (3) | 3 (10) | |
| p = 0.020 * | a | b | a,b | |
| Pain | Absent | 25 (83) | 25 (83) | 25 (83) |
| Present | 5 (17) | 5 (17) | 5 (17) | |
| p = 1.000 * | a | a | a | |
| Sociodemograpfic Data | Socket Inflammation | Eyelid Edema | Crusting | Pain | Discharge |
|---|---|---|---|---|---|
| Gender | 1.000 * | 0.709 * | 0.417 * | 1.000 * | 0.544 ** |
| Age | 0.153 ** | 0.340 ** | 0.487 ** | 0.266 ** | 0.398 ** |
| Cause of loss | 0.364 ** | 0.162 ** | 0.470 ** | 0.254 ** | 0.546 ** |
| Time of loss | 0.111 ** | 0.510 ** | 0.341 ** | 0.604 ** | 0.566 ** |
| Type of prostheses | 1.000 * | 0.702 * | 0.417 * | 0.129 * | 0.157 ** |
| Type of surgery | 0.137 * | 0.112 * | 0.076 * | 0.876 * | 0.461 ** |
| Hygiene products | 0.158 ** | 0.420 ** | 0.380 ** | 0.111 ** | 0.301 ** |
| Eyedrops | 0.102 * | 0.030 * | 0.666 * | 0.016 * | 0.582 ** |
| Socket Inflammation | Eyelid Edema | Crusting | Pain | Discharge | ||
|---|---|---|---|---|---|---|
| B | Eyelid edema | <0.001 * | - | |||
| DPt | Eyelid edema | 0.018 * | - | |||
| WPt | Eyelid edema | 0.183 | - | |||
| B | Crusting | 0.003 * | <0.001 * | |||
| DPt | Crusting | 0.2 | 1 | |||
| WPt | Crusting | 1 | 0.064 | |||
| B | Pain | 0.064 | 0.3 | 0.589 | ||
| DPt | Pain | 1 | 0.538 | 1 | ||
| WPt | Pain | 1 | 0.183 | 0.064 | ||
| B | Discharge | 0.158 | 0.382 | 0.118 | 0.159 | |
| DPt | Discharge | 0.843 | 0.133 | 0.508 | 0.876 | |
| WPt | Discharge | 0.467 | 1 | <0.001 * | 0.154 |
| Ocular Prosthesis | Anophthalmic Socket | |||||||
|---|---|---|---|---|---|---|---|---|
| B | DPt | WPt | B | DPt | WPt | |||
| Total aerobes | Inflammation | r | 0.215 | 0.315 | 0.49 | 0.271 | 0.408 | 0.596 |
| p | 0.253 | 0.09 | 0.006 * | 0.147 | 0.025 * | 0.001 * | ||
| Eyelid Edema | r | 0.157 | 0.136 | 0.399 | 0.07 | 0.254 | 0.307 | |
| p | 0.408 | 0.472 | 0.029 * | 0.712 | 0.176 | 0.099 | ||
| Discharge | r | 0.275 | 0.161 | 0.235 | 0.235 | 0.125 | −0.124 | |
| p | 0.142 | 0.396 | 0.211 | 0.211 | 0.51 | 0.512 | ||
| Crusting | r | 0.219 | −0.09 | 0.056 | 0.333 | −0.031 | −0.162 | |
| p | 0.246 | 0.638 | 0.768 | 0.072 | 0.871 | 0.393 | ||
| Pain | r | −0.108 | 0.02 | 0.052 | −0.083 | 0.236 | −0.075 | |
| p | 0.569 | 0.918 | 0.784 | 0.664 | 0.209 | 0.695 | ||
| Gram-negative | Inflammation | r | 0.395 | 0.345 | 0.375 | 0.076 | 0.432 | 0.45 |
| p | 0.031 | 0.062 | 0.041 | 0.689 | 0.017 | 0.013 | ||
| Eyelid Edema | r | 0.276 | 0.225 | 0.242 | −0.14 | 0.301 | 0.453 | |
| p | 0.14 | 0.232 | 0.198 | 0.459 | 0.106 | 0.012 | ||
| Discharge | r | 0.089 | 0.143 | 0.311 | 0.037 | 0.154 | 0.207 | |
| p | 0.639 | 0.452 | 0.095 | 0.848 | 0.416 | 0.272 | ||
| Crusting | r | 0.083 | −0.121 | 0.109 | −0.277 | −0.11 | 0.199 | |
| p | 0.661 | 0.523 | 0.566 | 0.139 | 0.564 | 0.291 | ||
| Pain | r | −0.141 | −0.157 | −0.018 | −0.216 | −0.102 | 0.045 | |
| p | 0.458 | 0.408 | 0.926 | 0.251 | 0.591 | 0.814 | ||
| Staphylococcus spp. | Inflammation | r | 0.402 | 0.438 | 0.403 | 0.361 | 0.282 | 0.571 |
| p | 0.028 | 0.016 | 0.027 | 0.05 | 0.132 | 0.001 | ||
| Eyelid Edema | r | 0.169 | 0.2 | 0.14 | 0.135 | 0.103 | 0.351 | |
| p | 0.371 | 0.29 | 0.461 | 0.476 | 0.589 | 0.057 | ||
| Discharge | r | 0.381 | 0.158 | 0.052 | 0.199 | 0.21 | −0.055 | |
| p | 0.038 | 0.405 | 0.786 | 0.291 | 0.264 | 0.774 | ||
| Crusting | r | 0.285 | 0.045 | −0.24 | 0.348 | −0.005 | 0.013 | |
| p | 0.127 | 0.811 | 0.202 | 0.06 | 0.979 | 0.945 | ||
| Pain | r | −0.02 | 0.062 | 0.069 | 0.185 | 0.239 | −0.065 | |
| p | 0.917 | 0.744 | 0.717 | 0.328 | 0.203 | 0.732 | ||
| Candida spp. | Inflammation | r | 0.002 | 0.643 | 0.415 | 0.283 | 0.656 | 0.415 |
| p | 0.99 | 0.00 | 0.023 | 0.129 | 0.00 | 0.023 | ||
| Eyelid Edema | r | 0.054 | 0.077 | −0.083 | 0.217 | 0.521 | −0.083 | |
| p | 0.776 | 0.688 | 0.663 | 0.25 | 0.003 | 0.663 | ||
| Discharge | r | 0.22 | 0.163 | 0.129 | 0.273 | −0.101 | 0.129 | |
| p | 0.242 | 0.389 | 0.496 | 0.145 | 0.595 | 0.496 | ||
| Crusting | r | 0.113 | −0.06 | −0.062 | 0.287 | −0.061 | −0.062 | |
| p | 0.553 | 0.754 | 0.745 | 0.125 | 0.749 | 0.745 | ||
| Pain | r | −0.164 | 0.173 | 0.415 | −0.166 | 0.141 | 0.415 * | |
| p | 0.388 | 0.361 | 0.023 | 0.382 | 0.458 | 0.023 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makrakis, L.R.; Ribeiro, A.B.; Evelin, L.d.S.; Oliveira, V.d.C.; Macedo, A.P.; Watanabe, E.; Silva-Lovato, C.H. A Cross-Over Randomized Controlled Clinical Trial for Evaluation of Two Hygiene Protocols on Microbial Load, Tissue Health, and Opinion of Ocular Prosthesis Wearers. Hygiene 2023, 3, 428-440. https://doi.org/10.3390/hygiene3040032
Makrakis LR, Ribeiro AB, Evelin LdS, Oliveira VdC, Macedo AP, Watanabe E, Silva-Lovato CH. A Cross-Over Randomized Controlled Clinical Trial for Evaluation of Two Hygiene Protocols on Microbial Load, Tissue Health, and Opinion of Ocular Prosthesis Wearers. Hygiene. 2023; 3(4):428-440. https://doi.org/10.3390/hygiene3040032
Chicago/Turabian StyleMakrakis, Laís Ranieti, Adriana Barbosa Ribeiro, Letícia de Sá Evelin, Viviane de Cássia Oliveira, Ana Paula Macedo, Evandro Watanabe, and Cláudia Helena Silva-Lovato. 2023. "A Cross-Over Randomized Controlled Clinical Trial for Evaluation of Two Hygiene Protocols on Microbial Load, Tissue Health, and Opinion of Ocular Prosthesis Wearers" Hygiene 3, no. 4: 428-440. https://doi.org/10.3390/hygiene3040032