

Treatment with Gaseous Ozone Significantly Reduced the Number of Bacteria in Extended-Spectrum-β-Lactamase (ESBL)-Producing Escherichia coli Biofilm

Abstract
:1. Introduction
2. Materials and Methods
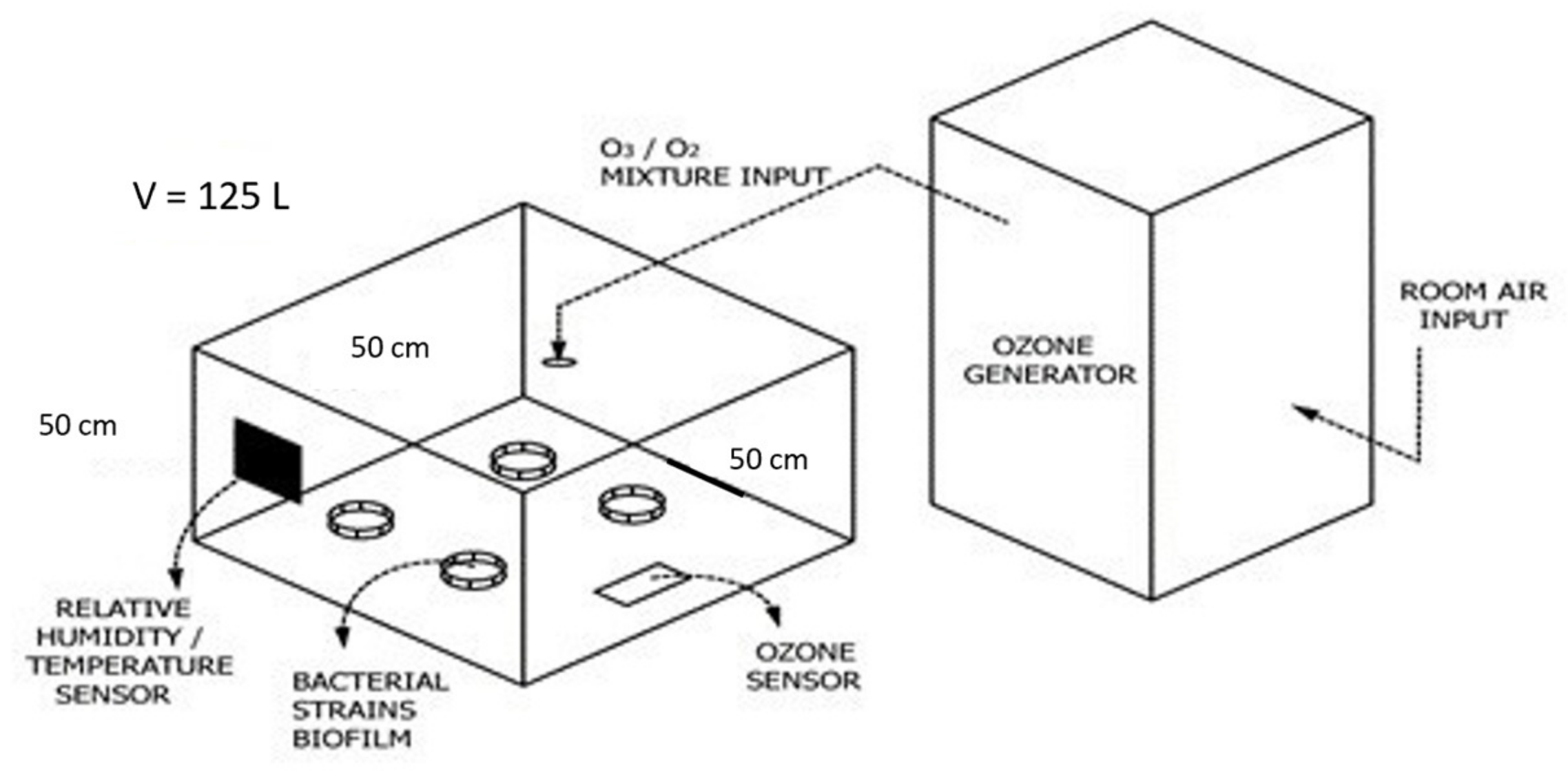
2.1. Test Chamber Characteristics
2.2. Bacterial Strains
2.3. Antibiotic Susceptibility Testing Results for All Used Strains
2.4. Preparation of Ceramic Tiles and Biofilm Formation
2.5. Total Bacteria Number Determination
2.6. Determining RLU Values by ATP Bioluminescence
2.7. Determining Biomass Reduction by Crystal-Violet Staining
2.8. Statistical Analysis and Graphing
3. Results
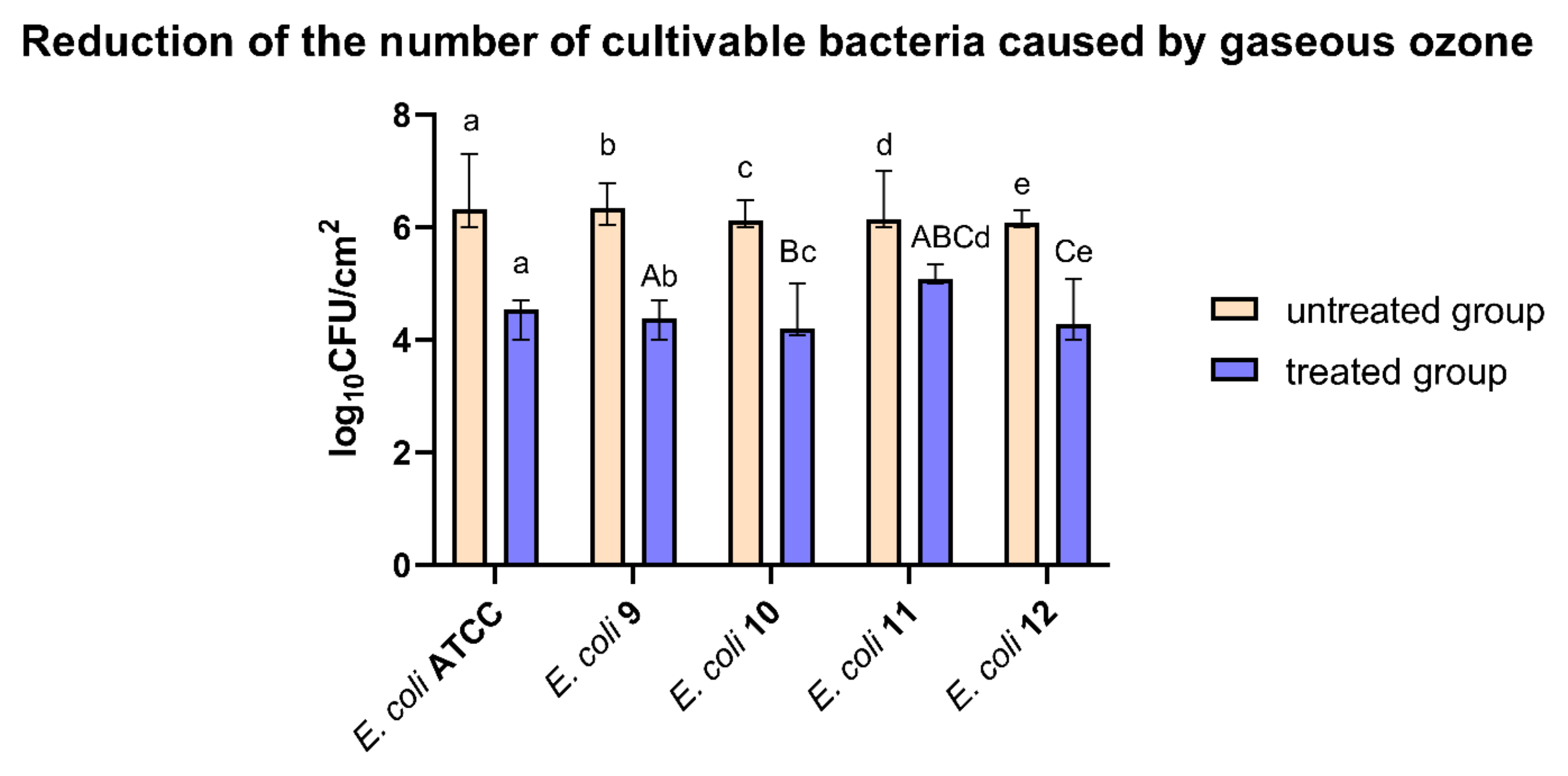
3.1. Reduction of the Number of Cultivable Bacteria Caused by Ozone Treatment
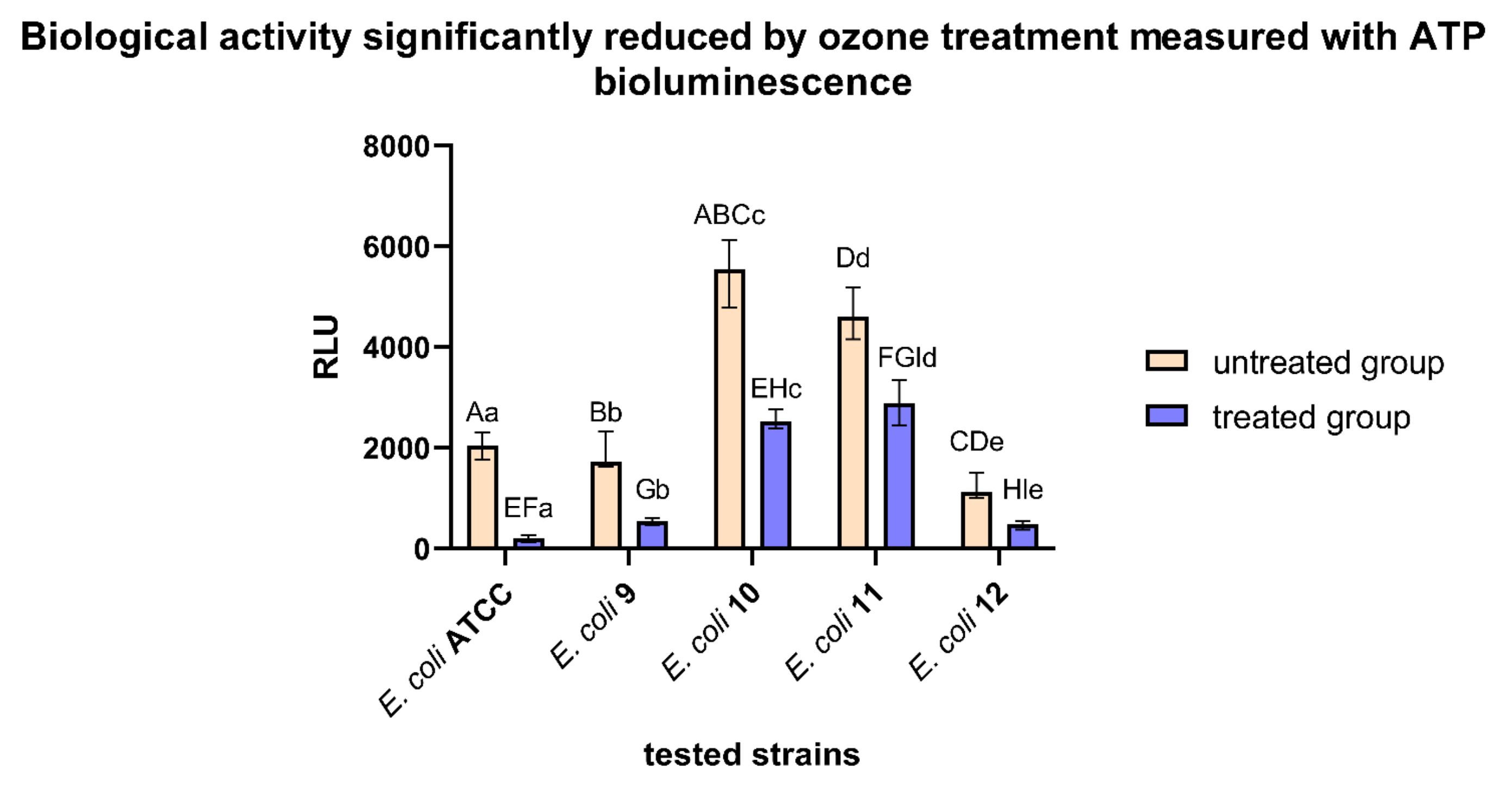
3.2. Biological Activity Significantly Reduced by 1 h Ozone Treatment Measured with ATP Bioluminescence
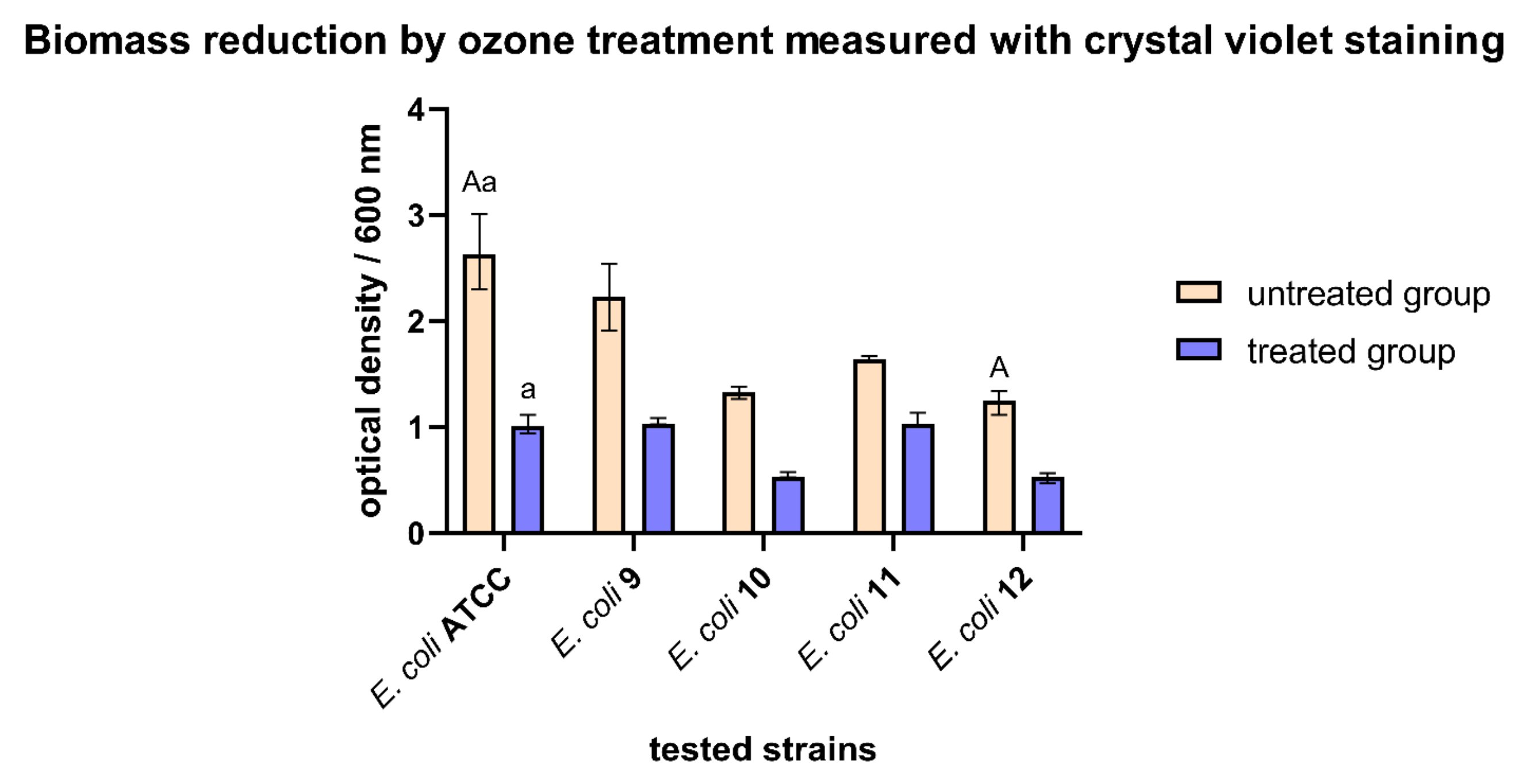
3.3. Biomass Reduction by Ozone Treatment Measured with Crystal Violet Staining
3.4. Biofilm Inhibition Rates Varied Using Different Detection Methods
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CFU/cm2 | colony forming unit per square centimeter |
| CV | crystal violet |
| E. coli | Escherichia coli |
| EPS | extracellular polymer substance |
| ESBL | extended-spectrum-β-lactamase |
| HUS | hemolytic uremic syndrome |
| OD | optical density |
| MHB | Müller Hinton broth |
| PBP | penicillin-binding protein |
| RLU | relative light units |
| VBNC | viable but not cultivable state of bacteria |
References
- Allocati, N.; Masulli, M.; Alexeyev, M.; Di Ilio, C. Escherichia Coli in Europe: An Overview. Int. J. Environ. Res. Public. Health 2013, 10, 6235–6254. [Google Scholar] [CrossRef] [PubMed]
- Martinson, J.N.V.; Walk, S.T. Escherichia Coli Residency in the Gut of Healthy Human Adults. EcoSal Plus 2020, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.H.; Jeong, H.; Kwon, S.-K.; Kim, J.F. Genomics, Biological Features, and Biotechnological Applications of Escherichia Coli B: “Is B for Better?!” In Systems Biology and Biotechnology of Escherichia coli; Lee, S.Y., Ed.; Springer: Dordrecht, The Netherlands, 2009; pp. 1–17. ISBN 978-1-4020-9393-7. [Google Scholar]
- Hadžić, L.; Šeol Martinec, B.; Pintarić, S. Extended spectrum β-lactamase producing Escherichia coli. Hrvat. Vet. Vjesn. 2021, 29, 3. [Google Scholar]
- Andrašević, S.; Vranić-Ladavac, M.; Tambić-Andrašević, A. Antibiotic sensitivity of enterobacteriaceae. Infektološki Glas. 2009, 29, 171–176. [Google Scholar]
- Bezabih, Y.M.; Sabiiti, W.; Alamneh, E.; Bezabih, A.; Peterson, G.M.; Bezabhe, W.M.; Roujeinikova, A. The Global Prevalence and Trend of Human Intestinal Carriage of ESBL-Producing Escherichia Coli in the Community. J. Antimicrob. Chemother. 2021, 76, 22–29. [Google Scholar] [CrossRef]
- von Wulffen, J.; RecogNice-Team; Sawodny, O.; Feuer, R. Transition of an Anaerobic Escherichia Coli Culture to Aerobiosis: Balancing MRNA and Protein Levels in a Demand-Directed Dynamic Flux Balance Analysis. PLoS ONE 2016, 11, e0158711. [Google Scholar] [CrossRef]
- Behzadi, P.; Urbán, E.; Gajdács, M. Association between Biofilm-Production and Antibiotic Resistance in Uropathogenic Escherichia coli (UPEC): An In Vitro Study. Diseases 2020, 8, 17. [Google Scholar] [CrossRef]
- Hooton, T.M.; Bradley, S.F.; Cardenas, D.D.; Colgan, R.; Geerlings, S.E.; Rice, J.C.; Saint, S.; Schaeffer, A.J.; Tambayh, P.A.; Tenke, P.; et al. Diagnosis, Prevention, and Treatment of Catheter-Associated Urinary Tract Infection in Adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 625–663. [Google Scholar] [CrossRef]
- Ciani, O.; Grassi, D.; Tarricone, R. An Economic Perspective on Urinary Tract Infection: The “Costs of Resignation”. Clin. Drug Investig. 2013, 33, 255–261. [Google Scholar] [CrossRef]
- Niveditha, A.; Pandiselvam, R.; Prasath, V.A.; Singh, S.K.; Gul, K.; Kothakota, A. Application of Cold Plasma and Ozone Technology for Decontamination of Escherichia coli in Foods—A Review. Food Control 2021, 130, 108338. [Google Scholar] [CrossRef]
- Garcia, A.; Fox, J.G.; Besser, T.E. Zoonotic Enterohemorrhagic Escherichia coli: A One Health Perspective. ILAR J. 2010, 51, 221–232. [Google Scholar] [CrossRef]
- Bryan, A.; Youngster, I.; McAdam, A.J. Shiga Toxin Producing Escherichia coli. Clin. Lab. Med. 2015, 35, 247–272. [Google Scholar] [CrossRef]
- Doi, Y.; Iovleva, A.; Bonomo, R.A. The Ecology of Extended-Spectrum β-Lactamases (ESBLs) in the Developed World. J. Travel Med. 2017, 24, S44–S51. [Google Scholar] [CrossRef]
- Chong, Y.; Shimoda, S.; Shimono, N. Current Epidemiology, Genetic Evolution and Clinical Impact of Extended-Spectrum β-Lactamase-Producing Escherichia coli and Klebsiella Pneumoniae. Infect. Genet. Evol. 2018, 61, 185–188. [Google Scholar] [CrossRef]
- Shaikh, S.; Fatima, J.; Shakil, S.; Rizvi, S.M.D.; Kamal, M.A. Antibiotic Resistance and Extended Spectrum Beta-Lactamases: Types, Epidemiology and Treatment. Saudi J. Biol. Sci. 2015, 22, 90–101. [Google Scholar] [CrossRef]
- Singh, N. Prevalence of ESBL in Escherichia coli Isolates among ICU Patients in a Tertiary Care Hospital. J. Clin. Diagn. Res. 2016, 10, DC19. [Google Scholar] [CrossRef]
- Pandey, N.; Cascella, M. Beta Lactam Antibiotics. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Sieber, S.A.; Böttcher, T.; Staub, I.; Orth, R. Small Molecules as Versatile Tools for Activity-Based Protein Profiling Experiments. In Comprehensive Natural Products II; Elsevier: Amsterdam, The Netherlands, 2010; pp. 629–674. ISBN 978-0-08-045382-8. [Google Scholar]
- Su, M.; Satola, S.W.; Read, T.D. Genome-Based Prediction of Bacterial Antibiotic Resistance. J. Clin. Microbiol. 2019, 57, e01405-18. [Google Scholar] [CrossRef]
- Ballén, V.; Cepas, V.; Ratia, C.; Gabasa, Y.; Soto, S.M. Clinical Escherichia coli: From Biofilm Formation to New Antibiofilm Strategies. Microorganisms 2022, 10, 1103. [Google Scholar] [CrossRef]
- Sharma, G.; Sharma, S.; Sharma, P.; Chandola, D.; Dang, S.; Gupta, S.; Gabrani, R. Escherichia Coli Biofilm: Development and Therapeutic Strategies. J. Appl. Microbiol. 2016, 121, 309–319. [Google Scholar] [CrossRef]
- Piletić, K.; Kovač, B.; Perčić, M.; Žigon, J.; Broznić, D.; Karleuša, L.; Lučić Blagojević, S.; Oder, M.; Gobin, I. Disinfecting Action of Gaseous Ozone on OXA-48-Producing Klebsiella Pneumoniae Biofilm In Vitro. Int. J. Environ. Res. Public. Health 2022, 19, 6177. [Google Scholar] [CrossRef]
- Vickery, K.; Deva, A.; Jacombs, A.; Allan, J.; Valente, P.; Gosbell, I.B. Presence of Biofilm Containing Viable Multiresistant Organisms despite Terminal Cleaning on Clinical Surfaces in an Intensive Care Unit. J. Hosp. Infect. 2012, 80, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Vickery, K. Special Issue: Microbial Biofilms in Healthcare: Formation, Prevention and Treatment. Materials 2019, 12, 2001. [Google Scholar] [CrossRef]
- Assefa, M.; Amare, A. Biofilm-Associated Multi-Drug Resistance in Hospital-Acquired Infections: A Review. Infect. Drug Resist. 2022, 15, 5061–5068. [Google Scholar] [CrossRef] [PubMed]
- Weinbren, M.; Inkster, T. The Hospital-Built Environment: Biofilm, Biodiversity and Bias. J. Hosp. Infect. 2021, 111, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, M.H.; Idris, A.L.; Fan, X.; Guo, Y.; Yu, Y.; Jin, X.; Qiu, J.; Guan, X.; Huang, T. Beyond Risk: Bacterial Biofilms and Their Regulating Approaches. Front. Microbiol. 2020, 11, 928. [Google Scholar] [CrossRef]
- Li, B.; Chen, H.; Cao, L.; Hu, Y.; Chen, D.; Yin, Y. Escherichia Coli Exopolysaccharides Induced by Ceftriaxone Regulated Human Gut Microbiota in Vitro. Front. Microbiol. 2021, 12, 634204. [Google Scholar] [CrossRef]
- Aponte, M.; Anastasio, A.; Marrone, R.; Mercogliano, R.; Peruzy, M.F.; Murru, N. Impact of Gaseous Ozone Coupled to Passive Refrigeration System to Maximize Shelf-Life and Quality of Four Different Fresh Fish Products. LWT 2018, 93, 412–419. [Google Scholar] [CrossRef]
- Panebianco, F.; Rubiola, S.; Chiesa, F.; Civera, T.; Di Ciccio, P.A. Effect of Gaseous Ozone Treatment on Biofilm of Dairy-Isolated Pseudomonas Spp. Strains. Ital. J. Food Saf. 2022, 11, 10350. [Google Scholar] [CrossRef]
- Epelle, E.I.; Macfarlane, A.; Cusack, M.; Burns, A.; Okolie, J.A.; Mackay, W.; Rateb, M.; Yaseen, M. Ozone Application in Different Industries: A Review of Recent Developments. Chem. Eng. J. 2023, 454, 140188. [Google Scholar] [CrossRef]
- Cai, Y.; Zhao, Y.; Yadav, A.K.; Ji, B.; Kang, P.; Wei, T. Ozone Based Inactivation and Disinfection in the Pandemic Time and beyond: Taking Forward What Has Been Learned and Best Practice. Sci. Total Environ. 2023, 862, 160711. [Google Scholar] [CrossRef]
- Fan, X. Gaseous Ozone to Preserve Quality and Enhance Microbial Safety of Fresh Produce: Recent Developments and Research Needs. Compr. Rev. Food Sci. Food Saf. 2021, 20, 4993–5014. [Google Scholar] [CrossRef]
- Piletić, K.; Kovač, B.; Planinić, M.; Vasiljev, V.; Karačonji, I.B.; Žigon, J.; Gobin, I.; Oder, M. Combined Biocidal Effect of Gaseous Ozone and Citric Acid on Acinetobacter Baumannii Biofilm Formed on Ceramic Tiles and Polystyrene as a Novel Approach for Infection Prevention and Control. Processes 2022, 10, 1788. [Google Scholar] [CrossRef]
- Piletić, K.; Linšak, D.T.; Kovač, B.; Mežnarić, S.; Repustić, M.; Radmanović-Skrbić, M.; Gobin, I. Ozone Disinfection Efficiency against Airborne Microorganisms in Hospital Environment: A Case Study. Arch. Ind. Hyg. Toxicol. 2023, 73, 270–276. [Google Scholar] [CrossRef]
- Kovač, B.; Piletić, K.; Kovačević Ganić, N.; Gobin, I. The Effectiveness of Benzalkonium Chloride as an Active Compound on Selected Foodborne Pathogens Biofilm. Hygiene 2022, 2, 226–235. [Google Scholar] [CrossRef]
- Failor, K.C.; Silver, B.; Yu, W.; Heindl, J.E. Biofilm Disruption and Bactericidal Activity of Aqueous Ozone Coupled with Ultrasonic Dental Scaling. JADA Found. Sci. 2022, 1, 100003. [Google Scholar] [CrossRef]
- Marino, M.; Maifreni, M.; Baggio, A.; Innocente, N. Inactivation of Foodborne Bacteria Biofilms by Aqueous and Gaseous Ozone. Front. Microbiol. 2018, 9, 2024. [Google Scholar] [CrossRef]
- Panebianco, F.; Rubiola, S.; Di Ciccio, P.A. The Use of Ozone as an Eco-Friendly Strategy against Microbial Biofilm in Dairy Manufacturing Plants: A Review. Microorganisms 2022, 10, 162. [Google Scholar] [CrossRef]
- Robben, C.; Witte, A.K.; Schoder, D.; Stessl, B.; Rossmanith, P.; Mester, P. A Fast and Easy ATP-Based Approach Enables MIC Testing for Non-Resuscitating VBNC Pathogens. Front. Microbiol. 2019, 10, 1365. [Google Scholar] [CrossRef]
- Arroyo, M.G.; Ferreira, A.M.; Frota, O.P.; Rigotti, M.A.; de Andrade, D.; Brizzotti, N.S.; Peresi, J.T.M.; Castilho, E.M.; de Almeida, M.T.G. Effectiveness of ATP Bioluminescence Assay for Presumptive Identification of Microorganisms in Hospital Water Sources. BMC Infect. Dis. 2017, 17, 458. [Google Scholar] [CrossRef]
- Sanchez, M.; Llama-Palacios, A.; Marin, M.; Figuero, E.; Leon, R.; Blanc, V.; Herrera, D.; Sanz, M. Validation of ATP Bioluminescence as a Tool to Assess Antimicrobial Effects of Mouthrinses in an in Vitro Subgingival-Biofilm Model. Med. Oral Patol. Oral Cirugia Bucal 2013, 18, e86–e92. [Google Scholar] [CrossRef]
- Castro, J.; Lima, Â.; Sousa, L.G.V.; Rosca, A.S.; Muzny, C.A.; Cerca, N. Crystal Violet Staining Alone Is Not Adequate to Assess Synergism or Antagonism in Multi-Species Biofilms of Bacteria Associated with Bacterial Vaginosis. Front. Cell. Infect. Microbiol. 2022, 11, 795797. [Google Scholar] [CrossRef] [PubMed]
- Gascón, E.; Merino, N.; Pagán, E.; Berdejo, D.; Pagán, R.; García-Gonzalo, D. Assessment of In Vitro Biofilms by Plate Count and Crystal Violet Staining: Is One Technique Enough? In Detection and Enumeration of Bacteria, Yeast, Viruses, and Protozoan in Foods and Freshwater; Magnani, M., Ed.; Methods and Protocols in Food Science; Springer: New York, NY, USA, 2021; pp. 53–63. ISBN 978-1-07-161931-5. [Google Scholar]
- Hazan, R.; Que, Y.-A.; Maura, D.; Rahme, L.G. A Method for High Throughput Determination of Viable Bacteria Cell Counts in 96-Well Plates. BMC Microbiol. 2012, 12, 259. [Google Scholar] [CrossRef] [PubMed]
- Monica, S.; Bancalari, E.; Castellone, V.; Rijkx, J.; Wirth, S.; Jahns, A.; Bottari, B. ATP Bioluminescence for Rapid and Selective Detection of Bacteria and Yeasts in Wine. Appl. Sci. 2021, 11, 4953. [Google Scholar] [CrossRef]
- Griffith, C. Surface Sampling and the Detection of Contamination. In Handbook of Hygiene Control in the Food Industry; Elsevier: Amsterdam, The Netherlands, 2016; pp. 673–696. ISBN 978-0-08-100155-4. [Google Scholar]
- Amador, C.I.; Stannius, R.O.; Røder, H.L.; Burmølle, M. High-Throughput Screening Alternative to Crystal Violet Biofilm Assay Combining Fluorescence Quantification and Imaging. J. Microbiol. Methods 2021, 190, 106343. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibiotic | ESBL Strains | ||||
|---|---|---|---|---|---|
| E. coli ATCC 25922 | E. coli 9 | E. coli 10 | E. coli 11 | E. coli 12 | |
| AMX | R | R | R | R | R |
| AMC (sys) | R | R | R | R | R |
| AMC (ncuti) | R | R | R | R | * ND |
| TZP | S | S | S | S | S |
| CPN | S | R | R | R | R |
| CXM | S | R | R | R | R |
| CRO | S | R | R | R | R |
| CAZ | S | R | R | R | R |
| CPD | S | R | R | R | R |
| CFM * | S | R | R | R | R |
| CEF | S | R | R | R | R |
| IPM | S | S | S | S | S |
| MEM | S | S | S | S | S |
| ETP | S | S | S | S | S |
| GM | S | S | S | R | R |
| AMK | S | S | R | S | S |
| NIT | S | S | S | S | R |
| NOR | S | R | R | R | R |
| CIP | S | R | R | R | R |
| SXT | S | R | R | R | R |
| FOS | S | S | S | S | S |
| ESBL Strains | |||||
|---|---|---|---|---|---|
| E. coli ATCC 25922 | E. coli 9 | E. coli 10 | E. coli 11 | E. coli 12 | |
| CFU/cm2 | 99.41 | 98.91 | 99.06 | 96.89 | 97.54 |
| RLU | 90.31 | 71.90 | 53.47 | 37.84 | 60.85 |
| OD (600 nm) | 61.40 | 52.99 | 59.05 | 35.80 | 57.87 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovač, B.; Planinić, A.; Planinić, M.; Piletić, K.; Gobin, I. Treatment with Gaseous Ozone Significantly Reduced the Number of Bacteria in Extended-Spectrum-β-Lactamase (ESBL)-Producing Escherichia coli Biofilm. Hygiene 2023, 3, 125-135. https://doi.org/10.3390/hygiene3020011
Kovač B, Planinić A, Planinić M, Piletić K, Gobin I. Treatment with Gaseous Ozone Significantly Reduced the Number of Bacteria in Extended-Spectrum-β-Lactamase (ESBL)-Producing Escherichia coli Biofilm. Hygiene. 2023; 3(2):125-135. https://doi.org/10.3390/hygiene3020011
Chicago/Turabian StyleKovač, Bruno, Ana Planinić, Matej Planinić, Kaća Piletić, and Ivana Gobin. 2023. "Treatment with Gaseous Ozone Significantly Reduced the Number of Bacteria in Extended-Spectrum-β-Lactamase (ESBL)-Producing Escherichia coli Biofilm" Hygiene 3, no. 2: 125-135. https://doi.org/10.3390/hygiene3020011