
Trends in Octogenarian Pathology

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Population Prospects—Population Division—United Nations. Available online: https://population.un.org/wpp/ (accessed on 31 August 2021).
- Johnson, K.J.; Mutchler, J.E. The Emergence of a Positive Gerontology: From Disengagement to Social Involvement. Gerontologist 2014, 54, 93–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oksuzyan, A.; Jeune, B.; Juel, K.; Vaupel, J.W.; Christensen, K. Changes in Hospitalisation and Surgical Procedures among the Oldest-Old: A Follow-up Study of the Entire Danish 1895 and 1905 Cohorts from Ages 85 to 99 Years. Age Ageing 2013, 42, 476–481. [Google Scholar] [CrossRef] [Green Version]
- Mandawat, A.; Mandawat, A.; Mandawat, M.K.; Tinetti, M.E. Hospitalization Rates and In-Hospital Mortality among Centenarians. Arch. Intern. Med. 2012, 172, 1179–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, C.; Mitchell, S.; Paine, S.-J.; Kerse, N. Retrospective Analysis of the 13-Year Trend in Acute and Elective Surgery for Patients Aged 60 Years and over at Auckland City Hospital, New Zealand. J. Epidemiol. Community Health 2020, 74, 42–47. [Google Scholar] [CrossRef] [Green Version]
- Berlet, M.; Weber, M.-C.; Neumann, P.-A.; Friess, H.; Reim, D. Gastrectomy for Cancer beyond Life Expectancy. A Comprehensive Analysis of Oncological Gastric Surgery in Germany between 2008 and 2018. Front. Oncol. 2022, 12, 1032443. [Google Scholar] [CrossRef]
- Turri, G.; Caliskan, G.; Conti, C.; Martinelli, L.; De Giulio, E.; Ruzzenente, A.; Guglielmi, A.; Verlato, G.; Pedrazzani, C. Impact of Age and Comorbidities on Short- and Long-Term Outcomes of Patients Undergoing Surgery for Colorectal Cancer. Front. Oncol. 2022, 12, 959650. [Google Scholar] [CrossRef]
- Gajdos, C.; Kile, D.; Hawn, M.T.; Finlayson, E.; Henderson, W.G.; Robinson, T.N. Advancing Age and 30-Day Adverse Outcomes Following Non-Emergent General Surgical Operations. J. Am. Geriatr. Soc. 2013, 61, 1608–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haynes, W. Benjamini–Hochberg Method. In Encyclopedia of Systems Biology; Dubitzky, W., Wolkenhauer, O., Cho, K.-H., Yokota, H., Eds.; Springer: New York, NY, USA, 2013; p. 78. ISBN 978-1-4419-9863-7. [Google Scholar]
- International Senior Citizen’s Day 2020: Selected Data on Various Topics Regarding Israeli Senior Citizens Aged 65 and Over. Available online: https://www.cbs.gov.il/en/mediarelease/Pages/2020/International-Day-of-Senior-Citizens-Day-2020.aspx (accessed on 30 July 2023).
- Shaukat, A.; Kahi, C.J.; Burke, C.A.; Rabeneck, L.; Sauer, B.G.; Rex, D.K. ACG Clinical Guidelines: Colorectal Cancer Screening 2021. Am. J. Gastroenterol. 2021, 116, 458–479. [Google Scholar] [CrossRef]
- Siu, A.L. U.S. Preventive Services Task Force Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2016, 164, 279–296. [Google Scholar] [CrossRef] [Green Version]
- Engberg, H.; Christensen, K.; Andersen-Ranberg, K.; Jeune, B. Cohort Changes in Cognitive Function among Danish Centenarians. A Comparative Study of 2 Birth Cohorts Born in 1895 and 1905. Dement. Geriatr. Cogn. Disord. 2008, 26, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Engberg, H.; Christensen, K.; Andersen-Ranberg, K.; Vaupel, J.W.; Jeune, B. Improving Activities of Daily Living in Danish Centenarians--but Only in Women: A Comparative Study of Two Birth Cohorts Born in 1895 and 1905. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 1186–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, A.W.; Ogunwole, S.U.; Blakeslee, L.; Rabe, M.A. The Population 65 Years and Older in the United States: 2016; US Census Bureau: Suitland, MD, USA, 2016.
- Mondal, B.; Dubey, J.D. Gender Discrimination in Health-Care Expenditure: An Analysis across the Age-Groups with Special Focus on the Elderly. Soc. Sci. Med. 2020, 258, 113089. [Google Scholar] [CrossRef] [PubMed]
- Muzic, J.G.; Schmitt, A.R.; Wright, A.C.; Alniemi, D.T.; Zubair, A.S.; Olazagasti Lourido, J.M.; Sosa Seda, I.M.; Weaver, A.L.; Baum, C.L. Incidence and Trends of Basal Cell Carcinoma and Cutaneous Squamous Cell Carcinoma: A Population-Based Study in Olmsted County, Minnesota, 2000–2010. Mayo Clin. Proc. 2017, 92, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.H.; Chen, K.H.; Tseng, M.P.; Sun, C.C. Pattern of Skin Diseases in a Geriatric Patient Group in Taiwan: A 7-Year Survey from the Outpatient Clinic of a University Medical Center. Dermatology 2001, 203, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Lubeek, S.F.K.; van Vugt, L.J.; Aben, K.K.H.; van de Kerkhof, P.C.M.; Gerritsen, M.-J.P. The Epidemiology and Clinicopathological Features of Basal Cell Carcinoma in Patients 80 Years and Older: A Systematic Review. JAMA Dermatol. 2017, 153, 71–78. [Google Scholar] [CrossRef]
- Minami, C.A.; Bryan, A.F.; Freedman, R.A.; Revette, A.C.; Schonberg, M.A.; King, T.A.; Mittendorf, E.A. Assessment of Oncologists’ Perspectives on Omission of Sentinel Lymph Node Biopsy in Women 70 Years and Older with Early-Stage Hormone Receptor–Positive Breast Cancer. JAMA Netw. Open 2022, 5, e2228524. [Google Scholar] [CrossRef]
- Bomback, A.S.; Herlitz, L.C.; Markowitz, G.S. Renal Biopsy in the Elderly and Very Elderly: Useful or Not? Adv. Chronic Kidney Dis. 2012, 19, 61–67. [Google Scholar] [CrossRef]
- Moutzouris, D.-A.; Herlitz, L.; Appel, G.B.; Markowitz, G.S.; Freudenthal, B.; Radhakrishnan, J.; D’Agati, V.D. Renal Biopsy in the Very Elderly. Clin. J. Am. Soc. Nephrol. 2009, 4, 1073–1082. [Google Scholar] [CrossRef] [Green Version]
- Verde, E.; Quiroga, B.; Rivera, F.; López-Gómez, J.M. Renal Biopsy in Very Elderly Patients: Data from the Spanish Registry of Glomerulonephritis. Am. J. Nephrol. 2012, 35, 230–237. [Google Scholar] [CrossRef]
- Nair, R.; Bell, J.M.; Walker, P.D. Renal Biopsy in Patients Aged 80 Years and Older. Am. J. Kidney Dis. 2004, 44, 618–626. [Google Scholar] [CrossRef]
- Gupta, P.; Rana, D.S. Importance of Renal Biopsy in Patients Aged 60 Years and Older: Experience from a Tertiary Care Hospital. Saudi J. Kidney Dis. Transpl. 2018, 29, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Welch, B.T.; Welch, T.J.; Maus, T.P. Percutaneous Image-Guided Biopsy in an Elderly Population. J. Vasc. Interv. Radiol. 2010, 21, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.S.; Kanthapillai, P. Transthoracic Needle Biopsy for Suspected Thoracic Malignancy in Elderly Patients Using CT Guidance. Clin. Radiol. 1998, 53, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Lobo, B.; Casellas, F.; de Torres, I.; Chicharro, L.; Malagelada, J.R. Usefulness of Jejunal Biopsy in the Study of Intestinal Malabsorption in the Elderly. Rev. Esp. Enferm. Dig. 2004, 96, 259–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, O.S. Performing Colonoscopy in Elderly and Very Elderly Patients: Risks, Costs and Benefits. World J. Gastrointest. Endosc. 2014, 6, 220–226. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
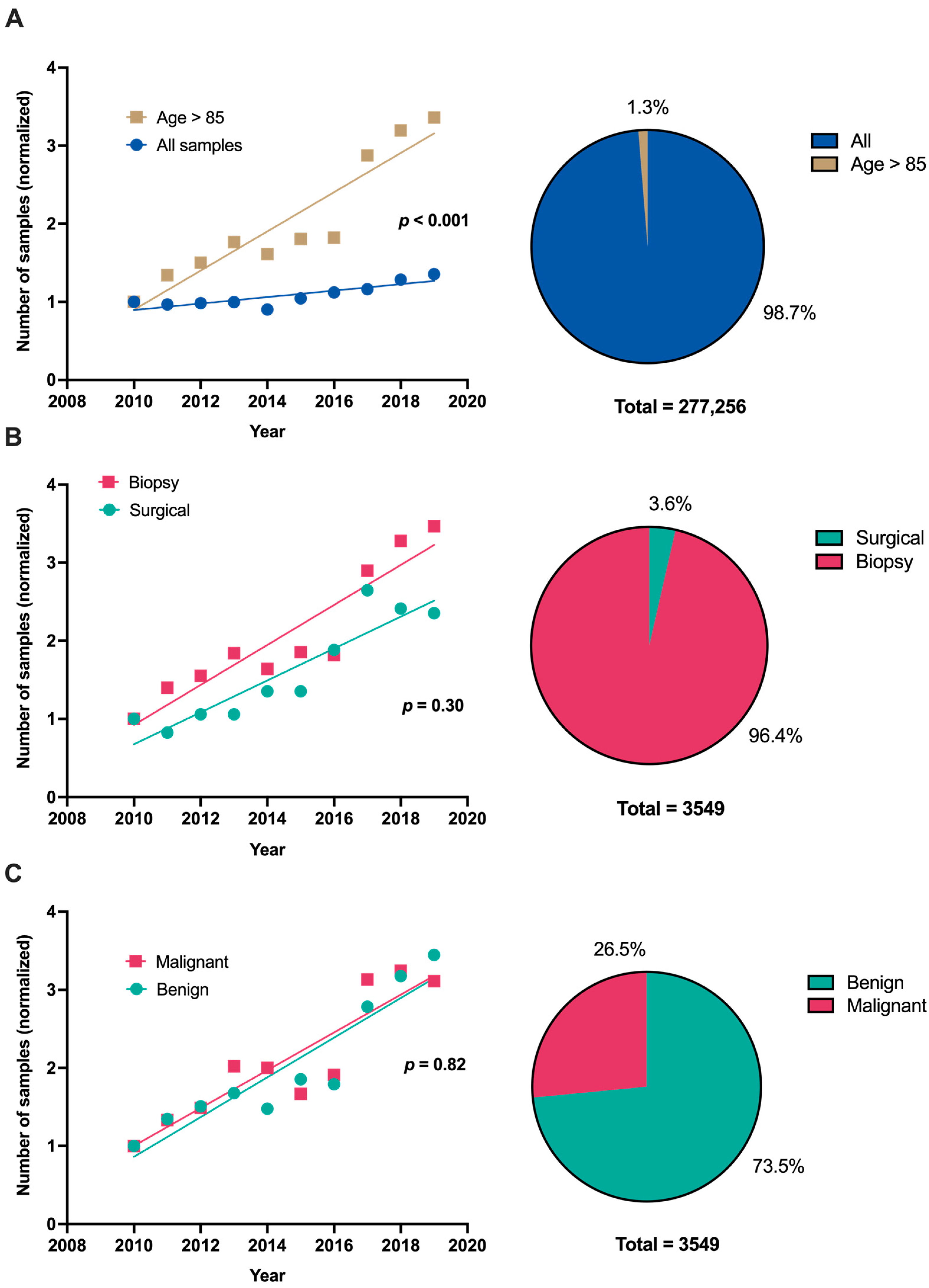
| 2010–2014 Avg./yr. ± SD (%) | 2015–2019 Avg./yr. ± SD (%) | p-Value | |
|---|---|---|---|
| Total samples | 253 ± 51 (100%) | 457 ± 131 (100%) | p = 0.022 |
| Malignant | 71 ± 20 (27.6%) | 118 ± 34 (25.7%) | p = 0.053 |
| Surgical | 18 ± 3 (7.3%) | 36 ± 9 (8.1%) | p = 0.013 |
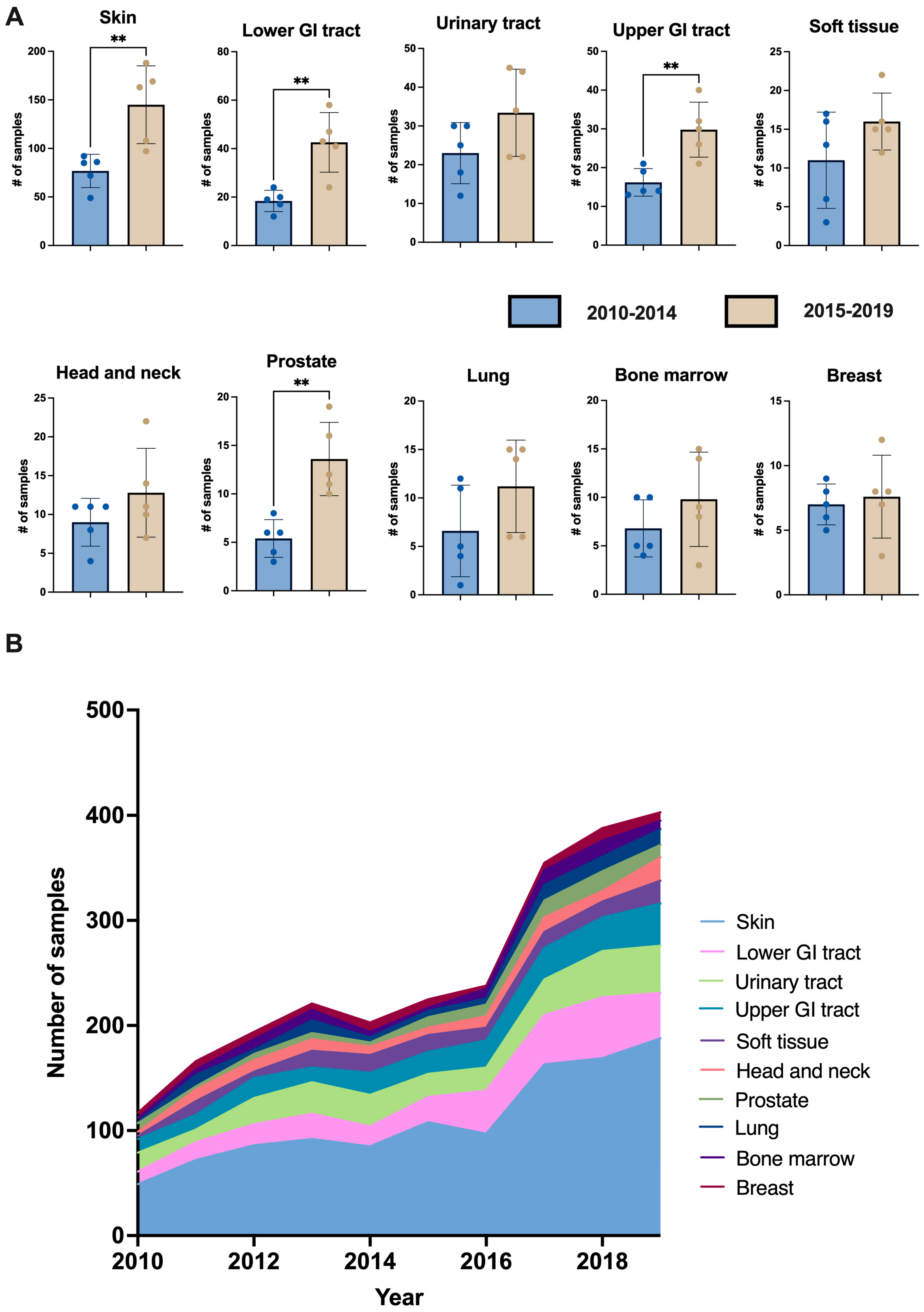
| Origin of sample: | |||
| Skin | 77 ± 17 (30.4%) | 145 ± 40 (31.9%) | p = 0.021 |
| Lower GI tract | 18 ± 4 (7.3%) | 43 ± 12 (9.5%) | p = 0.013 |
| Urinary tract | 23 ± 8 (9.1%) | 33 ± 11 (7.2%) | p = 0.195 |
| Upper GI tract | 16 ± 4 (6.5%) | 30 ± 7 (6.7%) | p = 0.013 |
| Soft tissue | 11 ± 6 (4.2%) | 16 ± 4 (3.7%) | p = 0.231 |
| Head and neck | 9 ± 3 (3.5%) | 13 ± 6 (2.8%) | p = 0.271 |
| Prostate | 5 ± 2 (2.3%) | 14 ± 4 (3.1%) | p = 0.026 |
| Lung | 7 ± 5 (2.5%) | 11 ± 5 (2.4%) | p = 0.208 |
| Bone marrow | 7 ± 3 (2.7%) | 10 ± 5 (2.1%) | p = 0.293 |
| Breast | 7 ± 2 (2.8%) | 8 ± 3 (1.7%) | p = 0.720 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keidar Haran, T.; Haran, A.; Pillar, N. Trends in Octogenarian Pathology. J. Ageing Longev. 2023, 3, 442-449. https://doi.org/10.3390/jal3030018
Keidar Haran T, Haran A, Pillar N. Trends in Octogenarian Pathology. Journal of Ageing and Longevity. 2023; 3(3):442-449. https://doi.org/10.3390/jal3030018
Chicago/Turabian StyleKeidar Haran, Tal, Arnon Haran, and Nir Pillar. 2023. "Trends in Octogenarian Pathology" Journal of Ageing and Longevity 3, no. 3: 442-449. https://doi.org/10.3390/jal3030018