
Artificial Intelligence and Democratization of the Use of Lung Ultrasound in COVID-19: On the Feasibility of Automatic Calculation of Lung Ultrasound Score

 ,
, 
Abstract
:1. Introduction
- •
- Irregular pleural lines and focal B lines: 1 point;
- •
- Confluent B lines (<50%): 2 points;
- •
- Confluent B lines (>50%): 3 points;
- •
- Subpleural or lobar consolidation or pleural effusion: 3 points.
2. Materials and Methods
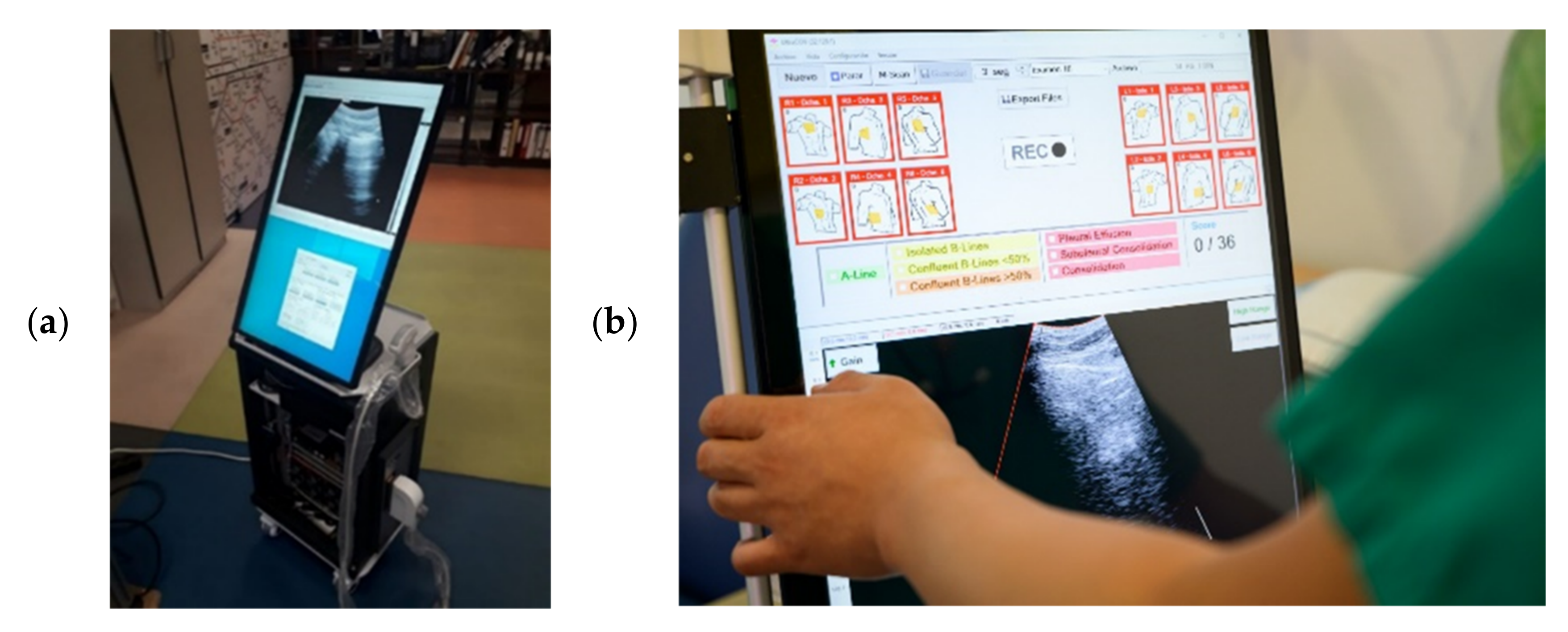
2.1. Lung-Scanner Prototype
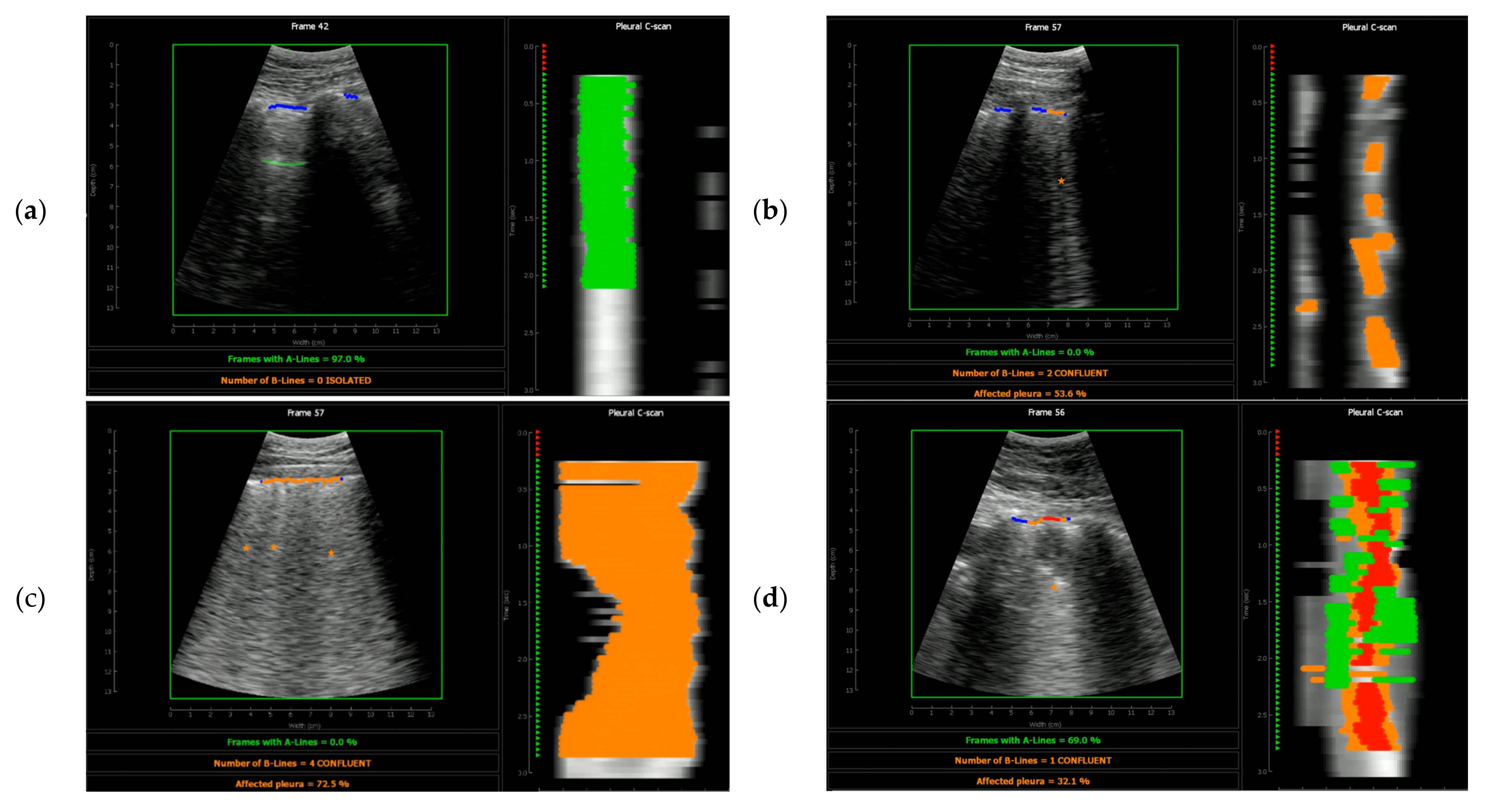
2.2. Automatic Detection Algorithm
- •
- Pleura detection. It based on the fact that, when the probe is still, the image above the pleura almost does not change, while variations can be observed below the pleura during the respiratory cycle. A motion filter identifies the boundary between the two zones, which is used as an initial guess to find the pleura as a continuous bright line around that depth.
- •
- A-Lines detection. A-Lines are identified as replicas of the pleura at depths multiple of the probe-pleura distance, looking for continuous and bright horizontal lines parallel to the pleura. Despite not being used for calculating the lung score, its presence is used to discard false B-Lines and consolidations;
- •
- B-Lines detection. Each one of the image lines is fitted to a first-degree polynomial, starting at the detected pleura. The criteria to detect a B-Line are based on the slope of that best fit line: Higher slopes correspond to bright vertical artifacts that increase their bright towards the bottom of the image, which corresponds with a B-Line. The percentage of the affected pleura is obtained by the ratio of lines marked as B-Lines to the total number of image lines containing the pleura;
- •
- Consolidations. There are two criteria that should be met to detect a consolidation. First, the pleura is not seen as a continuous bright line, which is measured through the standard deviation of the difference between consecutive pleura points. Second, the B-Line criterion is meet, but a dark zone is present between the pleura and the starting point of the B-Line. In this case, the image line is marked as consolidation;
- •
- Pleura effusion. A pleura effusion is detected when there is a dark zone above the pleura, and the pleura line moves vertically during the video. This way, they are differenced from consolidations, which usually move laterally but not vertically during the acquisition time.
2.3. Clinical Study Population
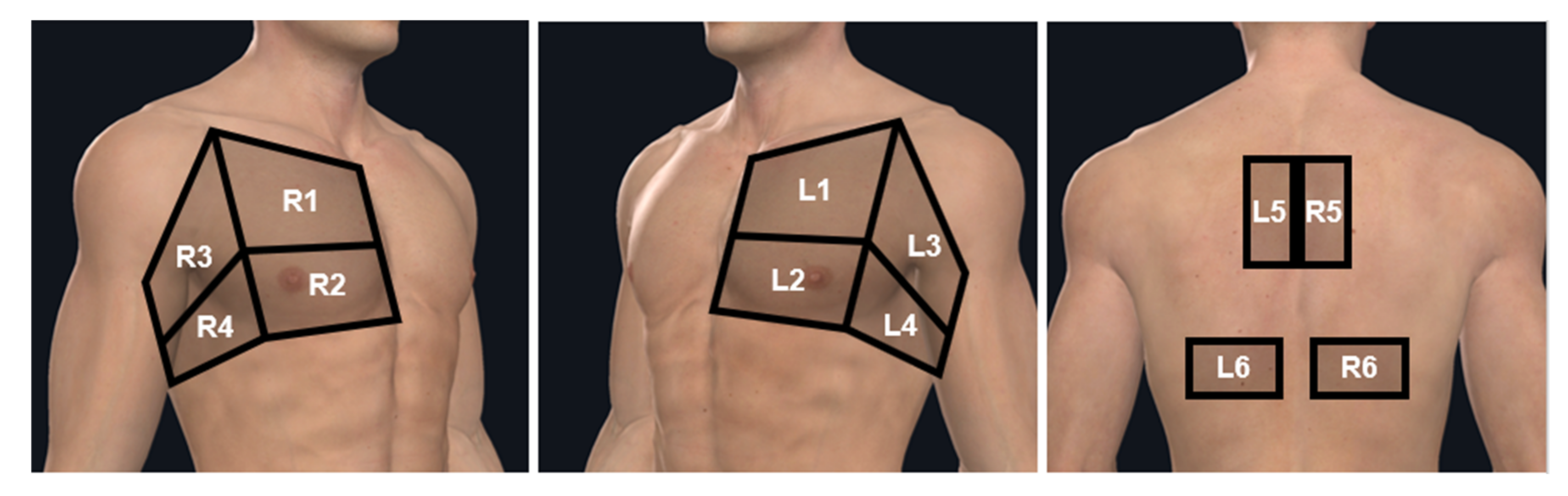
2.4. Exploration Zones
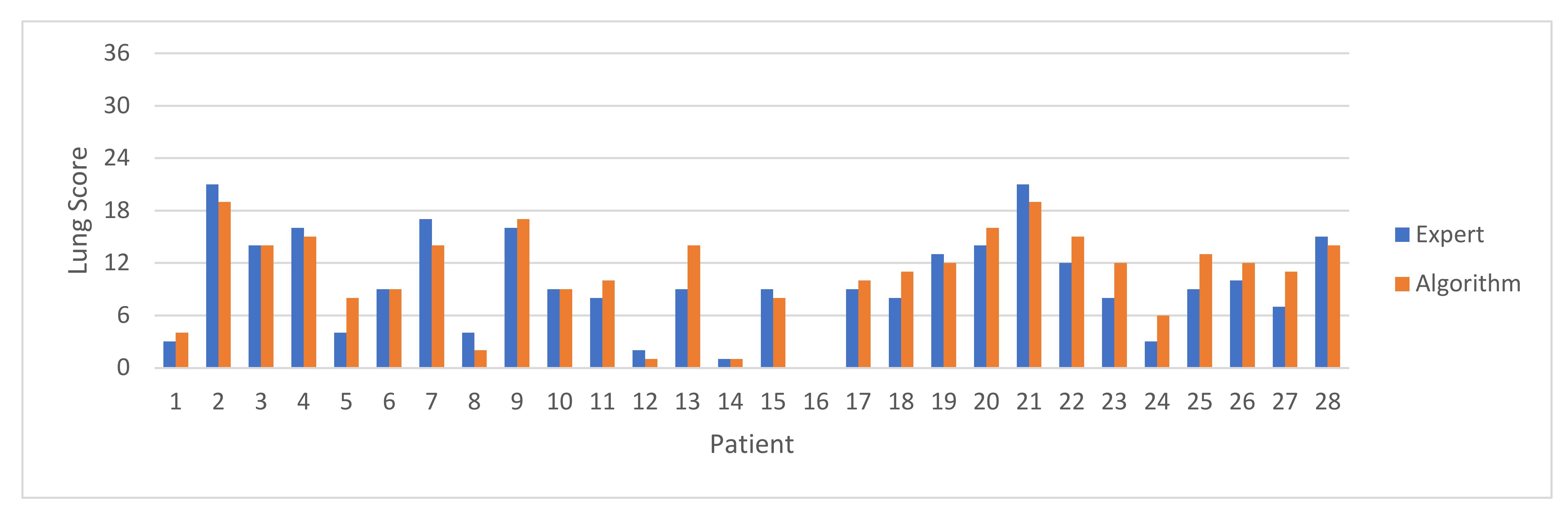
3. Results
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, R.B.; Tayal, V.S.; Panebianco, N.L.; Tung-Chen, Y.; Nagdev, A.; Shah, S.; Pivetta, E.; Henwood, P.C.; Nelson, M.J.; Moore, C.L. Ultrasound on the frontlines of COVID-19: Report from an international webinar. Acad. Emerg. Med. 2020, 27, 523–526. [Google Scholar] [CrossRef]
- Hernández-Píriz, A.; Tung-Chen, Y.; Jiménez-Virumbrales, D.; Ayala-Larrañaga, I.; Barba-Martín, R.; Canora-Lebrato, J.; Zapatero-Gaviria, A.; De Casasola-Sánchez, G.G. Importance of lung ultrasound follow-up in patients who had recovered from coronavirus disease 2019: Results from a prospective study. J. Clin. Med. 2021, 10, 3196. [Google Scholar] [CrossRef]
- Islam, N.; Ebrahimzadeh, S.; Salameh, J.-P.; Kazi, S.; Fabiano, N.; Treanor, L.; Absi, M.; Hallgrimson, Z.; Leeflang, M.M.G.; Hooft, L.; et al. Thoracic imaging tests for the diagnosis of COVID-19. Cochrane Database Syst. Rev. 2021, CD013639. [Google Scholar] [CrossRef]
- Tung-Chen, Y.; Martí de Gracia, M.; Díez-Tascón, A.; Alonso-González, R.; Agudo-Fernández, S.; Parra-Gordo, M.L.; Ossaba-Vélez, S.; Rodríguez-Fuertes, P.; Llamas-Fuentes, R. Correlation between chest computed tomography and lung ultrasonography in patients with coronavirus disease 2019 (COVID-19). Ultrasound. Med. Biol. 2020, 46, 2918–2926. [Google Scholar] [CrossRef] [PubMed]
- Tung-Chen, Y.; Gil-Rodrigo, A.; Algora-Martín, A.; Llamas-Fuentes, R.; Rodríguez-Fuertes, P.; Marín-Baselga, R.; Alonso-Martínez, B.; Rodríguez, E.S.; Soriano, P.L.; Ramos-Rincón, J.-M. The lung ultrasound “Rule of 7” in the prognosis of COVID-19 patients: Results from a prospective multicentric study [published online ahead of print, 2021 Sep 4]. Med. Clin. 2021; in press. [Google Scholar] [CrossRef]
- Anantrasirichai, N.; Hayes, W.; Allinovi, M.; Bull, D.; Achim, A. Line detection as an inverse problem: Application to lung ultrasound imaging. IEEE Trans. Med. Imaging 2017, 36, 2045–2056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baloescu, C.; Toporek, G.; Kim, S.; McNamara, K.; Liu, R.; Shaw, M.M.; McNamara, R.L.; Raju, B.I.; Moore, C.L. Automated lung ultrasound b-line assessment using a deep learning algorithm. IEEE Trans. Ultras. Ferr. Freq. Cont. 2020, 67, 2312–2320. [Google Scholar] [CrossRef] [PubMed]
- Born, J.; Wiedemann, N.; Cossio, M.; Buhre, C.; Brändle, G.; Leidermann, K.; Aujayeb, A.; Moor, M.; Rieck, B.; Borgwardt, K. Accelerating detection of lung pathologies with explainable ultrasound image analysis. Appl. Sci. 2021, 11, 672. [Google Scholar] [CrossRef]
- Diaz-Escobar, J.; Ordóñez-Guillén, N.E.; Villarreal-Reyes, S.; Galaviz-Mosqueda, A.; Kober, V.; Rivera-Rodriguez, R.; Lozano Rizk, J.E. Deep-learning based detection of COVID-19 using lung ultrasound imagery. PLoS ONE 2021, 16, e0255886. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Menapace, W.; Oei, S.; Luijten, B.; Fini, E.; Saltori, C.; Huijben, I.; Chennakeshava, N.; Mento, F.; Sentelli, A.; et al. Deep learning for classification and localization of covid-19 markers in point-of-care lung ultrasound. IEEE Trans. Med. Imaging 2020, 39, 2676–2687. [Google Scholar] [CrossRef] [PubMed]
- Mento, F.; Perrone, T.; Fiengo, A.; Smargiassi, A.; Inchingolo, R.; Soldati, G.; Demi, L. Deep learning applied to lung ultrasound videos for scoring COVID-19 patients: A multicenter study. J. Acoust. Soc. Am. 2021, 149, 3626–3634. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | Units |
|---|---|---|
| Scan type | Sector scan | |
| Active aperture | 32 | elements |
| No. of image lines | 82 | lines |
| Image depth | 13 | cm |
| Emission focus depth | 4 | cm |
| Digital band-pass filter | 1.8 to 5 | MHz |
| Time-gain compensation | 0.14 | dB/mm |
| Indication | Coincidence | False Positives | False Negatives |
|---|---|---|---|
| A-Lines | 70.7% | 23.1% | 6.2% |
| Isolated B-Lines | 84.4% | 7.5% | 8.1% |
| Confluent B-Lines (<50%) | 79.3% | 11.1% | 9.6% |
| Confluent B-Lines (>50%) | 85.3% | 8.1% | 6.6% |
| Any B-Line | 88.0% | 7.8% | 4.2% |
| Pleura effusion | 99.7% | 0.0% | 0.3% |
| Consolidation | 93.4% | 4.2% | 2.4% |
| Zone score | 72.8% | 16.5% | 10.7% |
| Artifact Type | Number of Videos | Percentage |
|---|---|---|
| Videos with A-Lines | 207 | 62.0% |
| Videos with B-Lines | 163 | 48.8% |
| Videos with pleura effusion | 1 | 0.3% |
| Videos with consolidations | 25 | 7.5% |
| Total | 334 | 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camacho, J.; Muñoz, M.; Genovés, V.; Herraiz, J.L.; Ortega, I.; Belarra, A.; González, R.; Sánchez, D.; Giacchetta, R.C.; Trueba-Vicente, Á.; et al. Artificial Intelligence and Democratization of the Use of Lung Ultrasound in COVID-19: On the Feasibility of Automatic Calculation of Lung Ultrasound Score. Int. J. Transl. Med. 2022, 2, 17-25. https://doi.org/10.3390/ijtm2010002
Camacho J, Muñoz M, Genovés V, Herraiz JL, Ortega I, Belarra A, González R, Sánchez D, Giacchetta RC, Trueba-Vicente Á, et al. Artificial Intelligence and Democratization of the Use of Lung Ultrasound in COVID-19: On the Feasibility of Automatic Calculation of Lung Ultrasound Score. International Journal of Translational Medicine. 2022; 2(1):17-25. https://doi.org/10.3390/ijtm2010002
Chicago/Turabian StyleCamacho, Jorge, Mario Muñoz, Vicente Genovés, Joaquín L. Herraiz, Ignacio Ortega, Adrián Belarra, Ricardo González, David Sánchez, Roberto Carlos Giacchetta, Ángela Trueba-Vicente, and et al. 2022. "Artificial Intelligence and Democratization of the Use of Lung Ultrasound in COVID-19: On the Feasibility of Automatic Calculation of Lung Ultrasound Score" International Journal of Translational Medicine 2, no. 1: 17-25. https://doi.org/10.3390/ijtm2010002