
Changes in Paediatric Injury-Related Emergency Department Presentations during the COVID-19 Pandemic


1
Australian Institute of Health Innovation, Macquarie University, Sydney 2109, Australia
2
Children’s Hospital Institute of Sports Medicine, The Children’s Hospital at Westmead, Sydney 2145, Australia
3
Discipline of Exercise and Sport Science, Faculty of Medicine and Health, The University of Sydney, Sydney 2006, Australia
4
Discipline of Child and Adolescent Health, Sydney Medical School, The University of Sydney, Sydney 2006, Australia
5
Emergency Department, The Children’s Hospital at Westmead, Sydney 2145, Australia
*
Author to whom correspondence should be addressed.
Trauma Care 2023, 3(2), 46-54; https://doi.org/10.3390/traumacare3020006
Submission received: 24 January 2023
/
Revised: 12 March 2023
/
Accepted: 30 March 2023
/
Published: 3 April 2023
Abstract
:This study aimed to quantify changes in paediatric injury-related Emergency Department (ED) presentations at a large metropolitan paediatric hospital during the first two years of the COVID-19 pandemic (i.e., 2020 and 2021). This retrospective cohort study included children aged ≤15 years who presented to the ED at the Children’s Hospital at Westmead, Sydney, New South Wales, Australia, with a principal diagnosis of injury during 1 January 2010 to 31 December 2021. Annual and monthly incidence of paediatric injury-related ED presentations from 2010 to 2019 were used to fit autoregressive integrated moving average models, from which forecast estimates with 95% prediction intervals were derived and compared against corresponding observed values to obtain estimates of absolute and relative forecast errors. The distributions of injuries by injury severity in 2020 and 2021 were compared against the 2010–2019 reference period. The annual incidence of paediatric injury-related ED presentations was 7.6% and 4.7% lower than forecasted in 2020 and 2021, respectively, equating to an estimated total of 1683 fewer paediatric injury-related ED presentations during the two-year period. The largest reductions in monthly incidence of paediatric injury-related ED presentations were observed during the periods of major societal restrictions (i.e., March–May 2020 and July–October 2021). Significant reductions in monthly incidence of injury-related ED presentations were observed for minor injuries only, with no discernable reductions in moderate and serious injuries. These findings highlight the impact of the COVID-19 pandemic on paediatric injury-related ED presentations and the need for future epidemiological studies examining secular trends in paediatric trauma volumes to account for the impact of the COVID-19 pandemic.
1. Introduction
The World Health Organization declared the novel coronavirus disease (COVID-19) a global pandemic on 11 March 2020 [1]. In the weeks and months that followed, many governments introduced wide-reaching public health measures to reduce community transmission of COVID-19 [2]. In New South Wales (NSW), Australia, the government cancelled major events with more than 500 people on 15 March 2020. This was followed by a ban on non-essential indoor public gatherings of 100 persons or more and the introduction of the social distancing requirements of 1.5 m on 18 March 2020. Additional measures were introduced on 23 March 2020, including closure of non-essential services such as pubs and clubs, gyms, indoor sporting venues, cinemas, and entertainment venues, while restaurants and cafes could provide takeaway services only. A general public lockdown requiring people to stay at home except for essential reasons was imposed on 31 March, and these public health measures remained in effect until a progressive easing of restrictions started on 15 May 2020. Following a major outbreak, another general lockdown was imposed in several local government areas in metropolitan Sydney on 25 June 2021. The area and duration of this lockdown were extended in the following weeks and remained in effect until 11 October 2021.
Government restrictions and public health measures aimed at reducing community transmission of COVID-19 can have unintended consequences such as reducing exposure to major external causes of injury in young people. For instance, stay-at-home orders reduced traffic volumes in metropolitan areas [3], which in turn reduced road traffic crashes [4,5]. Similarly, community sport was cancelled, indoor exercise and recreation facilities were closed, and outdoor exercise and recreation was limited to individual physical activity in local neighbourhoods, all of which contributed to reductions in physical activity [6,7,8,9]. With reductions in exposure to major external causes of injury, there have been corresponding reductions in injury-related trauma volumes. Previous studies have shown that the COVID-19 pandemic resulted in reduced major trauma volumes among Australian adults [10,11,12]. However, the impact of the COVID-19 pandemic on both minor and major trauma volumes among Australian children remains to be determined.
Therefore, the primary aim of this study was to quantify changes in the incidence of paediatric injury-related ED presentations at a large metropolitan paediatric hospital in Sydney, NSW, Australia, during the first two years of the COVID-19 pandemic (i.e., 2020 and 2021). The secondary aim was to compare the distributions of paediatric injury-related ED presentations by injury severity in 2020 and 2021 to the 2010–2019 reference period.
2. Materials and Methods
2.1. Study Design
Retrospective cohort study.
2.2. Study Population
This study included children aged ≤15 years who presented to the ED at the Children’s Hospital at Westmead (CHW), Sydney, Australia, with a principal diagnosis of injury during 1 January 2010 to 31 December 2021. Injury-related ED presentations were identified using the International Classification of Diseases, 10th Revision, Australian Modification (ICD-10-AM) principal diagnosis codes S00-T78 [13].
2.3. Data Sources
The ED presentation data were obtained from the CHW ED information system, which included patient demographics (i.e., sex, age, and residential postcode), arrival information (i.e., date, mode of arrival, and triage category), departure information (i.e., date, departure status), and ICD-10-AM principal diagnosis code.
The Index of Relative Socioeconomic Disadvantage (IRSD) is an index that summarises the general economic and social conditions of people and households within an area. The index is derived from Australian population census data such as household income, level of education, employment, and type of occupation, with lower scores indicating greater socioeconomic disadvantage. IRSD scores were categorised into quintiles and mapped to the residential postcode for each child [14].
The International Classification of Injury Severity Score (ICISS), which is based on previously validated survival rate ratios for a paediatric population, was used to categorise the ED presentations as either serious injury (ICISS ≤ 0.98), moderate injury (ICISS 0.98–0.99), and minor injury (ICISS ≥ 0.99) [15,16].
2.4. Data Analysis
Summary statistics were used to describe the characteristics of the cohort. Annual and monthly incidence of paediatric injury-related ED presentations were calculated with 95% confidence intervals (CI). Data from 1 January 2010 to 31 December 2019, which have been analysed and published previously [17], were used as a reference period for comparisons and forecasting. Time series forecasting involved fitting autoregressive integrated moving average models of annual incidence of paediatric injury-related ED presentations using the methods described by Hyndman and Athanasopoulos [18]. Forecast estimates with 95% prediction intervals for 2020 and 2021 were derived from autoregressive integrated moving average models and compared against the observed values for 2020 and 2021. The absolute and relative differences between forecasted and observed values were used as measures of absolute and relative impact of the COVID-19 pandemic on annual and monthly incidence of paediatric injury-related ED presentations.
The proportions of minor, moderate, and serious injuries in 2020 and 2021 were compared to the 2010–2019 reference period using two-tailed chi-square tests with the alpha set to 0.05.
All statistical analyses were conducted using R, version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria) and the forecast package [19].
2.5. Ethical Considerations
Ethical approval was provided by the Sydney Children’s Hospitals Network Human Research Ethics Executive Committee (reference number: 2020/ETH00083).
3. Results
A total of 27,395 children aged ≤15 years presented to the ED at CHW for injury during the first two years of the COVID-19 pandemic, with males and females accounting for 59.8% (n = 16,391) and 40.2% (n = 11,004) of the ED presentations, respectively (Table 1). With regard to severity, 85.9% (n = 23,529) were minor, 12.6% (n = 3456) were moderate, and 1.5% (n = 410) were serious. A total of 18.8% (n = 5143) of children were admitted to hospital. The most common types of injury were head injuries (27.4%; n = 7517) and elbow and forearm injuries (15.4%; n = 4230) (Table 2).
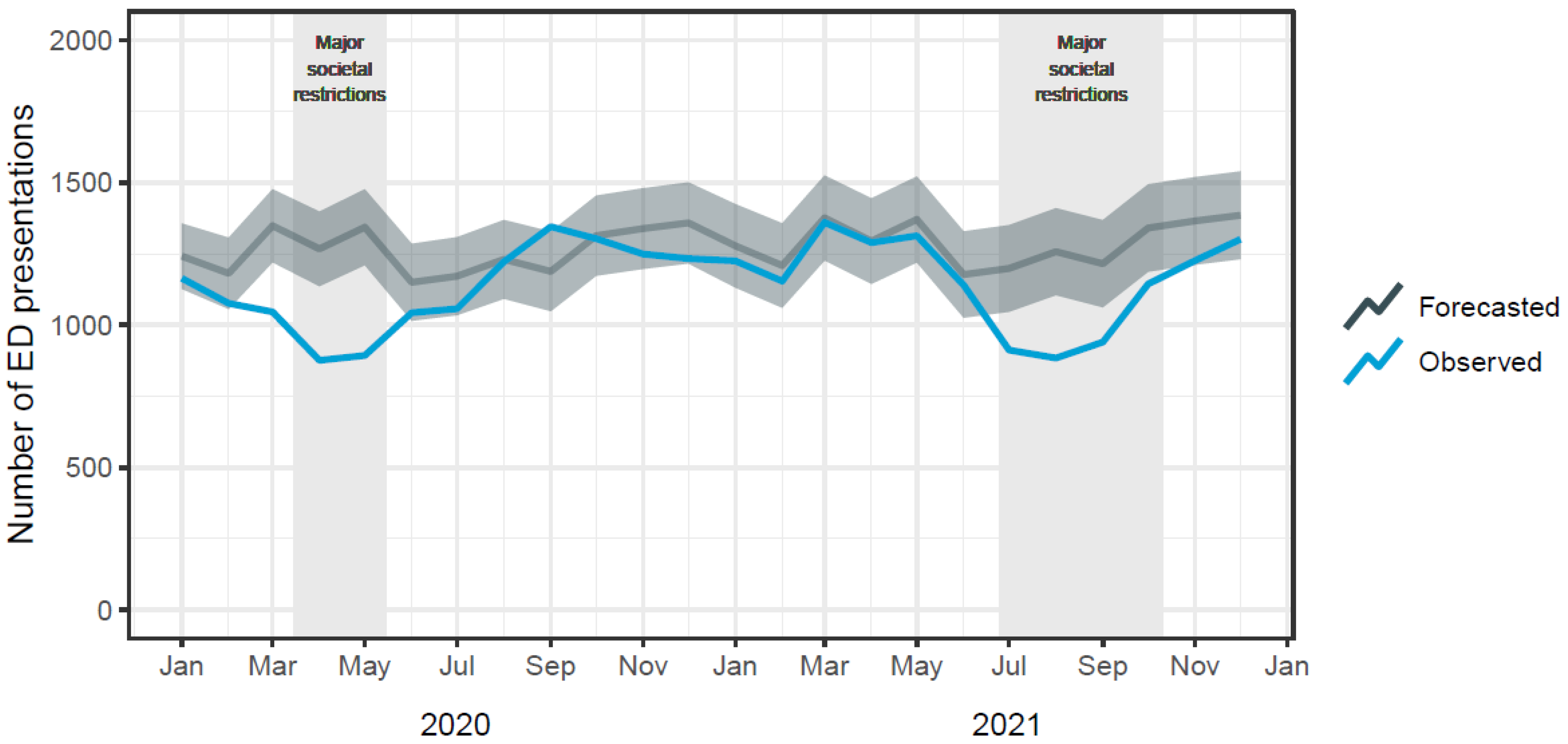
The annual incidence of paediatric injury-related ED presentations was forecasted to be 14,539 (95% PI 13,266–15,812) in 2020 and 14,539 (95% PI 12,738–16,340) in 2021. The observed annual incidence of paediatric injury-related ED presentations was 13,507 in 2020 and 13,888 in 2021. Compared to forecasts, there were an estimated 1032 (7.6%) and 651 (4.7%) fewer paediatric injury-related ED presentations during 2020 and 2021, respectively.
Figure 1 shows the forecasted and observed monthly incidence of paediatric injury-related ED presentations. The observed monthly incidence of paediatric injury-related ED presentations was lower than forecasted for every month except September 2020, with the largest relative differences observed during the periods March–May 2020 and July–October 2021 (Table 3).
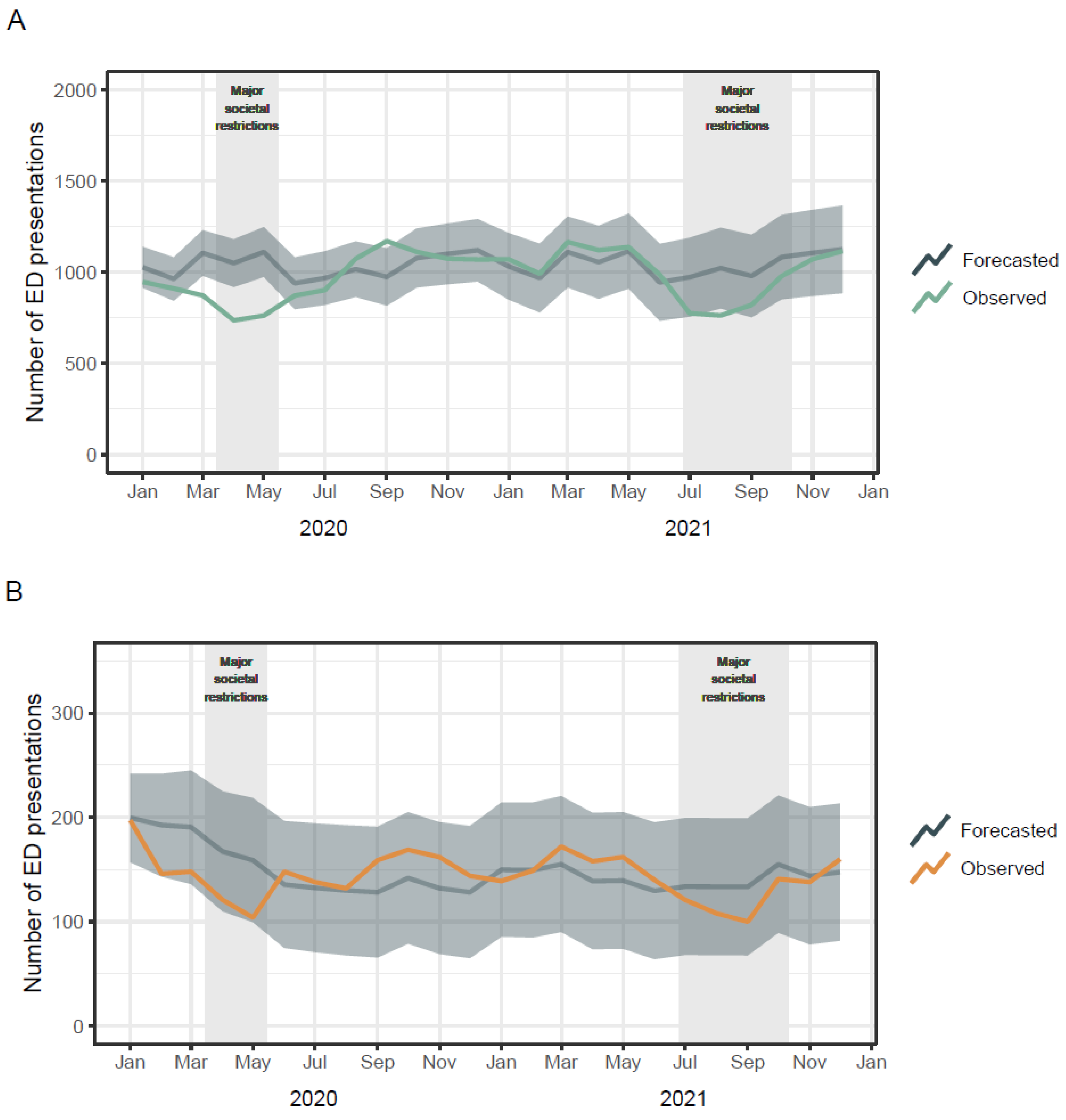
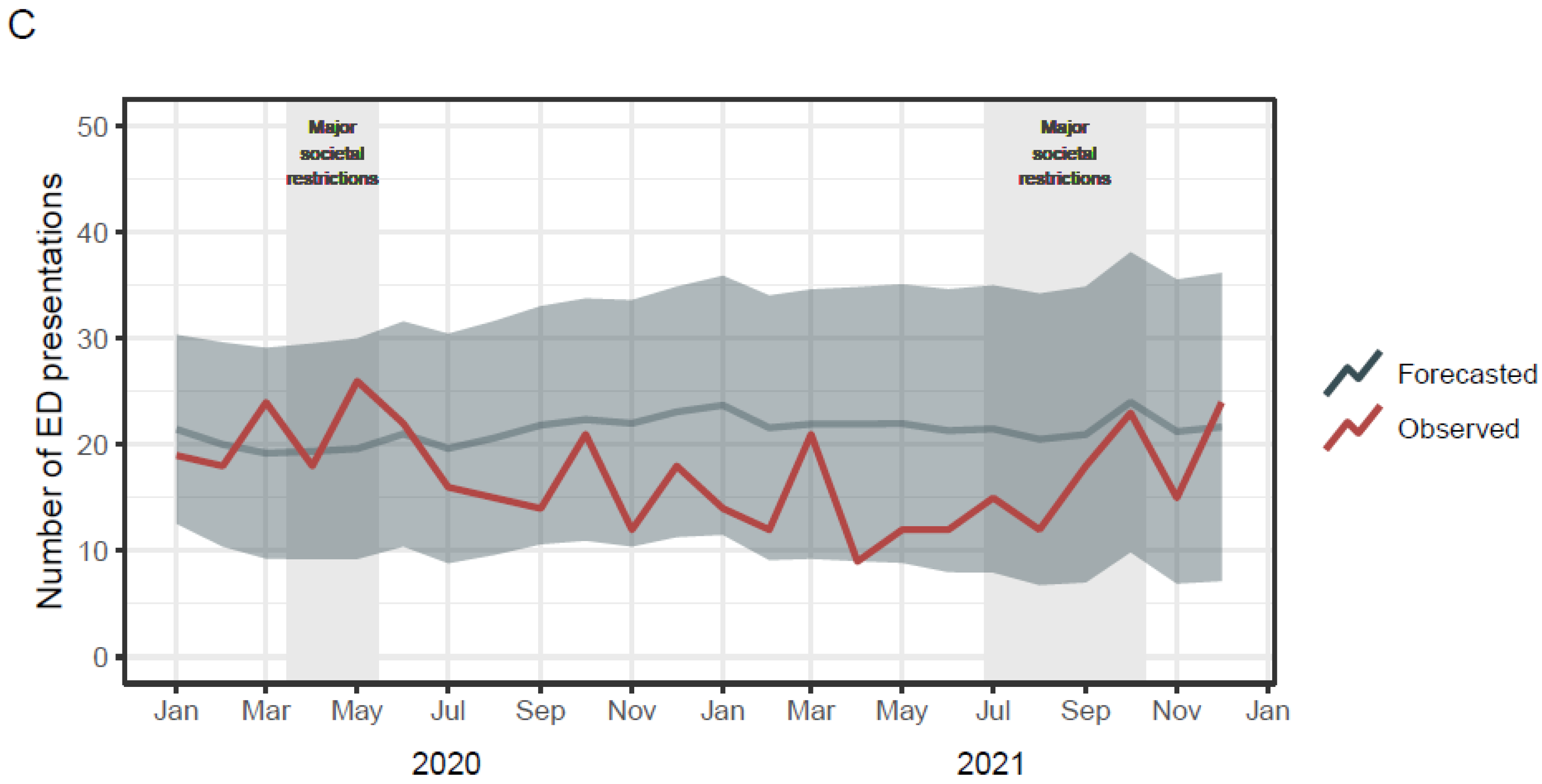
The proportions of minor, moderate, and serious injuries were significantly different in 2020 (mild: 85.2%; moderate: 13.1%; serious: 1.7%; χ2 = 177.46, p < 0.001) and 2021 (mild: 85.2%; moderate: 13.1%; serious: 1.7%; χ2 = 74.13, p < 0.001), compared to the 2010–2019 reference period (mild: 88.8%; moderate: 10.3%; serious: 0.9%). Figure 2 shows that the differences in proportions were due to significant reductions in the monthly incidence of minor injuries, with no discernable reductions in the monthly incidence of moderate and serious injuries.
4. Discussion
This study quantified the impact of the COVID-19 pandemic on paediatric trauma presentations at a large metropolitan paediatric hospital in Sydney, Australia. It found that the annual incidence of paediatric injury-related ED presentations was lower than forecasted during the first two years of the COVID-19 pandemic, with significantly lower trauma volumes observed during the periods with government-imposed major societal restrictions (i.e., from March–May 2020 and July–October 2021). This study also showed that the reductions in trauma volumes were driven by reductions in minor injuries, with no discernable reductions in moderate and serious injuries.
There are limited data on paediatric trauma volumes in Australia to which the main findings of the current study can be compared. Previous single-centre studies have shown that major trauma volumes among Australian adults were reduced by about 30% during the first wave of major societal restrictions during the COVID-19 pandemic [10,11,12]. The current study found similar reductions in paediatric trauma volumes during both periods of major societal restrictions in the relevant hospital catchment area.
This study found significant differences in the proportions of minor, moderate, and serious paediatric injury-related ED presentation between pandemic and pre-pandemic periods, and these changes were due to larger reductions in the volume of minor injuries than moderate and serious injuries. It is difficult to compare this finding to previous studies examining the impact to COVID-19 on trauma volumes in Australia because the previous studies examined adult admitted trauma patients [10,11,12]. The studies on Australian adult admitted trauma patients found reduced trauma volumes but no significant changes in median injury severity scores [10,11,12], which is consistent with the majority of studies from other countries [20].
Information on mechanisms of injury was not available in the ED data in the current study, thus precluding comparison with previous studies. Previous studies have found significant reductions in major trauma admissions due to road traffic collisions and falls in both Australia and other countries during periods of societal restrictions [11,12,20]. Previous studies have also reported significant increases in trauma due to assault and self-harm and trauma occurring in the home [12,20].
Although the COVID-19 pandemic has had a profound impact on global health and caused major socio-economic disruption worldwide [21], its full long-term societal impact is yet to be determined. The COVID-19 pandemic also has implications for future epidemiological studies investigating secular trends in trauma volumes. Future epidemiological studies are strongly recommended to employ analysis methods that account for both the impact of the COVID-19 pandemic and pre-pandemic secular trends in incidence. One alternative is interrupted time series analysis, which involves segmented regression modelling whereby the regression coefficients estimate the pre-event slope (i.e., trend in outcome before the event), the level change (i.e., change in level of the outcome at the time of the event), and the change in slope (i.e., difference between pre-event and post-event slopes) [22,23,24]. It should be noted that the independence assumption is unlikely to hold for time series of counts data or derivative incidence rates, with year-on-year observations very likely to be correlated. Because serial correlation can result in underestimation of standard errors and p-values, it may be necessary to fit regression models that can handle autocorrelated observations (e.g., autoregressive moving average models) [22,23]
A strength of this study is its application of forecasting methods to account for pre-pandemic trends and seasonality in the incidence of paediatric injury-related ED presentations. The generalisability of the findings may be limited because the data were obtained from a single hospital only. Unfortunately, no specific denominator data on children aged ≤15 years were available for the CHW catchment area, which precluded calculation of age- and sex-adjusted incidence rates of paediatric injury-related ED presentations. The data source for this study did not contain ICD-10-AM coded data on external cause of injury, place of occurrence, or activity, which precluded analyses of mechanisms of injury.
5. Conclusions
Paediatric trauma volumes were significantly reduced during periods of major societal restrictions aimed at reducing community transmission of COVID-19. The impact was greater on minor trauma volume, with no discernable reductions in moderate and serious injuries. These findings highlight the need for future epidemiological studies examining secular trends in paediatric trauma volumes to account for the impact of the COVID-19 pandemic.
Author Contributions
Conceptualization, R.P.L., A.F. and G.B.; methodology, R.P.L.; data analysis, R.P.L.; writing—original draft preparation, R.P.L.; writing—review and editing, A.F., R.O. and G.B.; visualization, R.P.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Sydney Children’s Hospitals Network Human Research Ethics Executive Committee (reference number: 2020/ETH00083).
Informed Consent Statement
Patient consent was waived because it involved a secondary analysis of administrative data, which could not practicably be carried out without a waiver of consent.
Data Availability Statement
The data used in this study are available at reasonable request from The Children’s Hospital at Westmead, Sydney, Australia, subject to obtaining relevant ethics and governance approvals required by the hospital.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 23 October 2022).
- Roth, L. NSW Public Health Restrictions to Deal with the COVID-19 Pandemic: A Chronology; Issues Backgrounder 5/2020; NSW Parliamentary Research Service: Sydney, NSW, Australia, 2020. [Google Scholar]
- Marchant, A. What Can Traffic Data Tell Us about the Impact of the Coronavirus? Available online: https://www.tomtom.com/newsroom/explainers-and-insights/covid-19-traffic/ (accessed on 30 November 2022).
- Qureshi, A.I.; Huang, W.; Khan, S.; Lobanova, I.; Siddiq, F.; Gomez, C.R.; Suri, M.F.K. Mandated societal lockdown and road traffic accidents. Accid. Anal. Prev. 2020, 146, 105747. [Google Scholar] [CrossRef] [PubMed]
- Chand, S.; Yee, E.; Alsultan, A.; Dixit, V.V. A descriptive analysis on the impact of COVID-19 lockdowns on road traffic incidents in Sydney, Australia. Int. J. Environ. Res. Public Health 2021, 18, 11701. [Google Scholar] [CrossRef] [PubMed]
- Schnitzer, M.; Schöttl, S.E.; Kopp, M.; Barth, M. COVID-19 stay-at-home order in Tyrol, Austria: Sports and exercise behaviour in change? Public Health 2020, 185, 218–220. [Google Scholar] [CrossRef] [PubMed]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef] [PubMed]
- Mutz, M.; Gerke, M. Sport and exercise in times of self-quarantine: How Germans changed their behaviour at the beginning of the COVID-19 pandemic. Int. Rev. Sociol. Sport 2021, 56, 305–316. [Google Scholar] [CrossRef]
- Hargreaves, E.A.; Lee, C.; Jenkins, M.; Calverley, J.R.; Hodge, K.; Houge Mackenzie, S. Changes in physical activity pre-, during and post-lockdown COVID-19 restrictions in New Zealand and the explanatory role of daily hassles. Front. Psychol. 2021, 12, 642954. [Google Scholar] [CrossRef] [PubMed]
- Way, T.L.; Tarrant, S.M.; Balogh, Z.J. Social restrictions during COVID-19 and major trauma volume at a level 1 trauma centre. Med. J. Aust. 2021, 214, 38–39. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.; Mwagiru, D.; Thakur, I.; Moghadam, A.; Oh, T.; Hsu, J. Impact of societal restrictions and lockdown on trauma admissions during the COVID-19 pandemic: A single-centre cross-sectional observational study. ANZ J. Surg. 2020, 90, 2227–2231. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.; Ellis, D.Y.; Gorman, D.; Foo, N.; Haustead, D. Impact of COVID-19 social restrictions on trauma presentations in South Australia. Emerg. Med. Australas. 2021, 33, 152–154. [Google Scholar] [CrossRef] [PubMed]
- National Centre for Classification in Health. ICD-10-AM, 5th ed.; National Centre for Classification in Health: Sydney, Australia, 2006. [Google Scholar]
- Australian Bureau of Statistics. Census of Population and Housing: Socio-Economic Indexes for Areas (SEIFA), Australia, 2016; Catalogue no. 2033.0.55.001; Australian Bureau of Statistics: Canberra, Australia, 2016.
- Do, V.Q.; Ting, H.P.; Curtis, K.; Mitchell, R. Internal validation of models for predicting paediatric survival and trends in serious paediatric hospitalised injury in Australia. Injury 2020, 51, 1769–1776. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.; Ting, H.P. Survival Risk Ratios for ICD-10-AM Injury Diagnosis Classifications for Children [Dataset]. Available online: https://figshare.mq.edu.au/articles/dataset/Survival_risk_ratios_for_ICD-10-AM_injury_diagnosis_classifications_for_children/14852949/1 (accessed on 18 January 2023).
- Lystad, R.P.; Fyffe, A.; Orr, R.; Browne, G. Incidence, trends, and seasonality of paediatric injury-related emergency department presentations at a large level 1 paediatric trauma centre in Australia. Trauma Care 2022, 2, 408–417. [Google Scholar] [CrossRef]
- Hyndman, R.J.; Athanasopoulos, G. Forecasting: Principles and Practice, 3rd ed.; OTexts: Melbourne, Australia, 2018. [Google Scholar]
- Hyndman, R.; Athanasopoulos, G.; Bergmeir, C.; Caceres, G.; Chhay, L.; O’Hara-Wild, M.; Petropoulos, F.; Razbash, S.; Wang, E.; Yasmeen, F. Forecasting Functions for Time Series and Linear Models, Version 8.18. 2022. Available online: https://pkg.robjhyndman.com/forecast/ (accessed on 1 January 2023).
- Antonini, M.; Hinwood, M.; Paolucci, F.; Balogh, Z.J. The epidemiology of major trauma during the first wave of COVID-19 movement restriction policies: A systematic review and meta-analysis of observational studies. World J. Surg. 2022, 46, 2045–2060. [Google Scholar] [CrossRef] [PubMed]
- Mofijur, M.; Fattah, I.M.R.; Alam, M.A.; Islam, A.S.; Ong, H.C.; Rahman, S.A.; Najafi, G.; Ahmed, S.F.; Uddin, M.A.; Mahlia, T.M. Impact of COVID-19 on the social, economic, environmental and energy domains: Lessons learnt from a global pandemic. Sustain. Prod. Consum. 2021, 26, 343–359. [Google Scholar] [CrossRef] [PubMed]
- Kontopantelis, E.; Doran, T.; Springate, D.A.; Buchan, I.; Reeves, D. Regression based quasi-experimental approach when randomisation is not an option: Interrupted time series analysis. BMJ 2015, 350, h2750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hudson, J.; Fielding, S.; Ramsay, C.R. Methodology and reporting characteristics of studies using interrupted time series design in healthcare. BMC Med. Res. Methodol. 2019, 19, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, S.L.; Karahalios, A.; Forbes, A.B.; Taljaard, M.; Grimshaw, J.M.; Cheng, A.C.; Bero, L.; McKenzie, J.E. Design characteristics and statistical methods used in interrupted time series studies evaluating public health interventions: A review. J. Clin. Epidemiol. 2020, 122, 1–11. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Forecasted and observed monthly incidence of paediatric injury-related ED presentations, 1 January 2020 to 31 December 2021. Forecasted values are presented with 95% prediction interval (dark grey area).
Figure 1.
Forecasted and observed monthly incidence of paediatric injury-related ED presentations, 1 January 2020 to 31 December 2021. Forecasted values are presented with 95% prediction interval (dark grey area).

Figure 2.
Forecasted and observed monthly incidence of minor (A), moderate (B), and serious (C) paediatric injury-related ED presentations, 1 January 2020 to 31 December 2021. Forecasted values are presented with 95% prediction interval (dark grey area).
Figure 2.
Forecasted and observed monthly incidence of minor (A), moderate (B), and serious (C) paediatric injury-related ED presentations, 1 January 2020 to 31 December 2021. Forecasted values are presented with 95% prediction interval (dark grey area).



{kind=link}
{kind=link}
{kind=link}
Table 1.
Characteristics of paediatric injury-related ED presentations, 1 January 2020 to 31 December 2021.
Table 1.
Characteristics of paediatric injury-related ED presentations, 1 January 2020 to 31 December 2021.
| Characteristic | 2020 N (%) | 2021 N (%) |
|---|---|---|
| Sex | ||
| Male | 8132 (60.2) | 8259 (59.5) |
| Female | 5375 (39.8) | 5629 (40.5) |
| Age group | ||
| 0 years | 817 (6.0) | 1047 (7.5%) |
| 1–5 years | 6001 (44.4) | 6389 (46.0) |
| 6–10 years | 3431 (25.4) | 3425 (24.7) |
| 11–15 years | 3258 (24.1) | 3027 (21.8) |
| Socioeconomic disadvantage 1 | ||
| 1 (most disadvantaged) | 3242 (24.3) | 3073 (22.4) |
| 2 | 892 (6.7) | 969 (7.1) |
| 3 | 1864 (14.0) | 1934 (14.1) |
| 4 | 3084 (23.2) | 3225 (23.5) |
| 5 (least disadvantaged) | 4234 (31.8) | 4498 (32.8) |
| Mode of arrival | ||
| Private car | 11,758 (87.1) | 12,017 (86.5) |
| Ambulance | 1667 (12.3) | 1833 (13.2) |
| Other | 82 (0.6) | 38 (0.3) |
| Triage category | ||
| Less urgent condition | 293 (2.2) | 184 (1.3) |
| Potentially serious condition | 9689 (71.7) | 10,566 (76.1) |
| Potentially life-threatening condition | 2556 (18.9) | 2441 (17.6) |
| Imminently life-threatening condition | 727 (5.4) | 531 (3.8) |
| Immediately life-threatening condition | 242 (1.8) | 166 (1.2) |
| Injury severity | ||
| Minor (ICISS > 0.99) 2 | 11,516 (85.3) | 12,013 (86.5) |
| Moderate (ICISS 0.98–0.99) 2 | 1768 (13.1) | 1688 (12.1) |
| Serious (ICISS < 0.98) 2 | 223 (1.7) | 187 (1.3) |
| Departure status | ||
| Discharged | 10,753 (79.6) | 10,724 (77.2) |
| Admitted | 2411 (17.9) | 2732 (19.7) |
| Departed | 317 (2.3) | 407 (2.9) |
| Transferred | 25 (0.2) | 25 (0.2) |
| Died | 1 (0.0) | 0 (0.0) |
1 Socioeconomic status was missing for n = 192 children in 2020 and n = 189 children in 2021. 2 ICISS: International Classification of Injury Severity Score.
Table 2.
Frequencies and proportions of paediatric injury-related ED presentations, 1 January 2020 to 31 December 2021.
Table 2.
Frequencies and proportions of paediatric injury-related ED presentations, 1 January 2020 to 31 December 2021.
| Diagnosis | 2020 N (%) | 2021 N (%) |
|---|---|---|
| Injuries to the head (S00–S09) | 3640 (26.9) | 3877 (27.9) |
| Injuries to the neck (S10–S19) | 60 (0.4) | 48 (0.3) |
| Injuries to the thorax (S20–S29) | 27 (0.2) | 29 (0.2) |
| Injuries to the abdomen, lower back, lumbar spine and pelvis (S30–S39) | 148 (1.1) | 153 (1.1) |
| Injuries to the shoulder and upper arm (S40–S49) | 803 (5.9) | 815 (5.9) |
| Injuries to the elbow and forearm (S50–S59) | 2103 (15.6) | 2127 (15.3) |
| Injuries to the wrist and hand (S60–S69) | 1581 (11.7) | 1375 (9.9) |
| Injuries to the hip and thigh (S70–S79) | 162 (1.2) | 140 (1.0) |
| Injuries to the knee and lower leg (S80–S89) | 701 (5.2) | 688 (5.0) |
| Injuries to the ankle and foot (S90–S99) | 817 (6.0) | 878 (6.3) |
| Injuries involving multiple body regions (T00–T07) | 47 (0.3) | 47 (0.3) |
| Injuries to unspecified part of trunk, limb or body region (T08–T14) | 1594 (11.8) | 1524 (11.0) |
| Effects of foreign body entering through natural orifice (T15–T19) | 699 (5.2) | 768 (5.5) |
| Burns (T20–T32) | 416 (3.1) | 255 (1.8) |
| Poisoning by drugs, medicaments, and biological substances (T36–T50) | 57 (0.4) | 64 (0.5) |
| Toxic effects of substances chiefly nonmedicinal as to source (T51–T65) | 58 (0.4) | 68 (0.5) |
| Other and unspecified effects of external causes (T66–T78) | 113 (0.8) | 651 (4.7) |
| Certain early complications of trauma (T79) | 42 (0.3) | 41 (0.3) |
| Complications of surgical and medical care (T80–T89) | 439 (3.3) | 340 (2.4) |
Table 3.
Forecasted and observed monthly incidence of paediatric injury-related ED presentations, 1 January 2020 to 31 December 2021.
Table 3.
Forecasted and observed monthly incidence of paediatric injury-related ED presentations, 1 January 2020 to 31 December 2021.
| Month | Forecasted (95% PI) | Observed | Absolute Difference | Relative Difference |
|---|---|---|---|---|
| 2020 | ||||
| January | 1242 (1127–1356) | 1164 | −78 | −6.7% |
| February | 1181 (1056–1307) | 1076 | −105 | −9.8% |
| March | 1348 (1220–1477) | 1046 | −302 | −28.9% |
| April | 1267 (1136–1398) | 876 | −391 | −44.7% |
| May | 1343 (1210–1476) | 893 | −450 | −50.4% |
| June | 1150 (1015–1285) | 1043 | −107 | −10.3% |
| July | 1171 (1034–1308) | 1057 | −114 | −10.8% |
| August | 1230 (1092–1369) | 1222 | −8 | −0.7% |
| September | 1188 (1048–1328) | 1345 | 157 | 11.7% |
| October | 1313 (1173–1454) | 1303 | −10 | −0.8% |
| November | 1338 (1197–1480) | 1249 | −89 | −7.2% |
| December | 1358 (1216–1501) | 1233 | −125 | −10.2% |
| 2021 | ||||
| January | 1278 (1131–1424) | 1225 | −53 | −4.3% |
| February | 1209 (1060–1357) | 1156 | −55 | −4.7% |
| March | 1376 (1226–1525) | 1360 | −16 | −1.2% |
| April | 1294 (1144–1445) | 1289 | −5 | −0.4% |
| May | 1370 (1219–1521) | 1313 | −57 | −4.4% |
| June | 1177 (1026–1329) | 1140 | −37 | −3.2% |
| July | 1198 (1046–1351) | 912 | −286 | −31.4% |
| August | 1257 (1105–1410) | 884 | −373 | −42.2% |
| September | 1215 (1062–1368) | 940 | −275 | 29.3% |
| October | 1340 (1187–1494) | 1144 | −196 | −17.2% |
| November | 1365 (1211–1519) | 1226 | −139 | −11.4% |
| December | 1385 (1231–1539) | 1301 | −84 | −6.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lystad, R.P.; Fyffe, A.; Orr, R.; Browne, G. Changes in Paediatric Injury-Related Emergency Department Presentations during the COVID-19 Pandemic. Trauma Care 2023, 3, 46-54. https://doi.org/10.3390/traumacare3020006
AMA Style
Lystad RP, Fyffe A, Orr R, Browne G. Changes in Paediatric Injury-Related Emergency Department Presentations during the COVID-19 Pandemic. Trauma Care. 2023; 3(2):46-54. https://doi.org/10.3390/traumacare3020006
Chicago/Turabian StyleLystad, Reidar P., Andrew Fyffe, Rhonda Orr, and Gary Browne. 2023. "Changes in Paediatric Injury-Related Emergency Department Presentations during the COVID-19 Pandemic" Trauma Care 3, no. 2: 46-54. https://doi.org/10.3390/traumacare3020006