
Trends in State Anxiety during the Full Lockdown in Italy: The Role Played by COVID-19 Risk Perception and Trait Emotional Intelligence


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants Recruitment
2.2. Measures
2.3. Data Analysis
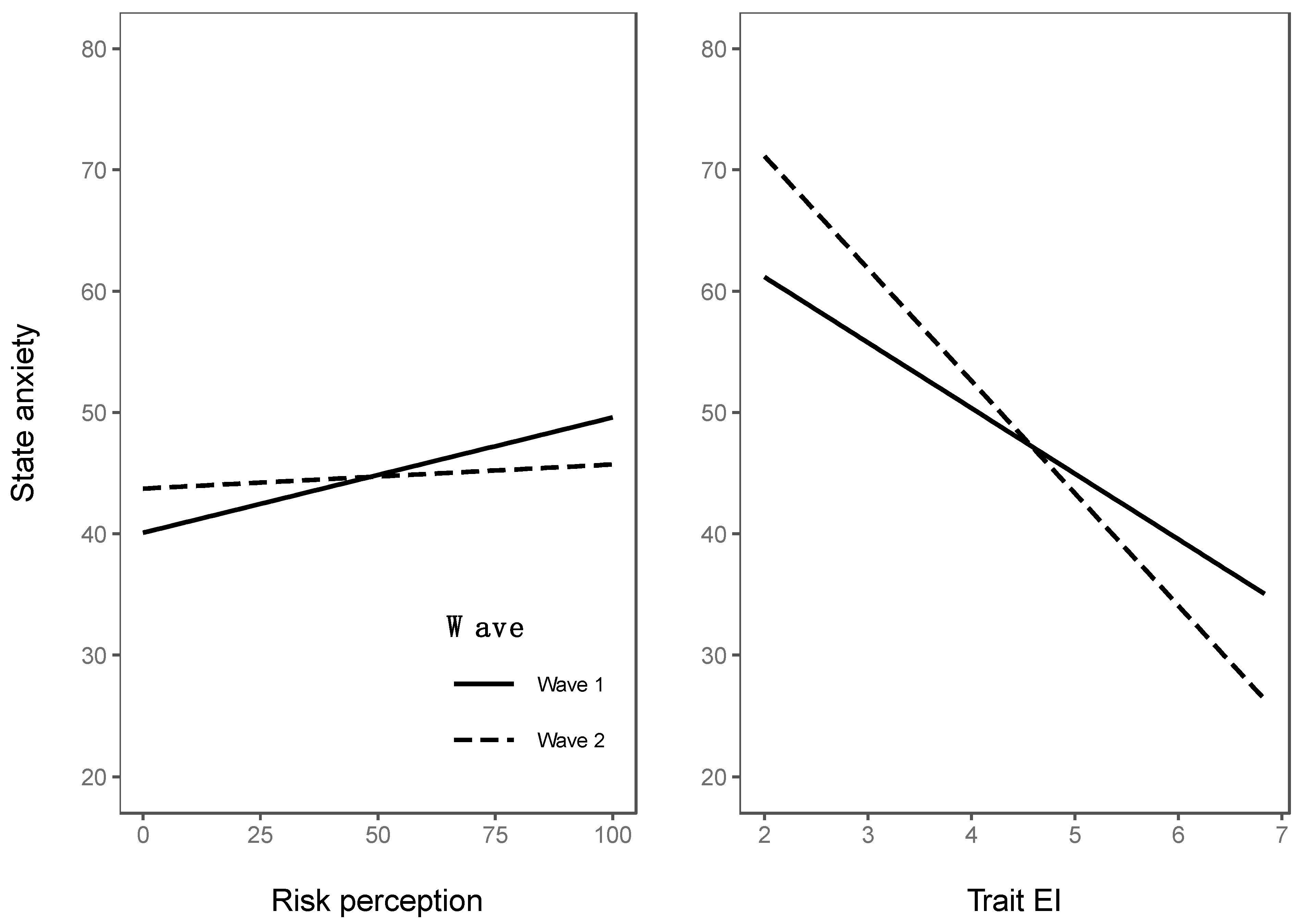
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Governo Italiano Presidenza del Consiglio dei Ministri, 2020. Decreto Del Presidente Del Consiglio Dei Ministri 8 Marzo 2020. Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/08/20A01522/sgDECRETO%20DEL%20PRESIDENTE%20DEL%20CONSIGLIO%20DEI%20MINISTRI%208%20marzo%202020 (accessed on 14 March 2020).
- Balaratnasingam, S.; Janca, A. Mass hysteria revisited. Curr. Opin. Psychiatr. 2006, 19, 171–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slovic, P. Perception of risk. Science 1987, 236, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Greco, V.; Roger, D. Uncertainty, stress, and health. Pers. Individ. Differ. 2003, 34, 1057–1068. [Google Scholar] [CrossRef]
- Reuman, L.; Jacoby, R.J.; Fabricant, L.E.; Herring, B.; Abramowitz, J.S. Uncertainty as an anxiety cue at high and low levels of threat. J. Behav.Ther. Exp. Psy. 2015, 47, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: Immediate psychological responses and associated factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- Moccia, L.; Janiri, D.; Pepe, M.; Dattoli, L.; Molinaro, M.; de Martin, V.; Chieffo, D.; Janiri, L.; Fiorillo, A.; Sani, G.; et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: An early report on the Italian general population. Brain Behav. Immun. 2020, 87, 75–79. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; di Marco, A.; Rossi, A.; Siracusano, A.; di Lorenzo, G. COVID-19 pandemic and lockdown measures impact on mental health among the general population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Rubaltelli, E.; Tedaldi, E.; Orabona, N.; Scrimin, S. Environmental and psychological variables influencing reactions to the COVID-19 outbreak. Br. J. Health Psychol. 2020, 25, 1020–1038. [Google Scholar] [CrossRef]
- Bonanno, G.A. Loss, trauma and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events? Am. Psychol. 2004, 59, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Troy, A.S.; Mauss, I.B. Resilience in the face of stress: Emotion regulation as a protective factor. In Resilience and Mental Health: Challenges Across the Lifespan; Southwick, S.M., Litz, B.T., Charney, D., Friedman, M.J., Eds.; Cambridge University Press: Cambridge, UK, 2011; pp. 30–44. [Google Scholar] [CrossRef] [Green Version]
- Masten, A.S.; Obradovic, J. Disaster preparation and recovery: Lessons from research on resilience in human development. Ecol. Soc. 2008, 13, 9–36. Available online: https://www.ecologyandsociety.org/vol13/iss1/art9/ (accessed on 25 February 2022). [CrossRef] [Green Version]
- Gross, J.J.; Muñoz, R.F. Emotion regulation and mental health. Clin. Psychol. Sci. Pr. 1995, 2, 151–164. [Google Scholar] [CrossRef]
- Thompson, R.A. Emotion regulation: A theme in search of definition. Monogr. Soc. Res. Child Dev. 1994, 59, 25–52. [Google Scholar] [CrossRef] [PubMed]
- Ciarrochi, J.; Deane, F.P.; Anderson, S. Emotional intelligence moderates the relationship between stress and mental health. Pers. Indiv. Differ. 2002, 32, 197–209. [Google Scholar] [CrossRef]
- Gross, J.J.; Jazaieri, H. Emotion, emotion regulation, and psychopathology: An affective science perspective. Clin. Psychol. Sci. 2014, 2, 387–401. [Google Scholar] [CrossRef]
- Peña-Sarrionandia, A.; Mikolajczak, M.; Gross, J.J. Integrating emotion regulation and emotional intelligence traditions: A meta-analysis. Front. Psychol. 2015, 6, 160. [Google Scholar] [CrossRef] [Green Version]
- Gross, J.J. Emotion regulation: Current status and future prospects. Psychol. Inq. 2015, 26, 1–26. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S. Specificity of cognitive emotion regulation strategies: A transdiagnostic examination. Behav. Res. Ther. 2010, 48, 974–983. [Google Scholar] [CrossRef]
- Khakpoor, S.; Saed, O.; Kian, A.A. Emotion regulation as the mediator of reductions in anxiety and depression in the Unified Protocol (UP) for transdiagnostic treatment of emotional disorders: Double-blind randomized clinical trial. Trends Psychiatry Psychother. 2019, 41, 227–236. [Google Scholar] [CrossRef]
- Bhullar, N.; Schutte, N.; Malouff, J.M. The nature of well-being: The roles of hedonic and eudaimonic processes and trait emotional intelligence. J. Psychol. 2013, 147, 1–16. [Google Scholar] [CrossRef]
- Schutte, N.S.; Malouff, J.M.; Thorsteinsson, E.B.; Bhullar, N.; Rooke, S.E. A meta-analytic investigation of the relationship between emotional intelligence and health. Pers. Individ. Differ. 2007, 42, 921–933. [Google Scholar] [CrossRef]
- Moroń, M.; Biolik-Moroń, M. Trait emotional intelligence and emotional experiences during the COVID-19 pandemic outbreak in Poland: A daily diary study. Pers. Individ. Differ. 2021, 168, 110348. [Google Scholar] [CrossRef] [PubMed]
- Persich, M.R.; Smith, R.; Cloonan, S.A.; Woods-Lubbert, R.; Strong, M.; Killgore, W.D. Emotional intelligence training as a protective factor for mental health during the COVID-19 pandemic. Depress. Anxiety 2021, 38, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Wang, S.; Wang, W.; Han, G.; Liu, Z.; Wu, Q.; Pang, X. Correlation between emotional intelligence and negative emotions of front-line nurses during the COVID-19 epidemic: A cross sectional study. J. Clin. Nurs. 2021, 30, 385–396. [Google Scholar] [CrossRef]
- Speilberger, C.D.; Gorsuch, R.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory STAI (Form Y); Consulting Psychology Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Petrides, K.V. Psychometric properties of the trait emotional intelligence questionnaire (TEIQue). In Advances in the Assessment of Emotional Intelligence; Stough, C., Saklofske, D.H., Parker, J.D., Eds.; Springer: Boston, MA, USA, 2009; pp. 85–101. [Google Scholar] [CrossRef]
- Our World in Data. Available online: https://ourworldindata.org/explorers/coronavirus-data-explorer?tab=table;zoomToSelection=true;time=2020-03-01..latest;facet=none;pickerSort=asc;pickerMetric=location;Metric=Confirmed+cases;Interval=7-day+rolling+average;Relative+to+Population=true;Color+by+test+positivity=false;country=~ITA (accessed on 4 June 2020).
- Akaike, H. Maximum likelihood identification of Gaussian autoregressive moving average models. Biometrika 1973, 60, 255–265. [Google Scholar] [CrossRef]
- Burnham, K.P.; Anderson, D.R.; Huyvaert, K.P. AIC model selection and multimodel inference in behavioral ecology: Some background, observations, and comparisons. Behav. Ecol. Sociobiol. 2011, 65, 23–35. [Google Scholar] [CrossRef]
- Slovic, P.; Weber, E. Perception of Risk Posed by Extreme Events. Regulation of Toxic Substances and Hazardous Waste; Applegate, G., Laitos, S., Eds.; Foundation Press: Palisades, NY, USA, 2002. [Google Scholar]
- Olff, M.; Primasari, I.; Qing, Y.; Coimbra, B.M.; Hovnanyan, A.; Grace, E.; Consortium, T.G.C. Mental health responses to COVID-19 around the world. Eur. J. Psychotraumatology 2021, 12, 1929754. [Google Scholar] [CrossRef]
- Gloster, A.T.; Lamnisos, D.; Lubenko, J.; Presti, G.; Squatrito, V.; Constantinou, M.; Nicolaou, C.; Papacostas, S.; Aydın, G.; Chong, Y.Y.; et al. Impact of COVID-19 pandemic on mental health: An international study. PLoS ONE 2020, 15, e0244809. [Google Scholar] [CrossRef]
- Muro, A.; Feliu-Soler, A.; Castellà, J. Psychological impact of COVID-19 lockdowns among adult women: The predictive role of individual differences and lockdown duration. Women Health 2021, 61, 668–679. [Google Scholar] [CrossRef]
- Martelletti, C.P.; Santirocchi, A.; Spataro, P.; Rossi-Arnaud, C.; Löfstedt, R.E.; Cestari, V. Predictors of COVID-19 risk perception, worry and anxiety in Italy at the end of the 2020 national lockdown. J. Risk. Res. 2022. [Google Scholar] [CrossRef]
- Clayton, S. Climate anxiety: Psychological responses to climate change. J. Anxiety Disord. 2020, 74, 102263. [Google Scholar] [CrossRef]
- Sampaio, F.; Sequeira, C. Climate anxiety: Trigger or threat for mental disorders? Lancet Planet. Health 2022, 6, e89. [Google Scholar] [CrossRef]
- Kotsou, I.; Nelis, D.; Grégoire, J.; Mikolajczak, M. Emotional plasticity: Conditions and effects of improving emotional competence in adulthood. J. Appl. Psychol. 2011, 96, 827–839. [Google Scholar] [CrossRef] [PubMed]
- Kotsou, I.; Mikolajczak, M.; Heeren, A.; Grégoire, J.; Leys, C. Improving emotional intelligence: A systematic review of existing work and future challenges. Emot. Rev. 2019, 11, 151–165. [Google Scholar] [CrossRef]
- Slovic, P.; Finucane, M.L.; Peters, E.; MacGregor, D.G. Risk as analysis and risk as feelings: Some thoughts about affect, reason, risk, and rationality. Risk. Anal. 2004, 24, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Lawton, R.; Conner, M.; McEachan, R. McEachan Desire or reason: Predicting health behaviors from affective and cognitive attitudes. Health Psychol. 2009, 28, 56–65. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Wave 1 (N = 1031) | Wave 2 (N = 700) | Difference |
|---|---|---|---|
| Age, y (range) | 30.63 (18–75) | 30.97 (18–75) | t = −0.528 |
| Gender | X2 = 2.11 | ||
| Female, no. (%) | 701 (67.99%) | 492 (69.98%) | |
| Highest level of education | t = −1.654 | ||
| Primary school, no. (%) | 1 (0.09%) | 0 (0%) | |
| Middle school, no. (%) | 50 (4.85%) | 23 (3.27%) | |
| High school, no. (%) | 460 (44.62%) | 306 (43.53%) | |
| Bachelor’s degree, no. (%) | 303 (29.39%) | 213 (30.30%) | |
| Master’s degree, no. (%) | 187 (18.14%) | 133 (18.92%) | |
| Specialization/Doctorate, no. (%) | 30 (2.91%) | 28 (3.98%) | |
| Income | t = 0.143 | ||
| >10,000 (%) | 65 (6.30%) | 37 (5.26%) | |
| 10,000–19,999 (%) | 190 (18.43%) | 124 (17.64%) | |
| 20,000–29,999 (%) | 9 (0.87%) | 7 (1%) | |
| 30,000–39,999 (%) | 260 (25.22%) | 172 (24.47%) | |
| 40,000–49,999 (%) | 153 (14.84%) | 114 (16.22%) | |
| 50,000–59,999 (%) | 93 (9.02%) | 63 (8.96%) | |
| 60,000–69,999 (%) | 50 (4.85%) | 39 (5.55%) | |
| 70,000–79,999 (%) | 29 (2.81%) | 23 (3.27%) | |
| 80,000–89,999 (%) | 27 (2.62%) | 25 (3.56%) | |
| 90,000–99,999 (%) | 17 (1.65%) | 5 (0.71%) | |
| 100,000–109,999 (%) | 3 (0.29%) | 6 (0.85%) | |
| 110,000–119,999 (%) | 7 (0.68%) | 13 (1.85%) | |
| 120,000–129,999 (%) | 3 (0.29%) | 2 (0.28%) | |
| 130,000–139,999 (%) | 3 (0.29%) | 1 (0.14%) | |
| 140,000–149,999 (%) | 0 (0%) | 0 (0%) | |
| >150,000 (%) | 1 (0.10%) | 2 (0.28%) | |
| Prefer not to say (%) | 121 (11.74%) | 70 (9.96%) | |
| Political orientation | t = −1.05 | ||
| Extreme left wing, no. (%) | 26 (2.52%) | 19 (2.70%) | |
| Left wing, no. (%) | 285 (27.64%) | 176 (25%) | |
| Center-left wing, no. (%) | 335 (32.50%) | 230 (32.72%) | |
| Center wing, no. (%) | 152 (14.74%) | 103 (14.65%) | |
| Center-left wing, no. (%) | 142 (13.77%) | 107 (15.2%) | |
| left wing, no. (%) | 85 (8.25%) | 58 (8.25%) | |
| Extreme left wing, no. (%) | 6 (0.58%) | 7 (1%) | |
| Religiosity, 1–7 scale (SD) | 2.944 (1.824) | 2.95 (1.791) | t = −0.152 |
| Trust authorities, 1–7 scale (SD) | 4.250 (1.357) | 4.124 (1.378) | t = 4.668 *** |
| Descriptive Statistics | |||||||||
| Wave 1 | Wave 2 | ||||||||
| Mean | SD | Range | Mean | SD | Range | t | d | 95% C.I. | |
| State anxiety | 46.06 | 13.82 | 20–75 | 45.59 | 14.32 | 20–80 | 0.68 | 0.03 | [−0.06, 0.13] |
| Trait EI | 4.88 | 0.75 | 2.13–6.83 | 4.75 | 0.76 | 2–6.77 | 3.66 *** | 0.18 | [0.08, 0.28] |
| Risk perception | 66.33 | 23.66 | 0–100 | 53.11 | 23.88 | 0–100 | 11.37 *** | 0.56 | [0.46, 0.65] |
| Cases per million | 211.2 | 85.52 | 122–521.1 | 16.79 | 3.43 | 7.88–21.12 | 60.1 *** | 2.94 | [2.81, 3.08] |
| Correlations | |||||||||
| Wave 2 | |||||||||
| State anxiety | Trait EI | Risk perception | Cases million | ||||||
| Wave 1 | State anxiety | --- | −0.51 *** | 0.13 *** | −0.10 ** | ||||
| Trait EI | −0.30 *** | --- | −0.15 *** | 0.11 ** | |||||
| Risk perception | 0.18 *** | −0.04 | --- | −0.06 | |||||
| Cases per million | −0.03 | −0.02 | 0.13 *** | --- | |||||
| β | B | SE | t | 95% C.I. | |
|---|---|---|---|---|---|
| Trait EI | −0.29 | −5.40 | 0.52 | −10.33 *** | [−6.43, −4.38] |
| Wave | 0.78 | 22.27 | 4.35 | 5.12 *** | [13.74, 30.79] |
| Risk perception | 0.17 | 0.10 | 0.02 | 5.78 *** | [0.06, 0.13] |
| Age | −0.14 | −0.15 | 0.02 | −6.55 *** | [−0.19, −0.11] |
| Gender | −0.12 | −3.38 | 0.61 | −5.58 *** | [−4.57, −2.19] |
| Education | 0.09 | 1.40 | 0.33 | 4.20 *** | [0.75, 2.06] |
| Political orientation | −0.06 | −0.59 | 0.23 | −2.56 * | [−1.03, −0.14] |
| Wave x Risk perception | −0.16 | −0.08 | 0.03 | −2.92 ** | [−0.13, −0.03] |
| Wave x Trait EI | −0.66 | −3.86 | 0.81 | −4.77 *** | [−5.45, −2.27] |
| AdjR2 = 0.22, p < 0.001, AIC baseline = 8731.4; AIC model = 8722.52 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tedaldi, E.; Orabona, N.; Hovnanyan, A.; Rubaltelli, E.; Scrimin, S. Trends in State Anxiety during the Full Lockdown in Italy: The Role Played by COVID-19 Risk Perception and Trait Emotional Intelligence. Trauma Care 2022, 2, 418-426. https://doi.org/10.3390/traumacare2030034
Tedaldi E, Orabona N, Hovnanyan A, Rubaltelli E, Scrimin S. Trends in State Anxiety during the Full Lockdown in Italy: The Role Played by COVID-19 Risk Perception and Trait Emotional Intelligence. Trauma Care. 2022; 2(3):418-426. https://doi.org/10.3390/traumacare2030034
Chicago/Turabian StyleTedaldi, Elisa, Noemi Orabona, Ani Hovnanyan, Enrico Rubaltelli, and Sara Scrimin. 2022. "Trends in State Anxiety during the Full Lockdown in Italy: The Role Played by COVID-19 Risk Perception and Trait Emotional Intelligence" Trauma Care 2, no. 3: 418-426. https://doi.org/10.3390/traumacare2030034