
Gross Pathology in COVID-19

Department of Pathology and Laboratory Medicine, The Robert Larner, M.D. College of Medicine at University of Vermont, Burlington, VT 05405, USA
Encyclopedia 2022, 2(4), 1790-1802; https://doi.org/10.3390/encyclopedia2040123
Submission received: 12 August 2022
/
Revised: 25 October 2022
/
Accepted: 26 October 2022
/
Published: 28 October 2022
(This article belongs to the Collection Encyclopedia of COVID-19)
{kind=link}
{kind=link}
Definition
:The global infectious disease COVID-19 is caused by SARS-CoV-2, a new member of the Coronaviridae family. Though presented as a novel disease that primarily affects the respiratory system, multi-organ involvement has been well-noticed and documented since the beginning of the pandemic. When performed properly with adequate safety measures, autopsy provides the most valuable information to decipher the pathogenesis of this novel disease, therefore providing a basis for clinical management. In addition to reviewing the macroscopic changes in organs and tissues involved in COVID-19, the relevant microscopic alterations and possible pathogenesis are also discussed.
1. Introduction
Coronavirus disease (COVID-19), a novel seventh coronavirus disease, initially broke out in Wuhan, China, in December 2019 [1]. It quickly spread worldwide and became a pandemic, as declared by the World Health Organization in March 2020 [2]. As of Friday, 22 July 2022, more than 567 million have been affected, with more than 6.38 million deaths all over the world [3]. The unprecedented public health threat and the gravity of the situation have inevitably overwhelmed the healthcare system of many countries and created much turmoil and emerging challenges in many aspects of human life [4]. Social distancing has been used worldwide to limit the spread of the virus [5]. COVID-19 and its causative agent, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), have been studied extensively.
The Coronaviridae family viruses are enveloped, positive-sense, single-stranded RNA viruses [6]. Previously, six coronaviruses have been identified to cause human diseases. Two of them, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), can cause severe respiratory illness with fatality rates of 10% and 40%, respectively. In contrast, the other four usually cause mild upper respiratory diseases similar to the common flu [7,8].
SARS-CoV-2 is transmitted via inhalation or direct contact of the virus with the mucous membrane [9]. Like SARS-CoV, SARS-CoV-2 also binds to the angiotensin-converting enzyme 2 (ACE2) receptor primarily present on the surface of the alveolar epithelial cells in the lung, resulting in respiratory symptoms [7]. ACE2 is also found in the small intestinal epithelium, endothelial cells of blood vessels, alveolar macrophage and monocyte, and epithelial cells of trachea and bronchi, which may explain the multiple organ involvement in COVID-19 [7]. The virus contains four structural proteins: spike (S), envelope (E), membrane glycoprotein (M), and nucleocapsid phosphoprotein (N). The virus enters the cell via the interaction between the viral spike (S) protein and the host cell proteases, TMPRSS2 [10].
Like other coronaviruses, SARS-CoV-2 continuously develops mutations. Since the global outbreak, five major variants of concern (VOC) with increased transmissibility, varied virulence, evasion from therapeutic drugs, or decreased effectiveness of vaccines have been reported after the ancestral one. Those VOCs are alpha (B.1.1.7), beta (B.1.351), gamma (P.1), delta (B.1.617.2), and omicron (B.1.1.529) [11]. Selective pressures such as the use of monoclonal antibodies further drive the evolution of SARS-CoV-2, especially in immunocompromised patients [12].
Though often present as a mild disease with typical flu-like symptoms such as fever, cough, myalgia, or fatigue [13], about 19%, however, develop severe to critical disease that may result in progressive respiratory failure, presumably due to massive alveolar damage [5]. Deceased patients present with severe pneumonitis and advance to acute respiratory distress syndrome, often accompanied by multi-organ failure [14], which may be contributed by severe endothelial damage, disseminated intravascular coagulation, and a cytokine storm [15,16]. The severity and prognosis of the disease seem to be associated with age; gender; blood group A; cigarette smoking; obesity; and a variety of comorbidities, including coronary artery disease, diabetes mellitus, chronic kidney disease, hypertension, congestive heart failure, and chronic obstructive pulmonary disease [14,17]. Most fatal cases have significant underlying diseases, with systemic hypertension and diabetes mellitus being the most common [18]. Besides the comorbidities listed above, HIV infection and tuberculosis are common among COVID-19 decedents in Africa [19].
The complexity of COVID-19 has been made well aware of since its outbreak. It is a multiorgan disease that presents with a broad spectrum of clinical manifestations and a wide range of degrees of severity [13,14,20]. For example, autopsies have revealed the systemic multiorgan involvement of vessels in the lungs, heart, kidney, liver, GI tract, kidney, brain, and skin [21]. Gross examination of involved organs obtained from autopsy provides valuable information, which is imperative for elucidating the pathogenesis of COVID-19 and laying out the basis for clinical management.
2. COVID-19 Autopsy
The importance of autopsy in deciphering the pathogenesis of a novel disease such as COVID-19 is undisputable [22]. It is one of the primary ways to access organs to perform gross examinations.
Initially, autopsies on deceased COVID-19 patients were scarce due to significant concerns, such as the risk of contagiousness, lack of healthcare specialists, and the abrupt outbreak of the disease [23]. The autopsy of COVID-19 patients is limited mainly due to strict biosafety measures and infection control over specimen collection and handling. Because of this, there was a minimal number of publications on postmortem findings in COVID-19 [24,25].
SARS-CoV-2 presents particular hazards to the professionals working in the lab or clinical settings [26,27]. Exposure risk levels of autopsies and specimen handling from deceased COVID-19 patients are considered “very high” [28]. Therefore, implementing strict security measures to manage the diseased from COVID-19 is essential in protecting healthcare professionals and family members, decreasing the risk of exposure, and preventing infection expansion [29]. Based on previous guidelines for working with SARS-CoV and MERS-CoV, the WHO and the CDC released postmortem guidance regarding COVID-19 [30]. The College of American Pathologists (CAP) endorsed the postmortem guidance from the CDC about specimen collection and handling involving confirmed or suspected COVID-19 [31]. Such administrative support and biosafety guidelines have promoted autopsy in COVID-19, which helps tremendously in gaining better knowledge about this new and complex infectious disease. It is essential that each lab access the risk, follow the protocol, and abide by the rules for biosafety practice.
After obtaining informed consent from the patient’s next of kin, an autopsy of COVID-19 should be performed in an autopsy suite that is adequately equipped. The essentials include an appropriately functioning ventilation system capable of six complete air exchanges in an hour with negative pressure and HEPA filters [8,32]. Airborne Infection Isolation Rooms (AIIRs) are recommended by the CDC when conducting autopsies of COVID-19 patients [30]. The number of personnel in the autopsy room should be minimized, and aerosol formation should be avoided as much as possible. Essential personal protective equipment (PPE) includes a fluid-resistant gown and apron, double gloves with cut-proofing, a surgical cap, face shields or goggles, boots or overshoes, and an N95 respirator face mask or equivalent [29,33]. Whole-body suits with individual respirators are not necessary [27].
Before the autopsy investigation and during the external examination, nasopharyngeal and oropharyngeal swabs are collected for diagnostic or virological research [34]. Each involved organ system is explored by following standard operating procedures. For example, the “en bloc” extraction technique can be used to obtain the respiratory block, including the tongue, hypopharynx, larynx, trachea, bronchi, and lungs [34]. Intro-autopsy swabs can then be collected from the removed and opened respiratory block [34]. A thorough examination of the brain is performed by adopting the protocol for Creutzfeldt-Jakob Disease brain autopsies [35]. Representative tissue samples obtained from the involved organs are first fixed in formalin for 24–48 h or even 72 h to inactivate the virus and then processed for histology examination sectioning and examination [33,35,36]. A new set of tools are used for each organ to avoid cross-contamination. Diagnostic testing for COVID-19 is performed by real-time reverse transcriptase PCR using swabs taken from the trachea, lung parenchyma, pericardium, pleural cavity, etc. [33].
Though creating critical challenges in the autopsy as a novel infectious disease for many institutions and clinics, autopsies for COVID-19 can be performed routinely by adequately trained personnel who carefully adhere to the most updated safety guidelines. As the pandemic evolves, more and more postmortem examinations have been performed to elaborately study the macroscopic changes in the multiple organs affected by the virus, aiming to elucidate the pathogenesis of the disease and the exact cause of death.
Multiple autopsy clinics have established a new biobanking model with shared and centralized biomaterial and data management. Such established autopsy networks provide high-quality biosample collection, data analysis and reports to support disease-related research, health policymaking, and public discussion [37]. By promoting communication and collaboration across different institutions, autopsy and an accompanied centralized model of biobanking have significantly increased the systemic understanding of COVID-19, which set up a successful model for studying other infectious diseases as well [37].
When safety regulations are too stringent to meet or the fear of contraction is too big to overcome, postmortem biopsies can be an acceptable and reasonable alternative, providing significant histopathological findings [38].
3. Pulmonary Findings in COVID-19
The respiratory tract is the primary target of SARS-CoV-2, with acute respiratory distress syndrome (ARDS) being the most common cause of death [18].
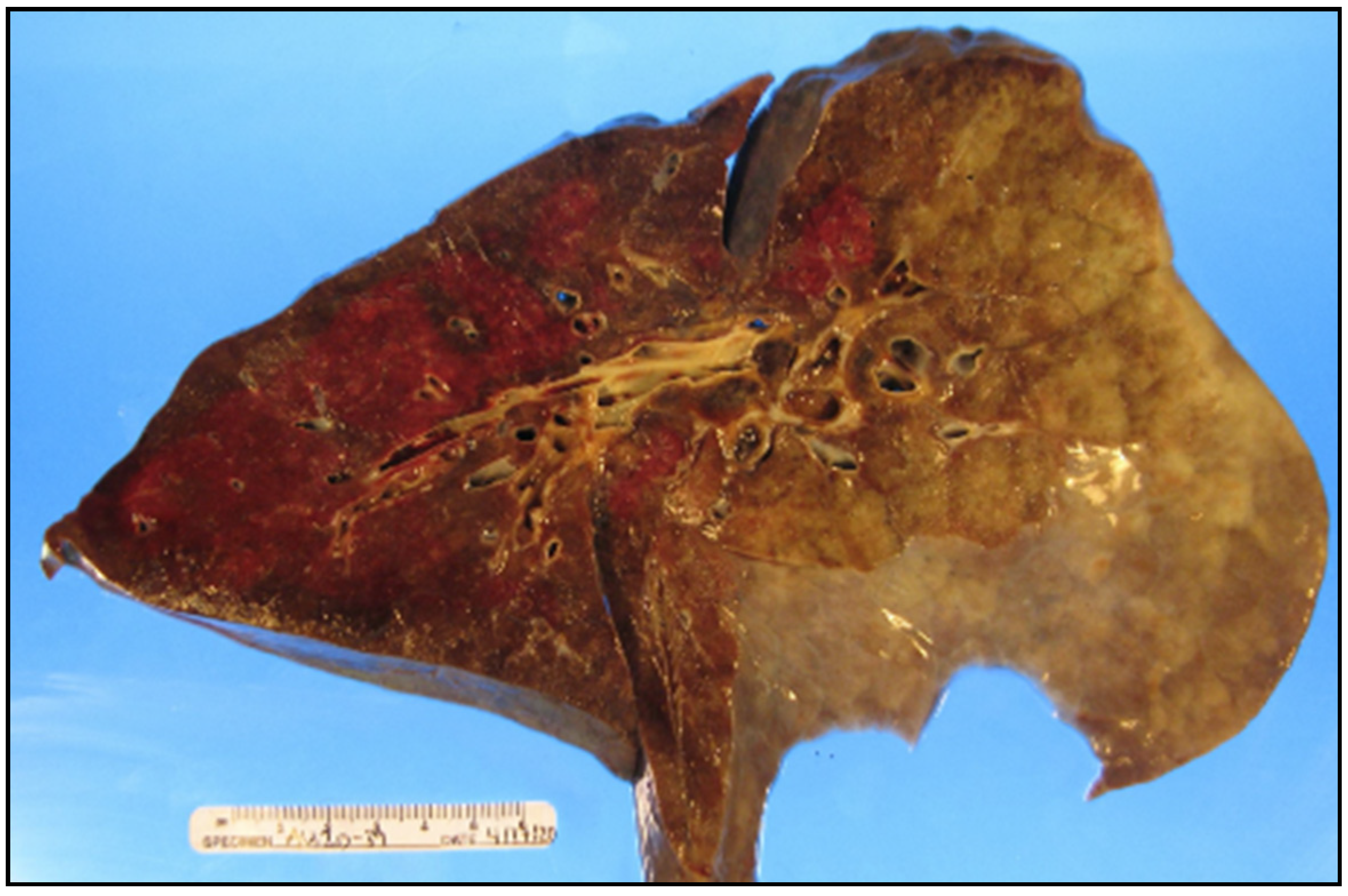
In general and grossly, the lungs are heavier due to edema, congestion is notable, and consolidation or hemorrhage may or may not be present (Figure 1). Microscopically, it is featured as diffuse alveolar damage (DAD) of the acute or organizing phases or a mixture of both [18]. ARDS/DAD has been the number one immediate cause of death in COVID-19, followed by multi-organ failure and bacterial pulmonary superinfection [39]. The pathological changes in the lung are varied depending on the stages and duration of the disease and the severity of the pulmonary damage.
Significant generalized pulmonary edema can be present at the early stage. The lungs weigh heavier than usual. Consistency of the lower lobes is slightly increased, with capillary endotheliitis infiltrated by neutrophils. Microthrombi formation in alveolar capillaries and small pulmonary vessels are seen microscopically. Inflammatory exudates with neutrophils, multinucleated giant cells, and scanty hyaline membranes are observed as well, but no focal changes are macroscopically visible, except the cutting surface is slightly sticky [36].
As the disease progresses, pulmonary edema becomes more remarkable, and consolidation occurs at both lower lobes. Thrombi are visible in small to medium-sized pulmonary arteries and veins at the cutting surface. The affected part changes color to dark red and is consolidated without air, suggesting lobar pneumonia [33]. Focal changes around thrombi include hemorrhage (petechial), consolidation, and fresh infarction indicated by discoloration. Accompanied histological changes demonstrate diffuse alveolar damage with fibrin deposition, fibromyxoid exudates, hyaline membrane, and an increased number of macrophages within the alveoli [33,36].
Consolidation expands to the upper and lower lobes of the lungs as the disease progresses. Both the size and the weight of the lungs increase significantly. The accompanied histological changes are consistent with prolonged ARDS featured by extensive epithelium hyperplasia and focal squamous metaplasia. Concentrically arranged fibroblasts and central accumulation of inflammatory cells inside the alveoli are seen at the organizing stage [36]. Hyperplasia and shedding of type II pneumocytes are quite notable [33].
Without medical treatment, the onset of severe acute lung injury can be very rapid, with all lobes affected equally. The cross-section reveals edema, diffused firm, and rubbery parenchyma without any mass. The parenchyma is colored from pale pink to dark with scattered hemorrhagic areas that are not well-defined. The bronchi are filled with frothy proteinaceous exudates. The corresponding microscopic findings are consistent with the early exudative phase of acute lung injury featured by hyaline membrane formation and hyperplasia of type II pneumocytes with atypical changes [40]. Lymphocytic infiltration is consistent with viral pneumonia [33].
The pleural is slightly thickened with decreased effusion [41]. Purulent sputum and pleural effusion with turbid fluid can be seen in the pleural cavity. Fibrinous exudate can be found over the visceral pleura in some cases [33].
Neither redness nor erosion is seen at the trachea and bronchi, but reactive and atypical epithelium changes are observed microscopically [40]. Frothy secretions of gray-white colored viscous fluid are prevalent in the airways, including the larynx, with or without mucous plugging [40,42]. Superimposed bronchopneumonia can present due to bacterial or fungal infection and has been found in a significant number of cases that are most likely bacterial-related [43,44]. It can be focal or diffused. Tracheitis has been reported [45]. Such findings are not surprising considering the expression of ACE-2 receptors at the upper respiratory tract [46].
4. Cardiovascular Findings in COVID-19
Cardiovascular co-morbidities are common in COVID-19 [48]. The multiple cardiovascular complications worsened or induced by SARS-CoV-2 include myocardial infarction (MI), myocarditis, acute coronary syndromes, arrhythmias, heart failure, cardiogenic shock, and sudden cardiac death [49]. Myocardial injury indicated by an increased level of troponin I is a common finding in COVID-19 patients [50,51]. A significant number of deaths are attributed to heart failure induced by COVID-19 without previous cardiovascular disease history [52]. The diversified cardiovascular consequences are caused by infiltration of inflammatory cells due to viral attack, the release of a large variety of pro-inflammatory cytokines, and micro-thrombosis due to endothelial damage [50]. Hypoxia caused by ARDS also contributes significantly to heart failure [14].
The gross weight of the infected heart can be normal but is mostly increased due to hypertrophy, edema, and chamber dilation [53,54]. The thickness of the myocardial wall is usually normal or slightly below normal [53]. The myocardium can have a firm texture and shows a red-brown color [47,55]. Intracardiac and coronary thrombosis is the most petrifying finding, with thrombin rich in platelets, fibrin, and neutrophil extracellular traps found in the chambers, coronary arteries, or veins [53,56]. In general, the three primary gross pathological findings are myocardial ischemia, thrombosis, and cardiac dilation, especially at the right heart [53]. Myocardial fibrosis, the end stage of cardiac injury, is found in about 25% of cases [53]. Senile amyloidosis is found in some cases [45]. The virus has been detected in the myocardium in about half of the cases without necessarily all resulting in myocarditis [51]. Myocarditis is much less frequently reported than expected, which turns out to be a rare sequela of certain cohort studies [18]. Pericardial effusion has been found in some COVID-19 patients who died from cardiogenic shock. Pericarditis has also been reported [57]. It is important to note that many postmortem findings in the hearts of COVID-19 patients are consequences of pre-existing chronic conditions. In the absence of ARDS/DAD or COVID-19 pneumonia, SARS-CoV-2 is most likely a contributing rather than a direct cause of death [18].
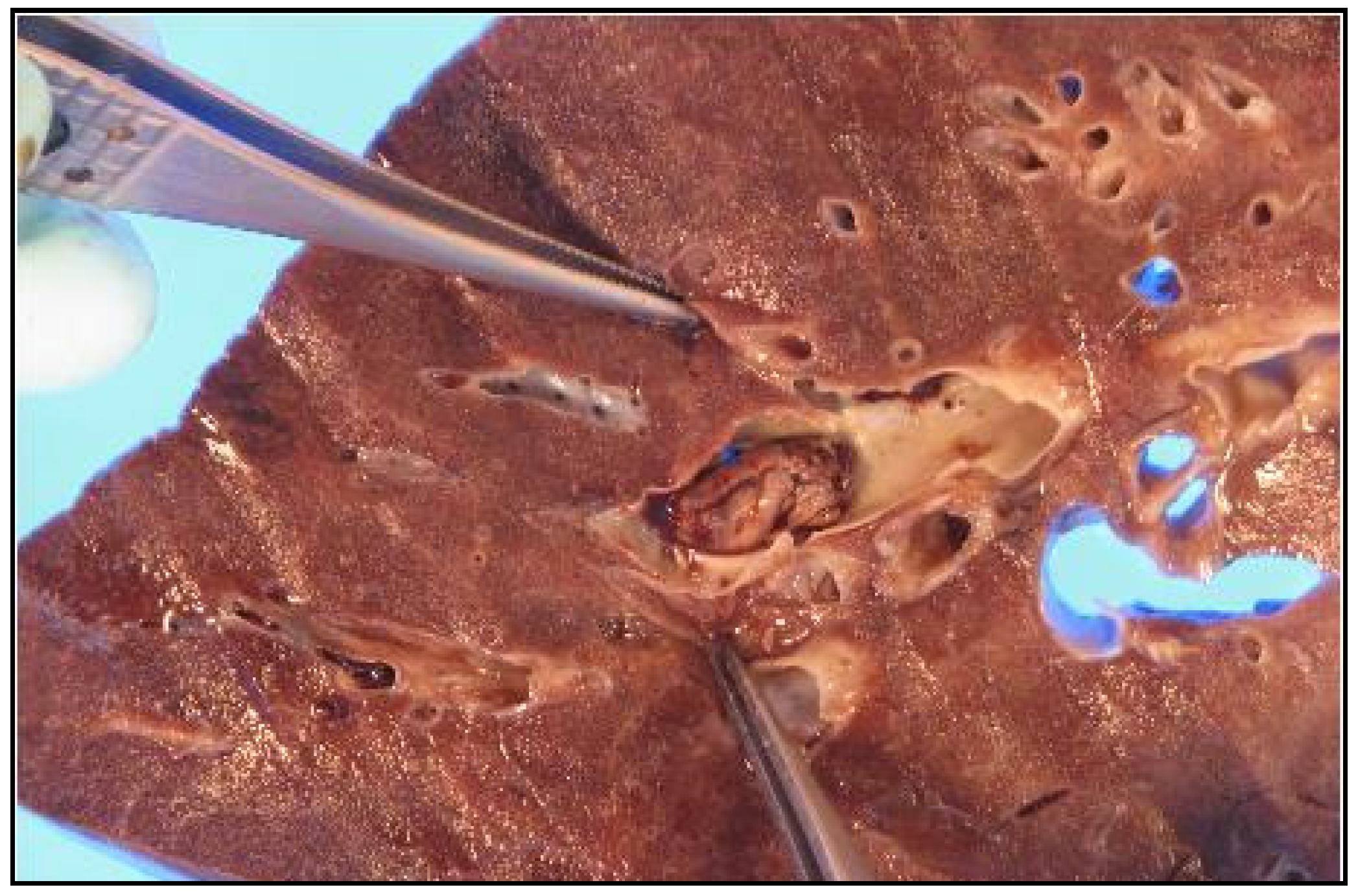
Vascular injury has been consistently reported in deceased COVID-19 patients [58]. Endotheliitis has been reported in multiple organs, including the heart, kidney, small bowel, and lungs, which could be caused by either the host’s inflammatory response or direct infection by the virus [59]. COVID-19 patients are prone to develop arterial, venous, and microvascular thrombosis, with pulmonary arterial thrombosis being the most common pattern in post-mortem studies [60,61]. The combination of diffused alveolar damage and thrombosis contributes to the rapid deterioration of severe COVID-19 cases. Thrombosis has been observed in small and medium-sized pulmonary arteries, even with prophylactic anticoagulant therapy, indicating profound coagulopathy [36] (Figure 2). Deep venous thrombosis (DVT) is found in a significant number of COVID-19 patients [62,63]. Cerebral DVT leads to encephalopathy [64]. Other systemic thromboses reported include thrombosis at the ophthalmic artery, femoral artery, portal vein, and superior mesenteric artery [61,65]. The COVID-19 thrombi are more likely to occur at the small peripheral blood vessels such as capillaries or arterioles and to consist of fibrin and platelets [66]. Damage or damage-associated molecular patterns caused by invasion of the endothelial cell of the virus, including the release of cytokines, activation of leukocytes, platelets, and completement, are thought to be contributors to the hyper coagulated state of COVID-19 [61].
5. Other Gross Pathological Findings in COVID-19
As the leading mortality cause of severe COVID-19, ARDS/CAD is not specific but seen in various direct or indirect lung injuries, including other respiratory viral infections. However, the disproportional hypoxia to radiographic abnormalities and multi-organ failure distinguish severe COVID-19 from other respiratory infectious diseases that end with ARDS/CAD [66]. Such a hallmark of COVID-19 is attributed to systemic endothelitis that disturbs the anti-coagulatory property of endothelium. This also explains why patients with certain pre-existing conditions are more likely to progress to severe COVID-19. All those conditions, including old age, hypertension, diabetes, and obesity, share one thing in common: altered endothelial metabolism [67]. A cytokine release syndrome induced by severe inflammation contributes to the adverse course of COVID-19 and multiple organ damage. The severity of the disease can be directly linked to the dramatic rise of a specific subset of cytokines, including IL-6, associated with mortality [68]. It is important to note that increased levels of specific cytokines are also predictable for mild COVID-19, for example, CCL17 [69]. The released pro-inflammatory cytokines trigger the capillary leaking syndrome, leading to disseminated intravascular coagulation (DIC) [70]. Local overactivation of completement is another important factor to consider in regarding organ damage, especially the lungs and kidneys [71]. RT-PCR has demonstrated invasion of SARS-CoV-2 at multiple organ systems besides the respiratory and cardiovascular systems [66,72,73,74]. The virus makes its way into those organs by binding the ACE2 receptors or through the blood circulation [7,13]. NRP-1 receptor has been reported to potentiate SARS-CoV-2 entry into the cell [75].
Renal complications are common and associated with a high mortality rate of COVID-19 [76]. Renal signs of shock are seen grossly in most autopsies [45]. Clinical manifestations range from mild proteinuria to acute kidney injury (AKI), most subclinical and AKI seen in severe cases [77]. Besides the mechanisms mentioned earlier of organ damage caused by SAR-CoV-2, disturbance of the renin-angiotensin-aldosterone (RAAS) regulation system is another critical detrimental factor. The binding of the virus to its receptor ACE2 downregulates the enzymatic activity of ACE2, which catalyzes the production of angiotensins that are cardio/renal protective [78]. Acute infarction and cortical necrosis have been reported [59,79]. The pitting and coarseness of the renal capsule, representing the arterionephrosclerosis observed microscopically, is typically seen in comorbidities such as hypertension and diabetes. Intrinsic acute kidney injury (AKI) is thought to be the most common form of AKI in COVID-19 patients, as evidenced by histopathological findings including acute tubular necrosis, loss of luminal brush border, eosinophilic hyaline casts, detached tubular epithelial cells, microthrombi, and fibrosis at the interstitium without glomerular injury and lymphocyte infiltration [74]. Small fibrin thrombi of the glomeruli indicate early signs of DIC [41]. Other reported genitourinary system pathological findings include prostate vein thrombosis, testicular atrophy, or testicular parenchyma damage [66].
The neurological and psychiatric symptoms presented by the COVID-19 patients suggest the involvement of both the central and peripheral nervous systems. The invasion of the central nervous system occurs via the route of the blood or nerves, with the aid of the deteriorated blood–brain barrier by the cytokine storm, whereas the infection at the peripheral nervous system is most likely immune-mediated [80]. The spectrum of neurological manifestations includes the more specific ones, such as anosmia and hypogeusia, and the nonspecific ones such as fatigue, headache, dizziness, and nausea [73,81]. The most frequently reported gross anomalies in the brain are ischemia, hemorrhage, and edema [73]. The neurons that execute cognitive functions seem more likely to be affected [82]. Microglial activation has been observed in many studies [80]; other abnormal histological findings such as microthrombi [83], brain stem encephalitis [72], and myelin loss are also reported [84]. Neurosensory skin system involvement has been evidenced by more and more reported cutaneous neurosensory symptoms. Burning pain or itching sensations start proximally in a diffused pattern irrespective of dermatomes. The affected skin area is erythematous with red-purple color. Histological examinations demonstrate hypertrophic nerve fibers without inflammation [85].
Gastrointestinal symptoms are common and can be the only manifestation, leading to delayed diagnosis of COVID-19. The symptoms are nonspecific, with loss of appetite and diarrhea being the most common [86]. Multiple punctate hemorrhages in the mucosa of the stomach and duodenum have been reported [41]. Acute mesenteric ischemia (AMI) is a rare but life-threatening emergent thrombotic complication of COVID-19 caused by arterial or venous thrombosis [87,88]. Exploratory laparotomy reveals the superior mesenteric artery without pulse and the gangrenous small intestine [89]. Thrombosis can occur at the portal or mesenteric veins as well [90].
Abnormal liver function is common in COVID-19 patients, especially in older and/or severe cases. The factors causing liver damage include direct attack by the virus, cytokine storm, hypoxia, and hepatotoxic drugs [91]. The compromised liver function indicated by elevated levels of liver enzymes can be persistent and chronic, with males being more susceptible to it [92]. Steatosis is the most common hepatic finding in COVID-19 autopsy. The liver is larger with fatty changes consistent with the common comorbidities of COVID-19, such as hypertension, obesity, and diabetes [54]. Ischemic and necrotic changes in the liver have been reported. Acute portal thrombosis secondary to COVID-19 has turned out not to be a rare case [65]. The hepatic sinus may become congested and dark red due to micro thrombosis [92]. The damaged liver can profoundly affect other organ systems and interfere with anti-viral treatment. For example, the skin color becomes darker in rare cases of COVID-19 due to adrenocortical insufficiency caused by decreased inactivation of estrogen by the liver [92].
Significantly increased incidence of type I diabetes mellitus during the pandemic calls for attention to the involvement of the pancreas in COVID-19 [93]. The rapid postmortem autolysis of the pancreas makes it quite a challenge to study it in much detail from autopsy, and gross examinations have not reported any severe injuries [80], but decreased insulin production and glucose-stimulated secretion after SARS-CoV-2 infection have been discovered [94].
Dysregulated immune responses and the typical peripheral lymphopenia in severe COVID-19 indicates the involvement of lymphoid organs [80]. The spleen can be impaired in COVID-19 by direct viral assault, cytokine storm, thrombosis, or lymphocyte apoptosis [95]. The spleen may serve as the reservoir of SARS-CoV-2, which may account for the recurrence of COVID-19 [96]. Grossly, the spleen is contracted by the shrinking capsule. Infarction, thrombi, and hemorrhage are common findings [97]. Several cases of spontaneous splenic rupture related to COVID-19 have been reported. The lacerations can be multiple, accompanied by hemorrhage or hematoma, necrosis, and blood clots [98]. Microscopically, neutrophil infiltration in the red pulp, necrosis, reduction in lymphoid follicles, and white pulp atrophy have been observed. Arterial thrombosis and fibrous tissue proliferation at the sinus are the common causes of spleen infarction. Persistent depletion of IgM memory B cells is associated with a higher mortality rate and increased risk of superimposed bacterial infections [38,95]. Mediastinal lymphadenopathy has been detected in hospitalized patients and, more often, in severe COVID-19 [99]. Enlarged intrathoracic lymph nodes were found in autopsy [97]. Characteristic lymph node changes include edema, capillary congestion, and hemorrhage. Histopathological alterations are manifested by disrupted boundaries between follicles and paracortical zones, focal necrosis and apoptosis, and reduction in or atrophy of lymphoid follicles and white pulp [97,99]. Blockage of lymphatic vessels by fibrin blots has been reported, indicating the coagulopathies associated with COVID-19 are not limited to blood vasculature [100].
In severe cases, cardiomegaly, liver damage, intestinal mucositis, and hemorrhage can be present altogether, besides respiratory symptoms [36]. Multiple organ failures are observed in many patients and may be contributed by the pro-inflammatory cytokine storm involving a variety of ILs, interferon-gamma, and activated macrophages [15,36].
6. Conclusions
- COVID-19 can be a multi-organ systemic disease. COVID-19 has often been considered a respiratory viral disease, yet it is clear that SARS-CoV-2 affects multiple extrapulmonary organs besides the lungs. It can spread systemically, which may explain the lingering symptoms of long-COVID. The complexity of COVID-19 has been made aware of as the pandemic evolved. The virus has been found in macrophages, monocytes, and endothelial cells at multiple blood–physiology barriers [101]. The mechanism of organ injury includes direct viral attack, hypoxia, and inflammatory response secondary to viral infection.
- The sequelae of COVID-19 can be highly individualized. Pathological studies have revealed that pre-existing conditions play critical roles in the clinical course of COVID-19. The most common comorbidities include systemic hypertension, diabetes, obesity, and coronary artery disease [18].
- The pathogenesis of long-COVID is still under investigation. It takes a varied length of time to recover from COVID-19 infection. A significant number of patients reported lasting symptoms over twelve weeks after acute infection, known as long-COVID, “long haulers”, or long-COVID syndrome [102]. The occurrence of long-COVID is not necessarily directly related to the severity of the initial disease [103]. The constellation of the symptoms such as fatigue, muscle weakness, dyspnea, pain, discomfort, etc. indicates the involvement of multiple organ systems and can significantly affect the quality of the patient’s life. The evolution of long-COVID can be attributed to either direct viral attacks or the outcomes of viral attacks, including inflammation and oxidative stress [104].
- Testing for a broader group of potential causative agents is necessary for acute diagnosis and appropriate patient management. The respiratory distress and the gross pathological changes observed in COVID-19 are not specific. Complete pathological examination using ancillary tools such as cytology, electron microscopy, and other tissue techniques are beneficial for making an accurate diagnosis, differentiation from other coronavirus infections, and deepening our understanding of the pathogenesis of COVID-19 as a newly emerging disorder.
Funding
This research received no external funding.
Data Availability Statement
All references used in this review can be found at PubMed.
Acknowledgments
I greatly appreciate Sharon Mount’s advice in preparing the paper and providing two autopsy photos.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zavascki, A.P.; Falci, D.R. Clinical Characteristics of COVID-19 in China. N. Engl. J. Med. 2020, 382, 1859. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. COVID-19: WHO declares pandemic because of "alarming levels" of spread, severity, and inaction. BMJ 2020, 368, m1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- JHU. COVID-19 Dashboard. Available online: https://coronavirus.jhu.edu/map.html (accessed on 31 May 2021).
- Beneke, R.; Leithäuser, R.M. COVID-19: Impact of a “Global Player”-A Reflection 1 Year On. Int. J. Sports Physiol. Perform 2021, 16, 323–324. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.A.; Sheikh, F.N.; Jamal, S.; Ezeh, J.K.; Akhtar, A. Coronavirus (COVID-19): A Review of Clinical Features, Diagnosis, and Treatment. Cureus 2020, 12, e7355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, G.; Liu, D. SARS-like virus in the Middle East: A truly bat-related coronavirus causing human diseases. Protein Cell 2012, 3, 803–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, P.; Wang, M.; Wei, Y.; Kim, T.; Wei, X. Coronavirus in human diseases: Mechanisms and advances in clinical treatment. MedComm 2020, 1, 270–301. [Google Scholar] [CrossRef]
- Calabrese, F.; Pezzuto, F.; Fortarezza, F.; Hofman, P.; Kern, I.; Panizo, A.; von der Thüsen, J.; Timofeev, S.; Gorkiewicz, G.; Lunardi, F. Pulmonary pathology and COVID-19: Lessons from autopsy. The experience of European Pulmonary Pathologists. Virchows Arch. 2020, 477, 359–372. [Google Scholar] [CrossRef]
- (CDC). Centers for Disease Control and Prevent. Scientific Brief: SARS-CoV-2 Transmission. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/sars-cov-2-transmission.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fscience%2Fscience-briefs%2Fscientific-brief-sars-cov-2.html#anchor_1619805167515 (accessed on 22 May 2021).
- Marsh, M.; Helenius, A. Virus entry: Open sesame. Cell 2006, 124, 729–740. [Google Scholar] [CrossRef] [Green Version]
- WHO. Tracking SARS-CoV-2 variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants (accessed on 26 July 2022).
- Scherer, E.M.; Babiker, A.; Adelman, M.W.; Allman, B.; Key, A.; Kleinhenz, J.M.; Langsjoen, R.M.; Nguyen, P.V.; Onyechi, I.; Sherman, J.D.; et al. SARS-CoV-2 Evolution and Immune Escape in Immunocompromised Patients. N. Engl. J. Med. 2022, 386, 2436–2438. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Li, H.; Liu, L.; Zhang, D.; Xu, J.; Dai, H.; Tang, N.; Su, X.; Cao, B. SARS-CoV-2 and viral sepsis: Observations and hypotheses. Lancet 2020, 395, 1517–1520. [Google Scholar] [CrossRef]
- Stasi, A.; Castellano, G.; Ranieri, E.; Infante, B.; Stallone, G.; Gesualdo, L.; Netti, G.S. SARS-CoV-2 and Viral Sepsis: Immune Dysfunction and Implications in Kidney Failure. J. Clin. Med. 2020, 9, 4057. [Google Scholar] [CrossRef] [PubMed]
- Al-Ansari, R.Y.; Alshaer, A.; Al-Anazi, A.; Al-Otaibi, N.; Abdalla, L.; Al-Tarrah, S.; Shilash, A.; Al-Zahrani, N. ABO in Correlation to the Requirement of Mechanical Ventilation and Mortality in Critically Ill Patients With COVID-19. J. Hematol. 2021, 10, 64–70. [Google Scholar] [CrossRef]
- Hooper, J.E.; Padera, R.F.; Dolhnikoff, M.; da Silva, L.F.F.; Duarte-Neto, A.N.; Kapp, M.E.; Lacy, J.M.; Mauad, T.; Saldiva, P.H.N.; Rapkiewicz, A.V.; et al. A Postmortem Portrait of the Coronavirus Disease 2019 (COVID-19) Pandemic: A Large Multi-institutional Autopsy Survey Study. Arch. Pathol. Lab. Med. 2021, 145, 529–535. [Google Scholar] [CrossRef]
- Himwaze, C.M.; Telendiy, V.; Maate, F.; Songwe, M.; Chanda, C.; Chanda, D.; Julius, P.; Mumba, C.; Marimo, C.; Hamukale, A.; et al. Post Mortem examination of Hospital Inpatient COVID-19 Deaths in Lusaka, Zambia—A Descriptive Whole Body Autopsy Series. Int. J. Infect. Dis. 2021, 108, 363–369. [Google Scholar] [CrossRef]
- Weiss, P.; Murdoch, D.R. Clinical course and mortality risk of severe COVID-19. Lancet 2020, 395, 1014–1015. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Sperhake, J.P. Autopsies of COVID-19 deceased? Absolutely! Leg. Med. 2020, 47, 101769. [Google Scholar] [CrossRef]
- Sapino, A.; Facchetti, F.; Bonoldi, E.; Gianatti, A.; Barbareschi, M.; SIAPEC. The autopsy debate during the COVID-19 emergency: The Italian experience. Virchows Arch. 2020, 476, 821–823. [Google Scholar] [CrossRef]
- Barton, L.M.; Duval, E.J.; Stroberg, E.; Ghosh, S.; Mukhopadhyay, S. COVID-19 Autopsies, Oklahoma, USA. Am. J. Clin. Pathol. 2020, 153, 725–733. [Google Scholar] [CrossRef] [Green Version]
- Wichmann, D.; Sperhake, J.P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19: A Prospective Cohort Study. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Kaufer, A.M.; Theis, T.; Lau, K.A.; Gray, J.L.; Rawlinson, W.D. Laboratory biosafety measures involving SARS-CoV-2 and the classification as a Risk Group 3 biological agent. Pathology 2020, 52, 790–795. [Google Scholar] [CrossRef] [PubMed]
- Hanley, B.; Lucas, S.B.; Youd, E.; Swift, B.; Osborn, M. Autopsy in suspected COVID-19 cases. J. Clin. Pathol. 2020, 73, 239–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OSHA. Postmortem Care Workers and Employers. Available online: https://www.osha.gov/coronavirus/control-prevention/postmortem-care (accessed on 20 May 2021).
- Baj, J.; Ciesielka, M.; Buszewicz, G.; Maciejewski, R.; Budzyńska, B.; Listos, P.; Teresiński, G. COVID-19 in the autopsy room-requirements, safety, recommendations and pathological findings. Forensic Sci. Med. Pathol. 2021, 17, 101–113. [Google Scholar] [CrossRef]
- CDC. Collection and Submission of Postmortem Specimens from Deceased Persons with Confirmed or Suspected COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-postmortem-specimens.html (accessed on 20 May 2021).
- CAP. Amended COVID-19 Autopsy Guideline Statement from the CAP Autopsy Committee. Available online: https://documents.cap.org/documents/COVID-Autopsy-Statement.pdf (accessed on 20 May 2021).
- Basso, C.; Calabrese, F.; Sbaraglia, M.; Del Vecchio, C.; Carretta, G.; Saieva, A.; Donato, D.; Flor, L.; Crisanti, A.; Dei Tos, A.P. Feasibility of postmortem examination in the era of COVID-19 pandemic: The experience of a Northeast Italy University Hospital. Virchows Arch. 2020, 477, 341–347. [Google Scholar] [CrossRef]
- Youd, E.; Moore, L. COVID-19 autopsy in people who died in community settings: The first series. J. Clin. Pathol. 2020, 73, 840–844. [Google Scholar] [CrossRef]
- Santurro, A.; Scopetti, M.; D’Errico, S.; Fineschi, V. A technical report from the Italian SARS-CoV-2 outbreak. Postmortem sampling and autopsy investigation in cases of suspected or probable COVID-19. Forensic Sci. Med. Pathol. 2020, 16, 471–476. [Google Scholar] [CrossRef]
- Fu, L.; Zak, T.; Shanes, E. A Framework for Maintaining a Fully Operational Autopsy Service at a Large Academic Teaching Institution During a Global Pandemic. Acad. Pathol. 2021, 8, 23742895211006821. [Google Scholar] [CrossRef]
- Bösmüller, H.; Traxler, S.; Bitzer, M.; Häberle, H.; Raiser, W.; Nann, D.; Frauenfeld, L.; Vogelsberg, A.; Klingel, K.; Fend, F. The evolution of pulmonary pathology in fatal COVID-19 disease: An autopsy study with clinical correlation. Virchows Arch. 2020, 477, 349–357. [Google Scholar] [CrossRef]
- Domke, L.M.; Klein, I.M.; Hartmann, L.; Schwab, C.; Marx, A.; Werner, M.; Möller, P.; Fend, F.; Bösmüller, H.; Schirmacher, P. Biobanking in times of crisis—The COVID-19 Autopsy and Biosample Registry Baden-Wuerttemberg. Pathol. Res. Pract. 2022, 237, 154011. [Google Scholar] [CrossRef] [PubMed]
- Yurdaisik, I.; Demiroz, A.S.; Oz, A.B.; Akker, M.; Agirman, A.; Aksoy, S.H.; Nurili, F. Postmortem Biopsies of the Lung, Heart, Liver, and Spleen of COVID-19 Patients. Cureus 2021, 13, e20734. [Google Scholar] [CrossRef] [PubMed]
- von Stillfried, S.; Bülow, R.D.; Röhrig, R.; Boor, P.; German Registry of COVID-19 Autopsies (DeRegCOVID), D.R.C. First report from the German COVID-19 autopsy registry. Lancet. Reg. Health Eur. 2022, 15, 100330. [Google Scholar] [CrossRef] [PubMed]
- Suess, C.; Hausmann, R. Gross and histopathological pulmonary findings in a COVID-19 associated death during self-isolation. Int. J. Legal. Med. 2020, 134, 1285–1290. [Google Scholar] [CrossRef]
- Adachi, T.; Chong, J.M.; Nakajima, N.; Sano, M.; Yamazaki, J.; Miyamoto, I.; Nishioka, H.; Akita, H.; Sato, Y.; Kataoka, M.; et al. Clinicopathologic and Immunohistochemical Findings from Autopsy of Patient with COVID-19, Japan. Emerg. Infect. Dis. 2020, 26, 2157–2161. [Google Scholar] [CrossRef]
- Attoh, S.; Segborwotso, R.P.; Akoriyea, S.K.; Teddy, G.; Edusei, L.; Hobenu, F.; Agyemang-Bediako, K.; Toppar, A.; Fatchu, R.D.; Akakpo, P.K. COVID-19 autopsy reports from the Ga-East Municipal and the 37 Military Hospitals in Accra, Ghana. Ghana Med. J. 2020, 54, 52–61. [Google Scholar] [CrossRef]
- Grosse, C.; Grosse, A.; Salzer, H.J.F.; Dünser, M.W.; Motz, R.; Langer, R. Analysis of cardiopulmonary findings in COVID-19 fatalities: High incidence of pulmonary artery thrombi and acute suppurative bronchopneumonia. Cardiovasc. Pathol. 2020, 49, 107263. [Google Scholar] [CrossRef]
- Tian, S.; Xiong, Y.; Liu, H.; Niu, L.; Guo, J.; Liao, M.; Xiao, S.Y. Pathological study of the 2019 novel coronavirus disease (COVID-19) through postmortem core biopsies. Mod. Pathol. 2020, 33, 1007–1014. [Google Scholar] [CrossRef] [Green Version]
- Menter, T.; Haslbauer, J.D.; Nienhold, R.; Savic, S.; Hopfer, H.; Deigendesch, N.; Frank, S.; Turek, D.; Willi, N.; Pargger, H.; et al. Postmortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings in lungs and other organs suggesting vascular dysfunction. Histopathology 2020, 77, 198–209. [Google Scholar] [CrossRef]
- Verger, A.; Rousseau, P.F.; Malbos, E.; Chawki, M.B.; Nicolas, F.; Lançon, C.; Khalfa, S.; Guedj, E. Involvement of the cerebellum in EMDR efficiency: A metabolic connectivity PET study in PTSD. Eur. J. Psychotraumatol. 2020, 11, 1767986. [Google Scholar] [CrossRef]
- Lacy, J.M.; Brooks, E.G.; Akers, J.; Armstrong, D.; Decker, L.; Gonzalez, A.; Humphrey, W.; Mayer, R.; Miller, M.; Perez, C.; et al. COVID-19: Postmortem Diagnostic and Biosafety Considerations. Am. J. Forensic Med. Pathol. 2020, 41, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Halushka, M.K.; Vander Heide, R.S. Myocarditis is rare in COVID-19 autopsies: Cardiovascular findings across 277 postmortem examinations. Cardiovasc. Pathol. 2021, 50, 107300. [Google Scholar] [CrossRef] [PubMed]
- Boukhris, M.; Hillani, A.; Moroni, F.; Annabi, M.S.; Addad, F.; Ribeiro, M.H.; Mansour, S.; Zhao, X.; Ybarra, L.F.; Abbate, A.; et al. Cardiovascular Implications of the COVID-19 Pandemic: A Global Perspective. Can. J. Cardiol. 2020, 36, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Adeghate, E.A.; Eid, N.; Singh, J. Mechanisms of COVID-19-induced heart failure: A short review. Heart Fail. Rev. 2021, 26, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Escher, F.; Pietsch, H.; Aleshcheva, G.; Bock, T.; Baumeier, C.; Elsaesser, A.; Wenzel, P.; Hamm, C.; Westenfeld, R.; Schultheiss, M.; et al. Detection of viral SARS-CoV-2 genomes and histopathological changes in endomyocardial biopsies. ESC Heart Fail. 2020, 7, 2440–2447. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [Green Version]
- Roshdy, A.; Zaher, S.; Fayed, H.; Coghlan, J.G. COVID-19 and the Heart: A Systematic Review of Cardiac Autopsies. Front. Cardiovasc. Med. 2020, 7, 626975. [Google Scholar] [CrossRef]
- Elsoukkary, S.S.; Mostyka, M.; Dillard, A.; Berman, D.R.; Ma, L.X.; Chadburn, A.; Yantiss, R.K.; Jessurun, J.; Seshan, S.V.; Borczuk, A.C.; et al. Autopsy Findings in 32 Patients with COVID-19: A Single-Institution Experience. Pathobiology 2021, 88, 56–68. [Google Scholar] [CrossRef]
- Fox, S.E.; Akmatbekov, A.; Harbert, J.L.; Li, G.; Quincy Brown, J.; Vander Heide, R.S. Pulmonary and cardiac pathology in African American patients with COVID-19: An autopsy series from New Orleans. Lancet Respir. Med. 2020, 8, 681–686. [Google Scholar] [CrossRef]
- Nicolai, L.; Leunig, A.; Brambs, S.; Kaiser, R.; Weinberger, T.; Weigand, M.; Muenchhoff, M.; Hellmuth, J.C.; Ledderose, S.; Schulz, H.; et al. Immunothrombotic Dysregulation in COVID-19 Pneumonia Is Associated With Respiratory Failure and Coagulopathy. Circulation 2020, 142, 1176–1189. [Google Scholar] [CrossRef]
- Hanley, B.; Jensen, M.; Osborn, M. Emerging spectrum of COVID-19-related cardiopulmonary pathology in adults. Diagn. Histopathol. 2021, 27, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Sadeghzadeh-Bazargan, A.; Rezai, M.; Nobari, N.N.; Mozafarpoor, S.; Goodarzi, A. Skin manifestations as potential symptoms of diffuse vascular injury in critical COVID-19 patients. J. Cutan. Pathol. 2021, 48, 1266–1276. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z. Endotheliitis in COVID-19. Pathologe 2020, 41, 99–102. [Google Scholar] [CrossRef]
- Romanova, E.S.; Vasilyev, V.V.; Startseva, G.; Karev, V.; Rybakova, M.G.; Platonov, P.G. Cause of death based on systematic post-mortem studies in patients with positive SARS-CoV-2 tissue PCR during the COVID-19 pandemic. J. Intern. Med. 2021, 290, 655–665. [Google Scholar] [CrossRef]
- Manolis, A.S.; Manolis, T.A.; Manolis, A.A.; Papatheou, D.; Melita, H. COVID-19 Infection: Viral Macro- and Micro-Vascular Coagulopathy and Thromboembolism/Prophylactic and Therapeutic Management. J. Cardiovasc. Pharmacol. Ther. 2021, 26, 12–24. [Google Scholar] [CrossRef]
- Rouyer, O.; Pierre-Paul, I.N.; Balde, A.T.; Jupiter, D.; Bindila, D.; Geny, B.; Wolff, V. High Prevalence of Deep Venous Thrombosis in Non-Severe COVID-19 Patients Hospitalized for a Neurovascular Disease. Cerebrovasc. Dis. Extra 2020, 10, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Guo, Y.; You, Y.; Hu, K.; Cai, F.; Xie, M.; Yang, L.; Ling, K.; Ye, D.; Misra, S.; et al. Deep Venous Thrombosis in COVID-19 Patients: A Cohort Analysis. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620982669. [Google Scholar] [CrossRef]
- Hoelscher, C.; Sweid, A.; Ghosh, R.; Al Saiegh, F.; Keppetipola, K.M.; Farrell, C.J.; Jallo, J.; Jabbour, P.; Tjoumakaris, S.; Gooch, M.R.; et al. Cerebral deep venous thrombosis and COVID-19: Case report. J. Neurosurg. 2020, 135, 17–20. [Google Scholar] [CrossRef]
- Hassan, W.; Ramadan, H.K. COVID-19 as a novel etiology of portal vein thrombosis: Change in the current management concepts. Infect. Dis. 2021, 53, 148–150. [Google Scholar] [CrossRef]
- Satturwar, S.; Fowkes, M.; Farver, C.; Wilson, A.M.; Eccher, A.; Girolami, I.; Pujadas, E.; Bryce, C.; Salem, F.; El Jamal, S.M.; et al. Postmortem Findings Associated With SARS-CoV-2: Systematic Review and Meta-analysis. Am. J. Surg. Pathol. 2021, 45, 587–603. [Google Scholar] [CrossRef]
- Maccio, U.; Zinkernagel, A.S.; Shambat, S.M.; Zeng, X.; Cathomas, G.; Ruschitzka, F.; Schuepbach, R.A.; Moch, H.; Varga, Z. SARS-CoV-2 leads to a small vessel endotheliitis in the heart. EBioMedicine 2021, 63, 103182. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; Sharif, K.; O’Regan, A.; Bridgewood, C. The Role of Cytokines including Interleukin-6 in COVID-19 induced Pneumonia and Macrophage Activation Syndrome-Like Disease. Autoimmun. Rev. 2020, 19, 102537. [Google Scholar] [CrossRef]
- Sugiyama, M.; Kinoshita, N.; Ide, S.; Nomoto, H.; Nakamoto, T.; Saito, S.; Ishikane, M.; Kutsuna, S.; Hayakawa, K.; Hashimoto, M.; et al. Serum CCL17 level becomes a predictive marker to distinguish between mild/moderate and severe/critical disease in patients with COVID-19. Gene 2021, 766, 145145. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.A.; Canna, S.W.; Schulert, G.S.; Volpi, S.; Lee, P.Y.; Kernan, K.F.; Caricchio, R.; Mahmud, S.; Hazen, M.M.; Halyabar, O.; et al. On the Alert for Cytokine Storm: Immunopathology in COVID-19. Arthritis Rheumatol. 2020, 72, 1059–1063. [Google Scholar] [CrossRef] [Green Version]
- Niederreiter, J.; Eck, C.; Ries, T.; Hartmann, A.; Märkl, B.; Büttner-Herold, M.; Amann, K.; Daniel, C. Complement Activation. Front. Immunol. 2022, 13, 835156. [Google Scholar] [CrossRef] [PubMed]
- Delavari, F.; Varzaneh, F.N.; Rezaei, N. Neurologic Manifestations of COVID-19. Adv. Exp. Med. Biol. 2021, 1318, 343–353. [Google Scholar] [CrossRef]
- Al-Sarraj, S.; Troakes, C.; Hanley, B.; Osborn, M.; Richardson, M.P.; Hotopf, M.; Bullmore, E.; Everall, I.P. Invited Review: The spectrum of neuropathology in COVID-19. Neuropathol. Appl. Neurobiol. 2021, 47, 3–16. [Google Scholar] [CrossRef]
- Diao, B.; Wang, C.; Wang, R.; Feng, Z.; Zhang, J.; Yang, H.; Tan, Y.; Wang, H.; Liu, L.; Liu, Y.; et al. Human kidney is a target for novel severe acute respiratory syndrome coronavirus 2 infection. Nat. Commun. 2021, 12, 2506. [Google Scholar] [CrossRef]
- Cantuti-Castelvetri, L.; Ojha, R.; Pedro, L.D.; Djannatian, M.; Franz, J.; Kuivanen, S.; van der Meer, F.; Kallio, K.; Kaya, T.; Anastasina, M.; et al. Neuropilin-1 facilitates SARS-CoV-2 cell entry and infectivity. Science 2020, 370, 856–860. [Google Scholar] [CrossRef]
- Pei, G.; Zhang, Z.; Peng, J.; Liu, L.; Zhang, C.; Yu, C.; Ma, Z.; Huang, Y.; Liu, W.; Yao, Y.; et al. Renal Involvement and Early Prognosis in Patients with COVID-19 Pneumonia. J. Am. Soc. Nephrol. 2020, 31, 1157–1165. [Google Scholar] [CrossRef]
- Martinez-Rojas, M.A.; Vega-Vega, O.; Bobadilla, N.A. Is the kidney a target of SARS-CoV-2? Am. J. Physiol. Renal. Physiol. 2020, 318, F1454–F1462. [Google Scholar] [CrossRef] [PubMed]
- Apetrii, M.; Enache, S.; Siriopol, D.; Burlacu, A.; Kanbay, A.; Kanbay, M.; Scripcariu, D.; Covic, A. A brand-new cardiorenal syndrome in the COVID-19 setting. Clin. Kidney J. 2020, 13, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Project, C.; Autopsias, P. The first COVID-19 autopsy in Spain performed during the early stages of the pandemic. Rev. Esp. Patol. 2020, 53, 182–187. [Google Scholar] [CrossRef]
- Jonigk, D.; Werlein, C.; Acker, T.; Aepfelbacher, M.; Amann, K.U.; Baretton, G.; Barth, P.; Bohle, R.M.; Büttner, A.; Büttner, R.; et al. Organ manifestations of COVID-19: What have we learned so far (not only) from autopsies? Virchows Arch. 2022, 481, 139–159. [Google Scholar] [CrossRef] [PubMed]
- Vakili, K.; Fathi, M.; Hajiesmaeili, M.; Salari, M.; Saluja, D.; Tafakhori, A.; Sayehmiri, F.; Rezaei-Tavirani, M. Neurological Symptoms, Comorbidities, and Complications of COVID-19: A Literature Review and Meta-Analysis of Observational Studies. Eur. Neurol. 2021, 84, 307–324. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.C.; Kern, F.; Losada, P.M.; Agam, M.R.; Maat, C.A.; Schmartz, G.P.; Fehlmann, T.; Stein, J.A.; Schaum, N.; Lee, D.P.; et al. Dysregulation of brain and choroid plexus cell types in severe COVID-19. Nature 2021, 595, 565–571. [Google Scholar] [CrossRef]
- Bryce, C.; Grimes, Z.; Pujadas, E.; Ahuja, S.; Beasley, M.B.; Albrecht, R.; Hernandez, T.; Stock, A.; Zhao, Z.; AlRasheed, M.R.; et al. Pathophysiology of SARS-CoV-2: The Mount Sinai COVID-19 autopsy experience. Mod. Pathol. 2021, 34, 1456–1467. [Google Scholar] [CrossRef]
- Reichard, R.R.; Kashani, K.B.; Boire, N.A.; Constantopoulos, E.; Guo, Y.; Lucchinetti, C.F. Neuropathology of COVID-19: A spectrum of vascular and acute disseminated encephalomyelitis (ADEM)-like pathology. Acta Neuropathol. 2020, 140, 1–6. [Google Scholar] [CrossRef]
- Grieco, T.; Gomes, V.; Rossi, A.; Cantisani, C.; Greco, M.E.; Rossi, G.; Sernicola, A.; Pellacani, G. The Pathological Culprit of Neuropathic Skin Pain in Long COVID-19 Patients: A Case Series. J. Clin. Med. 2022, 11, 4474. [Google Scholar] [CrossRef]
- Mao, R.; Qiu, Y.; He, J.S.; Tan, J.Y.; Li, X.H.; Liang, J.; Shen, J.; Zhu, L.R.; Chen, Y.; Iacucci, M.; et al. Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 667–678. [Google Scholar] [CrossRef]
- Calcagno, E.; Sogunro, O.; Nepal, P.; Assaker, R.; Sapire, J. COVID-19 induced mesenteric venous infarction. Radiol. Case Rep. 2021, 16, 1999–2002. [Google Scholar] [CrossRef] [PubMed]
- Segovia, F.D.; Ream, S.; Dang, T.; Chaganti, B.T.; Ortega, A.J.; Rhee, S.; Borges, J.C. COVID-19-Associated Superior Mesenteric Artery Thrombosis and Acute Intestinal Ischemia. Cureus 2022, 14, e27722. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.S.; Naqi, S.A.; Ashraf, M.; Saleem, M.; Raza, H.A.; Haider, U. A rare case report of short bowel anastomosis after acute mesenteric ischaemia in COVID-19 postive patient. J. Pak. Med. Assoc. 2022, 72, 1222–1224. [Google Scholar] [CrossRef] [PubMed]
- Batra, S.; Nair, A.G.; Syal, K. An Unusual Presentation of Superior Mesenteric Venous Occlusion in Mild COVID-19. Indian J. Clin. Biochem. 2022, 1–4. [Google Scholar] [CrossRef]
- Bertolini, A.; van de Peppel, I.P.; Bodewes, F.A.J.A.; Moshage, H.; Fantin, A.; Farinati, F.; Fiorotto, R.; Jonker, J.W.; Strazzabosco, M.; Verkade, H.J.; et al. Abnormal Liver Function Tests in Patients With COVID-19: Relevance and Potential Pathogenesis. Hepatology 2020, 72, 1864–1872. [Google Scholar] [CrossRef]
- Li, P.; Liu, Y.; Cheng, Z.; Yu, X.; Li, Y. COVID-19-associated liver injury: Clinical characteristics, pathophysiological mechanisms and treatment management. Biomed. Pharmacother. 2022, 154, 113568. [Google Scholar] [CrossRef]
- Kayhan, S.; Hepsen, S.; Kalkisim, H.K.; Sendur, I.N.; Altay, F.A.; Yalcindag, A. The evaluation of pancreas β-cell autoantibodies in non-diabetic COVID-19 patients. Arch. Endocrinol. Metab. 2022, 66, 459–465. [Google Scholar] [CrossRef]
- Szarpak, L.; Pruc, M.; Najeeb, F.; Jaguszewski, M.J. POST-COVID-19 and the pancreas. Am. J. Emerg. Med. 2022, 59, 174–175. [Google Scholar] [CrossRef]
- Cococcia, S.; Lenti, M.V.; Santacroce, G.; Achilli, G.; Borrelli de Andreis, F.; Di Sabatino, A. Liver-spleen axis dysfunction in COVID-19. World J. Gastroenterol. 2021, 27, 5919–5931. [Google Scholar] [CrossRef]
- Petroianu, A. COVID-19 recurrence associated with the virus storage in the Spleen. Rev. Assoc. Med. Bras. 2022, 68, 751–753. [Google Scholar] [CrossRef]
- Liu, Q.; Shi, Y.; Cai, J.; Duan, Y.; Wang, R.; Zhang, H.; Ruan, Q.; Li, J.; Zhao, L.; Ping, Y.; et al. Pathological changes in the lungs and lymphatic organs of 12 COVID-19 autopsy cases. Natl. Sci. Rev. 2020, 7, 1868–1878. [Google Scholar] [CrossRef] [PubMed]
- Trabulsi, N.H.; Alshammakh, S.S.; Shabkah, A.A.; Aladawi, M.; Farsi, A.H. Spontaneous rupture of spleen in a patient with COVID-19 disease: Case report and review of the literature. J. Surg. Case Rep. 2022, 2022, rjac124. [Google Scholar] [CrossRef] [PubMed]
- Abdullaev, A.; Odilov, A.; Ershler, M.; Volkov, A.; Lipina, T.; Gasanova, T.; Lebedin, Y.; Babichenko, I.; Sudarikov, A. Viral Load and Patterns of SARS-CoV-2 Dissemination to the Lungs, Mediastinal Lymph Nodes, and Spleen of Patients with COVID-19 Associated Lymphopenia. Viruses 2021, 13, 1410. [Google Scholar] [CrossRef]
- MacDonald, M.E.; Weathered, R.K.; Stewart, E.C.; Magold, A.I.; Mukherjee, A.; Gurbuxani, S.; Smith, H.; McMullen, P.; Mueller, J.; Husain, A.N.; et al. Lymphatic coagulation and neutrophil extracellular traps in lung-draining lymph nodes of COVID-19 decedents. Blood Adv. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.H.; Luo, T.; Shi, Y.; He, Z.C.; Tang, R.; Zhang, P.P.; Cai, J.; Zhou, X.D.; Jiang, D.P.; Fei, X.C.; et al. A cohort autopsy study defines COVID-19 systemic pathogenesis. Cell Res. 2021, 31, 836–846. [Google Scholar] [CrossRef]
- Baig, A.M. Chronic COVID syndrome: Need for an appropriate medical terminology for long-COVID and COVID long-haulers. J. Med. Virol. 2021, 93, 2555–2556. [Google Scholar] [CrossRef]
- Radtke, T.; Ulyte, A.; Puhan, M.A.; Kriemler, S. Long-term Symptoms After SARS-CoV-2 Infection in Children and Adolescents. JAMA 2021, 326, 869–871. [Google Scholar] [CrossRef]
- DePace, N.L.; Colombo, J. Long-COVID Syndrome and the Cardiovascular System: A Review of Neurocardiologic Effects on Multiple Systems. Curr. Cardiol. Rep. 2022. [Google Scholar] [CrossRef]
Figure 1.
A heavy lung from a deceased COVID-19 patient with patchy consolidation and hemorrhage. Figure courtesy of Dr. Sharon Mount from the University of Vermont Medical Center.
Figure 1.
A heavy lung from a deceased COVID-19 patient with patchy consolidation and hemorrhage. Figure courtesy of Dr. Sharon Mount from the University of Vermont Medical Center.

Figure 2.
A thromboembolus at the right lower lobe of the lung of a deceased COVID-19 patient. Figure courtesy of Dr. Sharon Mount from the University of Vermont Medical Center.
Figure 2.
A thromboembolus at the right lower lobe of the lung of a deceased COVID-19 patient. Figure courtesy of Dr. Sharon Mount from the University of Vermont Medical Center.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zhang, B. Gross Pathology in COVID-19. Encyclopedia 2022, 2, 1790-1802. https://doi.org/10.3390/encyclopedia2040123
AMA Style
Zhang B. Gross Pathology in COVID-19. Encyclopedia. 2022; 2(4):1790-1802. https://doi.org/10.3390/encyclopedia2040123
Chicago/Turabian StyleZhang, Bei. 2022. "Gross Pathology in COVID-19" Encyclopedia 2, no. 4: 1790-1802. https://doi.org/10.3390/encyclopedia2040123