
Pregnancy in Chronic Kidney Disease

1
Division of Nephrology, School of Medicine, Bezmialem Vakif University, Istanbul 34000, Türkiye
2
Division of Internal Medicine, Salus Hospital, 1000 Tirana, Albania
*
Authors to whom correspondence should be addressed.
Kidney Dial. 2023, 3(2), 152-162; https://doi.org/10.3390/kidneydial3020013
Submission received: 29 December 2022
/
Revised: 27 February 2023
/
Accepted: 24 March 2023
/
Published: 27 March 2023
(This article belongs to the Special Issue Feature Papers for Kidney and Dialysis: Advances in Nephrology and Dialysis)
Abstract
:While pregnancy among end-stage kidney disease patients is rare, the number of females becoming pregnant has been increasing worldwide during the last decade. The frequency of conception in this patient group has been reported to be between 0.3% and 7% per year. The aim of this review is to summarize the latest guidelines and practice points for ensuring the best outcome for both the fetus and the mother.
Keywords:
pregnancy; chronic kidney disease; hemodialysis; peritoneal dialysis; transplant; outcome; dialysis1. Introduction
The issue of pregnancy in advanced chronic kidney disease (CKD) is longstanding: early case series of pregnant women on hemodialysis were published by Herwing et al. in 1965 [1] and Orme et al. in 1968 [2], followed in 1971 by an Italian group study which reported the first successful pregnancies whilst on hemodialysis [3]. Subsequent studies conducted in Europe and the United States further described and characterized successful pregnancies in women on dialysis. Paralleling the data increase, from 1980 to the present day there has been up to a 90% increase in the pregnancy success rate in this patient population [4,5]. Confirmatory data of this trend are found in the ANZDATA registry (Australian and New-Zealand Dialysis and Transplant registry), which showed an increase in pregnancy rates of women under hemodialysis over the years, from 0.67 per 1000 patients per year between 1986 and 1995 to 3.3 per 1000 between 1996 and 2008 [6]. Pregnancies in women on hemodialysis present some of the most complicated clinical challenges for physicians [7]. Like pregnant women in the common population, a woman’s body undergoes several changes during pregnancy, including an increase in blood volume, urine protein excretion, cardiac output and an approximatively 50% rise in glomerular filtration rate (GFR) [8]. In kidney, hyperfiltration leads to reduced serum creatinine levels, as well as lower vascular resistance and blood pressure [8,9]. Chronic kidney disease (CKD) patients, whether on dialysis or not, have a complex set of comorbidities that can be difficult to manage, especially in this setting. CKD in itself may complicate pregnancy, which is also true for any of its accompanying comorbidities.
Women with CKD require specific management during pregnancy [7,8,9,10,11,12,13,14]. Women on dialysis have both lower fertility rates and a higher rate of unsuccessful or complicated pregnancies due to hypertension, preeclampsia, anemia, miscarriage, polyhydramnios, prematurity and intrauterine growth restriction [12]. Medications such as antihypertensive drugs, aspirin, iron, calcium, and ESA should be prescribed according to the clinical situation. It is important to increase the frequency and duration of HD to a minimum of 20 h per week, ideally higher than 36 h per week, to reduce the risk of preterm birth and small gestational age (SGA) [7,8,9,10,11]. The goal of dialysis intensification is to achieve better clearance of uremic toxins, increase ultrafiltration rate, reduce the risk of high blood pressure and cardiac hypertrophy and improve endothelial function [10].
2. CKD and Pregnancy
During pregnancy, kidneys undergo several physiological changes. The glomerular filtration rate increases by 50% in the second trimester, followed by a relative decrease in creatinine clearance in the third trimester [9]. In a meta-analysis, Wiles et al. showed that the upper-normal creatinine levels might be 0.86 mg/dL in the first trimester, 0.81 mg/dL in the second trimester, and 0.87 mg/dL in the third trimester [15]. A serum creatinine level greater than 0.87 may indicate acute kidney injury or undiagnosed chronic kidney disease [15].
In previous years, it was believed that pregnancy might worsen kidney function in patients with underlying CKD [16]. Due to their worsening effects on kidney function, glomerular diseases, especially IgA nephropathy and lupus nephritis, are potential risk factors for negative pregnancy-related outcomes [17]. Considering the link between kidney function and materno-fetal morbidity, in the past women with CKD were usually advised to seek a pregnancy after a renal transplant and having achieved stable kidney function. However, this concept has evolved due to emerging evidence. It has been shown that pregnancy does not have adverse effects on renal function, especially in the early stages of CKD. A meta-analysis found no significant difference in renal outcomes between pregnant women with stage 1–3 CKD and those without CKD-complicated pregnancy [16]. A retrospective study collected clinical data from 293 pregnant women with CKD stage 3–4 between 2005 and 2016, and found that higher serum creatinine levels and proteinuria were major risk factors for adverse kidney outcomes, but pregnancy itself did not significantly affect renal function decline [18]. Another study analyzed the effects of pregnancy on renal function in 49 patients with stage 3–5 CKD and found that the rate of GFR decline did not significantly change from a baseline taken before pregnancy and a data point after delivery [19]. However, for patients with an eGFR less than 40 mL/min/1.73 m2 and 24 h proteinuria greater than 1 g, the eGFR was significantly reduced after delivery [19].
3. Dialysis and Pregnancy
Infertility in women on dialysis is a common issue with a multifactorial etiopathogenesis. End-stage kidney disease (ESKD) alters the hormonal balance in a woman’s body. CKD may cause the lack of estradiol-stimulated luteinizing hormone surge which activates the hypothalamic–pituitary axis, and may also lead to an increase in prolactin levels, causing changes in ovulatory cycles [20,21]. Low anti-Müllerian hormone concentrations in advanced stages of CKD can be used to predict infertility in CKD women, but more research is needed to establish the link between low anti-Müllerian hormone concentrations and infertility in women with CKD [22,23]. Additional factors such as decreased libido, body image disturbances, depression, the impact of uremic toxins and pharmacologic side effects from antihypertensive agents or immunosuppressants may play a role in infertility [13]. Ideally, reproductive counseling should begin in the early stages of CKD with frequent re-evaluations during follow-up visits up to the conception period, and continue thereafter. Reproductive counselling should regard the desire of the woman to become or not become pregnant and comprise a discussion on fertility and a possible pregnancy with its related risks, as well as an explanation of contraceptive methods [24]. Factors such as woman’s age, medical history and stage of CKD can impact the risks to the mother, the child and the graft [24]. Therefore, individualized counseling and risk assessment are essential for women with CKD who want to conceive [24].
In a retrospective study conducted in the United States from 2005 to 2013, researchers identified 2352 pregnancies among 47,555 women on dialysis, resulting in a rate of 17.8 events per thousand person-years—a relatively high rate compared to other studies [25]. Several factors correlated with a higher pregnancy rate, such as younger age. More interestingly, compared to diabetic nephropathy, some specific etiologies of CKD, such as glomerulonephritis, vasculitis, neoplasia, and hypertensive nephropathy, have a higher rate of becoming pregnant [25].
In a subgroup analysis on women on dialysis, it was seen that women who had a shorter time on HD had a greater chance to get pregnant [7]; time on HD correlated to better residual kidney function, which in turn increases the chances of achieving a successful pregnancy [7]. Giatras et al. showed that only 6 out of 120 women who were under dialysis treatment for 10 years had a successful pregnancy [26]. Additionally, 47% of conceptions occurred in the first years of dialysis, further strengthening this relation [26]. Regarding the dialysis modality, one study revealed that women on peritoneal dialysis (PD) treatment were less likely to get pregnant compared to women on HD [6]. In the largest survey on pregnancy in the ESKD population from the United States, only 1.1% of women with PD got pregnant compared to 2.4% of women with HD [10]. The causes for the lower likelihood of conception in women with PD remain vague, especially since PD treatment has fewer hemodynamic complications and higher preserved residual kidney function rates when compared to HD [27].
3.1. Hemodialysis for Pregnancy Maintenance
Hemodialysis is the most commonly employed dialysis modality. In the past, low-flux dialyzers were recommended to prevent rapid changes in osmolarity and the volemic status during pregnancy. It is now possible to achieve better depuration of middle molecules without rapid fluid or electrolyte fluctuations by using a combination of low ultrafiltration, more frequent dialysis, and high-flux membranes [28]. Providing a higher dialytic rhythm (5–6 times per week and/or longer than 36 h per week), adjusted for residual kidney function, can reduce the risk of polyhydramnios, hypertension, small for gestational age (SGA), prematurity, and maternal malnutrition, in addition to increasing the possibility of live birth. In a comparison of data from an intensively dialyzed cohort in Canada (22 patients, mean of 43 h weekly) versus a retrospective cohort of patients in the United States (70 patients, mean of 17 h weekly), the live birth rates were 48% for those dialyzed for less than 20 h weekly and 85% for patients dialyzed for more than 36 h weekly (n = 13) [29]. Nocturnal HD is an intensive dialysis modality that has been shown to offer more clinical benefits compared to other modalities [30]. According to Marques et al., ultrafiltration rates of 6–8 mL/kg/h during HD sessions did not have any serious negative effects on fetal middle cerebral, placental, and umbilical artery blood flow [31]. Although evidence for adjusting renal-replacement therapy to target a specific BUN threshold is not strong, some experts suggest aiming for a BUN target of less than 35 mg/dL (12.5 mmol/L) [32]. In pregnant women with residual kidney function, the physician should prescribe the dialytic regimen (see Table 1) according to urine output (>1 L), time on dialysis (<1 year), and most importantly mid-week pre-dialysis urea (<35 mg/dL) [32]. However, to achieve a successful pregnancy, the physician must evaluate not only biochemical parameters but also obstetric parameters such as fetal growth and amniotic fluid volume. Due to the high intensity of electrolyte exchanges in the HD regimen, it is recommended to use dialysate with potassium 3.00 mmol/L, calcium 1.50 mmol/L, and high bicarbonate (28–32 mmol/L) [33]. Frequent dialysis sessions may lead to a decrease in magnesium levels, which is associated with hypertensive disorders of pregnancy and uterine contraction. Therefore, oral supplementation of magnesium may be necessary [29,34]. Heparin is considered safe for use during dialysis sessions in pregnant women as it does not cross the blood–placenta barrier [32]. It may be difficult to distinguish excess fluid gained between dialysis sessions from weight gain due to pregnancy-associated weight gain throughout the pregnancy. Dry weight is expected to increase by approximately 0.5 kg/week during the second and third trimesters [35]. Ultrafiltration goals should be adjusted according to the patient’s clinical situation and blood pressure to avoid hypotension and hypertension episodes. While the effects of hypotension on fetal outcomes may not be as severe as previously thought [35,36], the primary focus during dialysis should be to minimize hemodynamic instability. The CHAP study showed that the treatment of mild chronic hypertension resulted in a decrease in adverse pregnancy outcomes [36]. During the gestational period, it is recommended to transition to in-hospital hemodialysis for better multidisciplinary medical surveillance.
3.2. Peritoneal Dialysis for Pregnancy Maintenance
Conception is thought to be difficult to achieve in PD patients due to a potential barrier posed by the PD fluid for normal ovum migration [34]. According to data from the ANZDATA study, theconception rate in PD is half those in HD [6]. However, PD creates a more stable uterine micro-environment, as it avoids in the uterine niche and its large fluctuations of fluids, build-up of uremic toxins and electrolytes imbalances, whilst keeping positive systemic effects of hemodynamic stability and avoidance of anemia, also considering there is no requirement for systemic heparinization in PD. The more stable the intrauterine metabolic environment, the lower the risk of complications such as polyhydramnios, SGA and premature labor. These conditions are more likely to occur with elevated urea levels before an HD/PD session. Possible complications associated with PD include catheter obstruction, exit-site infection, as well as catheter and peritoneal membrane infections. Intensive dialysis can be provided through larger-volume and high-intensity cycles. There is no defined guideline for target Kt/V values for pregnancy on PD in the literature. In continuous ambulatory peritoneal dialysis (CAPD), increasing volumes are not preferable, so the dialytic prescription should focus on increasing the number of cycles rather than increasing the exchange volume, particularly during the third trimester [35]. On the other hand, in automated peritoneal dialysis (APD), the dialysis prescription should be based on increasing the total volume and prolonging time, which can be achieved by using small dwell volumes and increasing the number of exchanges [35]. A 2015 Italian study recommended that nephrologists take a patient-centered approach, avoiding hemodynamic instability and managing PD cycles as required by the overall clinical status, rather than solely following clearance values [37].
4. Pregnancy in Kidney Transplant Recipients
Kidney transplantation is the best way to restore fertility and reproductive function in women with advanced CKD requiring kidney replacement therapy [38]. In recent years, there has been an increase in the pregnancy rate among kidney transplant recipients (KTRs) [38,39]. However, although the probability of a successful pregnancy in KTR is ten times higher than in dialysis patients, it remains a challenge both in terms of graft and patient outcomes as well as delivery and fetal outcomes [40]. Compared with the general population, pregnancy in KTR is associated with higher rates of preeclampsia, cesarean section (C-section), preterm delivery, SGA, neonatal deaths, and stillbirths [40]. Maternal and fetal outcomes are affected by factors such as graft function, serum creatinine, proteinuria, and hypertension, which are all routinely evaluated by kidney transplant centers before allowing a planned pregnancy in a KTR [39,41]. Guidelines recommend delaying pregnancy for 1 to 2 years after kidney transplantation [8,14,42]. Due to the use of immunosuppressive drugs, it is also recommended to take prophylaxis and early and aggressively treat bacterial and viral infections [43]. The most common infection in this regard is urinary tract infection [43]. Although the risk of cytomegalovirus infection is low, it is important to monitor its impact because of its potential effects on the fetus such as congenital hearing loss, microcephaly, mental retardation, and perinatal death [43]. Herpes simplex is another virus that increases the risk of abortion and neonatal morbidity due to perinatal infection. Therefore, antiviral treatment and cesarean delivery are recommended [43].
In kidney transplant recipients who seek pregnancy, certain medications must be discontinued. Mycophenolate mofetil, for example, should be discontinued at least six weeks before conception due to the increased risk of spontaneous miscarriage and fetal abnormalities. Similarly, rituximab should not be used due to the risk of neonatal B cell depletion and unknown long-term outcomes. Sirolimus and everolimus also lack sufficient safety data, and should be avoided [8]. Other immunosuppressive drugs, such as azathioprine and calcineurin inhibitor (CNI), may still be used, but require careful monitoring [44]. Azathioprine dosages should be adjusted according to leucocyte levels, while CNI dosages should be increased by 20–30% in the first trimester due to variations in pharmacokinetics and pharmacodynamics [44]. It is recommended that patients be monitored weekly or biweekly, especially during the third trimester [44].
Different studies have reported varying kidney allograft outcomes after delivery. The reported allograft rejection rate during pregnancy or 3 months postpartum ranges from 1% to 14.5% [40,42]. A reduction in kidney function is relatively common, as seen in a retrospective cohort study that followed 254 KTR women for 2 years after delivery which documented an increase of creatinine by 11–12% [44]. The antigenic stimulus produced by the fetus may cause graft rejection [43], but it is also true that pregnancy is a condition of immunological tolerance associated with lymphocyte immunosuppressive activity that promotes tolerance to the semi-allogenic fetus and may therefore aid the kidney allograft [43]. Factors such as high Scr, previous rejection history, and oscillations of blood immunosuppressive drug levels may increase the risk of allograft rejection [45]. The best way to diagnose rejection is through an allograft kidney biopsy because the small increase in Scr levels can be underestimated due to a hyperfiltration-related decrease in creatinine during pregnancy [43].
In relation to the incidence of long-term graft loss, two meta-analyses that included 4174 KT recipients and 3570 recipients showed that after 2 years post-delivery the graft loss rate was 9.2% and 8.1%, respectively [46,47]. Another meta-analysis showed that the incidence of long-term graft loss was higher after 10 years postpartum, specifically 9.4% within 2 years after pregnancy, 9.2% within 2 to 5 years, 22.3% within 5 to 10 years, and 38.5% >10 years postpartum [48]. However, recent cohort studies have shown better results related to long-term kidney allograft outcomes after delivery [49,50]. Van Buren demonstrated that although the reduction of kidney function after the first pregnancy was estimated to 2.8 mL/min/1.73 m2, the slope eGFR did not significantly decrease after the first, second, and third pregnancy compared to pre-pregnancy eGFR [49]. Another cohort study showed that the rate of graft loss at 5 years and 10 years post-delivery was 3.1% and 12.5%, respectively [50]. According to the authors, most patients had stable normal kidney function and no proteinuria before conception, and had regular follow-ups at the outpatient clinic, which may explain these good results [50].
5. Pregnancy-Related Problems
5.1. Hypertension
The target blood pressure should be <140/90 mmHg (Table 2) [51]. Hypertension is one of the most common symptoms associated with complicated pregnancies, present in approximately 6–8% of pregnancies [52]. Pre-eclampsia and HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count) are often seen in these hypertension-complicated pregnancies. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers should not be used during pregnancy due to their teratogenic effects but may be resumed after delivery. Captopril, enalapril, and quinapril are not present in breast milk and can be given until 6 weeks of amenorrhea [53]. Diuretics are not recommended because pregnant women are dialyzed almost daily, and fluid removal is best achieved by careful ultrafiltration. Antihypertensives that can be used safely during pregnancy include labetalol, methyldopa, and nifedipine [54].
5.2. Anemia
Anemia can cause serious complications for both the mother and child, even though dilutional anemia is part of normal pregnancy physiology. All recommendations are based on expert opinion because there is no evidence-based data for the treatment of anemia in pregnant women with CKD. The use of erythropoiesis-stimulating agents (ESAs) (pregnancy category C) is generally necessary, and the dose may be increased up to two-fold the baseline requirement [51]. The efficacy of ESAs can be enhanced by using iron supplementation (1–15 mg/day) and folic acid (1 mg/day) [37]. It is advisable for the patient’s hemoglobin levels, hematocrit, and serum ferritin to be 10–11 g/dL, 30–35%, and 200–300 µg/mL, respectively (Table 2) [37].
5.3. Mineral Bone Disease
Pregnant women with renal dysfunction may require intensive dialysis to maintain stable electrolyte levels. Hyperphosphatemia is a common complication in this population but is rarely observed in pregnant women receiving dialysis because phosphorus is removed during the process. However, when hyperphosphatemia levels remain uncontrolled, calcium-based phosphorus binders should be prescribed. Alternative drugs such as sevelamer, lanthanum, aluminum, cinacalcet, and paricalcitol are not recommended for use during pregnancy or lactation [37].
In addition to maintaining stable electrolyte levels, the use of vitamin D during pregnancy has been shown to reduce the incidence of adverse pregnancy outcomes such as preeclampsia, prematurity, and small for gestational age (SGA) [55]. To address low levels of 1,25-dihydroxy vitamin D, the recommended dose of calcitriol is <1.5 μg/week [32]. Furthermore, to support fetal needs, oral calcium supplementation at a dosage of 1.5–2 g/day is suggested (Table 2) [10]. However, caution should be exercised when recommending calcium supplementation to pregnant women, as hypercalcemia may lead to fetal hypoparathyroidism [10].
6. Nutrition
Pregnant women with end-stage kidney disease (ESKD) commonly experience malnutrition due to the hypercatabolic effect of pregnancy and decreased appetite resulting from acidosis and urea levels. Intensive dialysis may further exacerbate certain nutritional deficiencies by removing essential water-soluble vitamins. As such, it is recommended that the usual dose of water-soluble vitamins be doubled in pregnant women receiving dialysis. In terms of dietary protein intake, pregnant women receiving dialysis should aim for 1.8 g/pre-pregnancy weight/day + 20 g/day, while caloric intake should be increased to 25–35 kcal/kg pregnant weight/day (Table 2) [56]. Nonetheless, dietary prescriptions during the gestational period should be provided by a dietitian to ensure that all essential nutritional requirements for a successful pregnancy are met.
7. Obstetric Outcomes and Fetal Care
Early recognition of pregnancy in women with ESKD can be challenging, as they may experience irregular menstrual cycles and amenorrhea while on dialysis. The kidney’s reduced parenchymal and excretory function may also hinder the detection of elevated serum concentrations of β-human chorionic gonadotropin (β-HCG), a key biomarker for pregnancy. A study has suggested utilizing a higher cutoff of 25 mlU/mL to exclude pregnancy when fertility status is unclear [57]. By doing so, clinicians may be better equipped to accurately diagnose pregnancy in ESKD patients and tailor appropriate treatment strategies to optimize maternal and fetal outcomes.
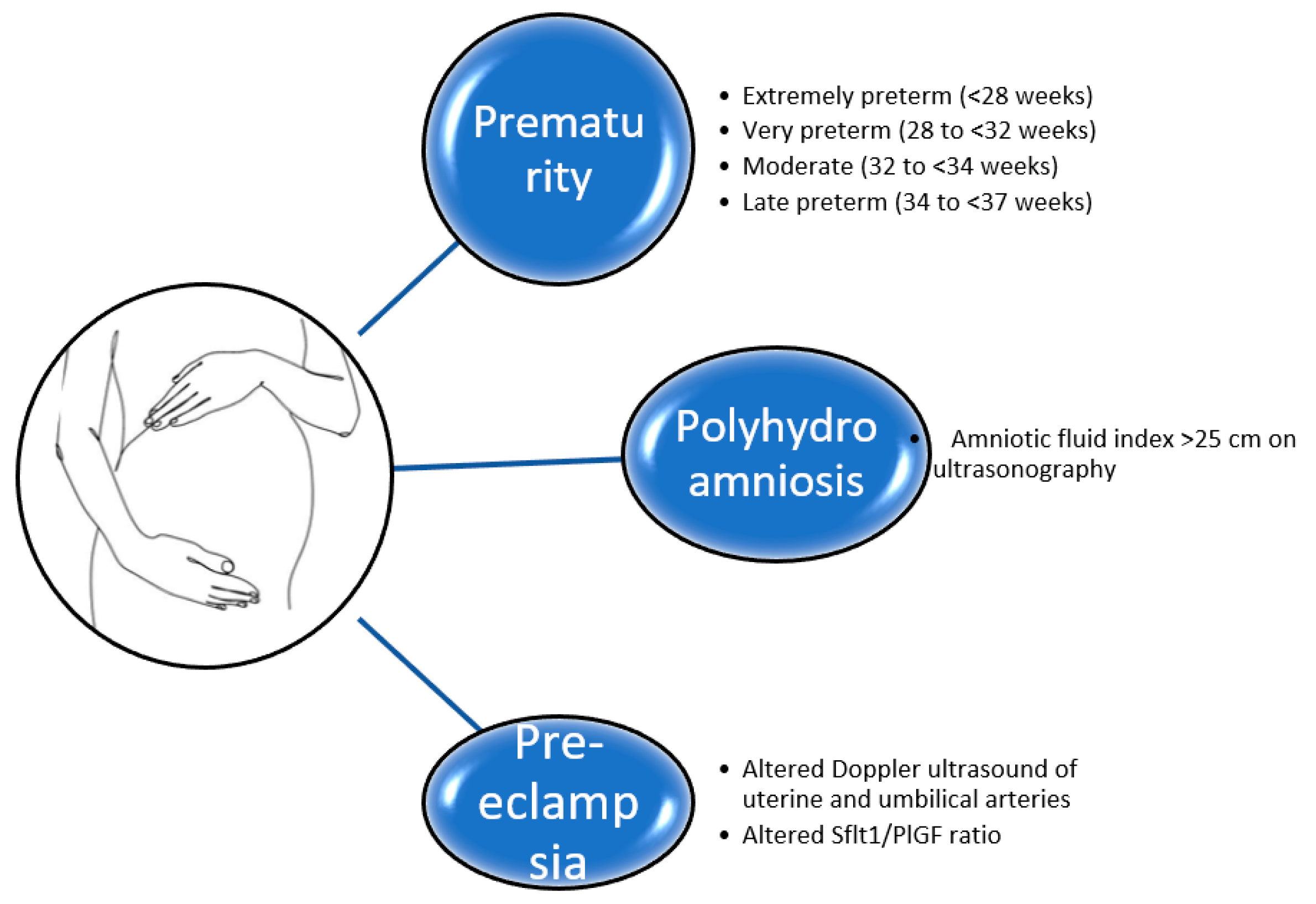
Pregnancy in women on hemodialysis (HD) is an infrequent occurrence, with reported conception rates ranging between 0.3 and 7% per year [13]. Despite advances in medical management, complications such as fetal loss, preterm birth, preeclampsia, polyhydramnios, and fetal growth restriction remain significant concerns for pregnant women on HD [13,41] (Figure 1).
Prematurity is commonly defined as a live birth before 37 weeks of gestation [58]. Preterm delivery can be further categorized based on gestational age: extremely preterm (<28 weeks), very preterm (28 to <32 weeks), and moderate to late preterm (32 to <37 weeks) [58]. The optimal delivery term is at 37 weeks of gestation, as the risk of fetal and maternal complications increases as delivery occurs earlier than this gestational age [59]. While advances in medical management have led to a reduction in complication rates, premature infants continue to experience higher rates of and more severe complications than those born at term. In pregnant patients with CKD and kidney transplant recipients (KTRs), hypertension, proteinuria, and serum creatinine levels exceeding 1.5 g/dL are considered high-risk factors for small for gestational age (SGA) infants, prematurity, and preeclampsia [60,61]. A study by Lavie et al. reported that approximately 14% of 307 pregnant women on dialysis experienced intrauterine growth restriction, and 45% experienced preterm delivery [62]. Additionally, a systematic review revealed that the incidence of SGA was higher in peritoneal dialysis (PD) patients compared to hemodialysis (HD) patients (31% versus 66.7%; p = 0.015) [49]. The review also highlighted that the more frequent the dialysis, the lower the rate of SGA and prematurity [63].
Polyhydramnios, defined as an amniotic fluid index exceeding 25 cm on ultrasonography, is a significant complication of pregnancy in women receiving dialysis. This complication occurs in a considerable proportion of pregnancies, ranging from 30% to 70% [64]. Although the precise pathophysiology of polyhydramnios is not entirely understood, it is believed that increased fetal urine production results from osmotic diuresis caused by the production of urea-rich urine [65]. Studies suggest that increasing the frequency of dialysis to reduce maternal uremia could lower fetal blood urea levels, thereby decreasing fetal osmotic diuresis [5,66]. However, a high amniotic fluid index relative to gestational age is indicative of normal fetal kidney blood flow and indirectly indicates adequate placental perfusion [66].
According to a meta-analysis, women with ESKD have a significantly higher risk of developing preeclampsia compared to women with normal kidney function. Specifically, the development of preeclampsia is ten times more likely in women with ESKD than in those without [16]. Preeclampsia is a well-known risk factor for the premature termination of pregnancy [33]. Preeclampsia is defined as the new onset of hypertension after 20 weeks of gestation in association with proteinuria and/or evidence of systemic disease, including maternal acute kidney injury, liver dysfunction, neurological features, hemolysis, thrombocytopenia, or fetal growth restriction [8]. The condition is further categorized into early onset (before 34 weeks of gestation) and late onset (after 34 weeks of gestation) [67]. However, diagnosing preeclampsia in women on dialysis can be challenging due to their pre-existing hypertension, proteinuria, and/or anuria. Regular prenatal care for pregnant women with ESKD involves periodic Doppler ultrasound assessments of flow in the uterine and umbilical arteries to monitor fetal growth after 20 weeks of gestation [68]. Abnormalities in the waveform of the umbilical artery have been utilized as a means of estimating fetal distress and assessing the possibility of preeclampsia. A retrospective study indicates that abnormal flow velocity waveform can differentiate preeclampsia during pregnancy in women with ESKD [68]. Recently, biomarkers such as Placental Growth Factor (PlGF) and soluble fms-like tyrosine kinase-1 (sFlt-1) have emerged as tools for detecting patients at high risk for pre-eclampsia. Low circulating concentrations of PlGF and/or high concentrations of sFlt-1 are recommended for predicting pre-eclampsia [69] and the necessity of delivery [70]. Wiles et al. demonstrated that high levels of PlGF (>150 pg/mL) can effectively rule out preeclampsia as a possible diagnosis with a sensitivity of 79% and specificity of 78% [71]. Conversely, the INSPIRE trial showed that the usage of continuous values of either sFlt-1/PlGF ratio or sFlt-1 alone had better predictive performance than continuous values of PlGF only and sFlt-1/PlGF cut-off at 38 [72]. However, factors that can influence the serum concentration of angiogenic and anti-angiogenic biomarkers make the diagnosis of preeclampsia challenging. Lavainne et al. reported that 2 h after the administration of heparin, serum levels of sFlt-1 and PlGF increase by 26% and 15%, respectively [73]. Despite these advances, PIGF/sFlt-1 alone is not recommended for clinical use. It is essential to highlight that the most crucial aspect of this relationship is its negative predictive value. Additionally, in the CKD population, although values exceeding 150 pg/mL may indicate a high risk of preeclampsia, they must not be interpreted as an indication for pregnancy termination.
8. Conclusions
In summary, pregnancies in women with CKD require close follow-up with a multidisciplinary approach. Special care is warranted in pregnant patients on dialysis and in KTR patients, in which respectively the dialytic prescription and medications should be reviewed. Obstetric follow-up, with serial controls of amniotic fluid index, Doppler ultrasound of uterine and umbilical arteries, and the interpretation of biomarkers sFlt-1/PIGF may identify predictive factors and may play a key role in materno-fetal outcomes.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Herwig, K.R.; Merill, J.P. Chronic renal disease and pregnancy. Am. J. Obstet. Gyn. 1965, 92, 1117–1121. [Google Scholar] [CrossRef]
- Orme, B.M.; Ueland, K. The effect of hemodialysis on fetal survival and renal function in pregnancy. Trans. Am. Soc. Artif. Intern. Organs. 1968, 14, 402–404. [Google Scholar] [PubMed]
- Confortini, P.; Galanti, G. Full term pregnancy and successful delivery in a patient on chronic hemodialysis. Proc. Eur. Dial. Transpl. Assoc. 1971, 8, 74–80. [Google Scholar]
- Reddy, S.; Holley, L. Management of the pregnant chronic dialysis patient. Adv. Chronic. Kidney Dis. 2007, 14, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Manisco, G.; Poti, M. Pregnancy in end stage renal disease patients on dialysis: How to achieve a successful deliver. Clin. Kidney J. 2015, 8, 293–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahir, A.K.; Briggs, N. An observational outcomes study from 1966–2008, examining pregnancy and neonatal outcomes from dialyzed women using data from the ANZDATA Registry. Nephrology (Carlton) 2013, 18, 276–284. [Google Scholar] [CrossRef]
- Jesudason, S.; Grace, B.S.; McDonald, S.P. Pregnancy Outcomes According to Dialysis Commencing Before or After Conception in Women with ESRD. Clin. J. Am. Soc. Nephrol. 2014, 9, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Wiles, K.; Chappell, L. Clinical practice guideline on pregnancy and renal disease. BMC Nephrol. 2019, 20, 401. [Google Scholar] [CrossRef] [Green Version]
- Harel, Z.; McArthur, E. Serum Creatinine Levels Before, During, and After Pregnancy. JAMA 2019, 321, 205–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kothari, M.; Hampton, T.D. Dialysis and Pregnancy-A Review. Int. J. Nephrol. Kidney Fail. 2019, 5. [Google Scholar] [CrossRef]
- Marcadal, L.; Nizard, J. Prepregnancy counselling and management of pregnancy in haemodialysis patients. Néphrol. Dial. Transpl. 2020, 35, 219–221. [Google Scholar] [CrossRef] [PubMed]
- Normand, G.; Xu, X. Pregnancy outcomes in French hemodialysis patients. Am. J. Nephrol. 2018, 47, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, M.; Barta, V. Pregnancy outcomes in women on hemodialysis: A national survey. Clin. Kidney J. 2017, 10, 276–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jong, M.F.C.; van Hamersvelt, H.W. Dutch Guideline Working Group on Pregnancy in CKD. Summary of the Dutch Practice Guideline on Pregnancy Wish and Pregnancy in CKD. Kidney Int. Rep. 2022, 7, 2575–2588. [Google Scholar] [CrossRef]
- Wiles, K.; Bramham, K. Serum Creatinine in Pregnancy: A Systematic Review. Kidney Int. Rep. 2018, 4, 408–419. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.J.; Ma, X.X. A Systematic Review and Meta-Analysis of Outcomes of Pregnancy in CKD and CKD Outcomes in Pregnancy. Clin. J. Am. Soc. Nephrol. 2015, 10, 1964–1978. [Google Scholar] [CrossRef] [Green Version]
- Fakhouri, F.; Schwotzer, N. Glomerular diseases in pregnancy: Pragmatic recommendations for clinical management. Kidney Int. 2023, 103, 264–281. [Google Scholar] [CrossRef]
- He, Y.; Liu, J. The pregnancy outcomes in patients with stage 3-4 chronic kidney disease and the effects of pregnancy in the long-term kidney function. J. Nephrol. 2018, 31, 953–960. [Google Scholar] [CrossRef] [Green Version]
- Imbasciati, E.; Gregorini, G. Pregnancy in CKD stages 3 to 5: Fetal and maternal outcomes. Am. J. Kidney Dis. 2007, 49, 753–762. [Google Scholar] [CrossRef]
- Holley, J.L.; Reddy, S.S. Pregnancy in dialysis patients: A review of outcomes, complications, and management. Semin. Dial. 2003, 16, 384–388. [Google Scholar] [CrossRef]
- Holley, J.L.; Schmidt, R.J. Gynecologic and reproductive issues in women on dialysis. Am. J. Kidney Dis. 1997, 29, 685–690. [Google Scholar] [CrossRef]
- Wiles, K.; Anckaert, E. Anti-Müllerian hormone concentrations in women with chronic kidney disease. Clin. Kidney J. 2019, 14, 537–542. [Google Scholar] [CrossRef] [Green Version]
- Stoumpos, S.; Lees, J. The utility of anti-Müllerian hormone in women with chronic kidney disease, on haemodialysis and after kidney transplantation. Reprod. Biomed. Online 2018, 36, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Klein, C.L.; Josephson, M.A. Post-Transplant Pregnancy and Contraception. Clin. J. Am. Soc. Nephrol. 2022, 17, 114–120. [Google Scholar] [CrossRef]
- Shah, S.; Christianson, A.L. Racial Differences and Factors Associated with Pregnancy in ESKD Patients on Dialysis in the United States. J. Am. Soc. Nephrol. 2019, 30, 2437–2448. [Google Scholar] [CrossRef]
- Giatras, I.; Levy, D.P. Pregnancy during dialysis: Case report and management guidelines. Nephrol. Dial. Transpl. 1998, 13, 3266–3272. [Google Scholar] [CrossRef] [Green Version]
- Okundaye, I.; Abrinko, P. Registry of pregnancy in dialysis patients. Am. J. Kidney Dis. 1998, 31, 766–773. [Google Scholar] [CrossRef]
- Lang, S.M.; Bergner, A. Preservation of residual renal function in dialysis patients: Effects of dialysis-technique-related factors. Perit. Dial. Int. 2001, 21, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Hladunewich, M.A.; Hou, S. Intensive hemodialysis associates with improved pregnancy outcomes: A Canadian and United States cohort comparison. J. Am. Soc. Nephrol. 2014, 25, 1103–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barua, M.; Hladunewich, M. Successful pregnancies on nocturnal home hemodialysis. Clin. J. Am. Soc. Nephrol. 2008, 3, 392–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques, L.P.J.; Marinho, P.R.S. Effect of ultrafiltration on placental-fetal blood flow in pregnancy of woman undergoing chronic hemodialysis. Hemodial. Int. 2018, 22, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Luders, C.; Titan, S.M. Risk Factors for Adverse Fetal Outcome in Hemodialysis Pregnant Women. Kidney Int. Rep. 2018, 3, 1077–1088. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, I.C.; Silva, N. Pregnancy and dialysis. J. Bras. Nefrol. 2020, 42, 349–356. [Google Scholar] [CrossRef]
- Schoenaker, D.A.; Soedamah-Muthu, S.S. The association between dietary factors and gestational hypertension and pre-eclampsia: A systematic review and meta-analysis of observational studies. BMC Med. 2014, 22, 157. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.T.C.; Kar Wah, K.F. Pregnancy and Peritoneal Dialysis: An Updated Review. EMJ Nephrol. 2018, 6, 74–84. [Google Scholar]
- Tita, A.T.; Szychowski, J.M. Chronic Hypertension and Pregnancy (CHAP) Trial Consortium. Treatment for Mild Chronic Hypertension during Pregnancy. N. Engl. J. Med. 2022, 386, 1781–1792. [Google Scholar] [CrossRef]
- Cabiddu, G.; Castellino, S. Best practices on pregnancy on dialysis: The Italian Study Group on Kidney and Pregnancy. J. Nephrol. 2015, 28, 279–288. [Google Scholar] [CrossRef]
- Saha, M.T.; Saha, H.H. Time course of serum prolactin and sex hormones following successful renal transplantation. Nephron 2002, 92, 735–737. [Google Scholar] [CrossRef]
- Gosselink, M.E.; van Buren, M.C. A nationwide Dutch cohort study shows relatively good pregnancy outcomes after kidney transplantation and finds risk factors for adverse outcomes. Kidney Int. 2022, 102, 866–875. [Google Scholar] [CrossRef]
- Koenjer, L.M.; Meinderts, J.R. Comparison of pregnancy outcomes in Dutch kidney recipients with and without calcineurin inhibitor exposure: A retrospective study. Transpl. Int. 2021, 34, 2669–2679. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Cabiddu, G. The children of dialysis: Live-born babies from on-dialysis mothers in Italy--an epidemiological perspective comparing dialysis, kidney transplantation and the overall population. Nephrol. Dial. Transpl. 2014, 29, 1578–1586. [Google Scholar] [CrossRef] [Green Version]
- Ong, S.C.; Kumar, V. Pregnancy in a kidney transplant patient. Clin. J. Am. Soc. Nephrol. 2020, 15, 120–122. [Google Scholar] [CrossRef] [PubMed]
- EBPG Expert Group on Renal Transplantation. European best practice guidelines for renal transplantation. Section IV: Long-term management of the transplant recipient. IV. 10. Pregnancy in renal transplant recipients. Nephrol. Dial. Transpl. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2002, 17, 50–55. [Google Scholar]
- Shah, S.; Verma, P. Overview of Pregnancy in Renal Transplant Patients. Int. J. Nephrol. 2016, 2016, 4539342. [Google Scholar] [CrossRef]
- Coscia, L.A.; Constantinescu, S. Report from the National Transplantation Pregnancy Registry (NTPR): Outcomes of pregnancy after transplantation. Clin. Transpl. 2010, 65–85. [Google Scholar] [PubMed]
- Zachariah, M.S.; Tornatore, K.M. Kidney transplantation and pregnancy. Curr. Opin. Organ. Transpl. 2009, 14, 386–391. [Google Scholar] [CrossRef]
- Fuchs, K.M.; Wu, D. Pregnancy in renal transplant recipients. Semin. Perinatol. 2007, 31, 339–347. [Google Scholar] [CrossRef]
- van Buren, M.C.; Schellekens, A. Long-term Graft Survival and Graft Function Following Pregnancy in Kidney Transplant Recipients: A Systematic Review and Meta-analysis. Transplantation 2020, 104, 1675–1685. [Google Scholar] [CrossRef]
- van Buren, M.C.; Gosselink, M. Effect of Pregnancy on eGFR After Kidney Transplantation: A National Cohort Study. Transplantation 2022, 106, 1262–1270. [Google Scholar] [CrossRef] [PubMed]
- Devresse, A.; Jassogne, C. Pregnancy Outcomes After Kidney Transplantation and Long-Term Evolution of Children: A Single Center Experience. Transpl. Proc. 2022, 54, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Wiles, K.; de Oliveira, L. Dialysis in pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2019, 57, 33–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beardmore, K.S.; Morris, J.M. Excretion of antihypertensive medication into human breast milk: A systematic review. Hypertens Pregnancy 2002, 21, 85–95. [Google Scholar] [CrossRef]
- Gonzales Suares, M.L.; Kattah, A. Disorders in Pregnancy: Core Curriculum 2019. Am. J. Kidney Dis. 2019, 73, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Garovic, V.D.; Dechend, R. Hypertension in Pregnancy: Diagnosis, Blood Pressure Goals, and Pharmacotherapy: A Scientific Statement from the American Heart Association. Hypertension 2022, 79, e21–e41. [Google Scholar] [CrossRef] [PubMed]
- De Regil, L.M. Vitamin D supplementation for women during pregnancy. Sao Paulo Med. J. 2016, 134, 274–275. [Google Scholar] [CrossRef] [Green Version]
- Hladunewich, M.A.; Vella, J. Pregnancy in women with nondialysis chronic kidney disease. UpToDate 2020. [Google Scholar]
- Haninger-Vacariu, N.; Herkner, H. Exclusion of pregnancy in dialysis patients: Diagnostic performance of human chorionic gonadotropin. BMC Nephrol. 2020, 21, 70. [Google Scholar] [CrossRef]
- Walani, S.R. Global burden of preterm birth. Int. J. Gynaecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef]
- Hou, S. Pregnancy in chronic renal insufficiency and end-stage renal disease. Am. J. Kidney Dis. 1999, 33, 235–252. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Venkatesan, R.L. Pregnancy outcomes in women with kidney transplant: Meta-analysis and systematic review. BMC Nephrol. 2019, 20, 24. [Google Scholar] [CrossRef] [PubMed]
- Dvořák, J.; Koucký, M. Chronic kidney disease and pregnancy outcomes. Sci. Rep. 2021, 11, 21299. [Google Scholar] [CrossRef] [PubMed]
- Lavie, A.; Czuzoj-Shulman, N. Characteristics and outcomes among pregnant women with end-stage renal disease on hemodialysis. J. Matern. Fetal Neonatal Med. 2021, 24, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Minelli, F. Pregnancy in dialysis patients in the new millennium: A systematic review and meta-regression analysis correlating dialysis schedules and pregnancy outcomes. Nephrol. Dial. Transpl. 2016, 31, 1915–1934. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Hladunewich, M.A. Chronic Kidney Disease and Pregnancy. Obstet. Gynecol. 2019, 133, 1182–1194. [Google Scholar] [CrossRef]
- Vecchio Bruno, C.R.; Del Negro, V. Dialysis on Pregnancy: An Overview. Women 2021, 1, 60–69. [Google Scholar] [CrossRef]
- Luders, C.; Castro, M.C.M. Obstetric outcome in pregnant women on long-term dialysis: A case series. Am. J. Kidney Dis. 2010, 56, 77–85. [Google Scholar] [CrossRef]
- Phipps, E.; Prasanna, D. Preeclampsia: Updates in Pathogenesis, Definitions, and Guidelines. Clin. J. Am. Soc. Nephrol. 2016, 11, 1102–1113. [Google Scholar] [CrossRef] [Green Version]
- Piccoli, G.B.; Gaglioti, P. Pre-eclmasia or chronic kidney disease? The flow hypothesis. Nephrol. Dial. Tranpl. 2013, 28, 1199–1206. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, S.; Cerdeira, A.S. Meta-Analysis and Systematic Review to Assess the Role of Soluble FMS-Like Tyrosine Kinase-1 and Placenta Growth Factor Ratio in Prediction of Preeclampsia: The SaPPPhirE Study. Hypertension 2018, 71, 306–316. [Google Scholar] [CrossRef]
- Chappell, L.C.; Duckworth, S. Diagnostic accuracy of placental growth factor in women with suspected preeclampsia: A prospective multicenter study. Circulation 2013, 128, 2121–2131. [Google Scholar] [CrossRef] [Green Version]
- Wiles, K.; Bramham, K. Placental and endothelial biomarkers for the prediction of superimposed pre-eclampsia in chronic kidney disease. Pregnancy Hypertens. 2021, 24, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Kifle, M.M.; Dahal, P. The prognostic utility of soluble fms-like tyrosine kinase-1 (sFlt-1) and placental growth factor (PIGF) biomarkers for predicting preeclampsia: A secondary analysis of data from the INSPIRE trial. BMC Pregnancy Childbirth 2022, 22, 520. [Google Scholar] [CrossRef] [PubMed]
- Lavainne, F.; Meffray, E. Heparin use during dialysis sessions induces an increase in the antiangiogenic factor soluble Flt1. Nephrol. Dial. Transpl. 2014, 29, 1225–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Pregnancy outcomes in women with CKD.


{kind=link}
Table 1.
Dialysis prescription during pregnancy.
| HD Prescription during Pregnancy | |
|---|---|
| Frequency | 5–6 time/week |
| Duration of dialysis | >36 h/week (>6 h/day) |
| Dry weight | Increase by 0.5 kg/week during the second and third trimesters |
| UF rate | 6–8 mL/kg/h |
| Dialysate | K = 3 mmol/L, Ca = 1.5 mmol/L, HCO3 = 28–32 mmol/L |
| Anticoagulation | Low-dose unfractionated heparin |
HD: hemodialysis; UF: ultrafiltration.
Table 2.
Treatment of pregnancy-related problems in women with CKD according to guidelines.
| Blood pressure | Target blood pressure <140/80 Do not use Ace-I, ARB. |
| Anemia | Hgb = 10–11 gr/dL Hct = 30–35% Ferritin = 200–300 µg/mL |
| MBD | Ca supplementation 1.5–2 g/day Do not use sevelamer, lanthanum, aluminum, cinacalcet, or paricalcitol |
| Nutrition | Protein intake: 1.8 g/pre-pregnancy weight/day + 20 g/day Calories: 25–35 kcal/kg pregnant weight/day |
Ace-I: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; Hgb: hemoglobin; Hct: hematocrit; MBD: mineral bone disease; Ca: calcium.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Shehaj, L.; Kazancıoğlu, R. Pregnancy in Chronic Kidney Disease. Kidney Dial. 2023, 3, 152-162. https://doi.org/10.3390/kidneydial3020013
AMA Style
Shehaj L, Kazancıoğlu R. Pregnancy in Chronic Kidney Disease. Kidney and Dialysis. 2023; 3(2):152-162. https://doi.org/10.3390/kidneydial3020013
Chicago/Turabian StyleShehaj, Larisa, and Rümeyza Kazancıoğlu. 2023. "Pregnancy in Chronic Kidney Disease" Kidney and Dialysis 3, no. 2: 152-162. https://doi.org/10.3390/kidneydial3020013