
Acute Kidney Injury and Hypothyroidism in a Patient with CKD

Abstract
:1. Introduction
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nelson, S.R.; Phillips, A.O.; Hendry, B.M. Hypothyroidism and rhabdomyolysis in a marathon runner. Nephrol. Dial. Transpl. 1993, 8, 375–376. [Google Scholar]
- Sekine, N.; Yamamoto, M.; Michikawa, M.; Enomoto, T.; Hayashi, M.; Ozawa, E.; Kobayashi, T. Rhabdomyolysis and Acute Renal Failure in a Patient with Hypothyroidism. Intern. Med. 1993, 32, 269–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neves, P.D.M.D.M.; Bridi, R.A.; Balbi, A.; Ponce, D. Hypothyroidism and acute kidney injury: An unusual association. BMJ Case Rep. 2013, 2013, bcr2013200585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naz, A.; Issa, M. Rhabdomyolysis and Acute Renal Impairment in a Patient with Hypothyroidism: A Case Report. Case Rep. Med. 2014, 2014, 139170. [Google Scholar] [CrossRef] [Green Version]
- Ghayur, A.; Elahi, Q.; Patel, C.; Raj, R. Rhabdomyolysis-induced acute kidney injury in a patient with non-compliance to levothyroxine therapy. Endocrinol. Diabetes Metab. Case Rep. 2021, 21-0034. [Google Scholar] [CrossRef]
- Baghi, M.A.; Sirajudeen, J.; Naushad, V.A.; Alarbi, K.S.; Benshaban, N. Severe hypothyroidism-induced rhabdomyolysis: A case report. Clin. Case Rep. 2021, 9, e05107. [Google Scholar] [CrossRef] [PubMed]
- Janjua, I.; Bashir, T.; Haq, M.Z.U.; Arshad, M.F.; Sharif, M. Severe Hypothyroidism Presenting with Rhabdomyolysis in a Young Patient. Cureus 2021, 13, e13993. [Google Scholar] [CrossRef]
- Alshamam, M.S.; Gurung, D.O.; Nso, N.; Saliaj, M.; Seitaj, A. Rhabdomyolysis Secondary to Hypothyroidism: Report of a Case. Cureus 2021, 13, e12746. [Google Scholar] [CrossRef]
- Mooraki, A.; Broumand, B.; Neekdoost, F.; Amimokri, P.; Bastani, B. Reversible acute renal failure associated with hypothy-roidism: Report of four cases with a brief review of literature. Nephrology 2003, 8, 57–60. [Google Scholar] [CrossRef]
- Altay, M.; Duranay, M.; Ceri, M. Rhabdomyolysis due to hypothyroidism. Nephrol. Dial. Transplant. 2005, 20, 847–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshi, B.; Jones, D.; Rochford, A.; Giblin, L. Hypothyroidism and associated acute renal failure. J. R. Soc. Med. 2009, 102, 199–200. [Google Scholar] [CrossRef] [PubMed]
- Altay, M.; Ceri, M.; Unverdi, S.; Duranay, M. An unusual cause of acute renal failure: Hypothyroidism. Clin. Kidney J. 2010, 3, 386–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardalan, M.R.; Ghabili, K.; Mirnour, R.; Shoja, M.M. Hypothyroidism-Induced Rhabdomyolysis and Renal Failure. Ren. Fail. 2011, 33, 553–554. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Tang, L. Rare Acute Kidney Injury Secondary to Hypothyroidism-Induced Rhabdomyolysis. Yonsei Med. J. 2013, 54, 172–176. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, G.S.; Zaid, H.M.; Moloney, M. Hashimoto’s thyroiditis presenting as Hoffman’s syndrome, rhabdomyolysis and acute kidney injury. BMJ Case Rep. 2014, 2014, bcr2013203269. [Google Scholar] [CrossRef]
- Katipoglu, B.; Ates, I.; Acehan, F.; Meteris, A.; Yılmaz, N. Rhabdomyolysis case based on hypothyroidism. Endocrinol. Diabetes Metab. Case Rep. 2016, 16-0083. [Google Scholar] [CrossRef]
- Woodrow, G.; Brownjohn, A.M.; Turney, J.H. Acute on chronic renal failure and hyponatremia associated with severe hy-pothyroidism. Nephrol. Dial. Transpl. 1993, 8, 557–559. [Google Scholar] [CrossRef]
- Connor, A.; Taylor, J.E. Renal impairment resulting from hypothyroidism. NDT Plus 2008, 1, 440–441. [Google Scholar] [CrossRef] [Green Version]
- Silva, G.C.P.L.; Carneiro, J.B.; Tardelli, C.C.; Risso, M.; Ventura, M.D.M. Kidney failure in the elderly due to hypothyroidism: A case report. Sao Paulo Med. J. 2008, 126, 291–293. [Google Scholar] [CrossRef] [Green Version]
- Liakopoulas, V.; Dovas, S.; Simopoulou, T.; Zarogiannis, S.; Giannopoulou, M.; Kourti, P.; Arampatzis, P.; Eleftheriadis, T.; Stefanidis, I. Acute renal failure: A rare presentation of hypothyroidism. Ren Fail. 2009, 31, 323–326. [Google Scholar] [CrossRef]
- Patel, M.L.; Unival, R. Two unusual cases of hypothyroidism with renal dyfunction. BMJ Case Rep. 2011, 2011, bcr0120113707. [Google Scholar] [CrossRef]
- Vikrant, S.; Chander, S.; Kumar, S.; Gupta, D. Hypothyroidism presenting as reversible renal impairment: An interesting case report. Ren. Fail. 2013, 35, 1292–1294. [Google Scholar] [CrossRef] [PubMed]
- Ters, M.E.; Patel, S.M.; Norby, S.M. Hypothyroidism and reversible kidney dysfunction: An essential relation to recognize. Endocr. Pract. 2014, 20, 490–499. [Google Scholar] [CrossRef] [PubMed]
- McAninch, E.A.; Lagari, V.S. Acute-on-Chronic Kidney Injury in Thyroid Hormone Withdrawal: A Case with Possible Implications for Radioactive Iodine Planning. Case Rep. Endocrinol. 2015, 2015, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Velzen, D.M.; Kruel-Poel, Y.H.; Den Heijer, M.; Simek, S. Subacute renal injury in hypothyroidism: A case report of an unusual phenomenon. Neth. J. Med. 2018, 76, 339–342. [Google Scholar]
- Tiong, M.; Wilson, S.; Walker, R. Hypothyroidism and renal impairment: An easily missed diagnosis. Intern. Med. J. 2019, 49, 276–278. [Google Scholar] [CrossRef]
- Shakoor, M.T.; Moahi, K.; Shemin, D. Hypothyroidism-induced acute kidney injury and hyponatremia. Rhode Isl. Med. J. 2020, 103, 61–64. [Google Scholar]
- Klein, I.; Ojamaa, K. Thyroid Hormone and the Cardiovascular System. N. Engl. J. Med. 2001, 344, 501–509. [Google Scholar] [CrossRef]
- Vargas, F.; Moreno, J.M.; Rodríguez-Gómez, I.; Wangensteen, R.; Osuna, A.; Álvarez-Guerra, M.; Garcia-Estañ, J. Vascular and renal function in experimental thyroid disorders. Eur. J. Endocrinol. 2006, 154, 197–212. [Google Scholar] [CrossRef] [Green Version]
- Iglesias, P.; Díez, J.J. Thyroid dysfunction and kidney disease. Eur. J. Endocrinol. 2009, 160, 503–515. [Google Scholar] [CrossRef] [Green Version]
- Mariani, L.H.; Berns, J.S. The Renal Manifestations of Thyroid Disease. J. Am. Soc. Nephrol. 2011, 23, 22–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, G.; Mohapatra, A. Interactions between thyroid disorders and kidney disease. Indian J. Endocrinol. Metab. 2012, 16, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Allon, M.; Harrow, A.; Pasque, C.B.; Rodriguez, M. Renal sodium and water handling in hypothyroid patients: The role of renal insufficiency. J. Am. Soc. Nephrol. 1990, 1, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Montenegro, J.; Gonzalez, O.; Saracho, R.; Aguirre, R.; Gonzalez, O.; Martinez, I. Change in renal function in primary hypo-thyroidism. Am. J. Kid. Dis. 1996, 27, 195–198. [Google Scholar] [CrossRef]
- Kreisman, S.H.; Hennessey, J.V. Consistent Reversible Elevations of Serum Creatinine Levels in Severe Hypothyroidism. Arch. Intern. Med. 1999, 159, 79–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villabona, C.; Sahun, M.; Roca, M.; Mora, J.; Gómez, N.; Gómez, J.M.; Puchal, R.; Soler, J. Blood Volumes and Renal Function in Overt and Subclinical Primary Hypothyroidism. Am. J. Med. Sci. 1999, 318, 277–280. [Google Scholar] [CrossRef]
- Karanikas, G.; Schutz, M.; Szabo, M.; Becherer, A.; Wiesner, K.; Dudczak, R.; Kletter, K. Iostopic renal function studies in severe hypothyroidism and after thyroid hormone replacement therapy. Am. J. Nephrol. 2004, 24, 41–45. [Google Scholar] [CrossRef]
- Salomon, M.; Di Scala, V.; Grishman, E.; Brener, J.; Churg, J. Renal lesions in hypothyroidism: A study based on kidney biopsies. Metabolism 1967, 16, 846–852. [Google Scholar] [CrossRef]
- Cassano, C.; Fabbrini, A.; Andres, G.A.; Cinotti, G.A.; DeMartino, C.; Minio, Z. Functional, light and electron microscopic studies of the kidney in myxoedema. Eur. Rev. Endocrinol. 1964, 1, 1–10. [Google Scholar]
- Rhee, C.M.; Brent, G.A.; Kovesdy, C.P.; Soldin, O.P.; Nguyen, D.; Budoff, M.J.; Brunelli, S.M.; Kalanter-Zadeh, K. Thyroid functional disease: An under-recognised cardiovascular risk factor in kidney disease patients. Nephrol. Dial. Tranplant. 2015, 30, 724–737. [Google Scholar] [CrossRef]
- Rhee, C.M. The interaction between thyroid and kidney disease: An overview of the evidence. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 23, 407–415. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
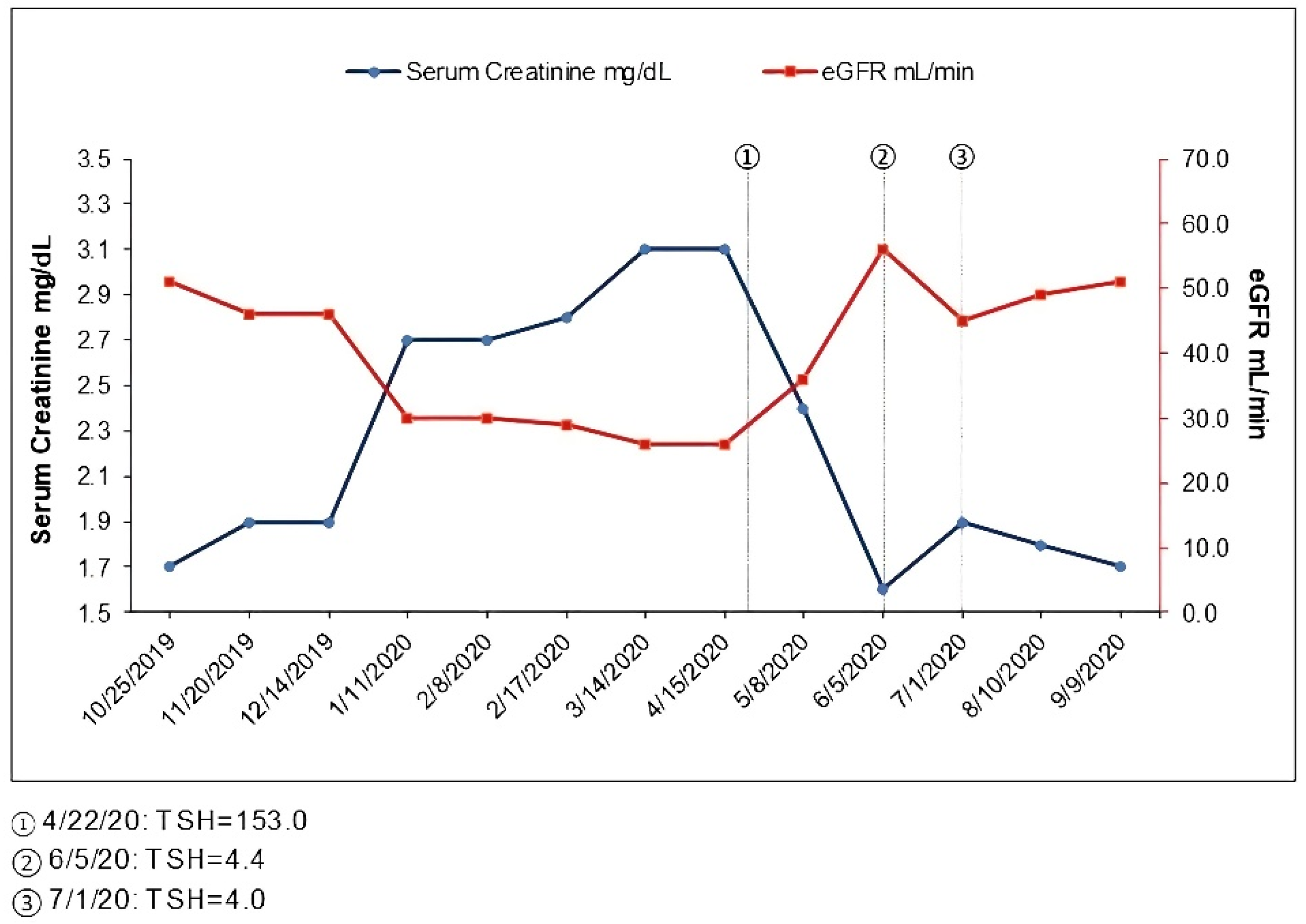
| Date | Serum Creatinine (mg/dL) | eGFR (mL/min) | TSH (mcIU/mL) |
|---|---|---|---|
| October 2019 | 1.7 | 51 | |
| November 2019 | 1.9 | 46 | |
| December 2019 | 1.9 | 46 | |
| January 2020 | 2.7 | 30 | |
| February 2020 | 2.7 | 30 | |
| February 2020 | 2.8 | 29 | |
| March 2020 | 3.1 | 26 | |
| April 2020 | 3.1 | 26 | 153.0 (22 April 2020) |
| May 2020 | 2.4 | 36 | |
| June 2020 | 1.6 | 56 | 4.4 |
| July 2020 | 1.9 | 45 | 4.0 |
| August 2020 | 1.8 | 49 | |
| September 2020 | 1.7 | 51 | |
| October 2020–August 2022 | 1.6–1.9 | 45–56 | 1.9 (March 2022) |
| 2019–2022-Urinalysis without blood or protein, no proteinuria. | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandra, P.; Haririan, A.; Drachenberg, C. Acute Kidney Injury and Hypothyroidism in a Patient with CKD. Kidney Dial. 2022, 2, 537-544. https://doi.org/10.3390/kidneydial2040048
Chandra P, Haririan A, Drachenberg C. Acute Kidney Injury and Hypothyroidism in a Patient with CKD. Kidney and Dialysis. 2022; 2(4):537-544. https://doi.org/10.3390/kidneydial2040048
Chicago/Turabian StyleChandra, Preeti, Abdolreza Haririan, and Cinthia Drachenberg. 2022. "Acute Kidney Injury and Hypothyroidism in a Patient with CKD" Kidney and Dialysis 2, no. 4: 537-544. https://doi.org/10.3390/kidneydial2040048