1. Introduction
Dexamethasone at 6 mg once per day for 10 days is the standard of care for hospitalized patients with COVID-19. The RECOVERY (Randomized Evaluation of COVID-19 thERapY) study found that steroid administration reduced death by one third in ventilated patients and by one-fifth in patients who were receiving oxygen therapy [
1]. Evidence has suggested that persons with diabetes have an increased risk of contracting COVID-19 and are more likely to suffer from severe complications and have a high mortality and morbidity risk. Innate immunity is compromised in diabetic patients. Furthermore, several physiologic changes in diabetic patients, including increased angiotensin-converting enzyme-2 and furin expression, both of which facilitate viral entry, impaired T cell function and increased interleukin-6, are all responsible for worsening disease severity [
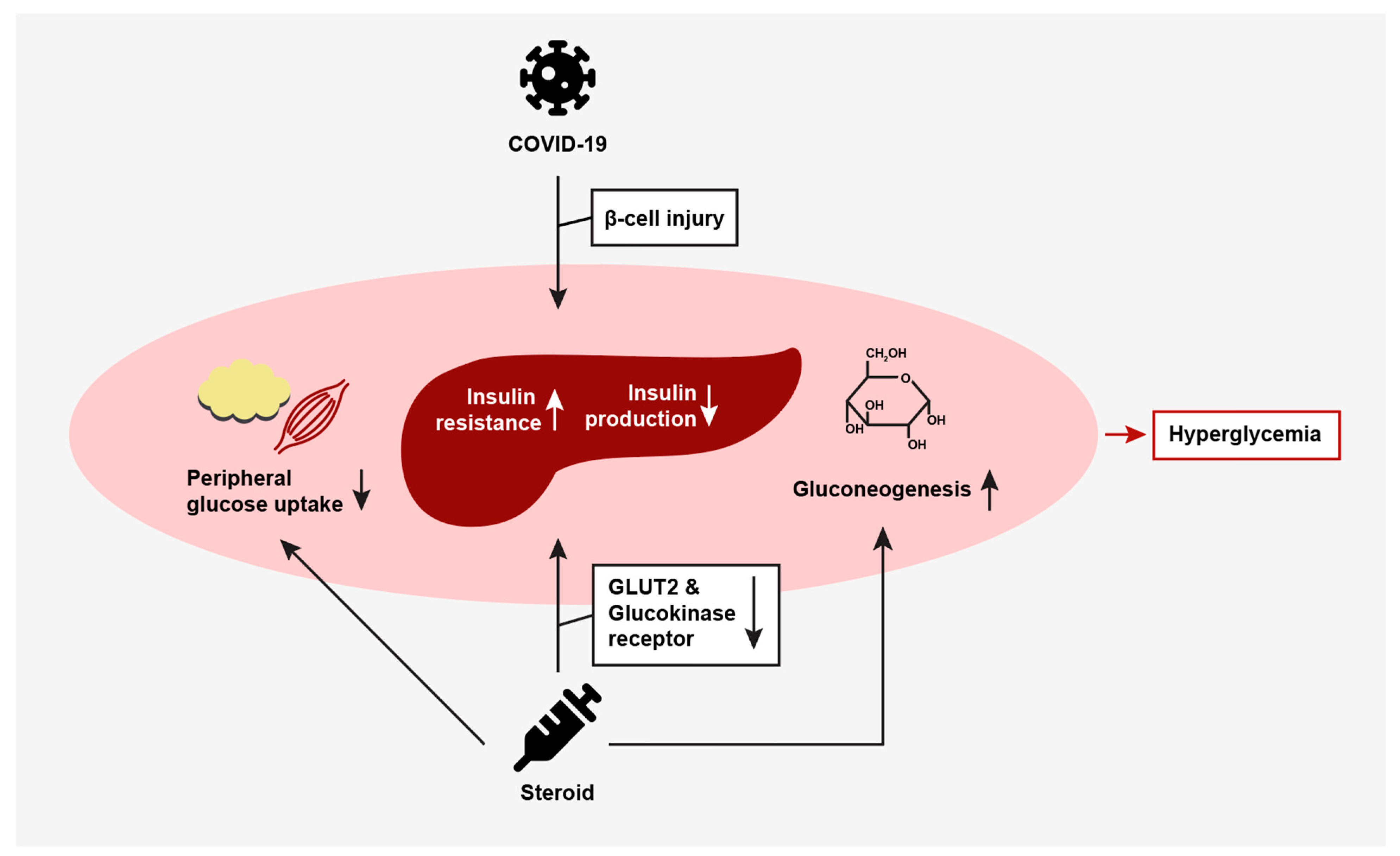
2]. COVID-19 has also been shown to induce insulin resistance and impair insulin production by directly damaging pancreatic beta cells [
3]. Treatment with dexamethasone further complicates this, especially in patients with pre-existing diabetes and those at risk of developing diabetes. Steroids exacerbate hyperglycemia, especially post-prandial hyperglycemia, and may unmask undiagnosed diabetes in those at risk of developing the disease [
4]. Steroids increase glucose production through gluconeogenesis and by enhancing the effects of glucagon and epinephrine. Steroids reduce peripheral glucose uptake at the level of the muscle and adipose tissue, and alter the production and secretion of insulin from the pancreas by reducing glucose transporter 2 (GLUT2) and glucokinase receptor expression [
5]. Ultimately, this vicious combination of COVID-19, diabetes and dexamethasone contributes to the propagation of hyperglycemia (
Figure 1).
This study will evaluate COVID-19 patients with diabetes who received the dexamethasone protocol with a focus on insulin requirements, as well as glycemic control and its effect on mortality and morbidity. There is limited research on basal and bolus insulin therapy for COVID-19 patients with diabetes on the dexamethasone treatment plan. Currently, only the United Kingdom has established research on the insulin dose adjustments for patients on the dexamethasone protocol for COVID-19. The guideline specifies using correction doses of rapid-acting insulin based on weight for initial hyperglycemia and NPH for maintaining glycemic control. In patients already on basal insulin, the guidelines indicate increasing the amount by 20–40% depending on the glucose response and titrating based on the glucose levels [
4]. In Saudi Arabia, a protocol that requires basal insulin only for those who are on insulin at home was developed for the inpatient setting. Otherwise, patients who do not use insulin at home are managed with insulin corrections only and are initiated on basal therapy if the daily requirements exceed 10 units [
6]. The hospital in our study uses the American Diabetes Association clinical practice guidelines for a weight-based regimen of basal and bolus insulin that ranges from 0.2 u/kg to 0.5 u/kg with a correction scale [
7]. A 0.5 unit/kg insulin factor is used for patients who are insulin resistant, obese patients with blood glucose greater than 200, or patients on a home insulin dose of greater than 50 units of total insulin per day. This dose is divided into basal and prandial insulin. In addition, a resistant correction scale using 3 units of insulin for every blood glucose 50 mg/dL above 150 mg/dL is added to the prandial dose. This study aims to use the hospital’s established basal/bolus weight-based protocol for inpatient insulin management to quantify and compare the actual insulin requirements in COVID-19 patients on the fixed dose of dexamethasone. Based on these data, the study will propose a new protocol for use in diabetic patients with COVID-19 that require dexamethasone therapy. Finally, this study aims to assess if glycemic management affects COVID-19 patients in terms of morbidity, as measured by the need for intensive care unit (ICU) admission, the length of hospital stay, and mortality.
2. Material and Methods
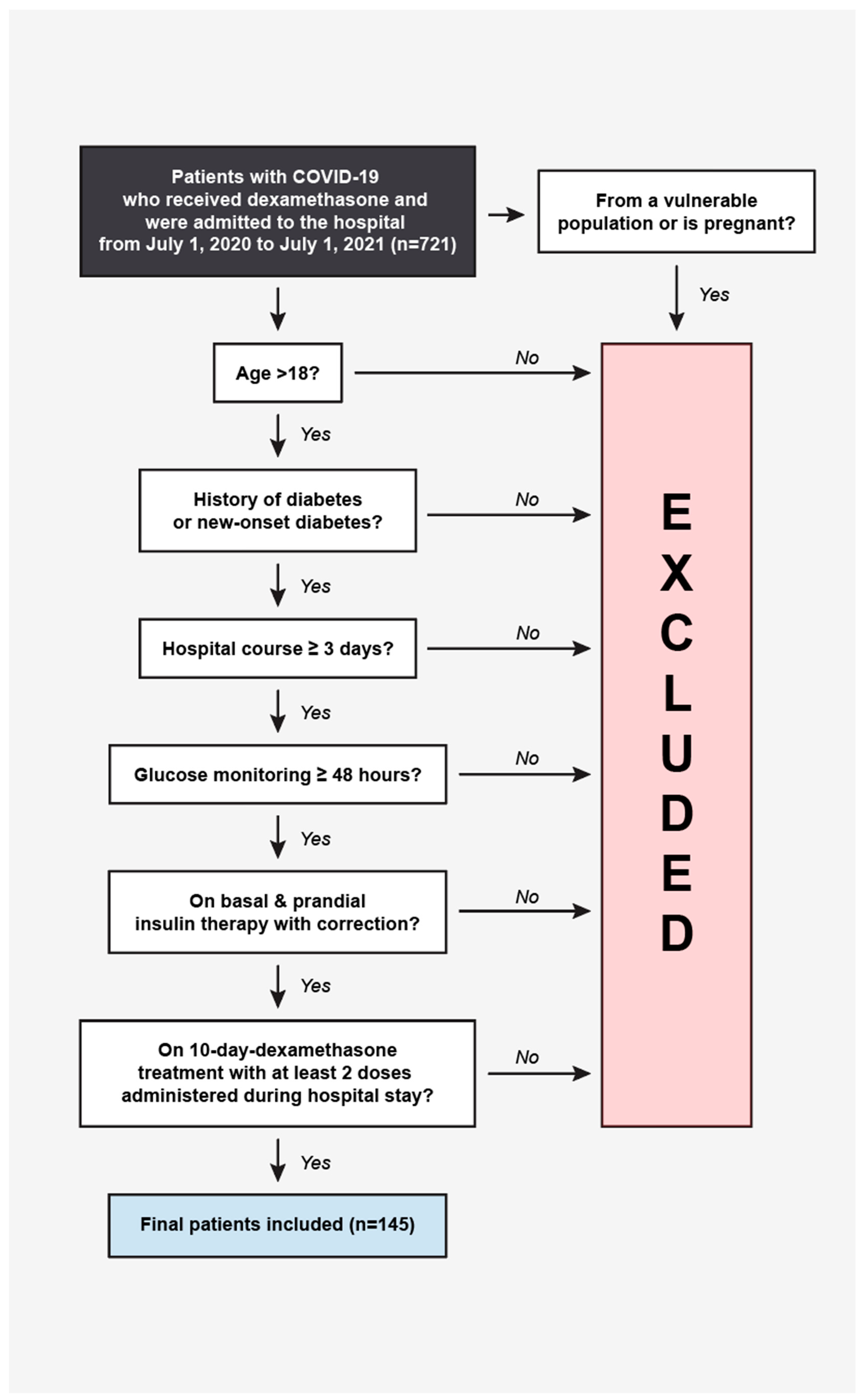
This is a retrospective cohort study from 1 July 2020 to 1 July 2021, as this represents the time when the dexamethasone protocol was initiated at this hospital. We used the hospital’s electronic health record system to obtain a list of all eligible cases. The initial review of patients with a documented diagnosis of COVID-19 who received dexamethasone and who were admitted to the hospital from 1 July 2020 to 1 July 2021 resulted in a sample size of 721 patients. We conducted a chart review of all cases to identify patients who met the inclusion criteria. The inclusion criteria had strict definitions to eliminate the potential biases that might arise from having multiple data collectors. Patients were required to be over 18 years of age with a history of diabetes or hemoglobin A1 (HgA1c) of 6.5% or greater on admission or new-onset diabetes, defined as HgA1c of 6.5% or higher or blood glucose greater than 200 mg/dL during their hospital course. They needed to be admitted to the hospital for at least 3 days, with a minimum of 48 h of glucose monitoring, and were required to be on basal and prandial therapy with correction during their hospital course. Finally, patients had to be on the 10-day dexamethasone treatment once admitted, with at least two doses of dexamethasone administration during their hospital stay. Patients were excluded if they did not fulfill the aforementioned criteria or were from a vulnerable population. Pregnant women were excluded from this study. We conducted an extensive chart view of 145 patients who were part of the final data collection (
Figure 2). The variables collected included basic demographic data, weight and height, the length of hospital stay, patient death, ICU admission, the glomerular filtration rate (GFR), admission glucose, diet (NPO, consistent carbohydrates, tube feeds or other), diabetic ketoacidosis (DKA) or hyperglycemic hyperosmolar syndrome (HHS) diagnosis, treatment for COVID-19, achievement of day glycemic control, basal, prandial and total daily doses of insulin, and hypoglycemic events. The blood glucose was monitored four times daily before each meal and at bedtime. Controlled blood glucose was defined as the average blood glucose over a 24 h period that was between 70 and 180 mg/dL and in the absence of hypoglycemia, as defined by <70 mg/dL. Uncontrolled blood glucose was defined as an average of the blood glucose over a 24 h period above 180 mg/dL or below 70 mg/dL. We assessed the total basal, prandial and daily doses of insulin on the day at which glycemic control was achieved, or if not achieved by the discharge date, then on the completion date of the dexamethasone protocol. Hypoglycemic events were recorded while patients were on the dexamethasone protocol during their hospital stay. The study was approved by the NYU-Langone Long Island Hospital Institutional Review Board.
Patients’ demographics and clinical characteristics were summarized using descriptive statistics such as the median (interquartile range) and frequency (percentage). The total basal and prandial doses were compared using the paired t-test, and change was presented as mean (95% confidence interval). Continuous variables were assessed for outliers and normality using formal statistical tests, histograms, and Q-Q plots. The insulin dose was computed using each patient’s total daily dose/weight (kg), then summarized using the mean (95% confidence interval). The percentages of patients who had expired, had ICU admission, and achieved control within 24 h were computed along with 95% confidence intervals. Logistic regression models were used to determine the factors associated with achieving control. The Akaike Information Criteria (AIC), C-statistic, and Hosmer and Lemeshow Goodness-of-Fit test were used to assess the model fit. SAS 9.4 was used for all analyses. A p-value less than 0.05 was considered statistically significant.
3. Results
There were 145 charts analyzed. The demographics are listed in
Table 1, including the differences between the uncontrolled and controlled groups. The average age is 65 years old. Female sex was associated with better control. A higher body mass index (BMI) was associated with poor control. The average hemoglobin A1c was not significantly different between the groups. Most patients received some type of treatment for their COVID-19, including, but not limited to, Azithromycin, Remdesivir or Convalescent Plasma. Most were on a consistent carbohydrate diet during the time they were on the dexamethasone protocol. There were 10 patients who developed DKA or HHS during their hospital course.
About 46% of patients achieved glycemic control with a 95% confidence interval (37.9–54.7%). The average insulin dose required was 0.67 (0.61–0.74) unit/kg. The mean total dose of insulin was 59 units. The mean total basal dose was 21 units and the mean total prandial dose was 38 units. The average prandial doses were higher than the basal doses for all participants. The uncontrolled group received 17% more prandial insulin than the controlled group, which was statistically significant (
Table 2).
We used logistic regression modeling to determine the factors associated with achieving control. Female sex and BMI < 30 were associated with achieving glycemic control, with adjusted odds ratio of 2.78 (1.29–6.01) and 0.92 (0.86–0.97), respectively. The
p-values for each were 0.009 and 0.004. The degree of uncontrolled blood glucose correlated with higher BMIs. Patients with BMIs above 35 had blood glucose levels closer to the 300 mg/dL range. Patients with BMI < 30 were more likely to achieve control using 0.6 u/kg of insulin. The relationship between the dose of insulin and BMI did not correlate once the BMI increased above 30 (
Table 3). The controlled group had a worse GFR than the uncontrolled group, as noted in
Table 1; however, after logistic regression modeling, this was not a predictor of control.
The controlled group had statistically significant longer lengths of stay, had greater ICU admissions and were more likely to die than uncontrolled patients (
Table 4).
4. Discussion
Treating steroid-induced hyperglycemia in the inpatient setting remains challenging due to significant variability in the type and duration of steroid dosing, the types of inpatient insulin regimens available, and the patient’s clinical situation and reason for admission. This is the first study using a fixed dose of steroids in the inpatient setting to assess the insulin requirements for patients diagnosed with COVID-19 on basal and bolus therapy. This study determined that patients on 6 mg dexamethasone therapy required a higher weight-based insulin dose of 0.17 u/kg, above the standard hospital regimen of 0.5 u/kg, in order to achieve tighter glycemic control. This is in line with the conclusion of a recent systemic review study by Brooks D et al.; although the insulin regimens utilized by the included studies vary widely, the insulin requirement in COVID-19 patients with dexamethasone-induced hyperglycemia consistently exceeded the standard dosing [
8]. Similar results were found in a study by Spanakis et al., who identified that noncritically ill hospitalized patients on steroids require at least 0.8 u/kg of insulin. Although our study required slightly less, our patient population is different in that it included critically ill patients who may be more sensitive to insulin. In addition, the patients in the study by Spanakis et al. were on various types and doses of steroids, resulting in more variability in their study population. Our study ensured a homogeneous study population, as all patients were on the fixed dose of dexamethasone. Spanakis et al. also determined that patients on steroids require about 30–35% of insulin to be administered as basal and about 65% to 70% to be administered as nutritional or premeal insulin [
9]. This is in agreement with our study, as patients had higher prandial requirements, almost two times the amount of basal insulin. In a study of 40 patients with known type 2 diabetes mellitus and a hematologic malignancy who received 40 mg dexamethasone orally or 8 to 12 mg via IV for 3 days, Gosmanov et al. found that the insulin requirements were increased to an average of 0.66 units/kg and uptitrated to a mean dose of 1.2 units/kg/day without the adverse outcomes of hypoglycemia [
10]. The insulin requirements here are likely higher, as patients were on higher doses of dexamethasone than in our study.
Despite aggressive therapy, a significant number of patients with COVID 19 on basal-bolus therapy still failed to achieve glycemic control in our study. Interestingly, higher total daily doses of insulin did not equate to better control. In this study, patients who achieved control required a total daily dose of 52 units compared to 63 units in patients who remained uncontrolled. Increasing insulin doses prevents further blood glucose elevations or potential complications such as DKA or HHS, but achieving control is difficult to attain in the setting of acute illness. The American Diabetes Association recommends a target glucose range of 140 to 180 in critically ill and 100 to 180 in noncritically ill patients, which is associated with decreased mortality [
7]. Klonoff et al. showed that non-ICU patients with COVID-19 who reached a glucose level of 141 to 180 within 2 to 3 days had a statistically significant lower mortality rate [
11]. The amount of insulin required to achieve glucose control, however, is often unattainable despite increasing doses. For example, Chertok Schacham et al. also found that 61% of hospitalized diabetic patients on steroids did not achieve glycemic control while on basal–bolus therapy compared to 36% of patients not on steroids who achieved glycemic control [
12]. The patients on steroids were on higher total daily doses of insulin. Our study equally found that more patients (54%) did not achieve glycemic control despite higher total daily doses of insulin.
This study did not have a control group, i.e., patients not on steroids, which is a limitation. It was designed as a retrospective cohort study, but there is tremendous value in developing a study that compares the results between a control group and an experimental group. Since our study indicates that there are other factors that contribute to achieving glycemic control and that increasing insulin does not equate to better control, future studies can consider creating a prospective, randomized controlled trial, with a control group to provide a more robust analysis of the impact of dexamethasone on insulin requirements. This will also decrease the effect of confounding factors, such as BMI, on insulin requirements.
A higher BMI is a predictor of worse glycemic control. Patients with BMI > 30 were more likely to fail at achieving glycemic control. Furthermore, the relationship between an increasing BMI and insulin requirements did not correlate as expected. Studies have established that obesity is highly prevalent in patients hospitalized for COVID-19 and has also been identified as an independent risk factor for the severity of the disease [
13]. There is no established literature on the insulin requirements for obese patients with COVID-19 on steroids. Previous studies have shown that obesity causes insulin resistance, that patients require higher total daily doses of insulin and that glycemic control is more difficult to achieve. In a study by Yki-Jarvinen et al., glycemic control deteriorated more in obese than nonobese patients in non-insulin-dependent diabetes [
14]. Determining insulin doses in obese diabetic patients on steroids with COVID-19 will continue to remain challenging due to the effects of insulin resistance propagated by the independent risk of steroid use and COVID-19-induced hyperglycemia.
A lower GFR did not hinder glycemic control. Patients with a lower GFR were able to achieve control and that was noted to be statistically significant, though this relationship was not seen after logistic regression modeling. The kidneys play a primary role in the metabolism of injected insulin. The renal clearance of insulin is dramatically reduced at a GFR less than 20 mL/min, which increases the risk of hypoglycemia in these patients [
15]. Patients in our study who achieved control had an average GFR in the mid-40s compared to normal kidney function in those who did not achieve control. We hypothesize that patients with a lower GFR had more careful titrations of insulin, which allowed these patients to achieve control. Further studies are needed to evaluate the relationship between insulin doses in patients with steroid-induced hyperglycemia and kidney disease.
This study also suggests that achieving inpatient glycemic control is not associated with improved COVID-19 outcomes. The controlled group was associated with longer length of stays, greater ICU admissions, and an increased mortality rate compared to the uncontrolled group. This is contrary to what we might hypothesize based on the effect of diabetes on the body’s immune system [
16]. The findings from other studies are conflicting. Riahi et al. found that although more advanced cases of diabetes requiring insulin therapy correlated with poorer outcomes, higher HgA1C on admission (and thus poorer outpatient glycemic control) was not [
17]. Ergenc et al. found that 72.5% of patients with HbA1C > 7% had a severe case of COVID-19, while 57.5% of patients with HbA1C < 7% had a severe case [
18]. When it comes to inpatient glycemic control specifically, Mehta et al. showed its lack of association with ICU admission, ventilator requirement, or mortality [
19]. Zhu et al., however, showed a significant association between better inpatient glycemic control and reduced medical interventions, major organ injuries, and mortality [
20]. Therefore, although our study results demonstrate that better inpatient glycemic control leads to worse COVID-19 outcomes, this could be explained by longer lengths of stay, offering more time to titrate the glucose level, and the ICU level of care, putting more focused attention on controlling glucose.
The results of this study have potentially significant clinical implications and can be incorporated into the inpatient glycemic management protocol of our hospital. The current protocol does not include patient populations on steroids or COVID-19-positive patients. Using the existing protocol, this patient population will only receive 0.5 u/kg of insulin at maximum, which is significantly less than the proposed minimum of 0.6–0.7 u/kg of insulin. The strength of this study is that it includes a strict inclusion and exclusion criteria, which allowed for a homogeneous study population that has not been documented in the existing literature. This helped strengthen both the internal validity and external validity of the study. This study, however, did not have a control group for patients not on steroids to fully elucidate the differences in the insulin requirements between the two groups. A prospective study is necessary to fully test whether a dose of 0.6–0.7 u/kg is required for patients with COVID-19 who start the dexamethasone protocol. Additionally, a future study looking at the insulin requirements for steroid-induced hyperglycemia in COVID-19 patients on dexamethasone in the outpatient setting would be useful to help manage patients outside of the hospital. Other suggestions include a future study demonstrating the physiologic mechanism behind the increased insulin needs of patients on dexamethasone.




{kind=link}
{kind=link}