


Assessing the Impacts of COVID-19 and Social Isolation on Mental Health in the United States of America
 , , and
, , and
Abstract
:1. Introduction
1.1. COVID-19 in the United States of America
1.2. Anxiety and Depression in the United States of America
2. Materials and Methods
2.1. Data
2.2. Model Formulation
3. Results
3.1. Vector Error Correction Model Results
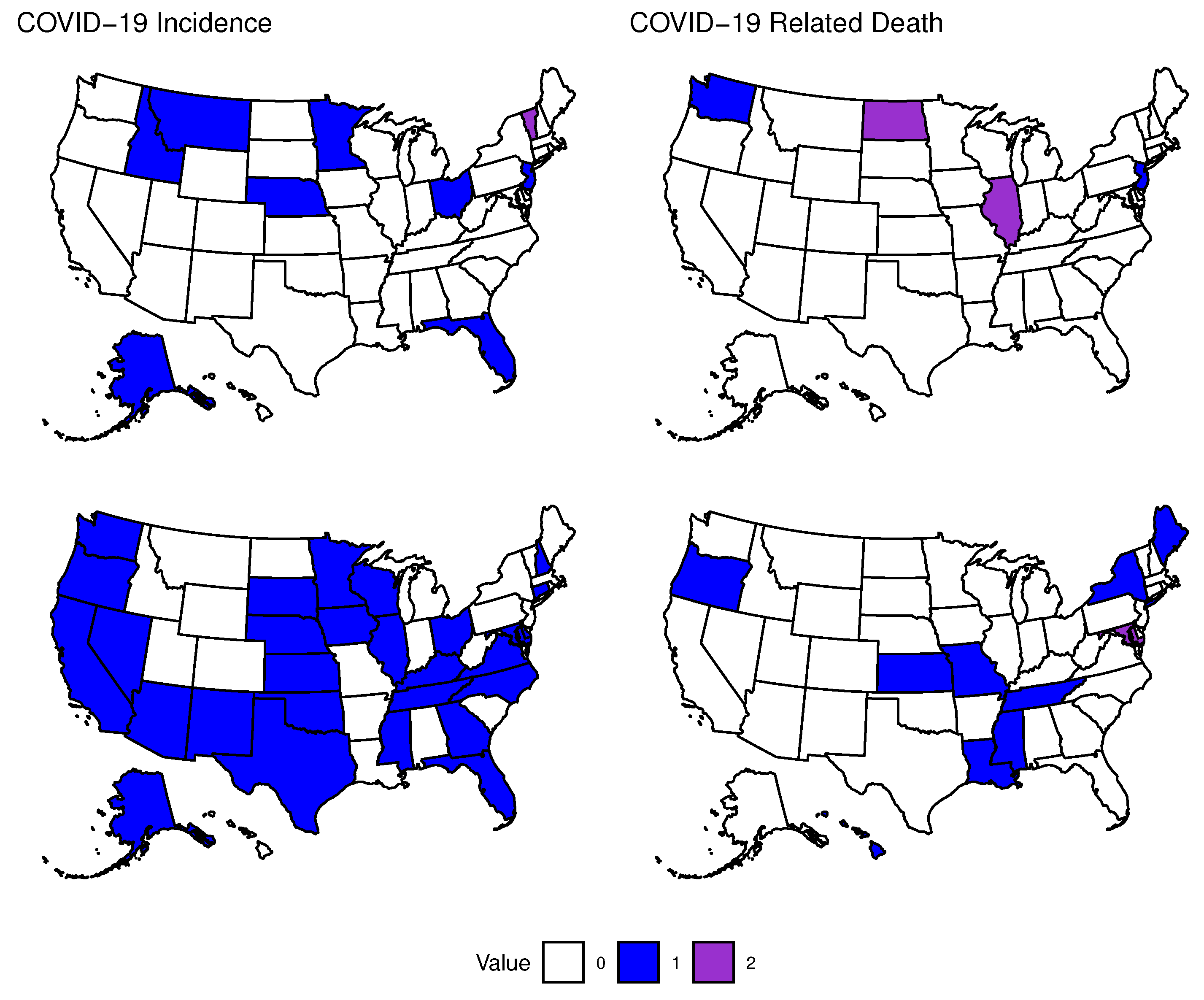
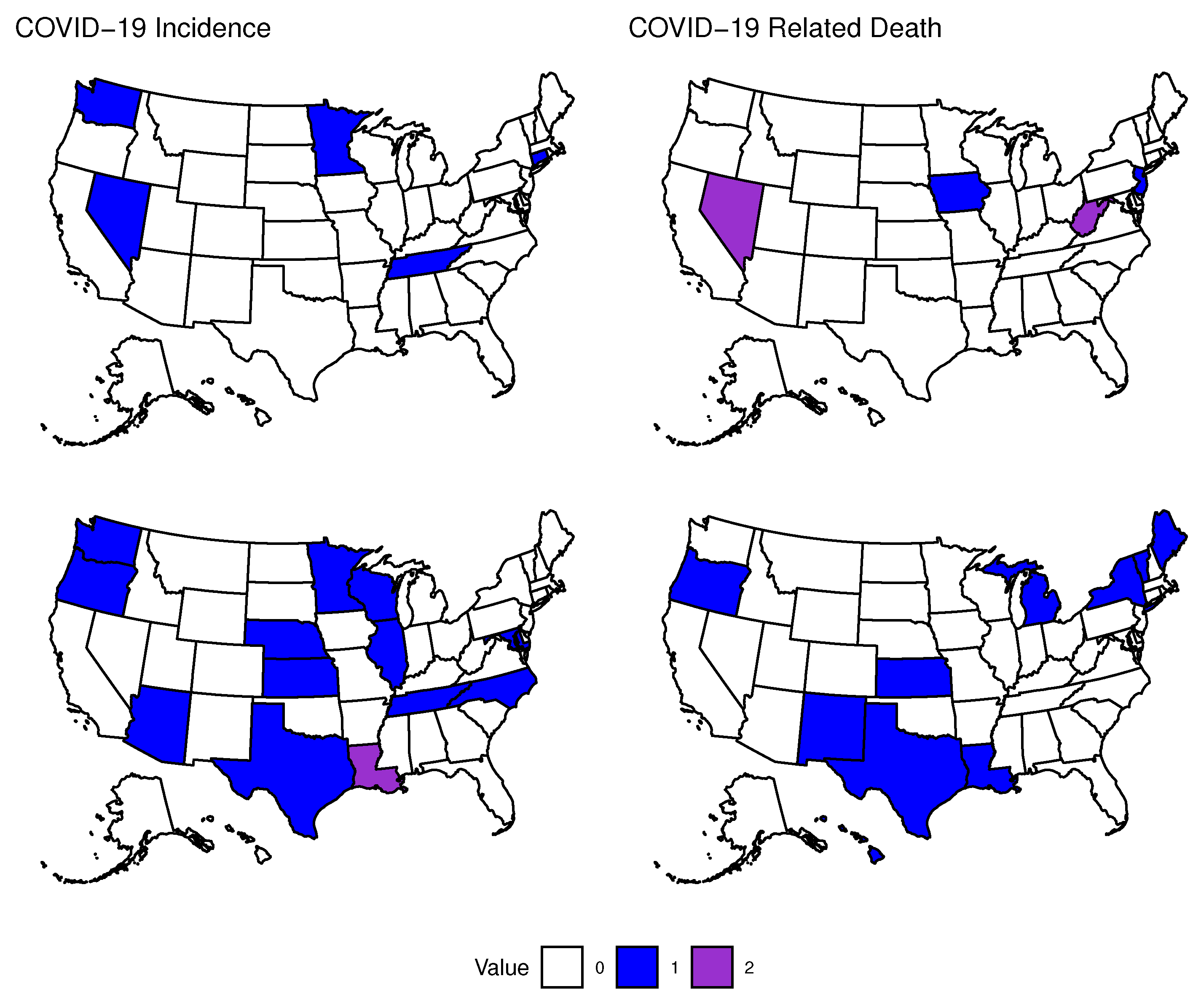
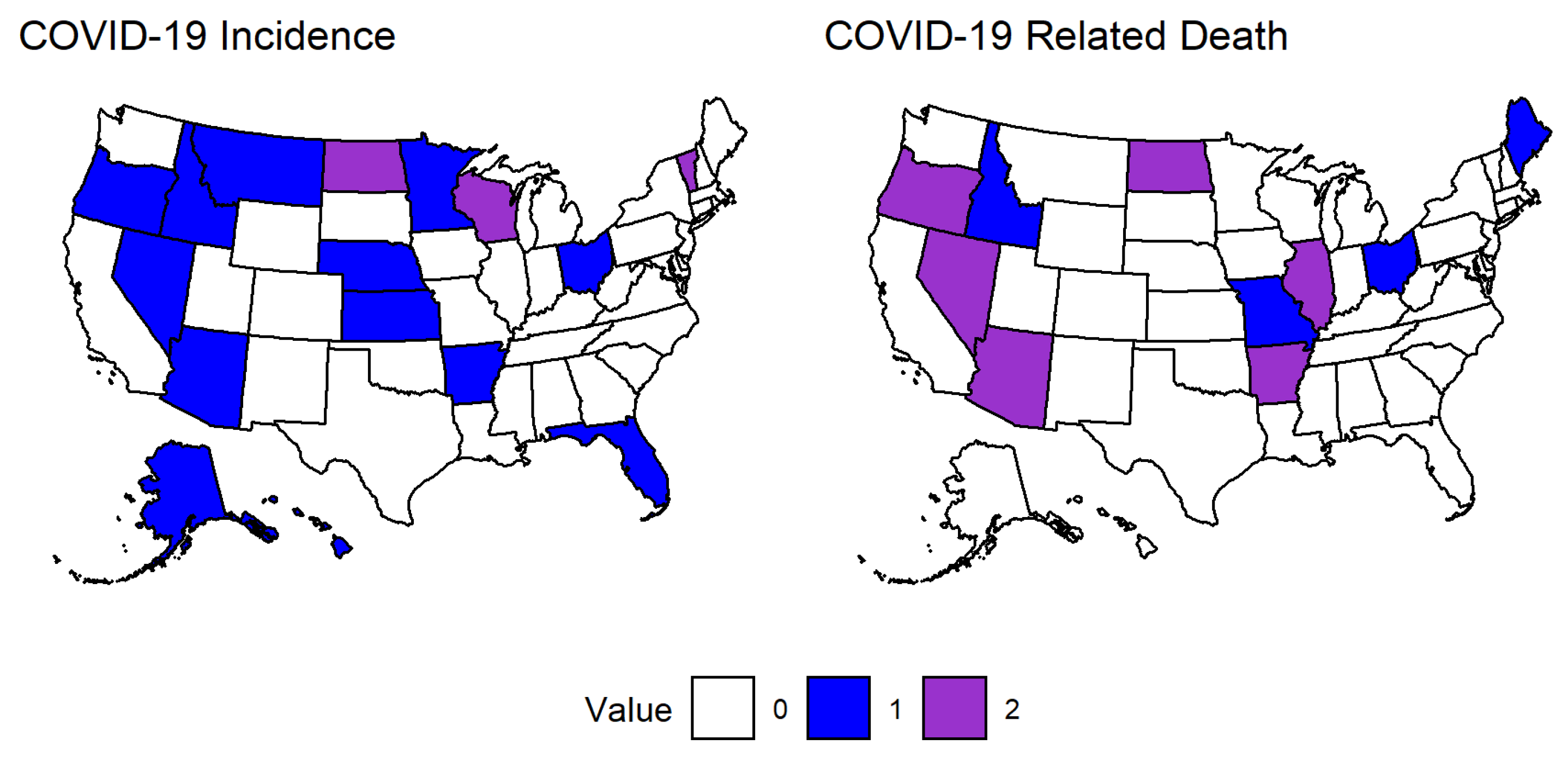
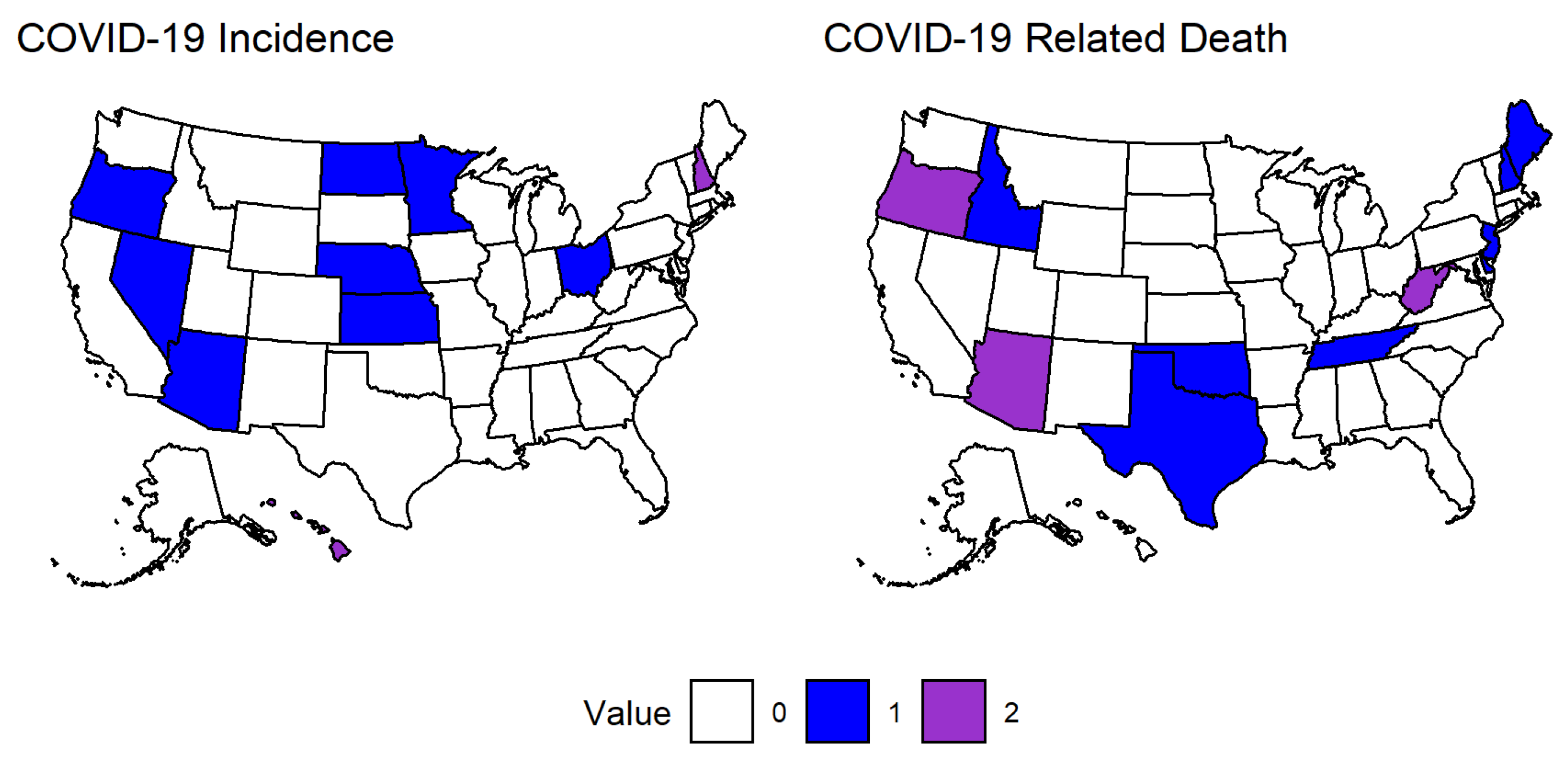
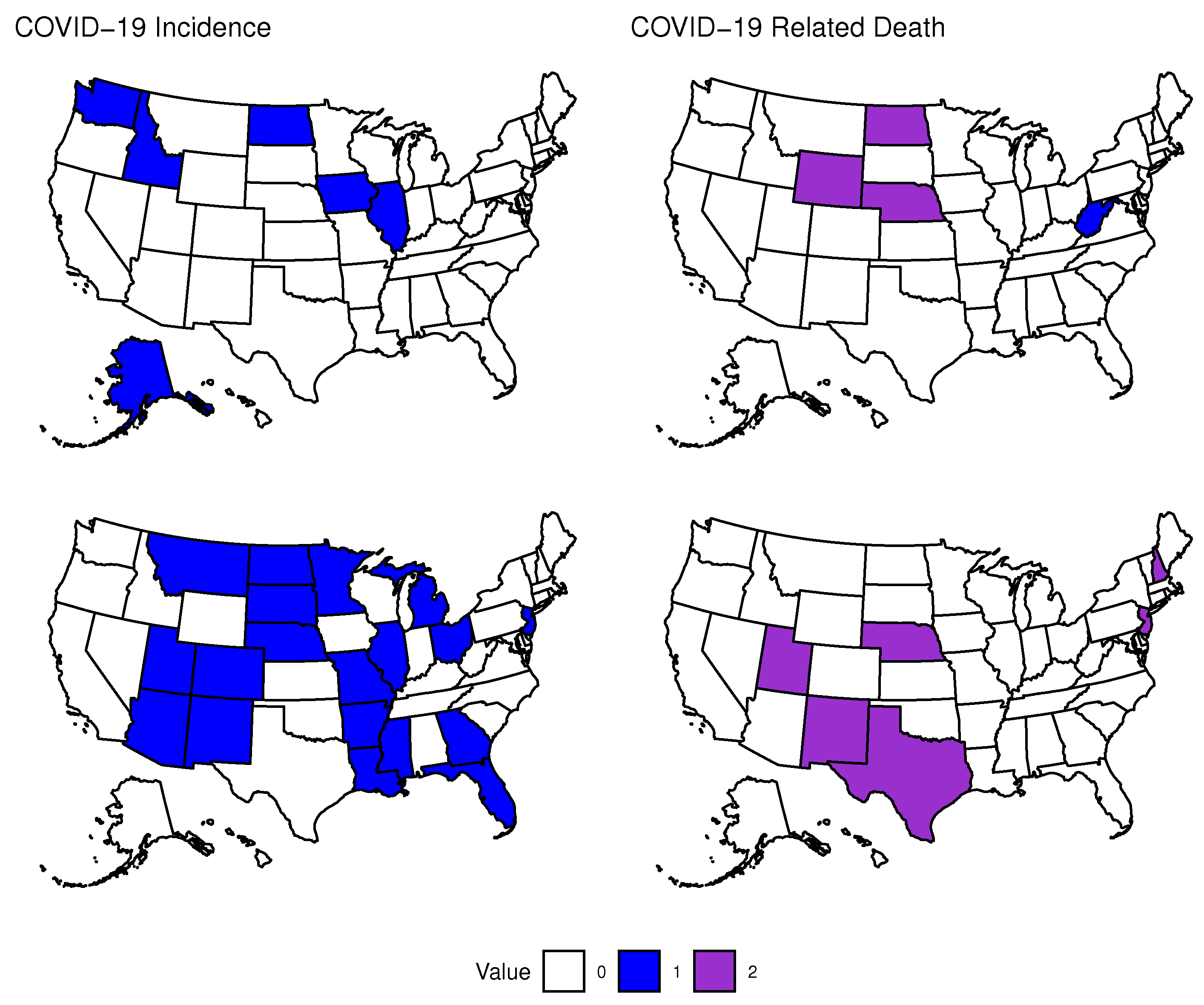
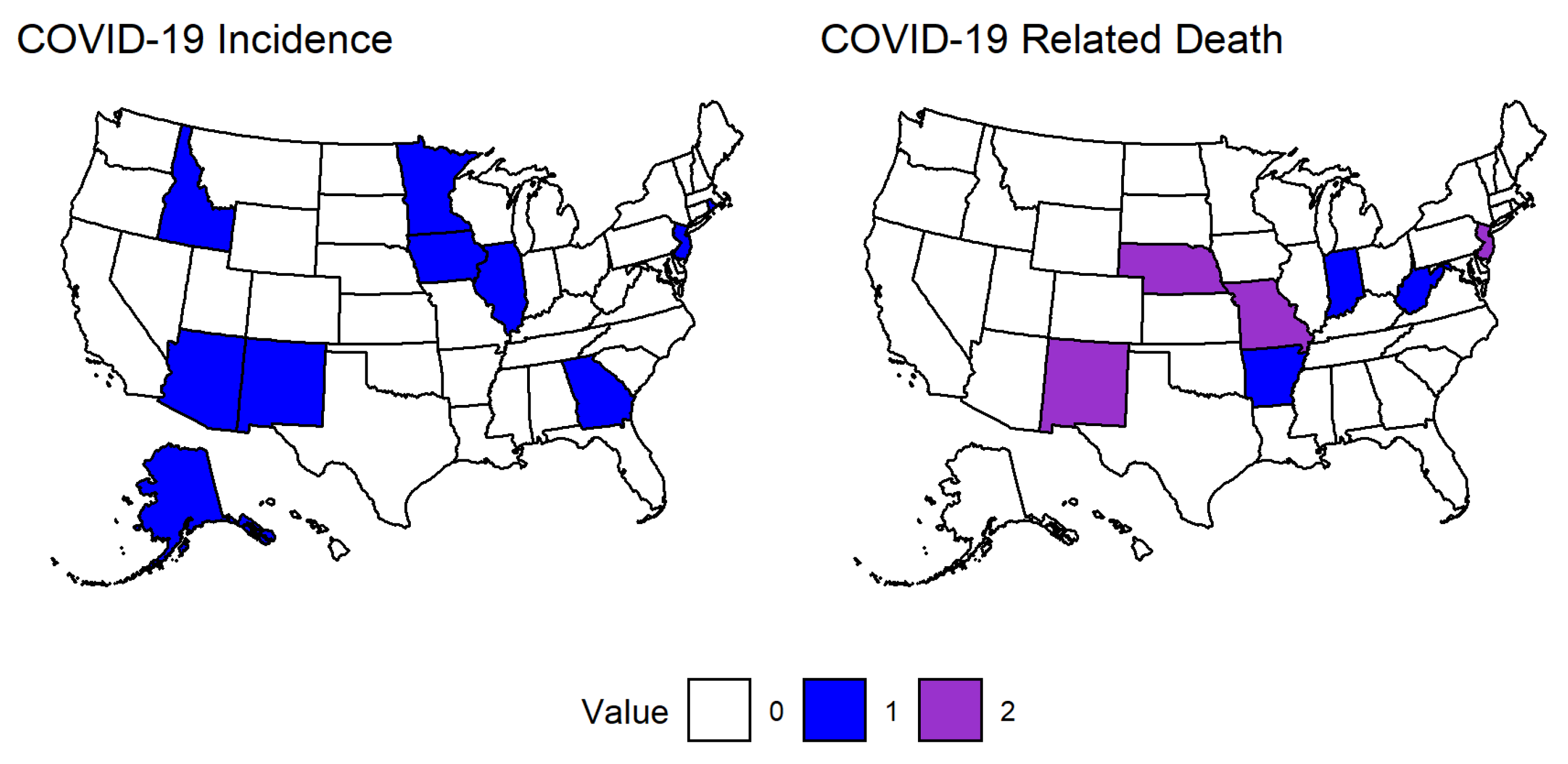
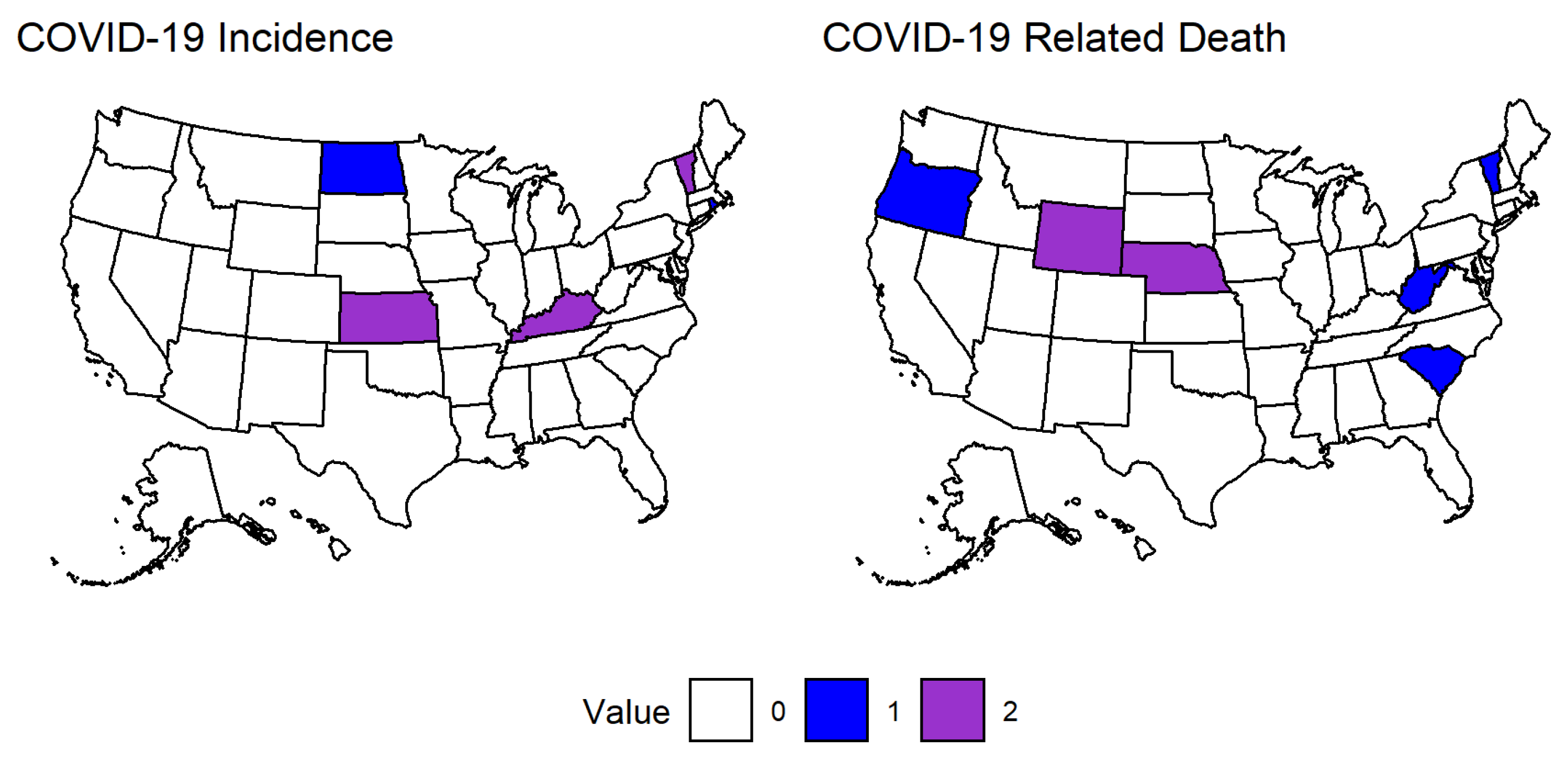
3.1.1. Effects of COVID-19 in the Second Time Period
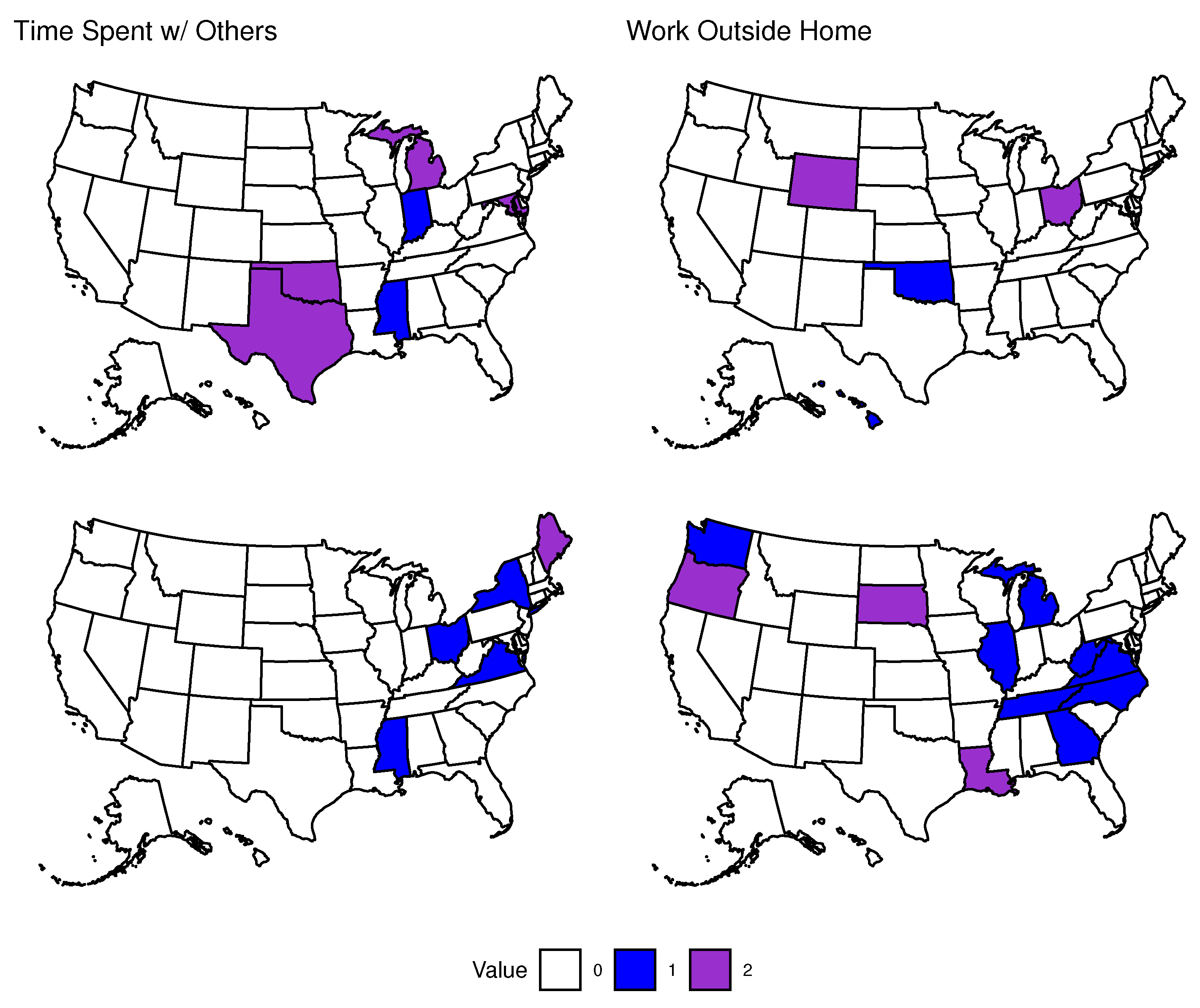
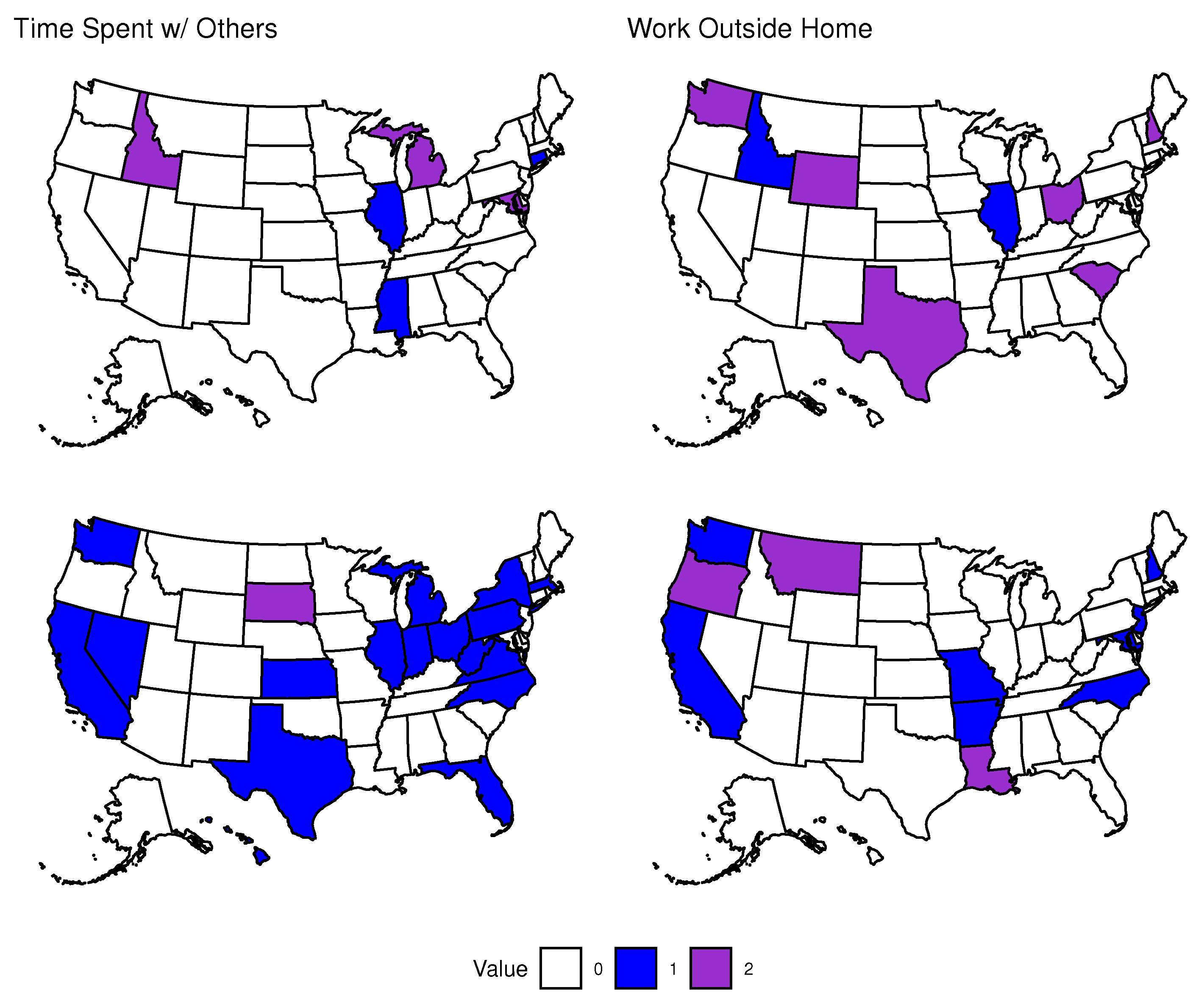
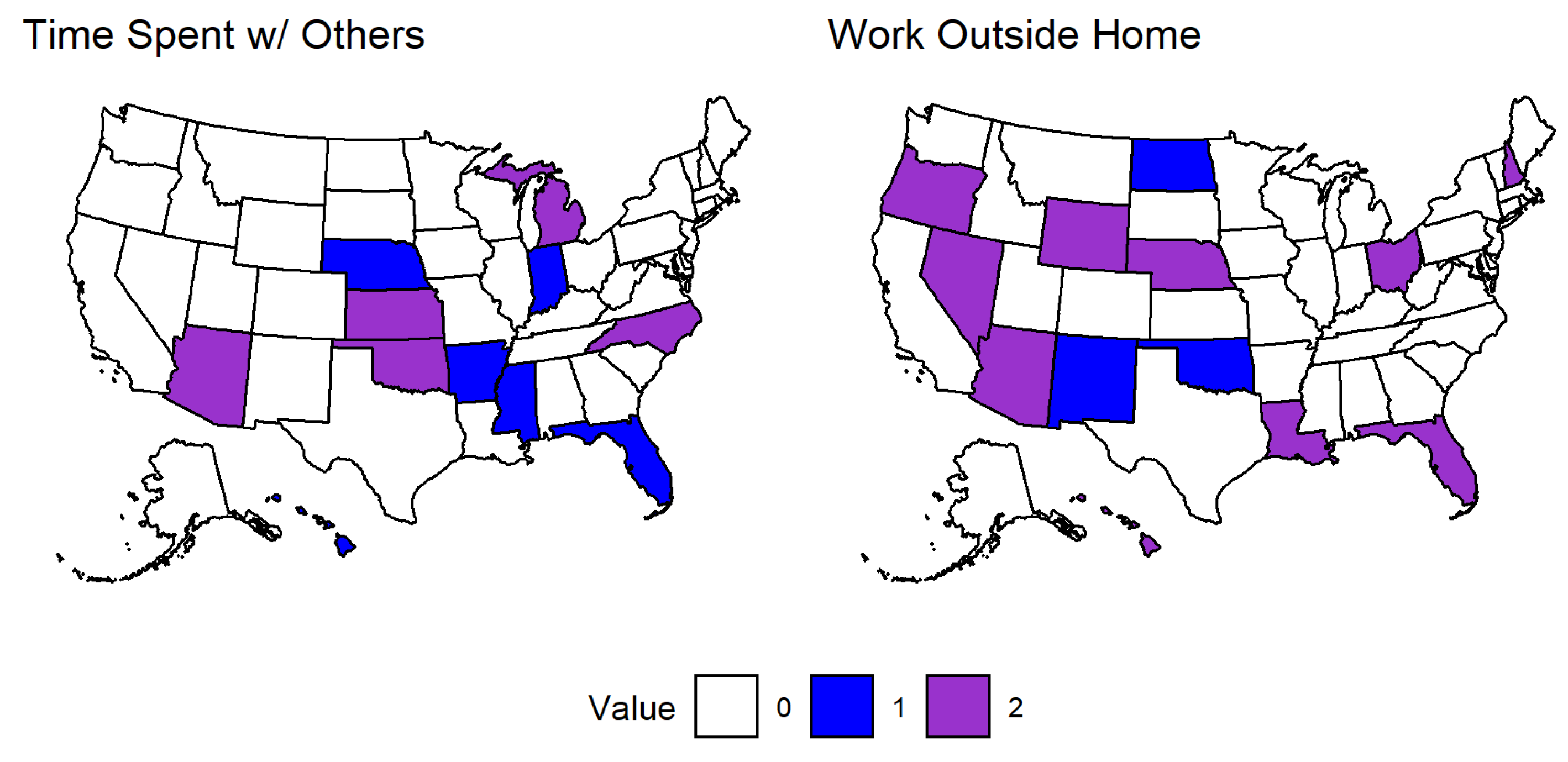
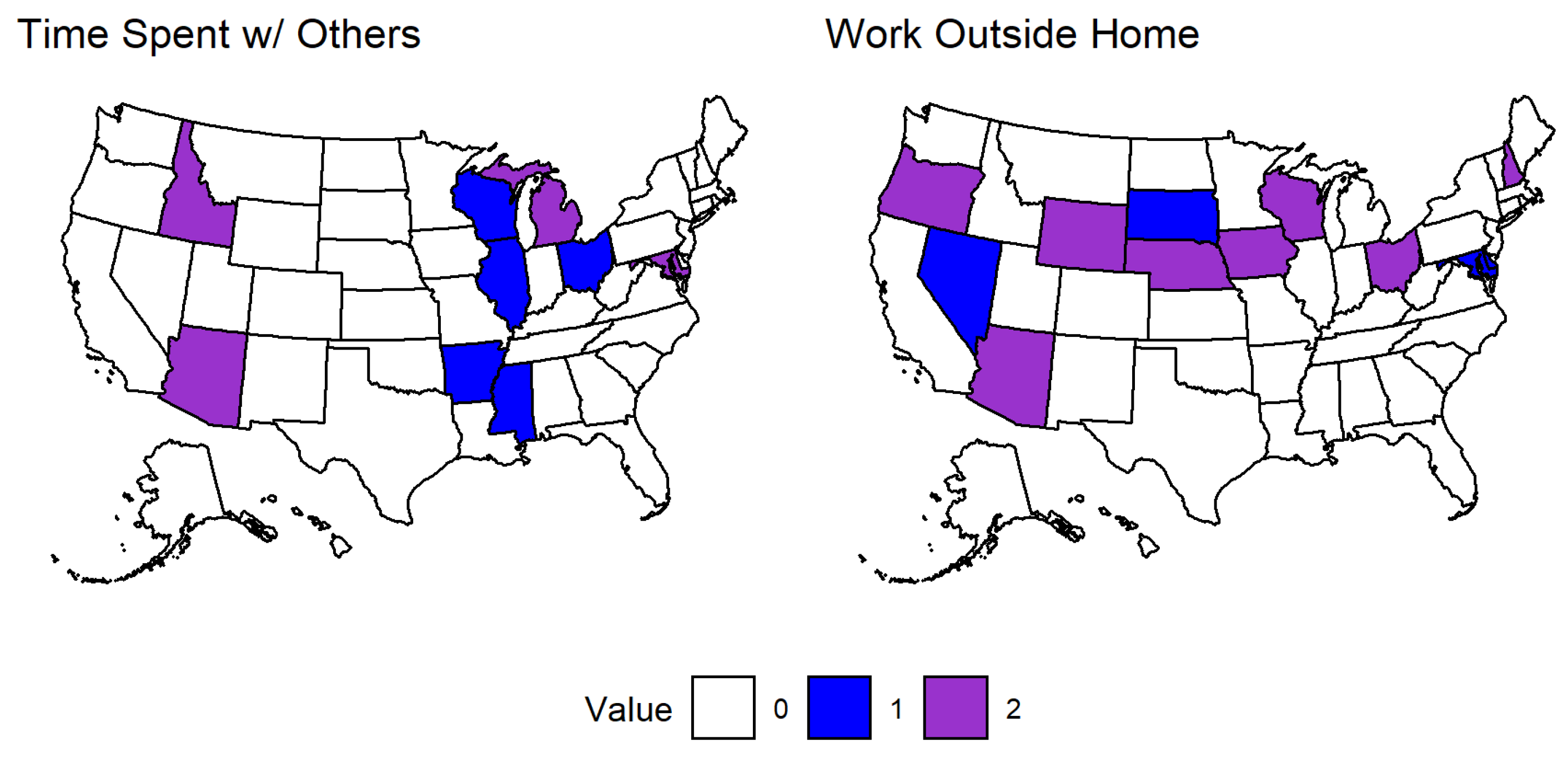
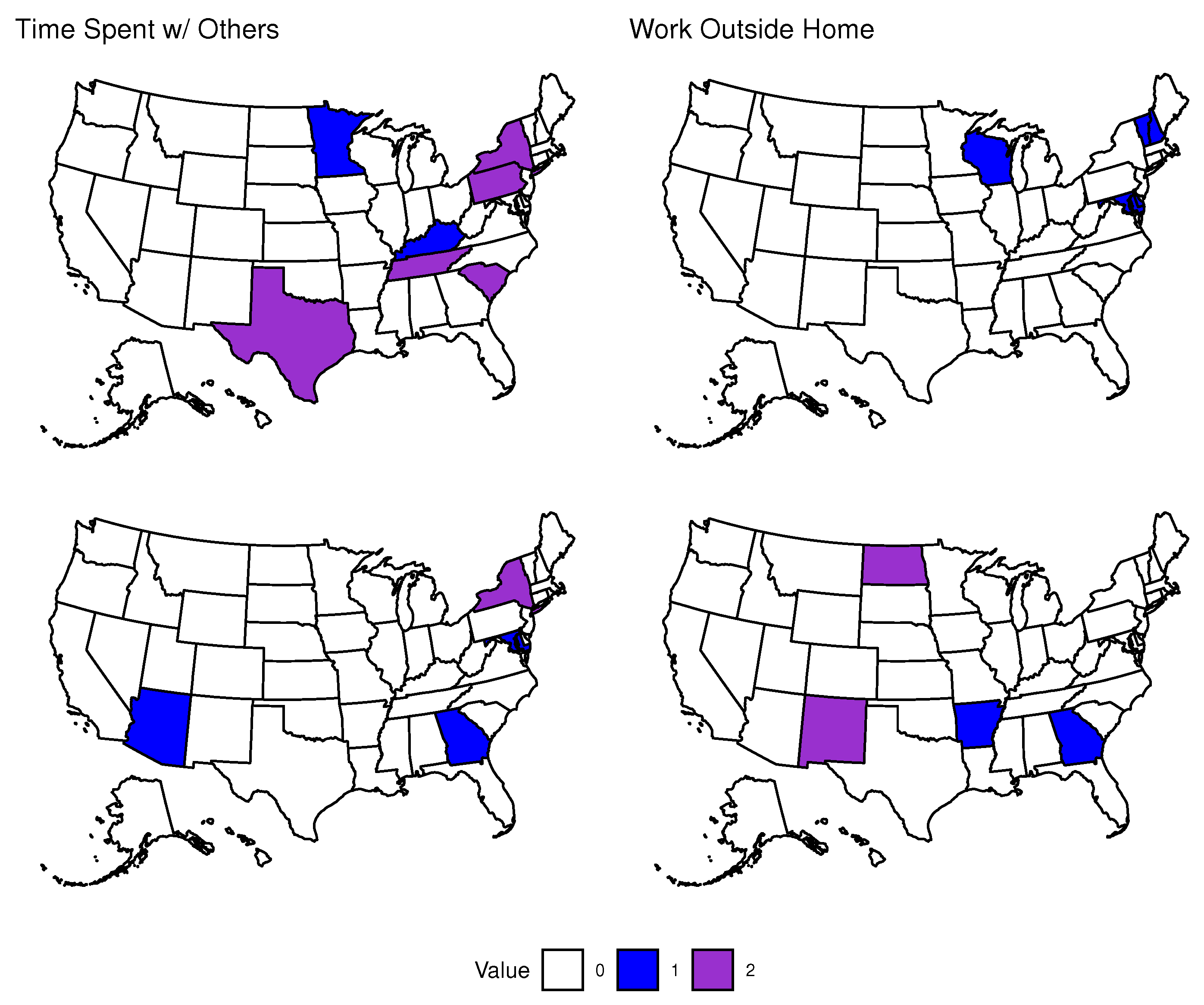
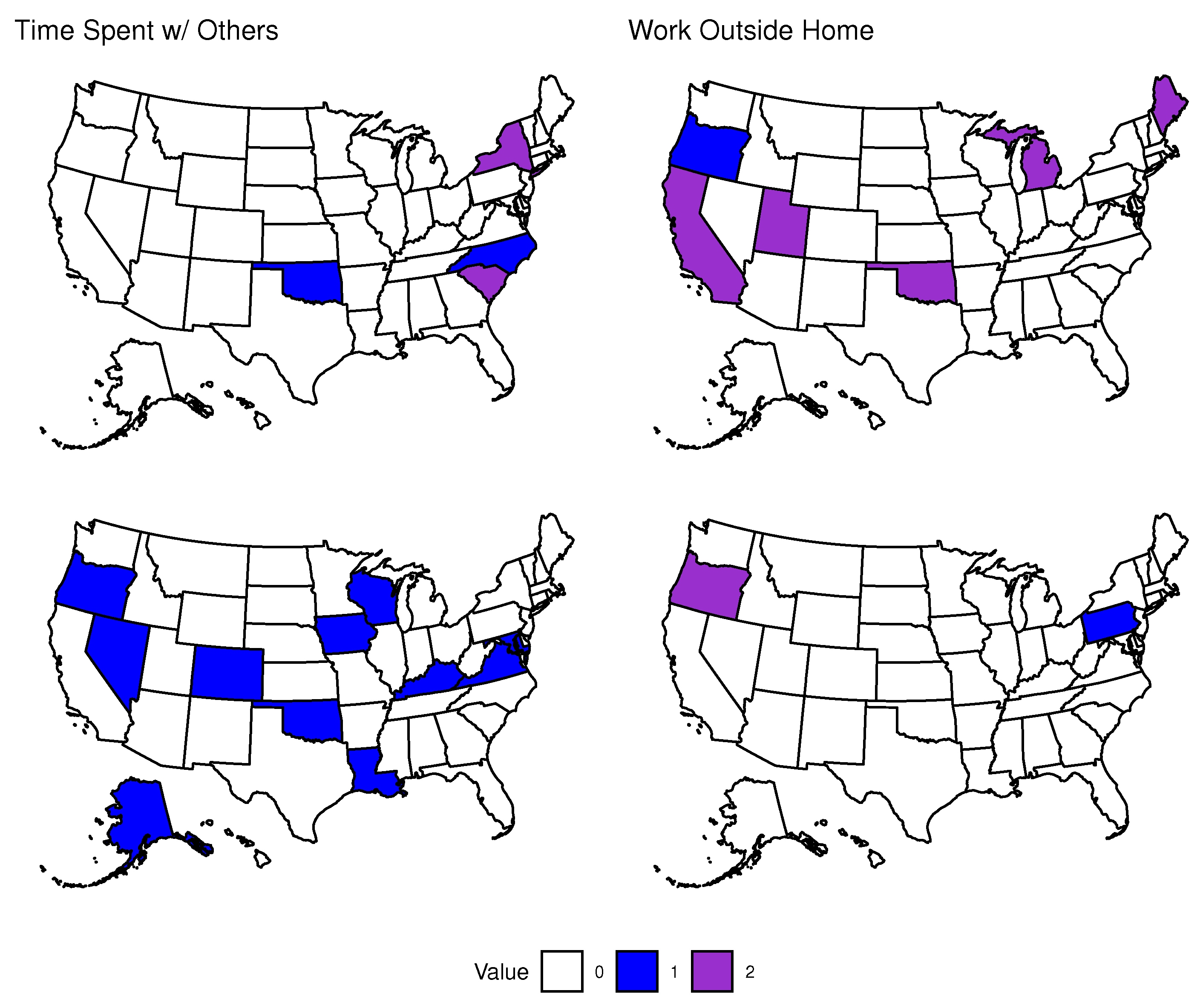
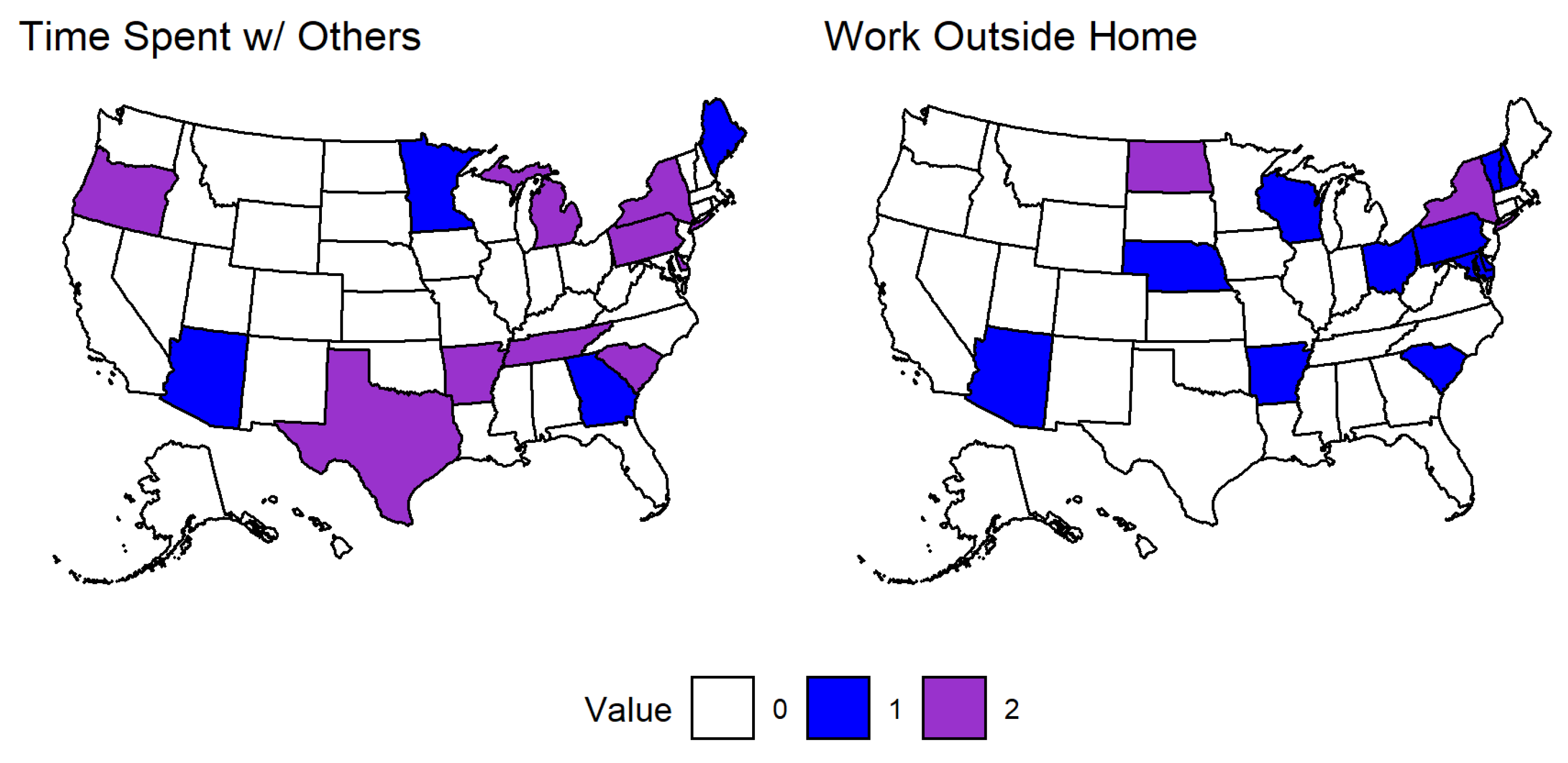
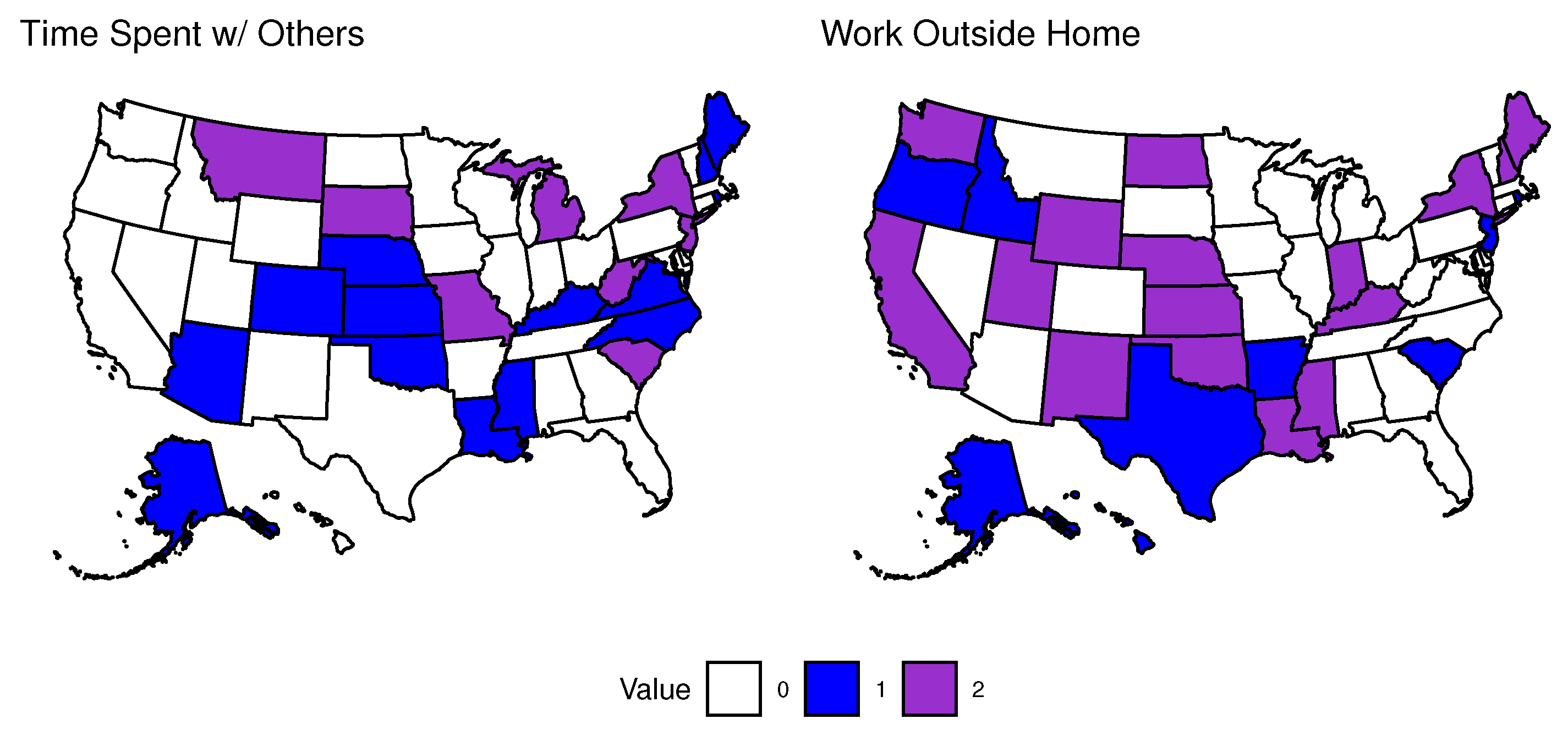
3.1.2. Effects of Social Isolation in the Second Time Period
3.2. Impulse Response Function Results
Effects of COVID-19 in the Second Time Period
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. VECM Equation Example

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Meaning |
|---|---|
| Estimated percentage of respondents who reported feeling nervous, | |
| anxious, or on edge for most or all of the past 5 days. | |
| Estimated percentage of respondents who reported feeling depressed | |
| for most or all of the past 5 days. | |
| Estimated percentage of respondents who spent time with someone | |
| who is not currently staying with you in the past 24 h. | |
| Estimated percentage of respondents who worked or went to school outside | |
| their home in the past 24 h. | |
| Number of new confirmed COVID-19 cases per 100,000 population per day. | |
| number of new confirmed COVID-19 deaths per 100,000 population per day. | |
| j-th coefficient of the i-th equation. | |
| constant associated with the i-th equation. |
Appendix B. Results of the First Time Period
Appendix B.1. Effects of COVID-19 in the First Time Period


Appendix B.2. Effects of Social Isolation in the First Time Period


Appendix B.3. Impulse Response Function Results
Appendix B.3.1. Effects of COVID-19 in the First Time Period


Appendix B.3.2. Effects of Social Isolation in the First Time Period


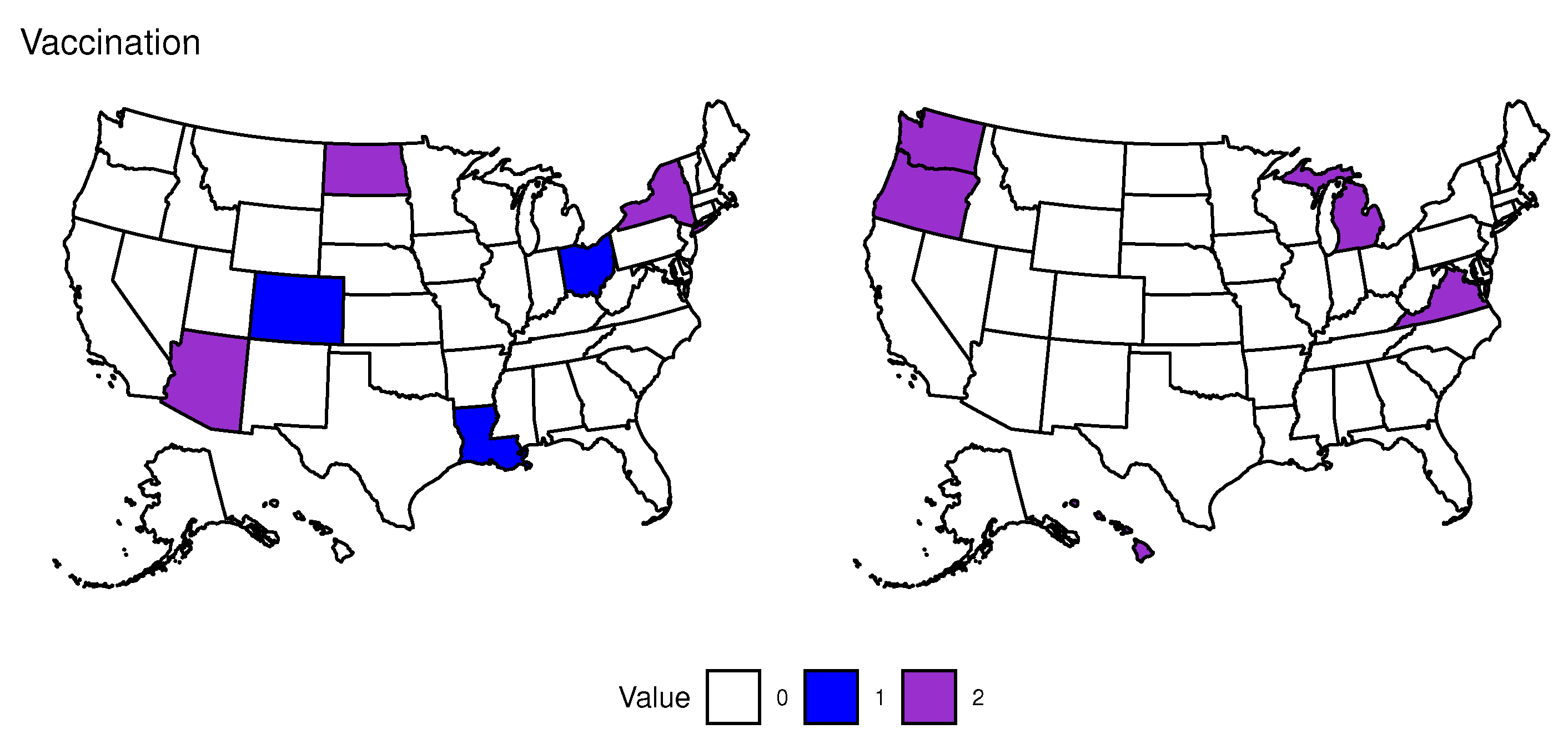
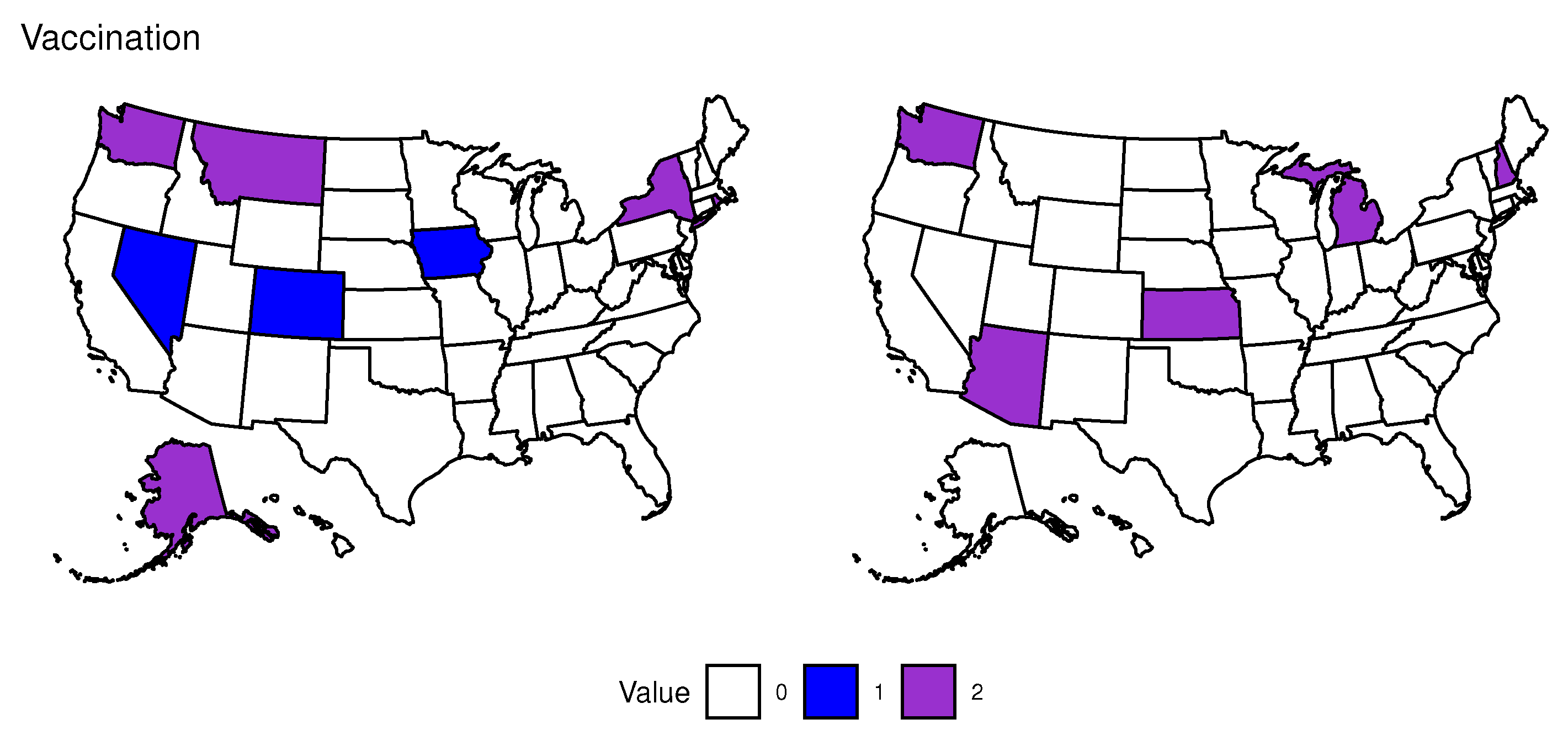
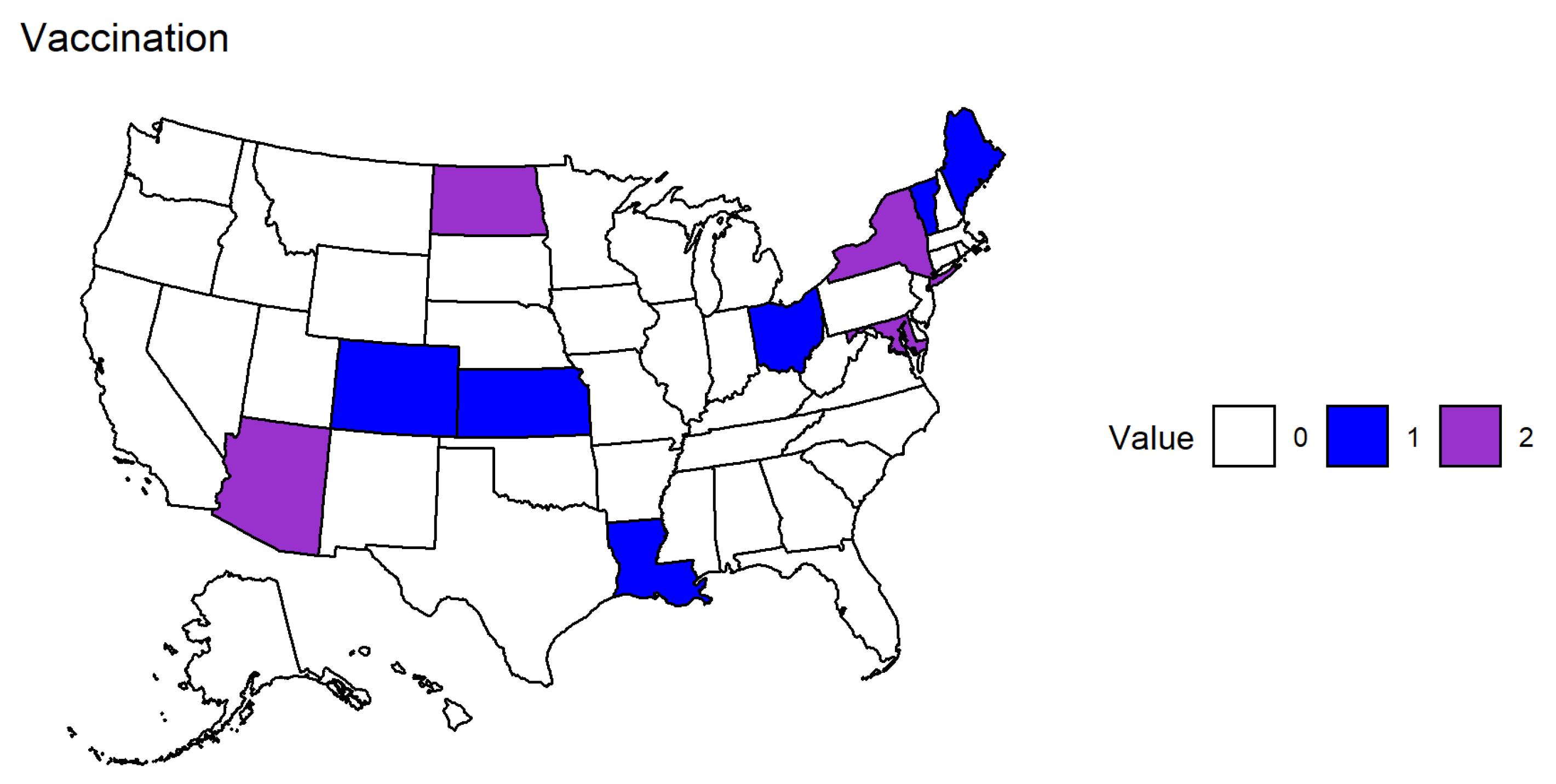
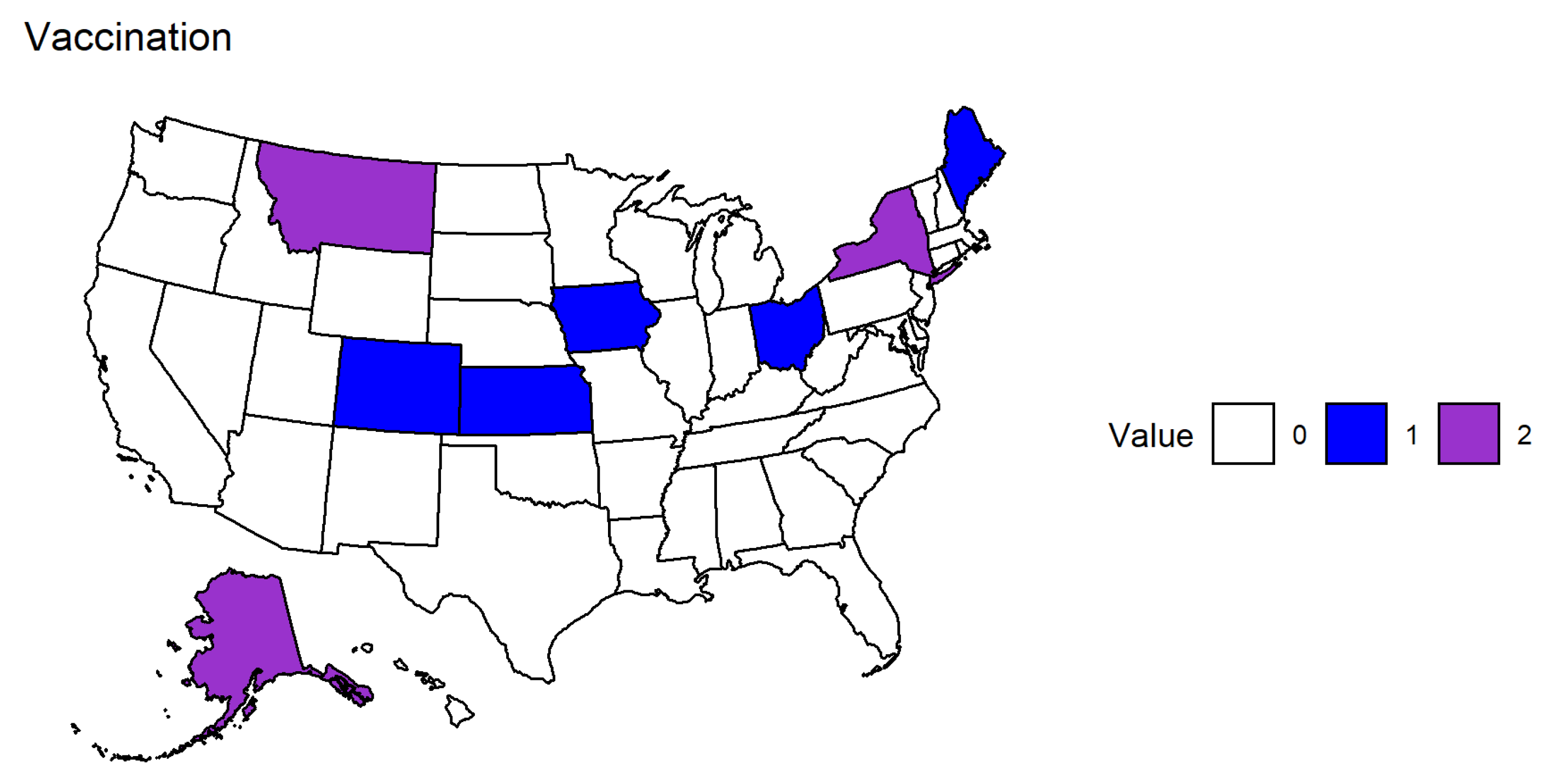
Appendix C. Effects of Vaccination in the Second Time Period




References
- World Health Organization (WHO). COVID-19 Dashboard; World Health Organization: Geneva, Switzerland, 2020; Available online: https://covid19.who.int/ (accessed on 6 March 2022).
- Centers for Disease Control and Prevention (CDC). COVID-19 Overview and Infection Prevention and Control Priorities in Non-U.S. Healthcare Settings. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/non-us-settings/overview/index.html# (accessed on 6 March 2022).
- World Health Organization (WHO). Coronavirus Disease (COVID-19): How Is It Transmitted? World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-covid-19-how-is-it-transmitted (accessed on 22 March 2022).
- Sauver, J.L.S.; Lopes, G.S.; Rocca, W.A.; Prasad, K.; Majerus, M.R.; Limper, A.H.; Jacobson, D.J.; Fan, C.; Jacobson, R.M.; Rutten, L.J.; et al. Factors Associated With Severe COVID-19 Infection Among Persons of Different Ages Living in a Defined Midwestern US Population. Mayo Clin. Proc. 2021, 96, 2528–2539. [Google Scholar] [CrossRef] [PubMed]
- Nouvellet, P.; Bhatia, S.; Cori, A.; Ainslie, K.E.; Baguelin, M.; Bhatt, S.; Boonyasiri, A.; Brazeau, N.F.; Cattarino, L.; Cooper, L.V.; et al. Reduction in mobility and COVID-19 Transmission. Nat. Commun. 2021, 12, 1090. [Google Scholar] [CrossRef] [PubMed]
- Fasano, M.V.; Padula, M.; Azrak, M.; Avico, A.J.; Sala, M.; Andreoli, M.F. Consequences of Lockdown During COVID-19 Pandemic in Lifestyle and Emotional State of Children in Argentina. Front. Pediatr. 2021, 9, 660033. [Google Scholar] [CrossRef] [PubMed]
- Richter, D.; Riedel-Heller, S.; Zürcher, S. Mental health problems in the general population during and after the first lockdown phase due to the SARS-CoV-2 pandemic: Rapid review of multi-wave studies. Epidemiol. Psychiatr. Sci. 2021, 30, e27. [Google Scholar] [CrossRef]
- Nie, X.; Feng, K.; Wang, S.; Li, Y. Factors Influencing Public Panic During the COVID-19 Pandemic. Front. Psychol. 2021, 12, e576301. [Google Scholar] [CrossRef]
- Novotný, J.S.; Gonzalez-Rivas, J.P.; Kunzová, Š.; Skladaná, M.; Pospíšilová, A.; Polcrová, A.; Medina-Inojosa, J.R.; Lopez-Jimenez, F.; Geda, Y.E.; Stokin, G.B. Risk Factors Underlying COVID-19 Lockdown-Induced Mental Distress. Front. Psychiatry 2020, 11, e603014. [Google Scholar] [CrossRef]
- Trivedi, M.M.; Das, A. Did the Timing of State Mandated Lockdown Affect the Spread of COVID-19 Infection? A County-level Ecological Study in the United States. J. Prev. Med. Public Health 2021, 54, 238–244. [Google Scholar] [CrossRef]
- Adeel, A.B.; Catalano, M.; Catalano, O.; Gibson, G.; Muftuoglu, E.; Riggs, T.; Sezgin, M.H.; Shvetsova, O.; Tahir, N.; VanDusky-Allen, J.; et al. COVID-19 Policy Response and the Rise of the Sub-National Governments. Can. Public Policy 2020, 46, 565–584. [Google Scholar] [CrossRef]
- Hennigan, W.J.; Park, A.; Ducharme, J. The U.S. Fumble Its Early Vaccine Rollout. Will the Biden Administration Put America Back on Track? Time 2021. Available online: https://time.com/5932028/vaccine-rollout-joe-biden/ (accessed on 10 April 2022).
- Wilson, C. The U.S. COVID-19 Vaccine Rollout Is Getting Faster. But Is It Fast Enough? Time 2021. Available online: https://time.com/5938128/covid-19-vaccine-rollout-biden/ (accessed on 10 April 2022).
- Staff, M.C. Herd Immunity and COVID-19: What You Need to Know. Mayo Clin. 2021. Available online: https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/herd-immunity-and-coronavirus/art-20486808 (accessed on 10 April 2022).
- Czeisler, M.É.; Lane, R.I.; Petrosky, E.; Wiley, J.F.; Christensen, A.; Njai, R.; Weaver, M.D.; Robbins, R.; Facer-Childs, E.R.; Barger, L.K.; et al. Mental Health, Substance Use, and Suicidal Ideation During the COVID-19 Pandemic—United States, 24–30 June 2020. MMWR Mor. Mortal. Wkly. Rep. 2020, 69, 1049–1057. [Google Scholar] [CrossRef]
- Novotney, A. The risks of social isolation. Monit. Psychol. 2019, 50, 32. [Google Scholar]
- Pearman, A.; Hughes, M.L.; Smith, E.L.; Neupert, S.D. Mental Health Challenges of United States Healthcare Professionals During COVID-19. Front. Psychol. 2020, 11, e2065. [Google Scholar] [CrossRef] [PubMed]
- Su, Z.; McDonnell, D.; Wen, J.; Kozak, M.; Abbas, J.; Šegalo, S.; Li, X.; Ahmad, J.; Cheshmehzangi, A.; Cai, Y.; et al. Mental health consequences of COVID-19 media coverage: The need for effective crisis communication practices. Glob. Health 2021, 17, 4. [Google Scholar] [CrossRef] [PubMed]
- Armiya’u, A.Y.U.; Yıldırım, M.; Muhammad, A.; Tanhan, A.; Young, J.S. Mental Health Facilitators and Barriers during COVID-19 in Nigeria. J. Asian Afr. Stud. 2022, 00219096221111354. [Google Scholar] [CrossRef]
- Hamka, M.W.S.; Ramadhan, Y.A.; Yusuf, M.; Wang, J.H. Spiritual Well-Being, Depression, Anxiety, and Stress in Indonesian Muslim Communities During COVID-19. Pyschology Res. Behav. Manag. 2022, 15, 3013–3025. [Google Scholar] [CrossRef]
- Rafique, N.; Al Tufaif, F.; Alhammali, W.; Alalwan, R.; Aljaroudi, A.; AlFaraj, F.; Latif, R.; Ibrahim Al-Asoom, L.; Alsunni, A.A.; Al Ghamdi, K.S.; et al. The Psychological Impact of COVID-19 on Residents of Saudi Arabia. Psychol. Res. Behav. Manag. 2022, 15, 1221–1234. [Google Scholar] [CrossRef] [PubMed]
- Fulk, A.; Saenz-Escarcega, R.; Kobayashi, H.; Maposa, I.; Agusto, F. Assessing the Impacts of COVID-19 and Social Isolation on Mental Health in the United States of America. medRxiv 2022. [Google Scholar] [CrossRef]
- Reinhart, A.; Brooks, L.; Jahja, M.; Rumack, A.; Tang, J.; Agrawal, S.; Al Saeed, W.; Arnold, T.; Basu, A.; Bien, J.; et al. An open repository of real-time COVID-19 indicators. Proc. Natl. Acad. Sci. USA 2021, 118, e2111452118. [Google Scholar] [CrossRef]
- Lütkepohl, H. A New Introduction to Multiple Time Series Analysis; Springer: Berlin/Heidelberg, Germany, 2005. [Google Scholar] [CrossRef]
- Stock, J.; Watson, M. Vector Autoregressions. J. Econ. Perspect. 2001, 15, 101–115. [Google Scholar] [CrossRef]
- Pfaff, B. Analysis of Integrated and Cointegrated Time Series with R, 2nd ed.; Springer: New York, NY, USA, 2008. [Google Scholar] [CrossRef]
- Pfaff, B. VAR, SVAR and SVEC Models: Implementation within R Package vars. J. Stat. Softw. 2008, 27, 1–32. [Google Scholar] [CrossRef]
- Skafle, I.; Nordahl-Hansen, A.; Quintana, D.S.; Wynn, R.; Gabarron, E. Misinformation about COVID-19 Vaccines on Social Media: Rapid Review. J. Med. Internet Res. 2022, 24, e37367. [Google Scholar] [CrossRef]
- Holcombe, M.; Yan, H.; Waldrop, T. Delta Variant Now Makes Up more than Half of Coronavirus Cases in US, CDC says. CNN 2021. Available online: https://www.cnn.com/2021/07/06/health/us-coronavirus-tuesday/index.html (accessed on 4 May 2023).
- Hagen, A. How Dangerous Is the Delta Variant (B.1.617.2)? Am. Soc. Microbiol. 2021. Available online: https://asm.org/Articles/2021/July/How-Dangerous-is-the-Delta-Variant-B-1-617-2 (accessed on 5 May 2023).
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Ramiz, L.; Contrand, B.; Rojas Castro, M.Y.; Dupuy, M.; Lu, L.; Sztal-Kutas, C.; Lagarde, E. A longitudinal study of mental health before and during COVID-19 lockdown in the French population. Glob. Health 2021, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Magnúsdóttir, I.; Lovik, A.; Unnarsdóttir, A.B.; McCartney, D.; Ask, H.; Kõiv, K.; Christoffersen, L.A.N.; Johnson, S.U.; Hauksdóttir, A.; Fawns-Ritchie, C.; et al. Acute COVID-19 severity and mental health morbidity trajectories in patient populations of six nations: An observational study. Lancet Public Health 2022, 7, E406–E416. [Google Scholar] [CrossRef] [PubMed]
- Mautong, H.; Gallardo-Rumbea, J.A.; Alvarado-Villa, G.E.; Fernández-Cadena, J.C.; Andrade-Molina, D.; Orellana-Román, C.E.; Cherrez-Ojeda, I. Assessment of depression, anxiety and stress levels in the Ecuadorian general population during social isolation due to the COVID-19 outbreak: A cross-sectional study. BMC Psychiatry 2021, 21, 212. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Kämpfen, F.; Kohler, I.V.; Ciancio, A.; Bruine de Bruin, W.; Maurer, J.; Kohler, H.P. Predictors of mental health during the COVID-19 pandemic in the US: Role of economic concerns, health worries and social distancing. PLoS ONE 2020, 15, e0241895. [Google Scholar] [CrossRef]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef]
- Santini, Z.I.; Jose, P.E.; Cornwell, E.Y.; Koyanagi, A.; Nielsen, L.; Hinrichsen, C.; Meilstrup, C.; Madsen, K.R.; Koushede, V. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): A longitudinal mediation analysis. Lancet Public Health 2020, 5, e62–e70. [Google Scholar] [CrossRef]
- Saddik, B.; Hussein, A.; Albanna, A.; Elbarazi, I.; Al-Shujairi, A.; Temsah, M.H.; Saheb Sharif-Askari, F.; Stip, E.; Hamid, Q.; Halwani, R. The psychological impact of the COVID-19 pandemic on adults and children in the United Arab Emirates: A nationwide cross-sectional study. BMC Psychiatry 2021, 21, 224. [Google Scholar] [CrossRef]
- Hwang, T.J.; Rabheru, K.; Peisah, C.; Reichman, W.; Ikeda, M. Loneliness and social isolation during the COVID-19 pandemic. Int. Psychogeriatr. 2020, 32, 1217–1220. [Google Scholar] [CrossRef]
- Burton, A.; McKinlay, A.; Aughterson, H.; Fancourt, D. Impact of the COVID-19 pandemic on the mental health and well-being of adults with mental health conditions in the UK: A qualitative interview study. J. Ment. Health 2021, 29, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lekkas, D.; Gyorda, J.A.; Price, G.D.; Wortzman, Z.; Jacobson, N.C. Using the COVID-19 Pandemic to Assess the Influence of News Affect on Online Mental Health-Related Search Behavior Across the United States: Integrated Sentiment Analysis and the Circumplex Model of Affect. J. Med. Internet Res. 2022, 24, e32731. [Google Scholar] [CrossRef] [PubMed]
- Olagoke, A.A.; Olagoke, O.O.; Hughes, A.M. Exposure to coronavirus news on mainstream media: The role of risk perceptions and depression. Br. J. Health Psychol. 2020, 25, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Saenz-Escarcega, R.; Fulk, A.; Agusto, F.B. Understanding mental health trends during COVID-19 pandemic in the United States using network analysis. medRxiv 2022. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fulk, A.; Saenz-Escarcega, R.; Kobayashi, H.; Maposa, I.; Agusto, F. Assessing the Impacts of COVID-19 and Social Isolation on Mental Health in the United States of America. COVID 2023, 3, 807-830. https://doi.org/10.3390/covid3060060
Fulk A, Saenz-Escarcega R, Kobayashi H, Maposa I, Agusto F. Assessing the Impacts of COVID-19 and Social Isolation on Mental Health in the United States of America. COVID. 2023; 3(6):807-830. https://doi.org/10.3390/covid3060060
Chicago/Turabian StyleFulk, Alexander, Raul Saenz-Escarcega, Hiroko Kobayashi, Innocent Maposa, and Folashade Agusto. 2023. "Assessing the Impacts of COVID-19 and Social Isolation on Mental Health in the United States of America" COVID 3, no. 6: 807-830. https://doi.org/10.3390/covid3060060