
A Qualitative Analysis of Older Adults’ Cognitive Appraisal in Coping during the COVID-19 Pandemic: The Role of Social Capital


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Research Methodology
3. Background
4. Data Collection
General Approach to Data Analysis
5. Findings
5.1. Primary Appraisal
There are some people who are just very physical people. So when you’re talking to them, they’re reaching over and brushing something off your shoulder or grabbing your hand and pointing at something. And that sort of in person, obviously, can not be replicated.—Interviewee #8
And I have tried to follow the recommendations for safety and security where possible. I’m amazed at how many people I see outside not taking care of masks, social distancing, and so on. So I do pay attention to what the government says.—Interviewee #37
The thing that has bothered me about lockdown is the lack of ability to choose to do something. Should I choose to go out and eat in a restaurant? I can’t…. …I talked to my friends in person or over the phone or through email; we exchanged information. We’ve done a little less of it during lockdown, because we haven’t been able to, you know, have coffee together and talk for two hours.—Participant #16
Endangered by the virus? No, I’ve been more impacted by the restrictions imposed by governments.—Interviewee #09
It’s just very difficult balance between keeping yourself safe physically and keeping yourself healthy mentally.—Interviewee #31
Summary
5.2. Secondary Appraisal
5.2.1. Situation #1—Family/Friend Connection
With my mother, I cannot [go online] you know. She doesn’t know anything about a computer. So, with my mother, it’s always face to face.—Interviewee #12
My friend, who is the mother of these kids. Her partner just died of an aneurysm in September. You know, the conversations were kind of heavy with her. Very hard. I actually went down there in December even though I wasn’t supposed to because she was just hysterical. She was in the room with him when he died.—Interviewee #31
And that’s occurring also in a couple of other areas where we plan socially distanced meetings in person. And have been doing that for a while now.—Interviewee #9
I’m going to be doing a helicopter to cross the border, and get—they have a flatbed truck service, which takes your car—and we’re going to see family in August. And we will do whatever has to be done. The testing, and the—we’ve done the vaccinating—and we’ll quarantine if it is still in Vogue at that time.—Interviewee #28
We did have meetings in the backyard over a distance from time to time, but certainly not as often as would be previously. When things were, even with my children you know, we would see each other at a distance.—Interviewee #25
We can plan a Christmas, one of my tea groups. We’re having Christmas in July socially. … So, we are socially distanced in someone’s backyard. Bring your own chair.—Interviewee #09
Other friends locally will occasionally email, and then occasionally still [meet] in person that is carefully distanced out in the backyard. The legally allowed number of people varied during the lockdown.—Interviewee #27
I walked with friends, especially in the last two months… In the fall, we were able to—we went down [to] Niagara a couple of times and had a patio, you know, dinner with friends at a winery. Them sitting, you know, at the next table. I mean, it wasn’t really isolated. Believe me. But yeah, we were able to do that. We had a lot last summer.—Interviewee #28
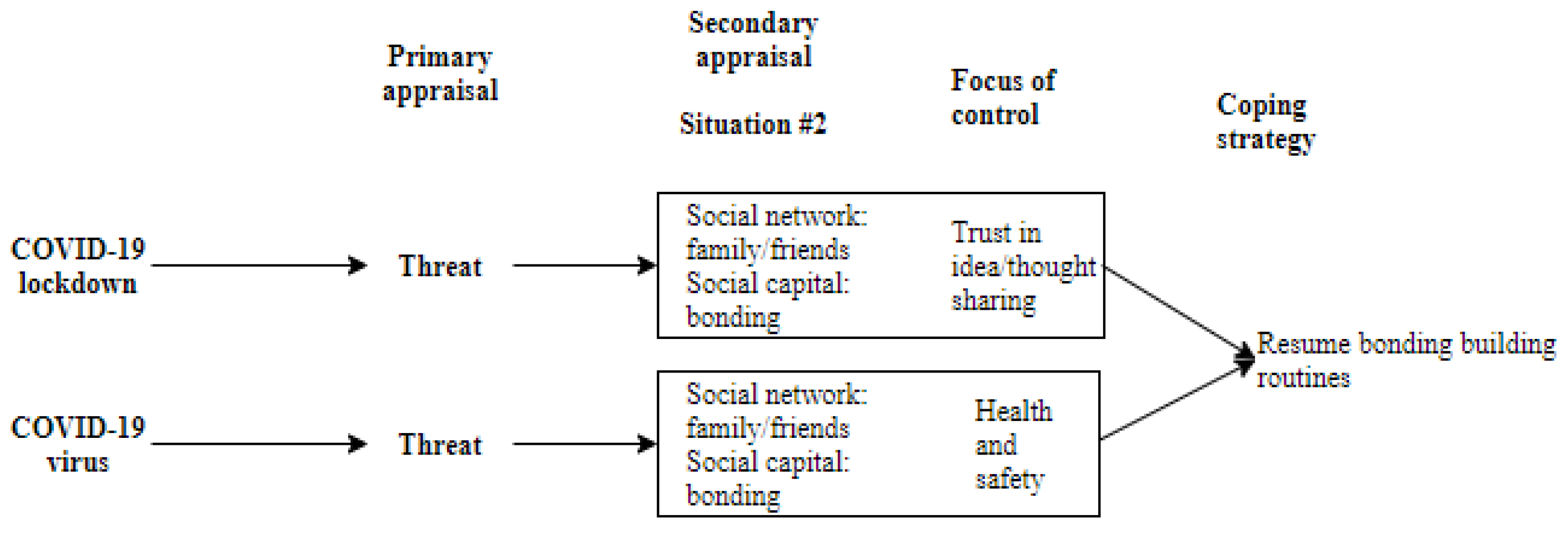
5.2.2. Situation #2—Disrupted Routines
When I’m in a mood to write, my writing friend and I will exchange what we’ve written and comment on it. One of the great pleasures of my life is to have her in my life.—Interviewee #35
I have a walking friend who lives in this building. And we go out with our masks on, around the lake, watching everybody else having their interactions. But other than that, we don’t go to each other’s place and sit and have tea or anything like that. And I have a friend that I exchanged books with. So, I would meet with her at some place, and we would exchange our books and sometimes go for a walk or whatever, masked.—Interviewee #29
Other interviewees spoke of maintaining existing friendships and routines but shifting communication from in person to more remote methods:I talked to my friends in person or over the phone or through email, we exchanged information. We’ve done a little less of it during lockdown. Because we haven’t been able to, you know, have coffee together and talk for two hours. But we’ve done the same things.—Interviewee #16
I was already going to the Pilates studio. And then there were no classes, of course, when the lockdown started. Then the studio started doing them online, so I do regular classes a week. 5 classes a week with some of the instructors I already knew from the studio.—Interviewee #38
I’m sure it’s not the same talking on Zoom as it is talking in person. But we do regularly meet on Zoom just to see how everybody’s doing and so on. But because then you get a group together. …When we’re on Zoom, there are 7 of us that meet regularly. And so you get everybody’s story, which is always fun. Right. It [her social network] certainly hasn’t grown, except there are a couple of people that I’ve gotten to know better.—Interviewee #35
There are weekly meetings, which I participate in. I’m a committee chair at senior college.—Participant #37
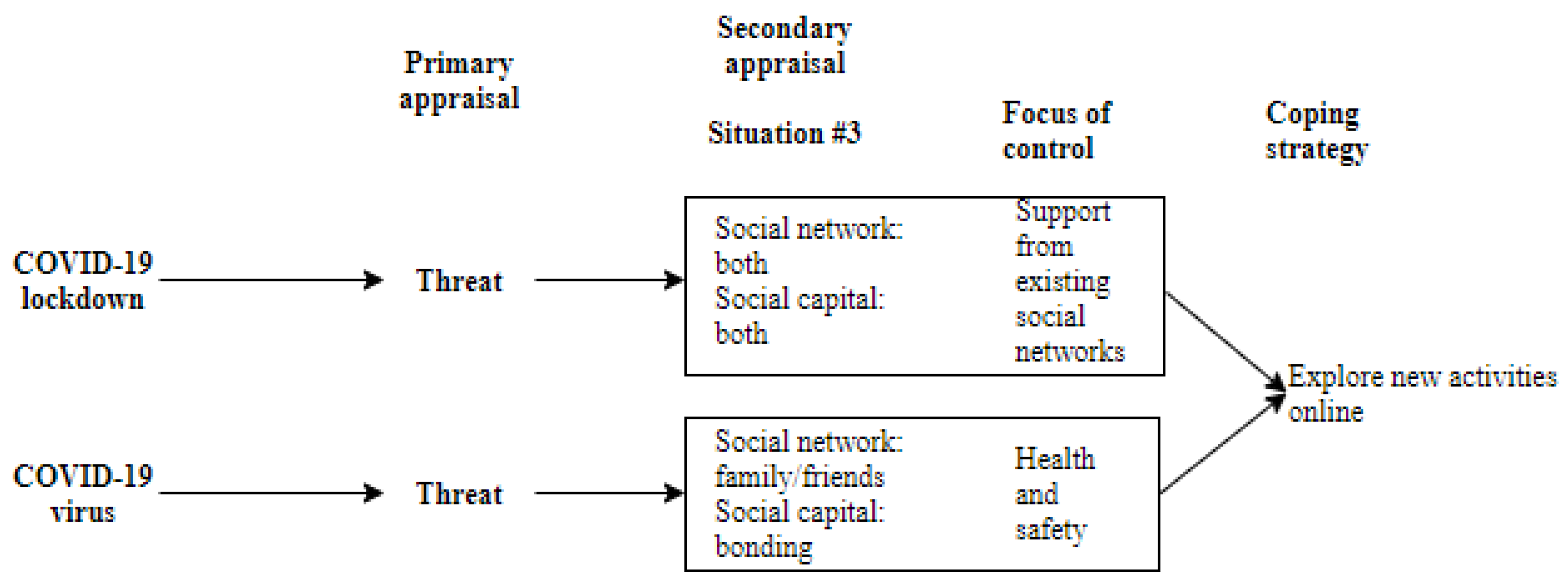
5.2.3. Situation #3—Opportunities for New Social Activities
… there are also people or events that wouldn’t even be happening online if it wasn’t for COVID. So I have managed to take advantage of things being online that I wouldn’t be.—Interviewee #8
We [the couple] joined a virtual church choir. And so that took up an awful lot of time because you’ve got to practice. Yeah, you go to a choir practice and you’ve got to practice on your own. And then you had to tape your singing, so you’d be listening to the music and then you would tape in front of Google Meet, a Google program, and then upload it to the church directory and the choir director put together the performance…. So we did that almost every week.—Participant #32
My arthritis doctor recommended that I get in touch with the Arthritis Society and they have zoom presentations.—Interviewee #6
I play a game called words with friends you know. It’s like a scrapbook game. Well, I’ve got about 9 clients now. So I’m on there too often playing this game because I’m addicted to it.—Interviewee #12
6. Data Analysis
6.1. Situation #1—Connection with Friends/Family
We were cautious. So we looked at who we interacted with, who was in our very small circle… We were very cautious of who we chose to be in our circle. And we maintained that since March of 2020. We had a very core group of people that we would allow in. And if we saw that any of those people were starting to get a little iffy, well, they were no longer in our core group.—Interviewee #32
6.2. Situation #2—Disrupted Routines
6.3. Situation #3—New Online Activities
7. Discussion
8. Practical Implications
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Interview Questions
- Basic demographics (e.g., age, gender, retirement status, marital status, living conditions)
- During the COVID-19 lockdown, did you engage in online social communities (e.g., interest group)?
- Did you connect with your family and friends during the lockdown?
- Has your social circle changed as a result of the lockdown? How so?
- During the lockdown, what news/information attracted most of your attention? Please give us a couple of examples
- Were you satisfied with your social engagement (including online using social media and using phone) during the lockdown? In what aspect were you benefited from the social engagements?
- Did you have any non-virtual social interactions during the lockdown? In what aspect were you benefited from the social engagements?
- To what extent did you believe people living around you were trustworthy during the lockdown? Please explain your answer
- Describe the support you received from your local community. On the scale of 1–10 (1 worst, and 10 the best) rate their support during the lockdown
Appendix B
Intervewee Profiles
| ID | Age | Gender | Retirement Status | Marital Status | Living Conditions |
| #3 | 73 | Female | Working part-time (Inferred from context—not directly answered) | Married | Lives with husband |
| #4 | 68 | Female | Retired | Single | Lives alone |
| #6 | 79 | Female | Retired | Single (Inferred from context—not directly answered) | Lives alone |
| #8 | 66 | Female | Retired | Single | Lives alone |
| #9 | 71 | Male | Retired | Single | Lives alone |
| #10 | 69 | Female | Retired | Married | Lives with husband |
| #11 | 69 | Female | Not Retired/Working | Divorced | Lives alone |
| #12 | 71 | Female | Retired | Common Law | Lives with spouse |
| #14 | 70 | Female | Retired | Divorced | Lives alone |
| #16 | Not specified | Female | Retired | Married | Lives with husband |
| #22 | 69 | Male | Retired | Married | Lives with wife |
| #24 | 77 | Female | Retired | Divorced | Lives alone |
| #25 | 72 | Male | Retired | Married | Lives with wife |
| #27 | 69 | Male | Semi-Retired | Married | Lives with wife |
| #28 | 76 | Female | Retired | Married | Lives with husband |
| #29 | 70 | Female | Retired | Separated | Lives alone |
| #30 | 74 | Male | Semi-Retired | With partner | Lives with partner |
| #31 | 75 | Female | Retired | Divorced | Shares duplex with sister |
| #32 | 67 | Male | Retired | With partner | Lives with partner |
| #35 | 89 | Female | Retired | Single (Inferred from context—not directly answered) | Lives alone |
| #37 | 82 | Male | Retired | Married | Lives with wife |
| #38 | 77 | Female | Retired | Widow | Lives alone |
References
- Demers, L.; Robichaud, L.; Gélinas, I.; Noreau, L.; Desrosiers, J. Coping Strategies and Social Participation in Older Adults. Gerontology 2008, 55, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Palmes, M.S.; Trajera, S.M.; Ching, G.S. Relationship of Coping Strategies and Quality of Life: Parallel and Serial Mediating Role of Resilience and Social Participation among Older Adults in Western Philippines. Int. J. Environ. Res. Public Health 2021, 18, 10006. [Google Scholar] [CrossRef] [PubMed]
- Balsamo, M.; Cataldi, F.; Carlucci, L.; Fairfield, B. Assessment of anxiety in older adults: A review of self-report measures. Clin. Interv. Aging 2018, 13, 573–593. [Google Scholar] [CrossRef]
- Li, F.; Luo, S.; Mu, W.; Li, Y.; Ye, L.; Zheng, X.; Xu, B.; Ding, Y.; Ling, P.; Zhou, M.; et al. Effects of sources of social support and resilience on the mental health of different age groups during the COVID-19 pandemic. BMC Psychiatry 2021, 21, 16. [Google Scholar] [CrossRef]
- Moos, R.H.; Schutte, K.K.; Brennan, P.L.; Moos, B.S. The Interplay Between Life Stressors and Depressive Symptoms Among Older Adults. J. Gerontol. Ser. B 2005, 60, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Nam, S.-J. Mediating effect of social support on the relationship between older adults’ use of social media and their quality-of-life. Curr. Psychol. 2019, 40, 4590–4598. [Google Scholar] [CrossRef]
- Vrach, I.T.; Tomar, R. Mental health impacts of social isolation in older people during COVID pandemic. Prog. Neurol. Psychiatry 2020, 24, 25–29. [Google Scholar] [CrossRef]
- Bixter, M.T.; Blocker, K.A.; Rogers, W.A. Enhancing social engagement of older adults through technology. In Aging, Technology and Health; Elsevier: Amsterdam, The Netherlands, 2018; pp. 179–214. [Google Scholar] [CrossRef]
- Bruggencate, T.T.; Luijkx, K.G.; Sturm, J. When your world gets smaller: How older people try to meet their social needs, including the role of social technology. Ageing Soc. 2018, 39, 1826–1852. [Google Scholar] [CrossRef]
- Choi, N.G.; Hegel, M.T.; Marti, C.N.; Marinucci, M.L.; Sirrianni, L.; Bruce, M.L. Telehealth Problem-Solving Therapy for Depressed Low-Income Homebound Older Adults. Am. J. Geriatr. Psychiatry 2014, 22, 263–271. [Google Scholar] [CrossRef]
- Jose, P.E.; Ryan, N.; Pryor, J. Does Social Connectedness Promote a Greater Sense of Well-Being in Adolescence Over Time? J. Res. Adolesc. 2012, 22, 235–251. [Google Scholar] [CrossRef]
- Dahlberg, L.; McKee, K.J.; Frank, A.; Naseer, M. A systematic review of longitudinal risk factors for loneliness in older adults. Aging Ment. Health 2022, 26, 225–249. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Jiang, S. Influence of social participation and support on self-rated health among Chinese older adults: Mediating role of coping strategies. Curr. Psychol. 2023, 42, 14368–14375. [Google Scholar] [CrossRef]
- Na, L.; Yang, L.; Mezo, P.G.; Liu, R. Age disparities in mental health during the COVID19 pandemic: The roles of resilience and coping. Soc. Sci. Med. 2022, 305, 115031. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, N.R. A Review of Social Isolation: An Important but Underassessed Condition in Older Adults. J. Prim. Prev. 2012, 33, 137–152. [Google Scholar] [CrossRef]
- Kiliam, K. Lessons from COVID-19: Improving Social Health to Build Community Resilience. Gener. J. 2022, 46, 1–11. [Google Scholar]
- CDC. Risk for COVID-19 Infection, Hospitalization, and Death by Age Group. Cdc.Gov. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html (accessed on 15 January 2023).
- National Centers for Health Statistics. Provisional Death Counts for Coronavirus Disease (COVID-19). Cdc.Gov. 2020. Available online: https://www.cdc.gov/nchs/nvss/vsrr/COVID19/index.htm (accessed on 15 January 2023).
- World Health Organization. WHO Delivers Advice and Support for Older People during COVID-World Health Organization. 2020. Available online: https://www.who.int/news-room/feature-stories/detail/who-delivers-advice-and-support-for-older-people-during-covid-19#:~:text=Althoughallagegroupsare,potentialunderlyinghealthconditions (accessed on 20 May 2022).
- Han, E.; Tan, M.M.J.; Turk, E.; Sridhar, D.; Leung, G.M.; Shibuya, K.; Asgari, N.; Oh, J.; García-Basteiro, A.L.; Hanefeld, J.; et al. Lessons learnt from easing COVID-19 restrictions: An analysis of countries and regions in Asia Pacific and Europe. Lancet 2020, 396, 1525–1534. [Google Scholar] [CrossRef]
- UNICEF. Don’t Let Children Be the Hidden Victimes of COVID-19 Pandemic. UNICEF. 2020. Available online: https://www.unicef.org/press-releases/dont-let-children-be-hidden-victims-covid-19-pandemic (accessed on 10 April 2022).
- Wu, B. Social isolation and loneliness among older adults in the context of COVID-19: A global challenge. Glob. Health Res. Policy 2020, 5, 27. [Google Scholar] [CrossRef]
- Fox, C. All People over the Age of 70 in Ontario Advised to Self-Isolate during COVID-19 Pandemic | CTV News. 2020. Available online: https://toronto.ctvnews.ca/all-people-over-the-age-of-70-in-ontario-advised-to-self-isolate-during-covid-19-pandemic-1.4874346 (accessed on 18 March 2022).
- Hajek, A.; König, H.-H. Social Isolation and Loneliness of Older Adults in Times of the COVID-19 Pandemic: Can Use of Online Social Media Sites and Video Chats Assist in Mitigating Social Isolation and Loneliness? Gerontology 2021, 67, 121–124. [Google Scholar] [CrossRef]
- Su, C.; Yang, L.; Dong, L.; Zhang, W. The Psychological Well-Being of Older Chinese Immigrants in Canada amidst COVID-19: The Role of Loneliness, Social Support, and Acculturation. Int. J. Environ. Res. Public Health 2022, 19, 8612. [Google Scholar] [CrossRef]
- Greenwood-Hickman, M.A.; Dahlquist, J.; Cooper, J.; Holden, E.; McClure, J.B.; Mettert, K.D.; Perry, S.R.; Rosenberg, D.E. “They’re Going to Zoom It”: A Qualitative Investigation of Impacts and Coping Strategies During the COVID-19 Pandemic Among Older Adults. Front. Public Health 2021, 9, 679976. [Google Scholar] [CrossRef]
- Gupta, R.; Pillai, V. Comparison of Coping Strategies and Resilience Among White, Non-White, and Asian Older Adults in San Francisco. Innov. Aging 2020, 4 (Suppl. 1), 579–580. [Google Scholar] [CrossRef]
- Nieto, M.; Romero, D.; Ros, L.; Zabala, C.; Martínez, M.; Ricarte, J.J.; Serrano, J.P.; Latorre, J.M. Differences in Coping Strategies Between Young and Older Adults: The Role of Executive Functions. Int. J. Aging Hum. Dev. 2020, 90, 28–49. [Google Scholar] [CrossRef] [PubMed]
- Provencher, V.; Desrosiers, J.; Demers, L.; Carmichael, P.-H. Optimizing social participation in community-dwelling older adults through the use of behavioral coping strategies. Disabil. Rehabil. 2016, 38, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, N.G.; Han, C.Q.Y.; Su, Y.; Klainin-Yobas, P.; Wu, X.V. Psychological impacts and online interventions of social isolation amongst older adults during COVID-19 pandemic: A scoping review. J. Adv. Nurs. 2022, 78, 609–644. [Google Scholar] [CrossRef]
- Webb, L.M.; Chen, C.Y. The COVID-19 pandemic’s impact on older adults’ mental health: Contributing factors, coping strategies, and opportunities for improvement. Int. J. Geriatr. Psychiatry 2022, 37. [Google Scholar] [CrossRef] [PubMed]
- Folkman, S.; Lazarus, R.S. Coping as a mediator of emotion. J. Pers. Soc. Psychol. 1988, 54, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Sun, X.; Li, B.J.; Zhang, H.; Zhang, G. Social media use for coping with stress and psychological adjustment: A transactional model of stress and coping perspective. Front. Psychol. 2023, 14, 1140312. [Google Scholar] [CrossRef]
- Folkman, S.; Moskowitz, J.T. Coping: Pitfalls and Promise. Annu. Rev. Psychol. 2004, 55, 745–774. [Google Scholar] [CrossRef]
- Lazarus, R.S. From Psychological Stress to the Emotions: A History of Changing Outlooks. Annu. Rev. Psychol. 1993, 44, 1–22. [Google Scholar] [CrossRef]
- Miller, T.A.; McCool, S.F. Coping with Stress in Outdoor Recreational Settings: An Application of Transactional Stress Theory. Leis. Sci. 2003, 25, 257–275. [Google Scholar] [CrossRef]
- Folkman, S. Personal control and stress and coping processes: A theoretical analysis. J. Pers. Soc. Psychol. 1984, 46, 839–852. [Google Scholar] [CrossRef] [PubMed]
- Wolfers, L.N.; Utz, S. Social media use, stress, and coping. Curr. Opin. Psychol. 2022, 45, 101305. [Google Scholar] [CrossRef] [PubMed]
- Folkman, S.; Lazarus, R.S. If it changes it must be a process: Study of emotion and coping during three stages of a college examination. J. Pers. Soc. Psychol. 1985, 48, 150–170. [Google Scholar] [CrossRef] [PubMed]
- Heth, J.T.; Somer, E. Characterizing stress tolerance: “controllability awareness” and its relationship to perceived stress and reported health. Pers. Individ. Differ. 2002, 33, 883–895. [Google Scholar] [CrossRef]
- Troy, A.S.; Shallcross, A.J.; Mauss, I.B. A Person-by-Situation Approach to Emotion Regulation: Cognitive Reappraisal Can Either Help or Hurt, Depending on the Context. Psychol. Sci. 2013, 24, 2505–2514. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, R.S.; Dunkel-Schetter, C.; DeLongis, A.; Gruen, R.J. Dynamics of a stressful encounter: Cognitive appraisal, coping, and encounter outcomes. J. Pers. Soc. Psychol. 1986, 50, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- Wolfers, L.N.; Schneider, F.M. Using Media for Coping: A Scoping Review. Commun. Res. 2021, 48, 1210–1234. [Google Scholar] [CrossRef]
- Fuller, H.R.; Huseth-Zosel, A. Lessons in Resilience: Initial Coping among Older Adults during the COVID-19 Pandemic. Gerontol. 2021, 61, 114–125. [Google Scholar] [CrossRef]
- Dong, L.; Yang, L. COVID-19 anxiety: The impact of older adults’ transmission of negative information and online social networks. Aging Health Res. 2023, 3, 100119. [Google Scholar] [CrossRef]
- Nitschke, J.P.; Forbes, P.A.G.; Ali, N.; Cutler, J.; Apps, M.A.J.; Lockwood, P.L.; Lamm, C. Resilience during uncertainty? Greater social connectedness during COVID-19 lockdown is associated with reduced distress and fatigue. Br. J. Health Psychol. 2021, 26, 553–569. [Google Scholar] [CrossRef]
- Dias, A.; Scavarda, A.; Reis, A.d.C.; Santos, I.; Fonseca, A. COVID-19 Pandemical Period: Issues and Strategies to Make Sustainable Socialization and Recreation for Elderly People in Long-Term Care Institutions. COVID 2023, 3, 392–404. [Google Scholar] [CrossRef]
- Hossain, K.M.A.; Shafin, R.; Yeasmin, M.H.; Jahid, I.K.; Hossain, M.A.; Rana, S.; Kabir, M.F.; Chokrovorty, S.K.; Faruqui, R. Community Coping Strategies for COVID-19 in Bangladesh: A Nationwide Cross-Sectional Survey. COVID 2023, 3, 320–335. [Google Scholar] [CrossRef]
- Schaefer, C.; Coyne, J.C.; Lazarus, R.S. The health-related functions of social support. J. Behav. Med. 1981, 4, 381–406. [Google Scholar] [CrossRef] [PubMed]
- Chan, M. Mobile phones and the good life: Examining the relationships among mobile use, social capital and subjective well-being. New Media Soc. 2015, 17, 96–113. [Google Scholar] [CrossRef]
- Coleman, J.S. Social capital in the creation of human capital. Am. J. Sociol. 1988, 94, S95–S120. [Google Scholar] [CrossRef]
- Lin, N. Social Capital: A Theory of Social Structure and Action; Cambridge University Press: Cambridge, UK, 2001. [Google Scholar]
- Adler, P.S.; Kwon, S.W. Social capital: Prospects for a new concept. Acad. Manag. Rev. 2002, 27, 17–40. [Google Scholar] [CrossRef]
- Inkpen, A.C.; Tsang, E.W.K. Social Capital, Networks, and Knowledge Transfer. Acad. Manag. Rev. 2005, 30, 146–165. [Google Scholar] [CrossRef]
- Nahapiet, J.; Ghoshal, S. Social capital, intellectual capital, and the organizational advantage. Acad. Manag. Rev. 1998, 23, 242–266. [Google Scholar] [CrossRef]
- Putnam, R.D. Bowling Alone: America’s Declining Social Capital. J. Democr. 1995, 6, 65–78. [Google Scholar] [CrossRef]
- Appel, L. Testing the validity of social capital measures in the study of information and communication technologies. Inf. Commun. Soc. 2014, 17, 398–416. Available online: http://resolver.scholarsportal.info/resolve/1369118x/v17i0004/398_ttvoscsoiact.xml (accessed on 20 March 2022). [CrossRef]
- Claridge, T. Functions of social capital—Bonding, bridging, linking. Soc. Cap. Res. 2018, 20, 1–7. [Google Scholar] [CrossRef]
- Shen, C.; Cage, C. Exodus to the real world? Assessing the impact of offline meetups on community participation and social capital. New Media Soc. 2013, 17, 394–414. [Google Scholar] [CrossRef]
- Williams, D. On and off the ‘Net: Scales for Social Capital in an Online Era. J. Comput. Mediat. Commun. 2006, 11, 593–628. [Google Scholar] [CrossRef]
- Putnam, R.D. Bowling Alone: The Collapse and Revival Of American Community; Simon & Schuster: New York, NY, USA, 2000. [Google Scholar]
- Zhang, F.; Kaufman, D. The impacts of social interactions in MMORPGs on older adults’ social capital. Comput. Hum. Behav. 2015, 51, 495–503. [Google Scholar] [CrossRef]
- Steinkuehler, C.A.; Williams, D. Where Everybody Knows Your (Screen) Name: Online Games as “Third Places”. J. Comput. Commun. 2006, 11, 885–909. [Google Scholar] [CrossRef]
- Amegbor, P.M.; Braimah, J.A.; Adjaye-Gbewonyo, D.; Rosenberg, M.W.; Sabel, C.E. Effect of cognitive and structural social capital on depression among older adults in Ghana: A multilevel cross-sectional analysis. Arch. Gerontol. Geriatr. 2020, 89, 104045. [Google Scholar] [CrossRef]
- Boen, F.; Pelssers, J.; Scheerder, J.; Vanbeselaere, N.; Vos, S.; Hurkmans, E.; Smits, T.; Fransen, K. Does Social Capital Benefit Older Adults’ Health and Well-Being? The Mediating Role of Physical Activity. J. Aging Health 2020, 32, 688–697. [Google Scholar] [CrossRef]
- Kim, A.C.H.; Ryu, J.; Lee, C.; Kim, K.M.; Heo, J. Sport Participation and Happiness Among Older Adults: A Mediating Role of Social Capital. J. Happiness Stud. 2021, 22, 1623–1641. [Google Scholar] [CrossRef]
- Nyqvist, F.; Forsman, A.K.; Giuntoli, G.; Cattan, M. Social capital as a resource for mental well-being in older people: A systematic review. Aging Ment. Health 2013, 17, 394–410. [Google Scholar] [CrossRef]
- Caïs, J.; Torrente, D.; Bolancé, C. The Effects of Economic Crisis on Trust: Paradoxes for Social Capital Theory. Soc. Indic. Res. 2021, 153, 173–192. [Google Scholar] [CrossRef]
- Page-Tan, C. Bonding, bridging, and linking social capital and social media use: How hyperlocal social media platforms serve as a conduit to access and activate bridging and linking ties in a time of crisis. Nat. Hazards 2021, 105, 2219–2240. [Google Scholar] [CrossRef]
- Aldrich, D.P. Building Resilience: Social Capital in Post-Disaster Recovery; University of Chicago Press: Chicago, IL, USA, 2015; Available online: https://press.uchicago.edu/ucp/books/book/chicago/B/bo13601684.html (accessed on 10 February 2020).
- Aldrich, D.P.; Sawada, Y. The physical and social determinants of mortality in the 3.11 tsunami. Soc. Sci. Med. 2015, 124, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, R.L.; Maurer, K. Bonding, Bridging and Linking: How Social Capital Operated in New Orleans following Hurricane Katrina. Br. J. Soc. Work. 2010, 40, 1777–1793. [Google Scholar] [CrossRef]
- Lu, N.; Zhang, J. A multiple-group analysis of social Capital and loneliness among community-dwelling older adults in urban China during the outbreak of the COVID-19 pandemic. Aging Ment. Health 2023, 27, 1368–1376. [Google Scholar] [CrossRef]
- Sato, K.; Kondo, N.; Kondo, K. Pre-pandemic individual- and community-level social capital and depressive symptoms during COVID-19: A longitudinal study of Japanese older adults in 2019–21. Health Place 2022, 74, 102772. [Google Scholar] [CrossRef]
- Zhang, P.; Liu, X.; Zhang, R.; Xia, N. Depression mediates the relationship between social capital and health-related quality of life among Chinese older adults in the context of the COVID-19 pandemic: A cross-sectional study. Nurs. Open 2023, 10, 6517–6526. [Google Scholar] [CrossRef]
- Nielsen, K. A Time of COVID-19 in Ontario. Global News. 2020. Available online: https://globalnews.ca/news/6859636/ontario-coronavirus-timeline/ (accessed on 6 March 2022).
- Westoll, N. Coronavirus: Ontario Government Orders Shutdown of All Outdoor Recreation Amenities. Global News. 2020. Available online: https://globalnews.ca/news/6754560/coronavirus-ontario-outdoor-recreation-amenities-closure-order/ (accessed on 6 March 2022).
- Rodrigues, G. ‘Ontario Is Now in the 2nd Wave of COVID-19′: Premier Doug Ford Says. Global News. 2020. Available online: https://globalnews.ca/news/7364019/ontario-second-wave-coronavirus-doug-ford/ (accessed on 6 March 2022).
- Syed, F. Ontario’s Chaotic Third Wave: A Timeline—Chatelaine. Chatelaine. 2021. Available online: https://www.chatelaine.com/living/politics/ontario-third-wave-timeline/ (accessed on 8 March 2022).
- Clarke, V.; Braun, V. Thematic analysis. J. Posit. Psychol. 2016, 12, 297–298. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Thematic Analysis. In APA Handbook of Research Methods in Psychology, Research Designs: Quantitative, Qualitative, Neuropsychological, and Biological; Cooper, H., Camic, P.M., Long, D.L., Panter, A.T., Rindskopf, D., Sher, K.J., Eds.; American Psychological Association: Washington, DC, USA, 2012; Volume 2, pp. 57–71. [Google Scholar]
- Braun, V.; Clarke, V. Successful Qualitative Research: A Practical Guide for Beginners; SAGE Publications Ltd.: London, UK, 2013; p. 400. [Google Scholar]
- Braun, V.; Clarke, V. Is thematic analysis used well in health psychology? A critical review of published research, with recommendations for quality practice and reporting. Health Psychol. Rev. 2023, 1–24. [Google Scholar] [CrossRef]
- Szolin, K.; Kuss, D.J.; Nuyens, F.M.; Griffiths, M.D. “I am the character, the character is me”: A thematic analysis of the user-avatar relationship in videogames. Comput. Hum. Behav. 2023, 143, 107694. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, L.; Katsiris, A.; Lecompte, M.; Skrotzki, C.; Yang, L. A Qualitative Analysis of Older Adults’ Cognitive Appraisal in Coping during the COVID-19 Pandemic: The Role of Social Capital. COVID 2023, 3, 1622-1638. https://doi.org/10.3390/covid3100111
Dong L, Katsiris A, Lecompte M, Skrotzki C, Yang L. A Qualitative Analysis of Older Adults’ Cognitive Appraisal in Coping during the COVID-19 Pandemic: The Role of Social Capital. COVID. 2023; 3(10):1622-1638. https://doi.org/10.3390/covid3100111
Chicago/Turabian StyleDong, Linying, Alexandra Katsiris, Mariah Lecompte, Cassandra Skrotzki, and Lixia Yang. 2023. "A Qualitative Analysis of Older Adults’ Cognitive Appraisal in Coping during the COVID-19 Pandemic: The Role of Social Capital" COVID 3, no. 10: 1622-1638. https://doi.org/10.3390/covid3100111