

Learning from the COVID-19 Pandemic and AKI Evolution for Extracorporeal and Adsorption Techniques in Kidney Replacement Therapy
 , , ,
, , ,
Abstract
:1. Introduction
2. Incidence
3. Pathophysiology
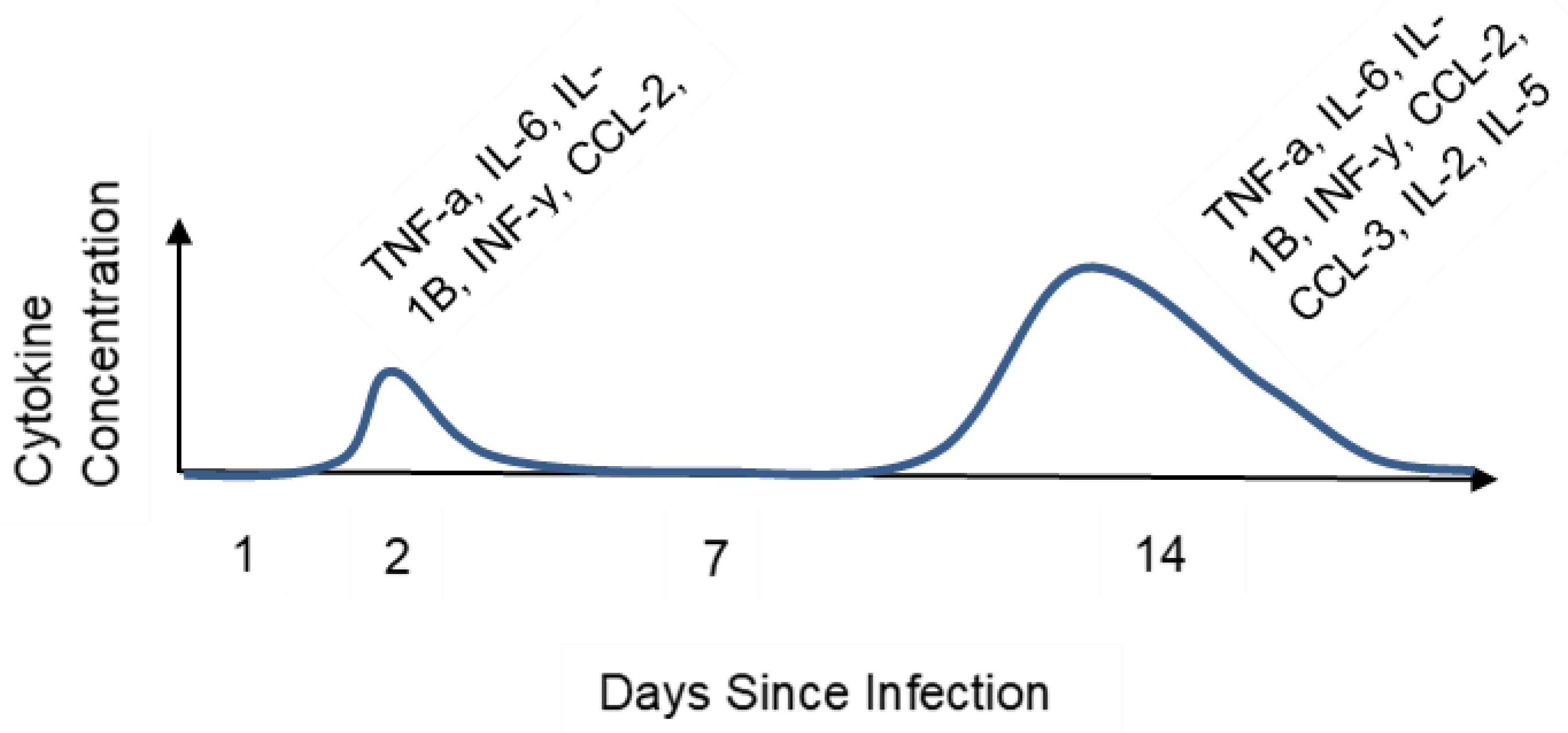
4. Cytokine Storm Syndrome
5. AKI and COVID-19
6. Extracorporeal Therapy
7. High-Flow Continuous Kidney Replacement Therapy
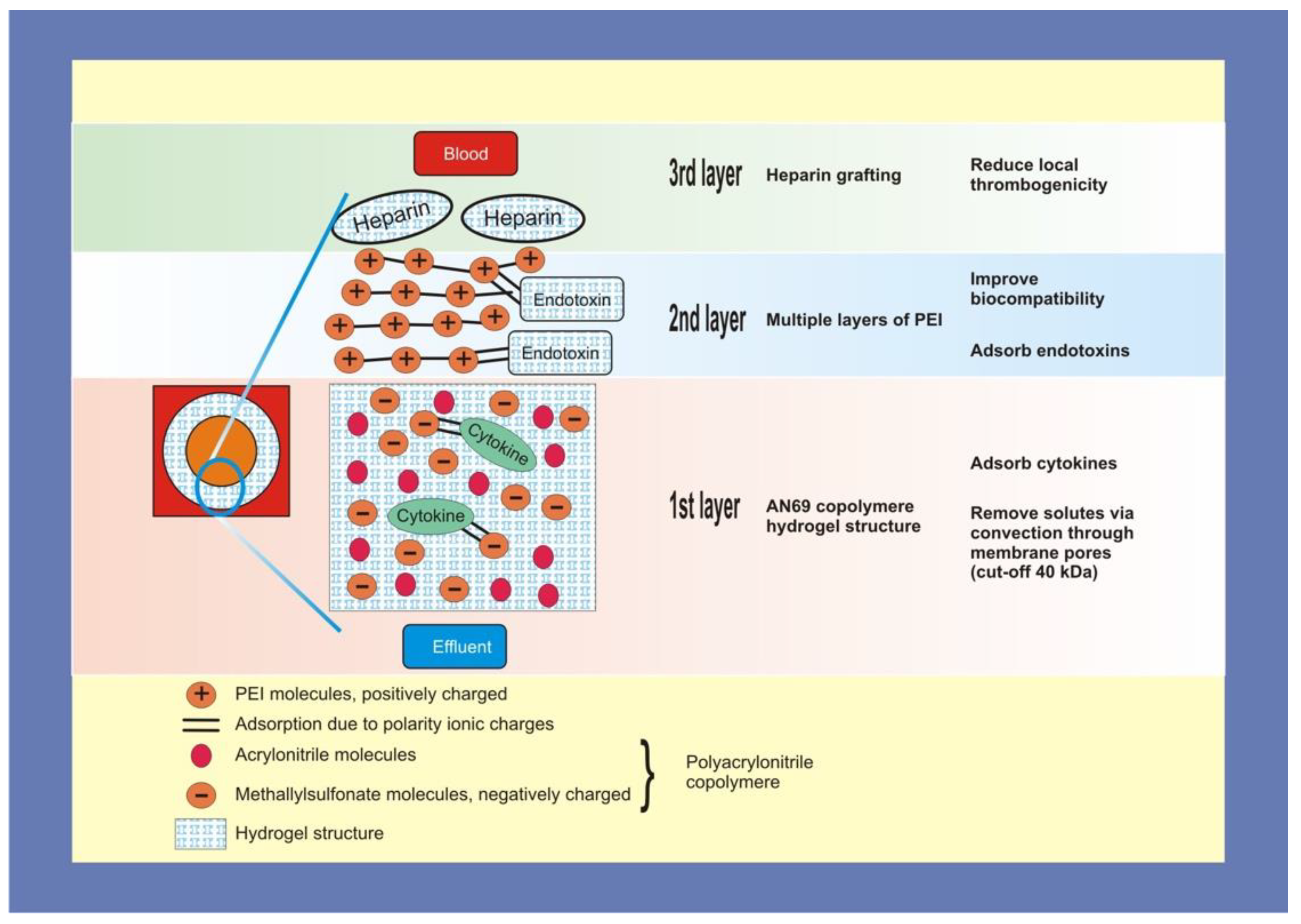
8. oXiris
9. CytoSorb
10. Other Modalities
11. Supporting Studies
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Helmy, Y.A.; Fawzy, M.; Elaswad, A.; Sobieh, A.; Kenney, S.P.; Shehata, A.A. The COVID-19 Pandemic: A Comprehensive Review of Taxonomy, Genetics, Epidemiology, Diagnosis, Treatment, and Control. J. Clin. Med. 2020, 9, 1225. [Google Scholar] [CrossRef] [PubMed]
- Boregowda, U.; Gandhi, D.; Jain, N.; Khanna, K.; Gupta, N. Comprehension Literature Review and Evidence evaluation of Experimental Treatment in COVID 19 Contagion. Clin. Med. Insights: Circ. Respir. Pulm. Med. 2020, 14, 1–7. [Google Scholar] [CrossRef]
- Chen, Y.T.; Shao, S.C.; Lai, E.C.C.; Hung, M.J.; Chen, Y.C. Mortality rate of acute kidney injury in SARS, MERS, and COVID-19 infection: A systematic review and meta-analysis. Crit. Care 2020, 24, 439. [Google Scholar] [CrossRef] [PubMed]
- COVID Data Tracker. Center for Disease Control and Prevention. Available online: https://covid.cdc.gov/covid-data-tracker/#datatracker-home (accessed on 16 April 2021).
- Villa, G.; Romagnoli, S.; De Rosa, S.; Greco, M.; Resta, M.; Pomarè Montin, D.; Prato, F.; Patera, F.; Ferrari, F.; Rotondo, G.; et al. Blood purification therapy with a hemodiafilter featuring enhanced adsorptive properties for cytokine removal in patients presenting COVID-19: A pilot study. Crit. Care 2020, 24, 605. [Google Scholar] [CrossRef]
- Supady, A.; Duerschmied, D.; Bode, C.; Rieder, M.; Lother, A. Extracorporeal cytokine adsorption as an alternative to pharmacological inhibition of IL-6 in COVID-19. Crit. Care 2020, 24, 51. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7439244/ (accessed on 28 August 2022). [CrossRef]
- Rabi, F.A.; Al Zoubi, M.S.; Kasasbeh, G.A.; Salameh, D.M.; Al-Nasser, A.D. SARS-CoV-2 and Coronavirus Disease 2019: What We Know So Far. Pathogens 2020, 9, 231. [Google Scholar] [CrossRef]
- Raina, R.; Chakraborty, R.; Sethi, S.K.; Bunchman, T. Kidney Replacement Therapy in COVID-19 Induced Kidney Failure and Septic Shock: A Pediatric Continuous Renal Replacement Therapy [PCRRT] Position on Emergency Preparedness with Resource Allocation. Front. Pediatr. 2020, 8, 413. [Google Scholar] [CrossRef]
- Fabrizi, F.; Alfieri, C.M.; Cerutti, R.; Lunghi, G.; Messa, P. COVID-19 and Acute Kidney Injury: A Systematic Review and Meta-Analysis. Pathogens 2020, 9, 1052. [Google Scholar] [CrossRef]
- Neerukonda, S.N.; Katneni, U. A Review on SARS-CoV-2 Virology, Pathophysiology, Animal Models, and Anti-Viral Interventions. Pathogens 2020, 9, 426. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Felsenstein, S.; Herbert, J.A.; McNamara, P.S.; Hedrich, C.M. COVID-19: Immunology and treatment options. Clin. Immunol. 2020, 215, 108448. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Sun, H.; Guo, P.; Zhang, L.; Wang, F. Serum Interleukin-6 Concentrations and the Severity of COVID-19 Pneumonia: A Retrospective Study at a Single Center in Bengbu City, Anhui Province, China, in January and February 2020. Med. Sci. Monit. 2020, 26, e926941. [Google Scholar] [CrossRef]
- Słomka, A.; Kowalewski, M.; Żekanowska, E. Coronavirus Disease 2019 (COVID–19): A Short Review on Hematological Manifestations. Pathogens 2020, 9, 493. [Google Scholar] [CrossRef]
- Singh, Y.P.; Chhabra, S.C.; Lashkari, K.; Taneja, A.; Garg, A.; Chandra, A.; Chhabra, M.; Singh, G.P.; Jain, S. Hemoadsorption by extracorporeal cytokine adsorption therapy (CytoSorb®) in the management of septic shock: A retrospective observational study. Int. J. Artif. Organs. 2020, 43, 372–378. [Google Scholar] [CrossRef]
- Min, C.-K.; Cheon, S.; Ha, N.-Y.; Sohn, K.M.; Kim, Y.; Aigerim, A.; Shin, H.M.; Choi, J.-Y.; Inn, K.-S.; Kim, J.-H.; et al. Comparative and kinetic analysis of viral shedding and immunological responses in MERS patients representing a broad spectrum of disease severity. Sci. Rep. 2016, 6, 25359. [Google Scholar] [CrossRef]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.; Li, B.; Song, X.; Zhou, X. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef]
- Zhang, J.; Hao, Y.; Ou, W.; Ming, F.; Liang, G.; Qian, Y.; Cai, Q.; Dong, S.; Hu, S.; Wang, W.; et al. Serum interleukin-6 is an indicator for severity in 901 patients with SARS-CoV-2 infection: A cohort study. J. Transl. Med. 2020, 18, 406. [Google Scholar] [CrossRef]
- DeDiego, M.L.; Nieto-Torres, J.L.; Regla-Nava, J.A.; Jimenez-Guardeño, J.M.; Fernandez-Delgado, R.; Fett, C.; Castaño-Rodriguez, C.; Perlman, S.; Enjuanes, L. Inhibition of NF-κB-mediated inflammation in severe acute respiratory syndrome coronavirus-infected mice increases survival. J. Virol. 2014, 88, 913–924. [Google Scholar] [CrossRef]
- Huang, K.J.; Su, I.J.; Theron, M.; Wu, Y.C.; Lai, S.K.; Liu, C.C.; Lei, H.Y. An interferon-gamma-related cytokine storm in SARS patients. J. Med. Virol. 2005, 75, 185–194. [Google Scholar] [CrossRef]
- Jiang, Y.; Xu, J.; Zhou, C.; Wu, Z.; Zhong, S.; Liu, J.; Luo, W.; Chen, T.; Qin, Q.; Deng, P. Characterization of cytokine/chemokine profiles of severe acute respiratory syndrome. Am. J. Respir. Crit. Care Med. 2005, 171, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Coperchini, F.; Chiovato, L.; Croce, L.; Magri, F.; Rotondi, M. The cytokine storm in COVID-19: An overview of the involvement of the chemokine/chemokine-receptor system. Cytokine Growth Factor Rev. 2020, 53, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Schulert, G.S.; Grom, A.A. Macrophage activation syndrome and cytokine-directed therapies. Best Pract Res. Clin. Rheumatol. 2014, 28, 277–292. [Google Scholar] [CrossRef] [PubMed]
- Snijder, E.J.; van der Meer, Y.; Zevenhoven-Dobbe, J.; Onderwater, J.J.; van der Meulen, J.; Koerten, H.K.; Mommaas, A.M. Ultrastructure and origin of membrane vesicles associated with the severe acute respiratory syndrome coronavirus replication complex. J. Virol. 2006, 80, 5927–5940. [Google Scholar] [CrossRef]
- Chan, J.F.; Lau, S.K.; To, K.K.; Cheng, V.C.; Woo, P.C.; Yuen, K.Y. Middle East respiratory syndrome coronavirus: Another zoonotic betacoronavirus causing SARS-like disease. Clin. Microbiol. Rev. 2015, 28, 465–522. [Google Scholar] [CrossRef]
- Barnes, B.J.; Adrover, J.M.; Baxter-Stoltzfus, A.; Borczuk, A.; Cools-Lartigue, J.; Crawford, J.M.; Daßler-Plenker, J.; Guerci, P.; Huynh, C.; Knight, J.S.; et al. Targeting potential drivers of COVID-19: Neutrophil extracellular traps. J. Exp. Med. 2020, 217, e20200652. [Google Scholar] [CrossRef]
- Apetrii, M.; Enache, S.; Siriopol, D.; Burlacu, A.; Kanbay, A.; Kanbay, M.; Scripcariu, D.; Covic, A. A brand-new cardiorenal syndrome in the COVID-19 setting. Clin. Kidney. J. 2020, 13, 291–296. [Google Scholar] [CrossRef]
- Izzedine, H.; Jhaveri, K.D.; Perazella, M.A. COVID-19 therapeutic options for patients with kidney disease. Kidney Int. 2020, 97, 1297–1298. [Google Scholar] [CrossRef]
- Sebastian, R.; Arunachalam, J.; Rajendran, M. Temporal Clustering of Anti-glomerular Basement Membrane Disease in COVID-19 Pandemic: A Case Series. Int. J. Nephrol. Renovasc. Dis. 2021, 14, 393–398. [Google Scholar] [CrossRef]
- Allez, M.; Denis, B.; Bouaziz, J.D.; Battistella, M.; Zagdanski, A.M.; Bayart, J.; Lazaridou, I.; Gatey, C.; Pillebout, E.; Chaix Baudier, M.L.; et al. COVID-19-Related IgA Vasculitis. Arthritis Rheumatol. 2020, 72, 1952–1953. [Google Scholar] [CrossRef]
- Kolhe, N.V.; Fluck, R.J.; Selby, N.M.; Taal, M.W. Acute kidney injury associated with COVID-19: A retrospective cohort study. PLoS Med. 2020, 17, e1003406. [Google Scholar] [CrossRef]
- Gomez, H.; Ince, C.; De Backer, D.; Pickkers, P.; Payen, D.; Hotchkiss, J.; Kellum, J.A. A unified theory of sepsis-induced acute kidney injury: Inflammation, microcirculatory dysfunction, bioenergetics, and the tubular cell adaptation to injury. Shock 2014, 41, 3–11. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506, Correction in Lancet 2020, 395, 496. [Google Scholar] [CrossRef]
- Patel, N.; Rein, J.L.; Sanchez-Russo, L.; Winston, J.; Uribarri, J. COVID-19-Associated Acute Kidney Injury: A Case Series. Kidney Med. 2020, 2, 668–669. [Google Scholar] [CrossRef]
- Jhaveri, K.D.; Meir, L.R.; Chang, B.S.F.; Parikh, R.; Wanchoo, R.; Barilla-LaBarca, M.L.; Bijol, V.; Hajizadeh, N. Thrombotic microangiopathy in a patient with COVID-19. Kidney Int. 2020, 98, 509–512. [Google Scholar] [CrossRef]
- Lewis, D.H.; Chan, D.L.; Pinheiro, D.; Armitage-Chan, E.; Garden, O.A. The immunopathology of sepsis: Pathogen recognition, systemic inflammation, the compensatory anti-inflammatory response, and regulatory T cells. J. Vet. Intern. Med. 2012, 26, 457–482. [Google Scholar] [CrossRef]
- Nadim, M.K.; Forni, L.G.; Mehta, R.L.; Connor, M.J., Jr.; Liu, K.D.; Ostermann, M.; Rimmelé, T.; Zarbock, A.; Bell, S.; Bihorac, A.; et al. COVID-19-associated acute kidney injury: Consensus report of the 25th Acute Disease Quality Initiative (ADQI) Workgroup. Nat. Rev. Nephrol. 2020, 16, 747–764. [Google Scholar] [CrossRef]
- Padala, S.A.; Vakiti, A.; White, J.J.; Mulloy, L.; Mohammed, A. First Reported Use of Highly Adsorptive Hemofilter in Critically Ill COVID-19 Patients in the USA. J. Clin. Med. Res. 2020, 12, 454–457. [Google Scholar] [CrossRef]
- Salvatori, G.; Ricci, Z.; Bonello, M.; Ratanarat, R.; D’Intini, V.; Brendolan, A.; Dan, M.; Piccinni, P.; Bellomo, R.; Ronco, C. First clinical trial for a new CRRT machine: The Prismaflex. Int. J. Artif. Organs 2004, 27, 404–409. [Google Scholar] [CrossRef]
- Shum, H.P.; Chan, K.C.; Kwan, M.C.; Yan, W.W. Application of endotoxin and cytokine adsorption haemofilter in septic acute kidney injury due to Gram-negative bacterial infection. Hong Kong Med. J. 2013, 19, 491–497. [Google Scholar] [CrossRef] [Green Version]
- Broman, M.E.; Hansson, F.; Vincent, J.L.; Bodelsson, M. Endotoxin and cytokine reducing properties of the oXiris membrane in patients with septic shock: A randomized crossover double-blind study. PLoS ONE 2019, 14, e0220444. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Xia, P.; Zhou, Y.; Liu, Z.; Zhou, X.; Wang, J.; Li, T.; Yan, X.; Chen, L.; Zhang, S.; et al. Potential effect of blood purification therapy in reducing cytokine storm as a late complication of critically ill COVID-19. Clin. Immunol. 2020, 214, 108408. [Google Scholar] [CrossRef] [PubMed]
- Schwindenhammer, V.; Girardot, T.; Chaulier, K.; Grégoire, A.; Monard, C.; Huriaux, L.; Illinger, J.; Leray, V.; Uberti, T.; Crozon-Clauzel, J.; et al. oXiris® Use in Septic Shock: Experience of Two French Centres. Blood Purif. 2019, 47 (Suppl. 3), 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ugurov, P.; Popevski, D.; Gramosli, T.; Neziri, D.; Vuckova, D.; Gjorgon, M.; Stoicovski, E.; Marinkovic, S.; Veljanovska-Kiridjievska, L.; Ignevska, K.; et al. Early Initiation of Extracorporeal Blood Purification Using the AN69ST (oXiris®) Hemofilter as a Treatment Modality for COVID-19 Patients: A Single-Centre Case Series. Braz. J. Cardiovasc. Surg. 2020. published online ahead of print. [Google Scholar] [CrossRef]
- Turani, F.; Barchetta, R.; Falco, M.; Busatti, S.; Weltert, L. Continuous Renal Replacement Therapy with the Adsorbing Filter oXiris in Septic Patients: A Case Series. Blood Purif. 2019, 47 (Suppl 3), 1–5. [Google Scholar] [CrossRef]
- Guan, M.; Wang, H.; Tang, X.; Zhao, Y.; Wang, F.; Zhang, L.; Fu, P. Continuous Renal Replacement Therapy with Adsorbing Filter oXiris in Acute Kidney Injury with Septic Shock: A Retrospective Observational Study. Front. Med. 2022, 9, 789623. [Google Scholar] [CrossRef]
- Xie, J.; Xiao, W.; Lin, J. Effect of oXiris-CVVH on the Clinical Outcomes of Patients with Septic Shock: An Inverse Probability of Treatment-Weighted Analysis. Blood Purif. 2022, 1–18. [Google Scholar] [CrossRef]
- Rizvi, S.; Danic, M.; Silver, M.; LaBond, V. Cytosorb filter: An adjunct for survival in the COVID-19 patient in cytokine storm? a case report. Heart Lung. 2021, 50, 44–50. [Google Scholar] [CrossRef]
- Hawchar, F.; László, I.; Öveges, N.; Trásy, D.; Ondrik, Z.; Molnar, Z. Extracorporeal cytokine adsorption in septic shock: A proof of concept randomized, controlled pilot study. J. Crit. Care 2019, 49, 172–178. [Google Scholar] [CrossRef]
- Wei, T.; Chen, Z.; Li, P.; Tang, X.; Marshall, M.R.; Zhang, L.; Fu, P. Early use of endotoxin absorption by oXiris in abdominal septic shock: A case report. Medicine 2020, 99, e19632. [Google Scholar] [CrossRef]
- Schädler, D.; Pausch, C.; Heise, D.; Meier-Hellmann, A.; Brederlau, J.; Weiler, N.; Marx, G.; Putensen, C.; Spies, C.; Jörres, A.; et al. The effect of a novel extracorporeal cytokine hemoadsorption device on IL-6 elimination in septic patients: A randomized controlled trial. PLoS ONE 2017, 12, e0187015. [Google Scholar] [CrossRef]
- Supady, A.; Weber, E.; Rieder, M.; Lother, A.; Niklaus, T.; Zahn, T.; Frech, F.; Müller, S.; Kuhl, M.; Benk, C.; et al. Cytokine adsorption in patients with severe COVID-19 pneumonia requiring extracorporeal membrane oxygenation (CYCOV): A single centre, open-label, randomised, controlled trial. Lancet Respir. Med. 2021. published online ahead of print. [Google Scholar] [CrossRef]
- Moore, J.B.; June, C.H. Cytokine release syndrome in severe COVID-19. Science 2020, 368, 473–474. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Huang, S.; Yin, L. The cytokine storm and COVID-19. J. Med. Virol. 2021, 93, 250–256. [Google Scholar] [CrossRef]
- Pomarè Montin, D.; Ankawi, G.; Lorenzin, A.; Neri, M.; Caprara, C.; Ronco, C. Biocompatibility and Cytotoxic Evaluation of New Sorbent Cartridges for Blood Hemoperfusion. Blood Purif. 2018, 46, 187–195. [Google Scholar] [CrossRef]
- Ankawi, G.; Fan, W.; Pomarè Montin, D.; Lorenzin, A.; Neri, M.; Caprara, C.; de Cal, M.; Ronco, C. A New Series of Sorbent Devices for Multiple Clinical Purposes: Current Evidence and Future Directions. Blood Purif. 2019, 47, 94–100. [Google Scholar] [CrossRef]
- Huang, Z.; Wang, S.R.; Yang, Z.L.; Liu, J.Y. Effect on extrapulmonary sepsis-induced acute lung injury by hemoperfusion with neutral microporous resin column. Ther. Apher. Dial. 2013, 17, 454–461. [Google Scholar] [CrossRef]
- Zhou, F.; Peng, Z.; Murugan, R.; Kellum, J.A. Blood purification and mortality in sepsis: A meta-analysis of randomized trials. Crit. Care Med. 2013, 41, 2209–2220. [Google Scholar] [CrossRef]
- Payen, D.M.; Guilhot, J.; Launey, Y.; Lukaszewicz, A.C.; Kaaki, M.; Veber, B.; Pottecher, J.; Joannes-Boyau, O.; Martin-Lefevre, L.; Jabaudon, M.; et al. Early use of polymyxin B hemoperfusion in patients with septic shock due to peritonitis: A multicenter randomized control trial. Intensive Care Med. 2015, 41, 975–984. [Google Scholar] [CrossRef]
- Poli, E.C.; Alberio, L.; Bauer-Doerries, A.; Marcucci, C.; Roumy, A.; Kirsch, M.; Stefano, E.; Liaudet, L.; Schneider, A. Cytokine clearance with CytoSorb® during cardiac surgery: A pilot randomized controlled trial. Crit. Care 2019, 23, 108. [Google Scholar] [CrossRef] [Green Version]
- Buckley, L.F.; Wohlford, G.F.; Ting, C.; Alahmed, A.; Van Tassell, B.W.; Abbate, A.; Devlin, J.W.; Libby, P. Role for Anti-Cytokine Therapies in Severe Coronavirus Disease 2019. Crit. Care Explor. 2020, 2, e0178. [Google Scholar] [CrossRef]
- Pei, G.; Zhang, Z.; Peng, J.; Liu, L.; Zhang, C.; Yu, C.; Ma, Z.; Huang, Y.; Liu, W.; Yao, Y.; et al. Renal Involvement and Early Prognosis in Patients with COVID-19 Pneumonia. J. Am. Soc. Nephrol. 2020, 31, 1157–1165. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1295. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Correction to: Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 1294–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Cytokines | Origin | Function |
|---|---|---|
| IL-1 | Macrophages | Induces fever, acute inflammation, T-cell stimulation Induces chemokine secretion for leukocyte recruitment Activates endothelium through adhesion molecule expression |
| IL-2 | T-cells | Stimulates T cells (regulatory, cytotoxic, killer) and NK cells |
| IL-6 | Multiple cells | Stimulates acute-phase protein production |
| IL-10 | Multiple cells | Attenuates inflammation: decreases MHC class II expression and Th1 cytokines; selectively inhibits macrophages and dendritic cells |
| IL-18 | Adrenal gland, osteoblasts | Released by adrenal gland during periods of stress Osteoblast-derived form results in suppressed osteoclast development |
| IL-33 | Lung epithelial cells | Innate and adaptive immune response Interacts with immune cells causing airway inflammation, tissue remodeling [16] |
| GM-CSF | Macrophages Fibroblasts T cells | Activates macrophages and induces myeloid cell-line differentiation |
| TGF-β | Abundant cells | Angiogenesis Fibroblast proliferation plus collagen synthesis Inhibits pro-inflammatory cytokines |
| IFN-α | Infected cells Plasmacytoid Dendritic cells | Innately immune against viral infections; activates ribonuclease and destroys viral mRNA Adjunctive treatment in Kaposi sarcoma, chronic hepatitis B and C |
| IFN-γ | T cells | Activates T cells, NK cells and macrophages |
| CXCL9 | Macrophages | T-cell trafficking; chemoattracts lymphocytes |
| CXCL10 | Many cells | Induces stimulation of NK cells, monocytes and T cells |
| CCL2 [17] | Many cells | Chemotaxis for monocytes and basophils Implicated in respiratory distress syndrome, psoriasis and atherosclerosis |
| CCL3 | Marrow cells | Directs stimulation of osteoclast production |
| CCL5 | Eosinophil granules Basophils | Stimulates release of histamine from basophils, activates eosinophils |
| Layer | Composition | Charge | Structure | Function |
|---|---|---|---|---|
| First | Polyacrylonitrile copolymer | Negative |  | Absorb cytokines |
| Second | Polyethyleneimine | Positive |  | Absorb endotoxins |
| Third | Heparin | Negative |  | Decrease systemic thrombogenicity |
| Emergency Use Authorization for the United States | oXiris Set Was Authorized by the FDA for Treatment of Patients with COVID-19 Infection in April of 2020 |
|---|---|
| Intended Use | oXiris Set is indicated for use for patients meeting all the following criteria:
|
| Indicated dialysis machine | For use only with the Prismaflex control unit or with the Prismax control unit |
| Indicated venovenous therapies | For use in slow continuous ultrafiltration (SCUF), continuous venovenous hemofiltration (CVVH), continuous venovenous hemodialysis (CVVHD), continuous venovenous hemodiafiltration (CVVHDF) |
| Absolute contraindications |
|
| Relative contraindications |
|
| Special considerations |
|
| Trial | Population | N | Duration | Intervention | Major Findings | Date |
|---|---|---|---|---|---|---|
| Padala [39] | Critically ill COVID-19; respiratory failure and septic shock | 3 | 72 h | oXiris® hemofilter CVVHDF | oXiris® filter significantly decreased CRP, IL-6 and D-dimer levels No side effects of oXiris® filter | 25 June 2020 |
| Hong Kong [41] | Gram-negative sepsis with AKI | 7 | 61 (35–72) h | oXiris® hemofilter CVVHDF | Sequential organ failure assessment score reduced by 37% at 48 h following oXiris–CVVHDF vs. 3% increase in historical controls | October 2011 to June 2012 |
| Broman [42] | Septic shock-associated AKI with endotoxin levels > 0.03 EU/mL | 16 | 24 h | CKRT with an oXiris filter or with a standard filter | Endotoxin concentration decreased more in oXiris vs. standard filter group at 3, 8 and 16 h (p = 0.02, 0.02 and 0.05, respectively) First treatment: endotoxin levels decreased in 7/9 (77.8%) with oXiris vs. 1/6 (16.7%) with standard filter group (p = 0.02) Levels of TNF-α, IL-6, IL-8 and IFN-γ decreased more with oXiris filter | 6 March 2019 |
| Ma [43] | Critically ill patients with COVID-19 | 3 | 3 months | CKRT with oXiris filter | Reduced CRP and IL-6 in six days in one patient; normalized cytokines in two days in another | January–March 2020 |
| Schwindenhammer [44] | Septic shock; hospitalized in ICU | 31 | 17 h (5–54) | CKRT with oXiris filter | 88% relative decrease in median norepinephrine dose Survival benefit for most patients | December 2014–January 2019 |
| Zhang [19] | COVID-19 patients; CRRT in Henan | 5 | - | - | Reduced level of overexpressed cytokines and improved organ function | January 2019 to March 2020 |
| Raina [8] | COVID-19 patient; AKI class III, ARDS admitted to ICU | 1 | 72 h | oXiris filter HF-CVVHDF | Patient improved clinically with decreasing D-dimer, IL-6 and CRP | - |
| Emergency Use Authorization for the United States | CytoSorb Set Was Authorized by FDA for Treatment of Patients with COVID-19 Infection in April of 2020 |
|---|---|
| Intended use | CytoSorb Set is indicated for use for patients with all the following criteria:
|
| Indicated therapies | CytoSorb Set for use in hemoperfusion configuration, venovenous configurations with CKRT slow continuous ultrafiltration (SCUF), continuous venovenous hemofiltration (CVVH), continuous venovenous hemodialysis (CVVHD), continuous venovenous hemodiafiltration (CVVHDF) and venoarterial extracorporeal membrane oxygenation (VA-ECMO) in a blood pump circuit |
| Absolute contraindications | Patients with:
|
| Relative contraindications |
|
| Side effects |
|
| Special considerations |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raina, R.; Singh, S.; Enukonda, V.; Pandher, D.; Abboud, B.; Bhola, V.; Bagga, S.; Zehrer, T.; Desmett, A. Learning from the COVID-19 Pandemic and AKI Evolution for Extracorporeal and Adsorption Techniques in Kidney Replacement Therapy. COVID 2022, 2, 1214-1227. https://doi.org/10.3390/covid2090088
Raina R, Singh S, Enukonda V, Pandher D, Abboud B, Bhola V, Bagga S, Zehrer T, Desmett A. Learning from the COVID-19 Pandemic and AKI Evolution for Extracorporeal and Adsorption Techniques in Kidney Replacement Therapy. COVID. 2022; 2(9):1214-1227. https://doi.org/10.3390/covid2090088
Chicago/Turabian StyleRaina, Rupesh, Siddhartha Singh, Vignasiddh Enukonda, Davinder Pandher, Brian Abboud, Vishnu Bhola, Sumedha Bagga, Tara Zehrer, and Ashley Desmett. 2022. "Learning from the COVID-19 Pandemic and AKI Evolution for Extracorporeal and Adsorption Techniques in Kidney Replacement Therapy" COVID 2, no. 9: 1214-1227. https://doi.org/10.3390/covid2090088