1. Introduction
Nearly 1 in 5 people currently live with disabilities that may limit social participation. The World Health Organization identified social participation as a fundamental right [
1]. The Human Development Model-Disability Creation Process (HDM-DCP) conceptual model defined social participation as the “
total accomplishment of life habits, resulting from the interaction between personal and environmental factors” [
2]. Social participation provides opportunities for the fulfilment of basic human needs and represents a determinant of the quality of life [
3], wellbeing, and life satisfaction [
4,
5,
6]. However, people with disabilities still experience participation restrictions in their daily life [
7], with people with more severe disabilities experiencing more participation restrictions [
8].
In France, a recent survey highlighted that among individuals aged 15 and above, 14% live with a disability, and 6.6% experience significant restrictions in social participation [
9]. This survey also revealed that people with disabilities have lower employment rates, lower educational attainment, and fewer financial resources. The international community has largely embraced the idea that participation restrictions are the product of social and environmental obstacles [
10,
11]. To improve individuals with disabilities’ participation, one identified way is to act on the environment. In the context of the ‘Handicap Innovation Territoire’ (HIT, Disability Innovation Territory) project (
https://hit-lorient.bzh, accessed on 1 October 2023), actions aiming to reduce participation restrictions induced by the environment will be undertaken. To initiate such actions, it is necessary to have an understanding of the context in which action is desired. Furthermore, it is essential to acknowledge the diverse and unique nature of individuals with disabilities when considering the broader global context of disability. Recognizing the challenges related to diversity and individuality is crucial for a more comprehensive global understanding of their social participation. However, no population survey offering a systemic description of the social participation of people with disabilities in the specific environment of Britany has been conducted. This lack of information greatly limits the evaluation of projects aimed to improve social participation. Therefore, this research bridges the existing knowledge gap by addressing the lack of information regarding the social participation and perceived environment of people with disabilities in Brittany. It was essential to explore and describe the context of the social participation of people with disabilities living in Brittany (France), in relation to their perception of their social and physical environment. Thus, the objectives of the present study were (1) to describe the level of social participation of people with disabilities living in Brittany and (2) to describe their perception of their social and physical environment according to the disability group.
2. Materials and Methods
2.1. Context
The HIT project, the only project labelled as ‘Innovative Territory’ in the ‘Handicap Investment Program for the Future’ [
12] of the government of France, aims to improve the social participation of people with disabilities through initiatives conducted in Brittany before nationwide and international deployment and dissemination.
2.2. Approach and Design
A cross-sectional investigation using standardized participation and environmental factor questionnaires was conducted to document participation of people with disability. Ethical approval was received from the local institutional review boards and ethics committees, Brest Ethical Committee (France) (B2021.33) and Quebec City (Canada) (2022-2392).
2.3. Participants and Recruitment
Individuals with any diagnosis were included if they (a) were adults ≥ 18 years of age, (b) reported a disability, and (c) lived in Brittany. Individuals were excluded if they (a) had significant behavioral disorders that could impact ability to consent or to complete the evaluations, or (b) were diagnosed with a degenerative disease with rapid progression. Convenience sampling was used to recruit participants mainly through community organizations and associations, rehabilitation centers and long-term care facilities were also solicitated. To mitigate potential limitations, such as selection bias introduced by convenience sampling during recruitment and to ensure transparency, the potential participants were not initially identified and contacted by the research team. Instead, they were first identified by various local professionals who were unaware of the research project.
Based on the results of similar projects, a convenience sample size of 25 individuals was considered sufficient to explore a diversity of users’ experiences [
13].
2.4. Procedure
Participants were recruited between December 2021 and June 2022. Data were collected either during face-to-face interviews or remotely by telephone or videoconference (Webex) over one or more instances depending on participant’s preferences. Questionnaires were completed with assistance of a research assistant or independently. The duration of the interview and the completion of the questionnaire was estimated at 90 min in total. All interviews were conducted in French by the same research associate (M.N.).
2.5. Data Collection
Sociodemographic and personal characteristics were collected, including age, gender, marital status, education, employment, living arrangement, and diagnosis.
The Assessment of Life Habits (LIFE-H; version 4.0) was used to evaluate participants’ participation assessing the perceived level of achievement of 12 life habits as well as satisfaction. The 12 life habits are divided into two categories: day-to-day habits (including nutrition, fitness, personal care, communication, housing, and mobility) and social role (including responsibilities, interpersonal relationships, community life, education, working, recreation). The 77 items from the LIFE-H capture the completion of each life habit considering (1) the level of difficulty and (2) the help needed (technical, adaptation of the environment, or human). The LIFE-H gives a continuous standardized score of level of participation ranging from 0 to 10, where 0 indicates that the habit is not accomplished, and 10 indicates optimal participation without difficulty or help. A score below 3 indicates severe perturbation in life habits, a score between 4 to 7 indicates moderate perturbation, and a score over 8 indicates few or no perturbations achievement of the life habits [
14]. The LIFE-H also includes a satisfaction scale to assess the person’s appreciation in relation to their degree of achievement of the life habit; results of this scale are not considered in the score calculation. The LIFE-H has demonstrated internal coherence and test re-test validity, internal fidelity, and convergent validity [
15,
16].
The Measure of the Quality of the Environment (MQE; version 2.0) was used to assess the perceived influence of the environment on social participation [
17]. Twenty-six factors are assessed in the MQE; they are grouped into 4 domains of the environment: (1) the political economic factors (including political, juridical, economic, socio-health, and education systems, and public infrastructures and community organizations), and (2) sociocultural factors (including social network and social rules) which comprise social factors; and (3) nature (including physical geography, climate, time, sound, electricity and magnetism, and lighting) and (4) development (including architecture, national and regional development, and technology) which comprise physical factors.
Each factor is judged by the individual on a 7-point scale ranging from major facilitator (+3) to major or complete obstacle (−3), responses ‘I don’t know’ or ‘not applicable’ were also possible.
The MQE and the LIFE-H were related according to the HDM-DCP [
17]. They are widely known tools in the field of rehabilitation research and intervention in support of social integration [
16]. Authors (A.P., M.N., and M.L.G.-P.) underwent a 3-day online training provided by the International Network on the Disability Creation Process (INDCP) to learn how to use and analyze the LIFE-H and the MQE.
2.6. Data Analysis
Descriptive statistics (means, standard deviations, medians, minimum–maximum values, and frequencies) were used to present the characteristics of the participants and to describe their participation (LIFE-H) and their perception of their environment (MQE).
The Mann–Whitney U test or Kruskal–Wallis test (non-parametric one-way ANOVA) were used when applicable to compare differences in social participation and perception of the environment differences according to (age < 30 years old, between 30 and 60 years old, >60 years old) and among disability groups. Participants were grouped according to their type of disability (sensory, motor, or cognitive/mental health). When differences were found, post hoc tests were applied. Results with p-values lower than or equal to 0.05 were considered significant.
3. Results
Twenty-five individuals with disabilities were recruited. The participants were, on average, 46.0 ± 23.6 years of age; 10 (40%) were females. The majority (18; 72%) were in a civil union or were married. A total of 7 (28%) were in employment, 10 (40%) were without professional employment but were involved in volunteer activities, 3 (12%) were students, and 5 (20%) were retired. The majority (17; 68%) lived in independent housing, 6 (24%) lived in a long-term care facility, and 2 (8%) were staying with family or a spouse. Nine (36%) reported living with a motor disability (i.e., spinal cord injury, multiple sclerosis), 11 (52%) with a mental health and/or cognitive disability (i.e., bipolarity, schizophrenia, autism, Down syndrome), 5 (20%) reported having a sensory disability (deaf or blind).
3.1. Social Participation and Satisfaction
Data related to social participation were collected from 24 participants; 1 participant with Down syndrome was unable to answer the questionnaire. The participants obtained a LIFE-H mean global score of 7.7 out of 10 ± 1.4, indicating a moderate perturbation of social participation. The mean scores of the LIFE-H were the highest for the life habits related to ‘communication’, 8.8 ± 1.2; ‘nutrition’, 8.7 ± 2.0; ‘personal care’, 8.8 ± 1.5; and ‘interpersonal relationship’, 9.6 ± 0.6. In contrast, the mean scores were the lowest for ‘residence’, 6.2 ± 3.5; ‘education’, 3.9 ± 4.4; and ‘work’, 6.4 ± 4.0.
Table 1 presents the mean scores of all the life habits of the LIFE-H for the whole sample according to the disability groups. The mean scores of all the life habits of the LIFE-H according to the age and disability groups are available in the
Supplementary Material, Table S1.
The overall global score (LIFE-H satisfaction subscore) indicated that 80% of the participants reported being satisfied, while 20% expressed non-satisfaction. The domains nutrition, personal care, social role, responsibilities, daily activities, communication, fitness, and transportation presented a satisfaction higher than 80%. In contrast, education displayed the lower level of satisfaction, with only 30% of the individuals reporting satisfaction. Work revealed 64% of the individuals reporting satisfaction. The domain of leisure demonstrated a level of satisfaction of 74% of the individuals reporting satisfaction. The percentages of social participation satisfaction are available in the
Supplementary Material, Table S2.
3.2. Differences in Social Participation According to Age
According to age, the subscores of the LIFE-H showed that there were statistically significant differences in transportation between the groups “30–60 years old” and “>61 years old”, with mean scores of 8.52 (1.35) and 6.46 (0.87), respectively (p = 0.027), and between the groups “18–30 years old” and “30–60 years old”, with mean scores of 9.14 (1.02) and 8.52 (1.35), respectively (p = 0.05). The sub-scores of the LIFE-H presented that there were statistically significant differences in this condition between the three groups; the post hoc analysis presented no differences between specific groups.
3.3. Differences in Social Participation According to Disability Group
The subscores of the LIFE-H showed that there were statistically significant differences in the participations scores related to daily activities (
p = 0.031), mobility (
p = 0.006), fitness (
p = 0.03), and personal care (
p < 0.001) depending on the disability group. The differences in social participation according to the disability group and post hoc analysis are presented in
Figure 1.
3.4. Perceived Quality of Environment
The results from the MQE presented participants’ perception of whether the factors of the environment are facilitators or obstacles to social participation. Data from the MQE were collected with 21 participants; 4 were unable to answer due to the comprehension of the items and scoring system. The responses to each factor are presented in
Figure 2 (environmental facilitators and obstacles of participants’ social participation). The mean scores of environmental factors according to the age and disability groups are available in the
Supplementary Material, Table S3.
3.5. Differences in Perceived Environment According to Age
According to the age, the subscores of the MQE showed that there were statistically significant differences in the perceived environment scores related to incomes (p = 0.018), stores and services (p = 0.008), care services (p = 0.015), and access to radio and television services (p = 0.017). The post hoc analysis indicated a statistically significant difference in the ‘personal incomes’ between the groups ‘18–30 years old’ and ‘30–60 years old’, with mean scores of 3.0 ± 0.0 and 0.9 ± 1.7, respectively (p = 0.03). The post hoc analysis indicated a statistically significant difference in ‘stores and services’ between the groups ‘18–30 years old’ and ‘30–60 years old’, with mean scores of 3.0 ± 0 and −0.3 ± 2.0, respectively (p = 0.05). The post hoc analysis indicated a statistically significant difference in ‘home care services’ between the groups ‘30–60 years old’ and ‘>61 years old’, with mean scores of 1.7 ± 2.0 and −2.8 ± 0.6, respectively (p = 0.03). The post hoc analysis indicated a statistically significant difference in ‘radio and television’ between the groups ‘30–60 years old’ and ‘>61 years old’, with mean scores of 1.8 ± 1.7 and −1.3 ± 2.1, respectively (p = 0.05).
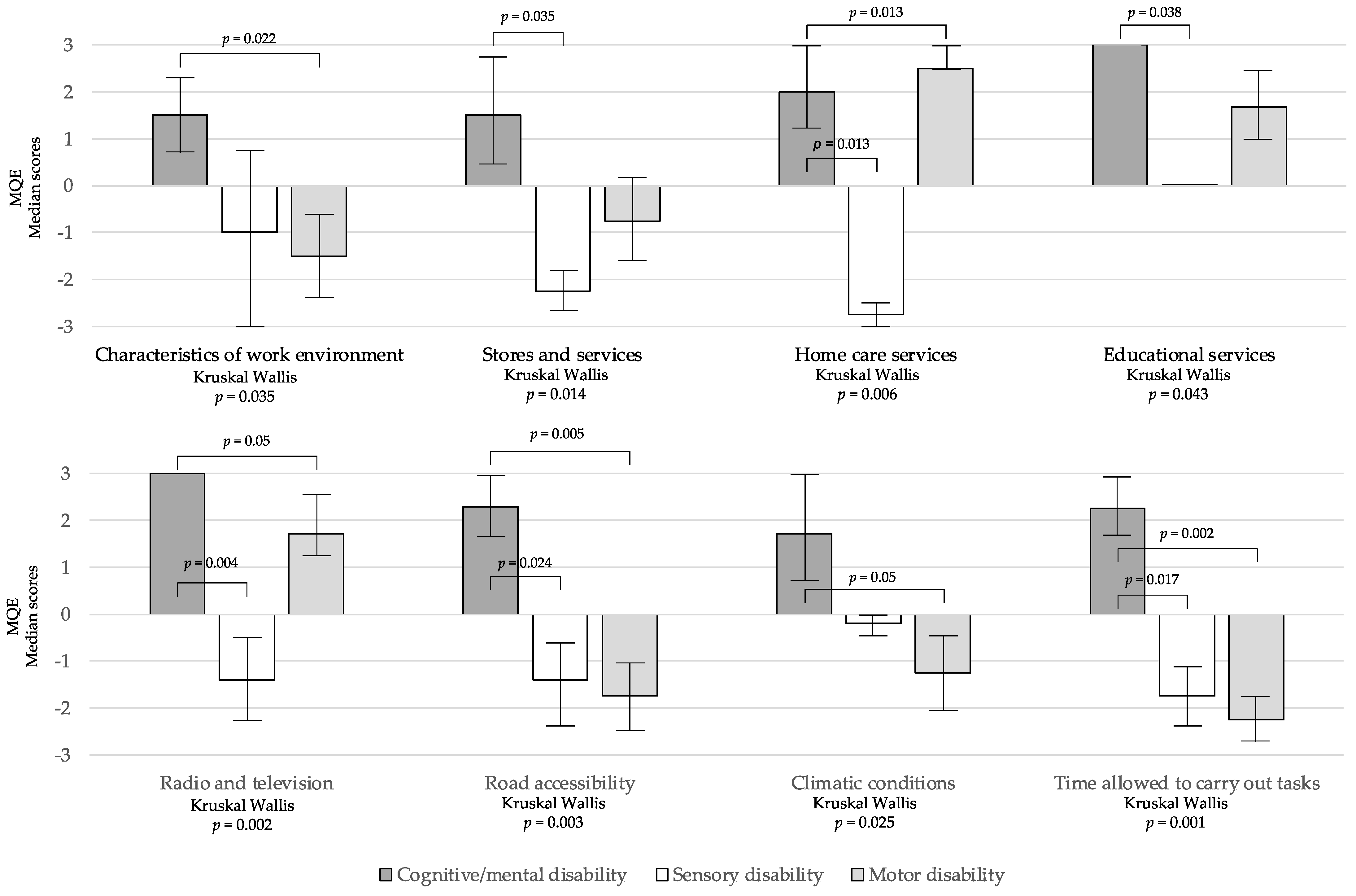
3.6. Differences in Perceived Environment According to Disability Group
The eight factors of the MQE were identified differently according to the group of disability. The scores of the MQE revealed differences in the perceived quality of the environment depending on the disability group related to ‘characteristics of work environment’ (
p = 0.035), ‘stores and services’ (
p = 0.014), ‘home care services’ (
p = 0.006), ‘educational services’ (
p = 0.043), ‘access to radio and television’ (
p = 0.002), ‘road accessibility’ (
p = 0.003), ‘climatic conditions’ (
p = 0.025) and ‘time allowed to carry out tasks’ (
p = 0.001). The differences in the perceived environment according to the disability group and post hoc analysis are presented in
Figure 3.
4. Discussion
To the best of our knowledge, this is the first study exploring social participation and factors that facilitate or limit the social participation of individuals living with disabilities in Brittany. In contrast to prior research [
18,
19,
20,
21,
22], its inclusive approach towards individuals with disabilities allows us to consider the experience of individuals with various disabilities. The results indicated a rather good global level of social participation, while also highlighting disparities among the disability groups. The findings also revealed that some environmental factors influencing social participation were perceived as barriers (i.e., time to carry out tasks, accessibility of roads, stores and services, rules and administrative procedures) and others as facilitators (support and attitudes of those around you). Also, the perception of the quality of the environment varied across the disability groups.
For the whole sample, the life habits with the highest scores were communication, transportation, nutrition, condition, personal care, responsibilities, and interpersonal relationships. On the contrary, the life habits with the lowest scores of social participation were the nature of occupation, being in work, education, and leisure. This distribution of the participation in life habits is similar to those founded in previous research investigating the social participation of individuals with spinal cord injury [
18,
19], Down syndrome [
20], mental disorders [
21], and stroke [
22]. Overall, occupational activities are more affected. Related to work, in France in 2021, people aged 15 to 64 who declare that they live with a disability are less present than others in the employment market; among them, only 44% are economically active (employed or unemployed), compared to 73% of the population [
9]. Restricted participation in work was also reported in Switzerland for individuals with spinal cord injury [
19], and internationally for individuals with various impairments [
23]. The domain of leisure activities, which represents a significant portion of daily activities, also obtained very low participation scores. This result is consistent with previous studies reporting a physical activity participation rate of 8% for wheelchair users, compared to 89% for individuals without mobility-related disabilities of the same age [
24]. It has also been previously demonstrated that the majority of adults with disabilities do not engage in any leisure activities, partly due to barriers related to the built and/or natural environment [
25,
26]. Actions are being taken to address the need for participation in leisure activities for people with disabilities.
While showing a rather good average level of social participation, the results presented disparities between the disability groups. The participants with motor disabilities reported more participation restriction in daily activities, transportation, and personal care. Accordingly, major participation restriction in such domains has previously been reported in studies [
19,
27]. A systematic literature review presented the potential positive impact of assistive living technology on the social participation of people with motor disabilities [
28]. The results of the present study associated with evidence from this systematic review suggested that actions allowing access to assistive living technology should be conducted by the HIT project to improve the social participation of people.
Also, participants with sensory disabilities reported a low level of social participation. Previous research exploring the social participation of individuals with visual and hearing disability found similar results [
29,
30]. For example, a reduced social participation in sports has been previously demonstrated [
31]. A systematic review of the literature reported that few studies were found to be related to the social participation of people with sensorial disability, due to a weak understanding of the relationship between sensory disability and social participation [
29]. Research should be conducted to continue to better understand the impacts of disabilities other than physical ones (e.g., invisible disabilities). The results of the present study are consistent with the idea that disability situations go well beyond motor aspects.
In contrast, the results of the present study did not highlight the difficulties faced by individuals with cognitive and/or mental disability. This group of participants reported higher participation levels than the other groups. However, previous studies have shown that individuals with mental disability also experience restrictions in social participation, mostly when they are not in employment [
32]. Importantly, this study grouped individuals with cognitive and/or mental disabilities into one group. Further research should differentiate such individuals, as was achieved by Orsmond and colleagues., using data from a national longitudinal study in the United States of America; this study found differences within a population of individuals with cognitive and/or mental disability [
21].
Additionally, consistent with the age-related decrease in sensorimotor and cognitive ability, the older participants in the present study had significantly more restrictions in participation related to transportation, accessing health services, stores, and media. Such restrictions of participation are in line with previous investigations proposing that ageing is associated with reduced mobility, implying participation restriction [
33] and that ageing with hearing disability is associated with a risk of frailty [
30]. The relationship between aging and disability has become a very important preoccupation for its consequences on participation, inclusion, and the quality of life and for its consequences on socio-sanitary organization [
34]. Overall, the present study confirmed that individuals with disabilities experience participation restrictions in Brittany. The results also show that their experience is dependent on the disability group and age, confirming that personal factors influence social participation [
14]. Importantly, the LIFE-H widely acknowledged that such participation restrictions stem from societal and environmental factors [
2]. The environmental factors, facilitating or restraining social participation for individuals with disability living in Brittany, are discussed in the following section.
The findings showed that the factors ‘support of those around you’ and ‘attitudes of those around you’ were considered as facilitators to social participation by most participants, exactly as previously indicated [
20]. The fundamental role of social support has already been highlighted in previous research [
35], with individuals who experienced increased social support also reporting higher life satisfaction and quality of life [
36,
37]. On the contrary, some factors were identified as obstacles. The factor ‘time allowed to carry out tasks’ was considered as an obstacle by the majority of participants. This time, like the time required for personal care, is an environmental factor for which it is up to the relatives, community, and society to adapt and accept that some individuals may need more time to complete tasks. Fortunately, several other environmental factors influencing social participation and orienting actions aim to improve social participation.
Regarding mobility, this study shows that the accessibility of roads, transportation, and accessibility to stores and services was perceived as a barrier. The results of this study also highlighted differences in participation related to mobility based on the type of disability, with individuals with mental disabilities reporting very few participation restrictions related to mobility, while those with motor and sensory disabilities reported important participation restrictions. For individuals with motor disabilities, these findings align with previous studies that have shown mobility as a factor affecting the participation of people with disabilities [
38], and was also demonstrated in studies involving the elderly [
33]. It is widely recognized by the international community that actions need to continue to be taken to improve the accessibility of physical environments [
39]. Mainly, the potential negative impact of the physical environment for individuals with disabilities, as mobility restriction have various consequences [
39]. For example, a previous study examining health care accessibility for adults with disability found that individuals reported a decline in social participation due to limited mobility resulting in the lack of access to health care services [
40]. Accordingly, the results of the present study showed that the majority of participants (67%) perceived accessibility to health care services as an obstacle to social participation. Since the 2000s, research has pointed out this is a significant concern [
41]. The results also showed that it is more the case that participants with sensorial disabilities encounter more difficulties accessing healthcare services than the other disability group. Individuals with disabilities may face physical constraints, such as limited accessibility, as well as procedural challenges, including scheduling difficulties, as previously indicated [
41]. Importantly, reduced access to health care services has negative consequences on domains such as social roles, depression, pain, fatigue, additional health care expenses, and family assistance needed [
40]. Overall, the results of the present study showed that participants with sensorial disabilities were those who perceive the most impact of their environment. They perceived several environmental factors (i.e., communication, media, transports, work environment, and stores) as impacting more negatively their social participation than the participants with motor and cognitive/mental health disability. Previous research has confirmed this result and showed that environmental obstacles, leading to participation restriction, contribute to negative feelings even leading to depressive symptoms [
42].
Limitations
The limitations of this study must be acknowledged. The relatively small sample size restricts the generalizability of our findings. This limitation implies that we had a limited number of participants in each sub-group, which, in turn, constrained the depth of our data analysis. Moreover, the convenience sample also introduces bias, and the participants may not be completely representative of the global population of people with disabilities living in Brittany. These limitations emphasize the need for caution when interpreting the results within a broader context, and they highlight opportunities for future research to explore these aspects in more depth with larger and more diverse participant groups. In addition, the active involvement in community volunteering of the participants may have influenced positively the participants’ social participation. Specifically, for the participants with cognitive and/or mental disabilities, the majority of them were recruited from institutions allowing for and supporting adapted work, indicating a good employment rate, which may have influenced the results in terms of their social participation. It would have been interesting to inquire about the participants’ level of education and the size of the city (rural/urban) in which they reside. Further research should be conducted to understand whether the level of education or living environment (urban/rural) impacts social participation among individuals with disabilities. Moreover, based on previous findings in an older population [
43], future research should aim to comprehend the LIFE-H scores of the adult general population for a comparative analysis.
On the other hand, the LIFE-H assessment tool has shown good convergent validity for individuals with mental disabilities [
44]. However, it has been highlighted that with this population, interviews are preferred to understand the complex environmental interactions that enable or restrict the social participation of individuals with mental disabilities. In line with this study, a qualitative study related to the life experiences of people with disabilities in Brittany is currently underway. The study aims to describe the facilitators and barriers to their social participation and to comprehend the cumulative impact of these factors on their life course. The findings from this ongoing research will provide further insights to enrich the understanding of the current results. Finally, there were some missing data in the social participation (LIFE-H) and perceived environment (MQE) measures. One limitation was that some individuals were not able to answer the questionnaires, mainly the MQE, resulting in missing data for three participants. The missing data were excluded from the data analysis, and the total amount of available data was systematically documented to ensure transparency. It would be interesting for future research to be conducted to understand the cognitive abilities required to answer the MQE. In previous research, this limitation was addressed by examining the parental perspective on participation with Down syndrome and the perceived environment [
20].
5. Conclusions
Therefore, the present study encompassed a wide range of disabilities. The findings revealed that individuals with disabilities in Brittany generally experience satisfactory levels of social participation, although limitations exist in the domains of employment, education, and leisure, consistent with the existing literature. The study also identified environmental factors such as accessibility to transportation, healthcare services, and administrative regulations, which may contribute to the reduced social participation among individuals with disabilities. It is crucial to note that some of these environmental factors can be addressed to promote higher levels of social participation, aligning with the objectives of the HIT project. In response to the identified areas with lower social participation rates, specific actions have been undertaken within the framework of the HIT project. These actions include targeted interventions to enhance leisure activities, as well as an internet platform for access to cultural, sports, and leisure activities being developed to evaluate and enhance the mobility accessibility in various locations. Recognizing the rich cultural, sports, tourism, and leisure offerings in the urban area, the project HIT aims to facilitate access to these opportunities for individuals with disabilities. This purpose aligns with the project’s goal of promoting social inclusion and equal participation for all members of the community. Furthermore, based on the results of the present study, an evaluation of the implemented measures, conducted as part of the HIT project, is scheduled to occur in three years. This evaluation aims to ensure continuous assessment and make any necessary adjustments to improve the social participation of people living with disabilities in Brittany.
Overall, the actions implemented in Brittany can serve as a valuable model for other regions and countries confronting similar challenges in promoting social participation for individuals with disabilities. By testing these actions in Brittany, they can be refined and tailored to suit the specific needs and dynamics of the local community. Once the effectiveness of the strategies has been proved, the intention is to disseminate these successful actions nationally and internationally. This sharing of knowledge and best practices can contribute to a broader, global effort to enhance social inclusion and participation for people with disabilities, fostering a more inclusive and accessible world for all.

 ,
, 



{kind=link}
{kind=link}
{kind=link}