1. Introduction
People with disabilities experience substantially higher rates of social isolation, loneliness, and lack of social support than people without disabilities [
1,
2]. Living well with a disability requires a strong connection to services, people, and programs within the local community [
3,
4]. However, community engagement (i.e., full physical or social participation in the community to meet the needs of people with disabilities) is impeded by a lack of accessible and inclusive support. Barriers to ease of access can include transportation-related issues (e.g., inability to drive or lack of support for obtaining transportation, long distances to facilities or programs), the built environment (steep or unsafe walkways), or inadequate government policies [
5]. Barriers related to community inclusion can include a lack of knowledgeable staff, social acceptance, and supportive relationships and support systems [
6,
7].
In the United States (U.S.), the southeastern states comprise a geographic region with some of the highest rates of disability, chronic health conditions and diseases, and people living in rural areas with low access to healthcare [
8]. Given that the outbreak of COVID-19 has exacerbated rates of depression, loneliness, social isolation, and limited healthcare access among people with disabilities living within the southeastern region [
9], there is an urgent need to intervene. To comprehensively understand and address disparities among people with disabilities, public health professionals can operate under the lens of the Socio-Ecological Model. Although there is a wealth of research investigating barriers and facilitators related to living well with a disability at the individual level (face-to-face interviews with people with disabilities) [
10,
11,
12], there is significantly less knowledge of such factors at the community and societal levels (higher levels of the Socio-Ecological Model).
Understanding how communities can meet the needs of people with disabilities within the Southeast could reveal a critical pathway for supporting the most difficult-to-reach individuals across the country. In the U.S., there are states that are each comprised of many counties. Each county includes many communities, which represent a larger pool of neighborhoods. At the lowest level, residents are represented by the presidents of their neighborhoods. Neighborhood presidents are volunteer officers that are elected and re-elected on an annual basis by local neighborhood residents. Elections occur through absentee mail-in or election day ballot votes, and candidates must then be approved by a higher level of government, the City Council, before election results are finalized and candidates assume their role as presidents. The role of neighborhood presidents is to represent the voices, needs, and concerns of their residents, as well as to seek assistance or aid to address residents needs using available resources. Specific roles vary depending on the size and resources of the neighborhood. Neighborhood presidents are potentially a gateway for both understanding and addressing the needs of people with disabilities at the community and societal levels.
This study involved qualitatively interviewing neighborhood presidents to identify community barriers and facilitators related to accessibility and inclusion that are experienced by residents with disabilities. The second purpose was to identify a substantive theory that could be used as a model for understanding and determining how to improve accessibility and inclusion for people with disabilities.
2. Materials and Methods
This study utilized a qualitative grounded theory design, based on Charmaz’s constructivist grounded theory framework [
13]. The philosophical assumptions for this study were based on a critical realism ontology [
14] and interpretivism epistemology [
15]. Full details on the qualitative procedures can be found elsewhere [
16].
2.1. Participants
This study aimed to enroll 12 neighborhood presidents of low-resource communities within the state of Alabama. A low-resource community was identified as an Empowerment or Opportunity Zone (an area that is economically distressed as classified by the federal government), which were primarily rural or suburban communities. The study team determined that a sample size of 12 was acceptable, given there were 99 total neighborhoods in the state. The 12 neighborhoods were selected based upon their participation in community outreach efforts by the National Center for Health Physical Activity and Disability (NCHPAD), a Center funded by the Center for Disease Control and Prevention. The 12 participants were chosen based on convenience. The first 12 to respond to recruitment efforts were selected to be included in the study. This study was approved by the University Institutional Review Board and verbal consent was obtained from participants prior to participation.
2.2. Procedures
One-on-one semi-structured interviews were conducted via phone or in person, as preferred by each participant. The maximum interview duration was set to 1 h. The interview included 9 questions: (1) an icebreaker question asking presidents what they do for fun on their free time; (2) overall perceived needs of people with disabilities in their neighborhood; (3) thoughts on the definition of accessibility for people with disabilities; (4) barriers and facilitators of accessibility for people with disabilities within their neighborhood; (5) thoughts on the definition of inclusion; (6) barriers and facilitators related to inclusive environments and programs; (7) perceived adequacy of policies and laws related to accessibility and inclusion; (8) thoughts about serving as a neighborhood president and the reasons for deciding to become one; (9) any additional thoughts related to accessibility and inclusion for people with disabilities. These questions included several follow-up questions to probe for greater details in responses. The interviews were audio-recorded so that they could be transcribed for a coding analysis.
2.3. Analysis
The interviews were conducted by two interviewers (B.L. and P.T.M.Q.). One interviewer (B.L.) had several years of experience interviewing greater than 400 people with disabilities in research studies. The other was a doctoral student who was trained by the senior interviewer. The coding process followed 3 phases: (1) generation of initial codes, (2) organization of codes into focused codes, and (3) creation of conceptual categories (themes) that represent one or more focused codes [
13]. This process also included strategies to enhance qualitative rigor [
16], which consisted of keeping an audit trail of code development; the interviewers acted as critical friends (reflexively understand personal biases and carefully discuss viewpoints for rich code development); and the procedures adhered to all eight core elements of grounded theory methodology [
13].
3. Results
A total of 12 neighborhood presidents completed the study. Since there was a small number of neighborhood presidents and they were public figures, no identifying information (age, sex, etc.) was recorded in order to preserve their confidentiality. A total of five presidents represented opportunity zones. The average interview duration was 27 min.
3.1. Themes
The analysis resulted in four themes (listed in
Table 1): (1) community engagement is a process from accessibility to inclusion; (2) knowledge supports people’s needs and empowers systemic changes to policies and laws; (3) neighborhood resources beget further resources; and (4) change necessitates benevolent leadership.
3.1.1. Community Engagement Is a Process from Accessibility to Inclusion
Community engagement begins with accessibility and ends with inclusion. A neighborhood cannot be inclusive of people with disabilities without first ensuring that programs and services are adequately accessible. Access, specifically transportation, was the primary point of discussion by presidents. Transportation barriers were prevalent and multifaceted. Barriers included no usable and reliable transportation; no family support for transportation and physical assistance; and unsafe environments (e.g., non-maintained or unsafe sidewalks or criminal activity). Public transportation (e.g., buses), when available, was generally accessible for wheelchair users but was generally reported as unreliable or unusable because of high wait times or tardiness.
Regarding inclusion, most presidents did not identify inclusion as a critical issue. They either were not aware of inclusive programs or did not perceive inclusion to be at the forefront of their priorities when compared to accessibility. All presidents were aware of laws related to accessibility and spent considerably more time discussing accessibility than inclusion. Four presidents explicitly noted that inclusion could not be achieved without access. Two of these presidents had a vision for what inclusive programs could be in their neighborhood, and two others represented neighborhoods that had inclusive programs. One neighborhood with inclusive programs was small and could allocate other residents to assist with transportation. The other had a strong network of neighborhood friends that relied on each other for transportation. For these two neighborhoods, staff members with knowledge of how to work with people with disabilities were available and critical for successful engagement. Thus, access and inclusion were perceived as a tiered process, where access and a vision for inclusion (i.e., not simply applying laws to promote access) were needed prior to creating inclusive opportunities.
3.1.2. Change Necessitates Benevolent Leadership
All presidents reported that creating even the smallest changes to their neighborhood was a long and difficult process. Creating change required perseverance and patience by the president. Presidents were motivated by a passion to aid their residents and reported a feeling of reward by addressing even the smallest of needs. Presidents were often thrilled about having the opportunity to have their voices heard by staff from a university of one of the largest cities in the state, making them ideal gatekeepers for a bottom-up political approach in addressing community and societal policies and laws to support community engagement of people with disabilities.
3.1.3. Resources Beget More Resources
A common theme across neighborhoods was that wealthier neighborhoods were perceived to have their needs addressed before smaller or less resource-rich areas. Newly paved sidewalks and roads, accessible public transportation, and safety were common requests that were not as easily addressed in low-resource areas. Presidents noted that resources provided by wealthier areas to low-resource areas should be considered as an investment. Sharing transportation resources could assist people with disabilities in attending hospital or health-related visits or interacting with businesses. In doing so, the individual could live a healthier, more productive lifestyle, which in turn bolsters their residing neighborhood. For example, one neighborhood was receiving strong police support to enhance safety by reducing criminal activity and prostitution. The president noted that this support increased residents’ outdoor activities. In addition to outside resources stimulating the growth of the neighborhood, internal resources, when available, could be used in conjunction with these resources to accelerate efforts to provide more services to residents with disabilities. Closer, denser neighborhoods could create friendship networks to rely upon each other for trips to the grocery store, work, or hospital visits. These networks typically were built through neighborhood meetings under the neighborhood president.
3.1.4. Knowledge Supports Needs and Empowers Changes to Policies and Laws
Knowledge was identified as a core theme that included several focused codes. These themes either addressed the access and inclusion needs of people with disabilities or were instrumental in initiating changes to policies and laws that could support people’s needs. Overall, neighborhood presidents reported that there were resources and laws (e.g., American with Disabilities Act) that could be utilized to support access needs of people with disabilities. Accessible home-service transportation was available in most neighborhoods and could often be paid for by a resident’s health insurance. Knowledge of other people within a community who could drive or had transportation to a major city could be shared with other residents. Nevertheless, obtaining and allocating these resources depended on either the resident or president’s knowledge. In most cases, presidents who were aware of people with disabilities in their community had resources that they could provide to alleviate transportation issues for their residents. The most rural neighborhoods reported that accessible transportation was non-existent and noted a need for external funding or support from larger, resource-rich neighborhoods to address this issue.
While presidents largely reported that resources were available, much less was known of their residents’ needs with regard to accessibility. Only one neighborhood partnered with a nearby university for a systematic survey regarding accessibility for their residents with disabilities, while another president from a smaller neighborhood was planning a door-to-door survey. All other neighborhoods depended on hearing residents’ needs through neighborhood meetings or other means of word-of-mouth. Presidents acknowledged a strong need to hear the voices of their residents with disabilities. They encouraged residents and external support (e.g., university investigators or students) to assist in this process. They reported that obtaining knowledge of needs is the first step toward resolving accessibility issues. A needs assessment was crucial because it provided a foundation to raise concerns that could be voiced on the political ladder in collective neighborhood council meetings.
3.2. Substantive Theory
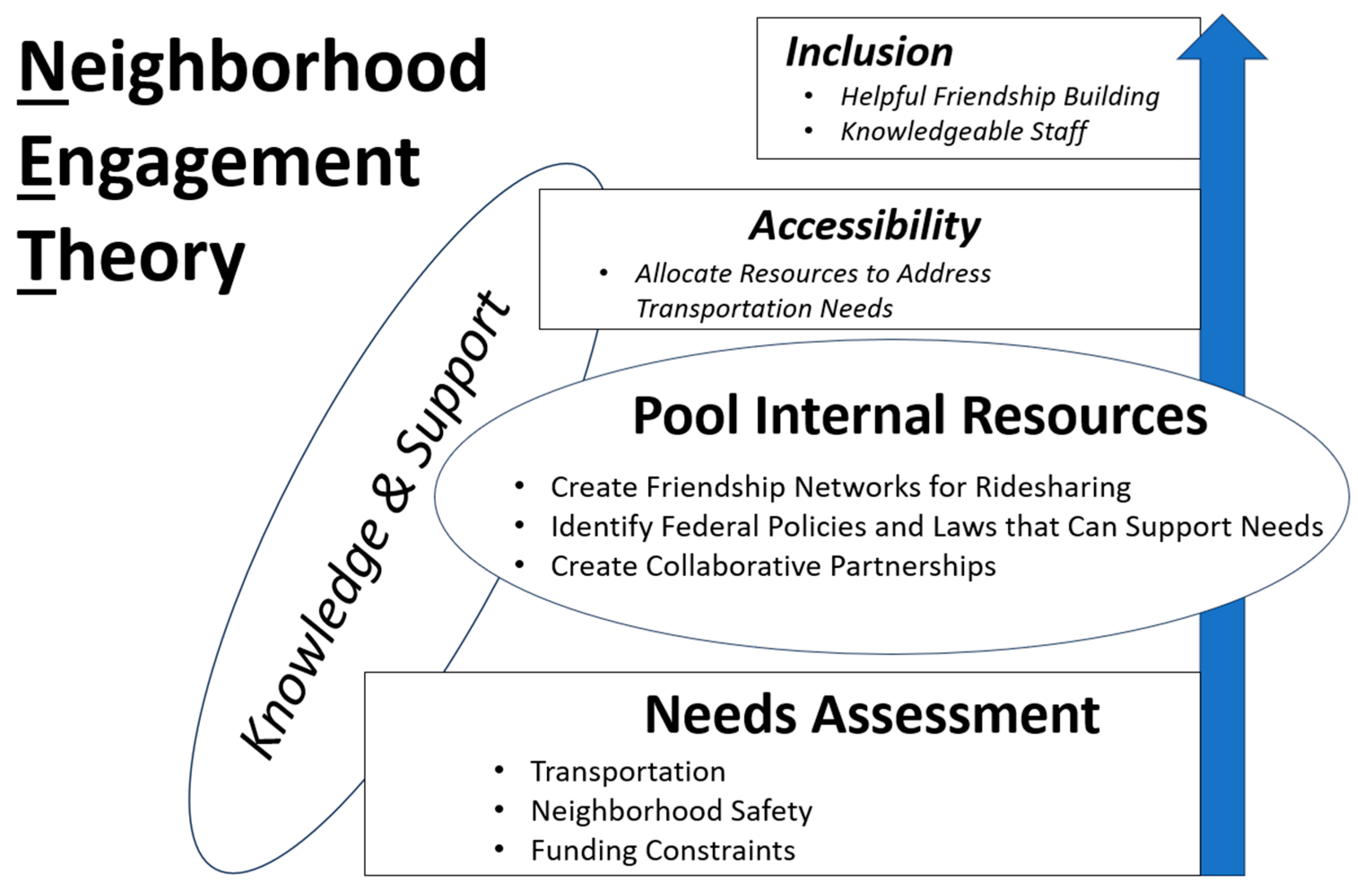
Figure 1 displays a theory, referred to as Neighborhood Engagement Theory (NET), that can be used by health professionals to support neighborhood presidents in bolstering the engagement of people with disabilities. The theory flows from a bottom-to-top approach and posits that health professionals must support presidents in conducting a needs assessment and pooling internal resources so that presidents can be sufficiently equipped to foster accessibility and inclusion for their residents with disabilities.
A needs assessment should identify residents’ barriers and facilitators to community engagement, with particular attention to transportation, neighborhood safety, and funding constraints. A systematic assessment, performed by an independent and professional third party, will strengthen presidents’ voices in advocating for the needs of people with disabilities in council meetings and will assist presidents in allocating resources to address barriers to accessibility.
After a needs assessment, health professionals should support presidents in creating support networks among residents for ridesharing, and seek partnerships with organizations, corporations, and academic institutions who can assist on various issues associated with making their community more accessible and inclusive. Seeking legal council is highly recommended, because there are several laws that mandate equal opportunities for people with disabilities or people who are marginalized. After conducting a needs assessment and identifying key issues associated with accessibility and inclusion, the first step will be to formulate a written plan to address the most pressing issues affecting residents with disabilities. This is where local colleges and universities can be of assistance in terms of helping presidents and their councils develop and execute a plan that meets the needs of their community. Presidents will need community support as they often handle multiple social issues simultaneously, have minimal staff to assist, and often work full-time in other positions, limiting the time they have available to devote to their role as a community president.
4. Discussion
This study investigated barriers and facilitators to community engagement as perceived by neighborhood presidents of low-resource and rural areas with residents being predominantly Black and living below the poverty level. Study findings identified several barriers at the community level that prevent successful access and inclusion. Previous investigations support these findings, particularly in emphasizing transportation as a key barrier to community participation [
11,
17]. While access to transportation among people with disabilities has been known to be a significant barrier across numerous studies, it became a predominant theme in this study, limiting our ability to get to a deeper level of understanding about the accessible nature of community events, services, and programs.
To advance the research on community access and inclusion for people with disabilities, we developed a theory, NET, to support neighborhood presidents in identifying and resolving barriers. Neighborhood presidents are the first representatives in the political hierarchy that can foster change at the community and societal level. From their voices, we identified working strategies that were taken from the perspectives of neighborhoods that were successful in engaging residents with disabilities. Researchers interested in disability access and inclusion in low-resource communities can benefit from this framework to better understand residents’ needs.
Empowering neighborhood presidents to tackle issues related to inclusion should not be ignored. Inclusive programs or the concept of inclusion was not well understood by presidents or addressed by neighborhoods. Two neighborhoods had inclusive programs and opportunities for their residents. In accordance with one of the resultant themes, “Knowledge supports needs and empowers changes”, health professionals can serve as a bridge for extracting knowledge of successful strategies that foster inclusion between neighborhoods. For example, a vision of inclusion seemed linked with actual inclusive opportunities or even hopes of creating these opportunities. Simply resolving issues with accessibility by applying local laws and resources will likely not be sufficient to resolve inclusion. Previous studies have demonstrated that empowering leaders within the community to foster inclusive opportunities for people with disabilities can be achieved through several relevant strategies, such as the creation of sustainable relationships and supportive networks, joint problem solving, welcoming disruption, and community-led objectives [
18,
19,
20,
21,
22]. These methods should align with the Social Model of Disability, where the focus or blame is not on the person with a disability that has an impairment that directly prevents them from participation, but instead places the blame on a society that socially isolates and oppresses [
23]. A benefit to this view is that it unites people with disabilities for political action [
23].
The needs assessment phase requires a thoughtful investigation from diverse perspectives to identify voices that are largely ignored. What prompted the development of this study was the lack of understanding on the intersectionality of race, poverty, and disability [
24]. The research literature reports that disability prevalence is higher among minority groups (e.g., African Americans and Hispanic Caucasians) [
25,
26], and this disparity is strongly linked to poverty [
26]. Disappointingly, this ‘silent majority’ can experience denial of disability rights, income inequality, and segregation of housing, education, and employment [
25], and may unintentionally be excluded from townhall meetings on discussions of key issues associated with a community’s social determinants of health (e.g., housing, healthcare, transportation).
The present paper presents one pathway for enacting change by connecting minority residents with disabilities to their neighborhood presidents. Considering difficulties with transportation, community meetings should provide remotely accessible options for participation (e.g., videoconference meetings) and attempt to reach people with disabilities at their home so that they can voice their opinion and needs. People with disabilities must be actively involved. Disability studies literature clearly emphasizes the concept of “nothing about us without us” and future research must include the voice of people with disabilities in each step of the research process [
27].
This study had limitations. Given its qualitative nature, the findings cannot be generalized to all neighborhood presidents. All people, with and without disabilities, are heterogenous and perceptions vary based upon environmental, personal, or cultural factors. In contrast, this study presented a theory that may have theoretical generalizability or transferability to other similar settings (low-resource or rural areas with marginalized communities) [
28]. Another limitation was the average length of interviews. Interview durations were planned to last up to an hour. The interview duration seemed to depend upon the size of the neighborhood and the president’s experiences and efforts to work with people with disabilities. Participants were selected to be included in the study on a first-come, first-served basis from our community outreach program. Those who responded first were selected to be included in the study, which could have inadvertently biased their responses. A convenience sample, as opposed to a purposive sample of people with specific characteristics, could also limit the generalizability of the findings to all neighborhood presidents within the state. Moreover, since participants were recruited from our community outreach program, this could have also led to bias in their responses.

 ,
, 

{kind=link}