
Family-Centred Care for Children with Biopsychosocial Support Needs: A Scoping Review



Abstract
:1. Introduction
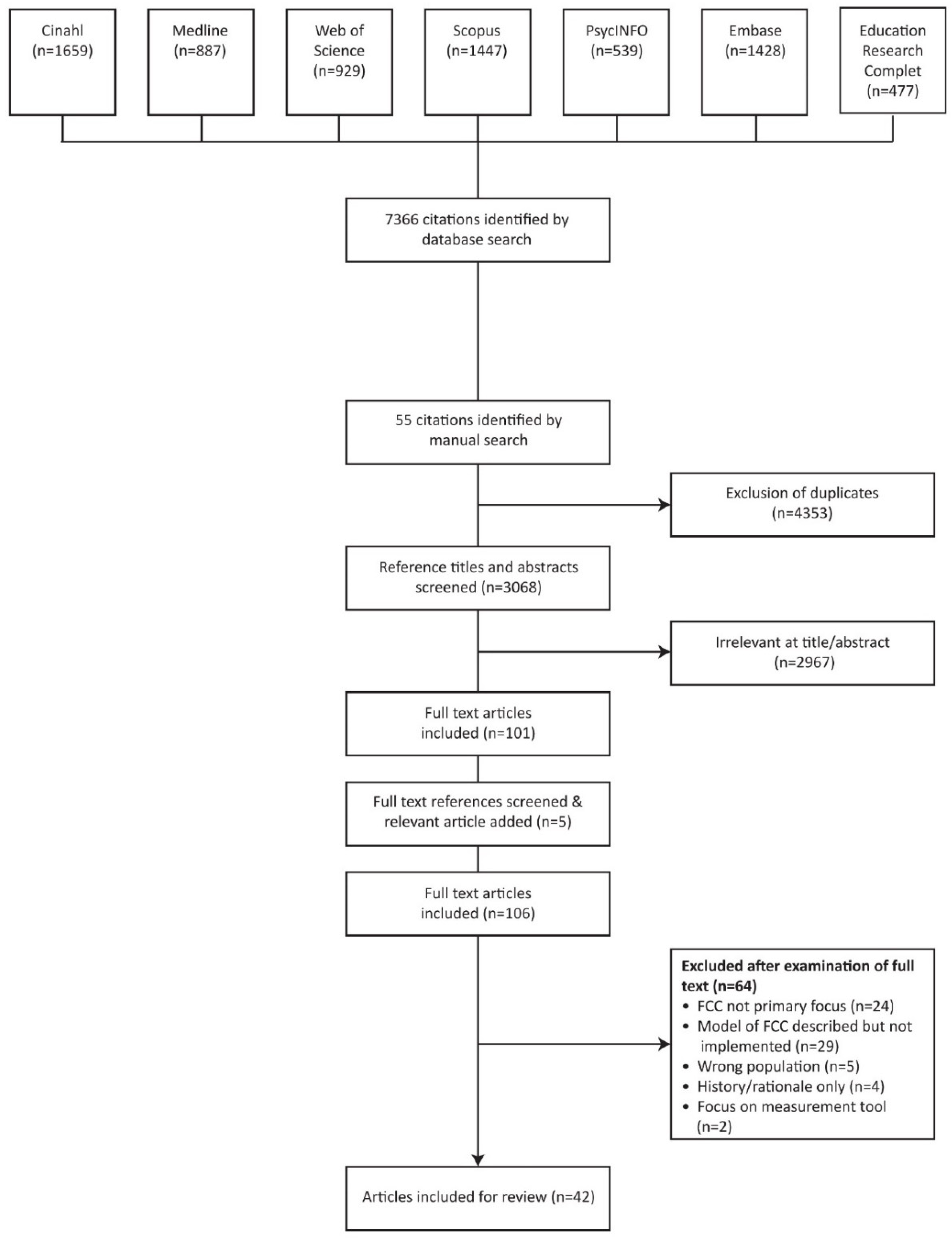
2. Materials and Methods
3. Results
3.1. Study Characteristics
3.2. Population Characteristics
3.3. Family-Centred Care Model Characteristics
3.4. Outcome Measures Used in Family-Centred Care Studies
3.5. Thematic Analysis: Key Features of Family-Centred Care Implementation Processes
3.5.1. Theme 1: Collaborative Decision Making and Goal Setting
3.5.2. Theme 2: Parental Supports
3.5.3. Theme 3: Intervention Content
3.5.4. Theme 4: Individualised Programming
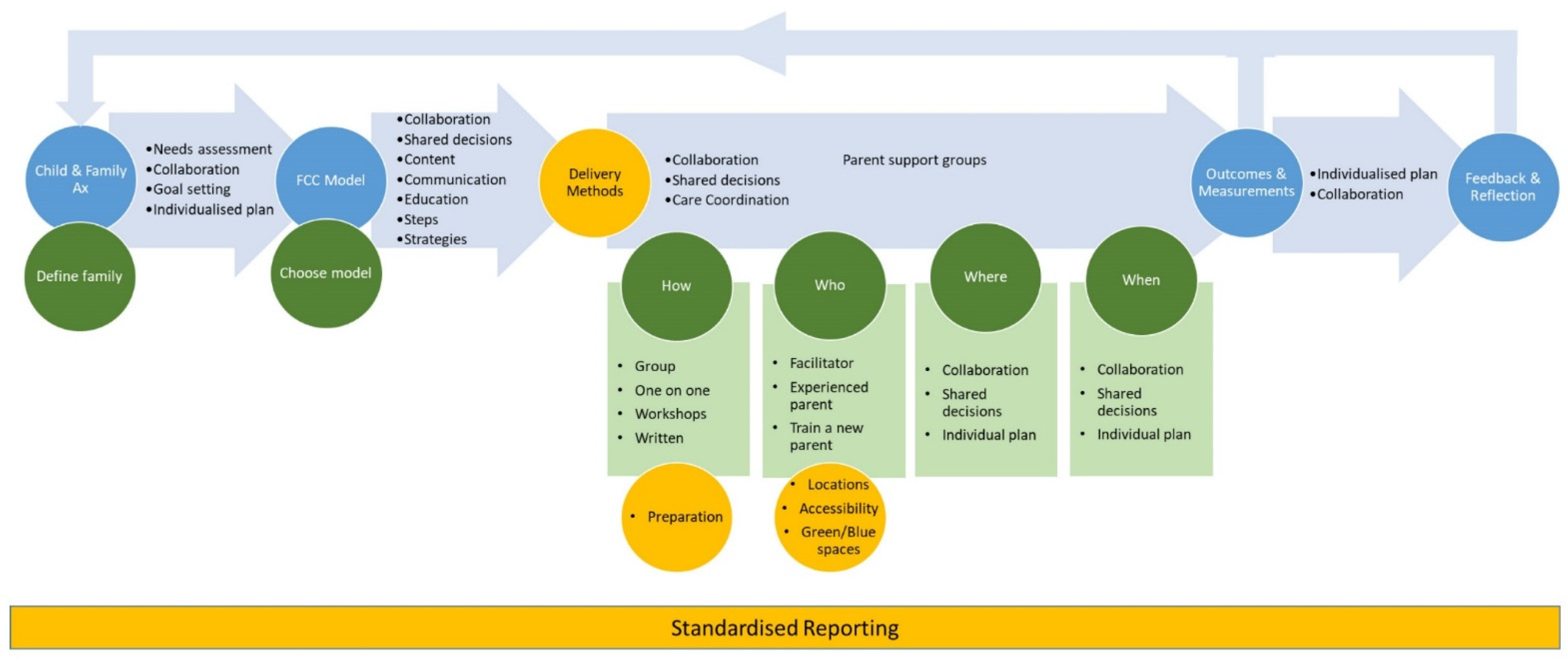
3.6. Framework for the Processes of Implementing Family-Centred Care
4. Discussion
4.1. Paucity of Demographic Reporting and Definitions of the Family Unit
4.2. Processes of Implementing Family-Centred Care Interventions
4.3. Outcome Measures Used in Family-Centred Care Studies
4.4. Implications for Practice
4.5. Strengths and Limitations
4.6. Recommendations
- Standardised questions to identify ‘family unit’,
- Standardised demographic questionnaires,
- Purpose of study and individual’s assessment mapped to the ICF model to ensure outcomes are meaningful to the family,
- Prepare the facilitator for the family-centred care intervention,
- Family to family support systems.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organisation. WHO Global Disability Action Plan 2014-2021. Better Health for All People with Disability; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- United Nations Children’s Fund. The State of the World’s Children 2013: Children with Disabilities; UNICEF: New York, NY, USA, 2013. [Google Scholar]
- Convention on the Rights of the Persons with Disabilities; Article 1. 2515 UNTS 3, Opened for Signature 30 March 2007, Entered into Force 3 May. 2008. Available online: https://treaties.un.org/doc/publication/UNTS/Volume%202515/v2515.pdf (accessed on 26 September 2021).
- World Health Organisation. International Classification of Functioning, Disability and Health (ICF); World Health Organization: Geneva, Switzerland, 2001; Available online: http://apps.who.int/iris/bitstream/handle/10665/42407/9241545429.pdf;jsessionid=796C3546180BDCB43D2978998785D506?sequence=1 (accessed on 26 September 2021).
- Spencer, N.; Raman, S.; Hare, B.; Tamburlini, G. Addressing inequities in child health and development: Towards social justice. BMJ Paediatr. 2019, 3, e000503. [Google Scholar] [CrossRef]
- Almasri, N.A.; An, M.; Palisano, R.J. Parents’ perception of receiving family-centered care for their children with physical disabilities: A meta-analysis. Phys. Occup. Ther. Pediatr. 2018, 38, 427–443. [Google Scholar] [CrossRef]
- Arakelyan, S.; Maciver, D.; Rush, R.; O’ Hare, A.; Forsyth, K. Family factors associated with participation of children with disabilities: A systematic review. Dev. Med. Child Neurol. 2019, 61, 514–522. [Google Scholar] [CrossRef]
- Arango, P. Family-centered care. Acad. Pediatr. 2011, 11, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Kuo, D.Z.; Houtrow, A.J.; Arango, P.; Kuhlthau, K.A.; Simmons, J.M.; Neff, J.M. Family-centered care: Current applications and future directions in pediatric health care. Matern. Child Health J. 2012, 16, 297–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jolley, J.; Shields, L. The evolution of family-centred care. J. Pediatr. 2009, 24, 164–170. [Google Scholar] [CrossRef] [Green Version]
- Carmen, S.; Teal, S.; Guzzetta, C.E. Development, testing, and national evaluation of a pediatric patient-family–centered care benchmarking survey. Holist. Nurs. Pract. 2008, 22, 61–74. [Google Scholar] [CrossRef] [PubMed]
- King, G.; Chiarello, L. Family-centered care for children with cerebral palsy: Conceptual and practical considerations to advance care and practice. J. Child Neurol. 2014, 29, 1046–1054. [Google Scholar] [CrossRef] [PubMed]
- Shields, L. What is “family-centred care”? EJPCH 2015, 3, 139–144. [Google Scholar] [CrossRef] [Green Version]
- Kuhlthau, K.A.; Bloom, S.; Van Cleave, J.; Knapp, A.A.; Romm, D.; Klatka, K.; Homer, C.J.; Newacheck, P.W.; Perrin, J.M. Evidence for family-centered care for children with special health care needs: A systematic review. Acad. Pediatr. 2011, 11, 136–143. [Google Scholar] [CrossRef]
- Perrin, J.M.; Romm, D.; Bloom, S.R.; Homer, C.J.; Kuhlthau, K.A.; Cooley, C.; Duncan, P.; Roberts, R.; Sloyer, P.; Wells, N.; et al. A family-centered, community-based system of services for children and youth with special health care needs. Arch. Pediatr. 2007, 161, 933–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokorelias, K.M.; Gignac, M.A.M.; Naglie, G.; Cameron, J.I. Towards a universal model of family centered care: A scoping review. BMC Health Serv. Res. 2019, 19, 564. [Google Scholar] [CrossRef] [PubMed]
- Uniacke, S.; Browne, T.K.; Shields, L. How should we understand family-centred care? J. Child Health Care. 2018, 22, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Litt, J.S.; McCormick, M.C. Care coordination, the family-centered medical home, and functional disability among children with special health care needs. Acad. Pediatr. 2015, 15, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. The ICF: An Overview. Available online: https://www.cdc.gov/nchs/data/icd/icfoverview_finalforwho10sept.pdf (accessed on 26 September 2021).
- CanChild. Research in Practice: ICF Resources. Available online: https://canchild.ca/en/research-in-practice/f-words-in-childhood-disability/icf-resources (accessed on 12 September 2021).
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; Johanna Briggs Institute: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 26 September 2021).
- Thomas, A.; Lubarsky, S.; Durning, S.J.; Young, M.E. Knowledge syntheses in medical education: Demystifying scoping reviews. Acad. Med. 2017, 92, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Colquhoun, H.L.; Levac, D.; O’Brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping reviews: Time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (prisma-scr): Checklist and explanation. Ann. Intern. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Wright, J. Removing Duplicates from an Endnote Library. Available online: https://blogs.lshtm.ac.uk/library/2018/12/07/removing-duplicates-from-an-endnote-library/ (accessed on 20 November 2020).
- New Zealand Government. Education and Training Act; Section 37; Parliamentary Counsel Office: Wellington, New Zealand, 2020. Available online: https://www.legislation.govt.nz/act/public/2020/0038/latest/LMS171368.html (accessed on 11 December 2020).
- United States Department of Education. Individuals with Disabilities Education Act. Available online: https://sites.ed.gov/idea/statuteregulations (accessed on 1 February 2021).
- Shields, L. Questioning family-centred care. J Clin Nurs. 2010, 19, 2629–2638. [Google Scholar] [CrossRef]
- Eccles, M.P.; Mittman, B.S. Welcome to Implementation Science. Implement. Sci. 2006, 1, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.R. Wright. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237. [Google Scholar] [CrossRef]
- World Health Organisation. How to Use the ICF, a Practical Manual for Using the International Classification of Functioning, Disability and Health (ICF). Available online: https://cdn.who.int/media/docs/default-source/classification/icf/drafticfpracticalmanual2.pdf?sfvrsn=8a214b01_4 (accessed on 3 June 2021).
- Wade, D.T.; Halligan, P.W. Do biomedical models of illness make for good healthcare systems? BMJ 2004, 329, 1398–1401. [Google Scholar] [CrossRef] [Green Version]
- An, M.; Palisano, R.J.; Dunst, C.J.; Chiarello, L.A.; Yi, C.-H.; Gracely, E.J. Strategies to promote family-professional collaboration: Two case reports. Disabil. Rehabil. 2016, 38, 1844–1858. [Google Scholar] [CrossRef]
- An, S.-J.L. Occupation-based family-centered therapy approach for young children with feeding problems in South Korea; A case study. Occup. Ther. Int. 2014, 21, 33–41. [Google Scholar] [CrossRef]
- Anderson, J.D.; Newby, R.; Kehm, R.; Barland, P.; Hearst, M.O. Taking steps together: A family and community-based obesity intervention for urban, multiethnic children. Health Educ. Behav. 2015, 42, 194–201. [Google Scholar] [CrossRef]
- Bailey, K.M.; Blair, K.S.C. Feasibility and potential efficacy of the family-centered Prevent-Teach-Reinforce model with families of children with developmental disorders. Res. Dev. Disabil. 2015, 47, 218–233. [Google Scholar] [CrossRef] [PubMed]
- Blauw-Hospers, C.H.; Dirks, T.; Hulshof, L.J.; Bos, A.F.; Hadders-Algra, M. Pediatric physical therapy in infancy: From nightmare to dream? a two-arm randomized trial. Phys. Ther. 2011, 91, 1323–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandao, M.B.; Frota, L.; Miranda, J.L.; Cavalcante Brasil, R.M.; Mancini, M.C. Family-centered early intervention program for Brazilian infants with congenital zika virus syndrome: A pilot study. Phys. Occup. Ther. Pediatr. 2019, 39, 642–654. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.L.; Irby, M.B.; Houle, T.T.; Skelton, J.A. Family-based obesity treatment in children with disabilities. Acad Pediatr. 2015, 15, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Bulkeley, K.; Bundy, A.; Roberts, J.; Einfeld, S. Family-centered management of sensory challenges of children with autism: Single-case experimental design. Am. J. Occup. Ther. 2016, 70, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Dirks, T.; Blauw-Hospers, C.H.; Hulshof, L.J.; Hadders-Algra, M. Differences between the family-centered “COPCA” program and traditional infant physical therapy based on neurodevelopmental treatment principles. Phys. Ther. 2011, 91, 1303–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falbe, J.; Cadiz, A.A.; Tantoco, N.K.; Thompson, H.R.; Madsen, K.A. Active and healthy families: A randomized controlled trial of a culturally tailored obesity intervention for Latino children. Acad. Pediatr. 2015, 15, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Fiallo-Scharer, R.; Palta, M.; Chewning, B.A.; Rajamanickam, V.; Wysocki, T.; Wetterneck, T.B.; Cox, E.D. Impact of family-centered tailoring of pediatric diabetes self-management resources. Pediatr Diab. 2019, 20, 1016–1024. [Google Scholar] [CrossRef] [Green Version]
- An, M.; Palisano, R.J.; Yi, C.-H.; Chiarello, L.A.; Dunst, C.J.; Gracely, E.J. Effects of a collaborative intervention process on parent–therapist interaction: A randomized controlled trial. Phys. Occup. Ther. Pediatr. 2019, 39, 259–275. [Google Scholar] [CrossRef] [PubMed]
- Fiallo-Scharer, R.; Palta, M.; Chewning, B.A.; Wysocki, T.; Wetterneck, T.B.; Cox, E.D. Design and baseline data from a PCORI-funded randomized controlled trial of family-centered tailoring of diabetes self-management resources. Contemp. Clin. 2017, 58, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Gardner, F.; Connell, A.; Trentacosta, C.J.; Shaw, D.S.; Dishion, T.J.; Wilson, M.N. Moderators of outcome in a brief family-centered intervention for preventing early problem behavior. J. Consult. Clin. Psychol. 2009, 77, 543–553. [Google Scholar] [CrossRef]
- George, M.W.; Trumpeter, N.N.; Wilson, D.K.; McDaniel, H.L.; Schiele, B.; Prinz, R.; Weist, M.D. Feasibility and preliminary outcomes from a pilot study of an integrated health-mental health promotion program in school mental health services. Fam. Community Health. 2014, 37, 19–30. [Google Scholar] [CrossRef] [Green Version]
- Hielkema, T.; Boxum, A.G.; Hamer, E.G.; La Bastide-Van Gemert, S.; Dirks, T.; Reinders-Messelink, H.A.; Maathuis, C.G.B.; Verheijden, J.; Geertzen, J.H.B.; Hadders-Algra, M. LEARN2MOVE 0-2 years, a randomized early intervention trial for infants at very high risk of cerebral palsy: Family outcome and infant’s functional outcome. Dis. Rehabil. 2020, 42, 3762–3770. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, R.L.; Hsieh, W.H.; Lee, W.C. Short-term family-centered workshop for children with developmental delays enhances family functioning and satisfaction: A prospective clinical trial. Medicine 2016, 95, e4200. [Google Scholar] [CrossRef]
- Hsieh, Y.H.; Liao, H.F.; Jeng, S.F.; Tseng, M.H.; Schiariti, V.; Tsai, M.Y.; Sun, S.C. Collaborative home-visit program for young children with motor delays in rural Taiwan: A pilot randomized controlled trial. Phys. Ther. 2020, 100, 979–994. [Google Scholar] [CrossRef] [PubMed]
- Huning, B.M.; Reimann, M.; Beerenberg, U.; Stein, A.; Schmidt, A.; Felderhoff-Muser, U. Establishment of a family-centred care programme with follow-up home visits: Implications for clinical care and economic characteristics. Klin. Padiatr. 2012, 224, 431–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, S.-T.; Hwang, Y.-S.; Chen, Y.-J.; Lee, P.; Chen, S.-J.; Lin, L.-Y. Home-based DIR/floortime™ intervention program for preschool children with autism spectrum disorders: Preliminary findings. Phys. Occup. Ther. Pediatr. 2014, 34, 356–367. [Google Scholar] [CrossRef]
- McAllister, J.W.; Keehn, R.M.; Rodgers, R.; Lock, T.M. care coordination using a shared plan of care approach: From model to practice. J. Pediatr. Nurs. 2018, 43, 88–96. [Google Scholar] [CrossRef]
- McConkey, R.; Cassin, M.T.; McNaughton, R. Promoting the social inclusion of children with ASD: A family-centred intervention. Brain Sci. 2020, 10, 318. [Google Scholar] [CrossRef]
- McKean, K.; Phillips, B.; Thompson, A. A family-centred model of care in paediatric speech-language pathology. Int. J. Speech Lang Pathol. 2012, 14, 235–246. [Google Scholar] [CrossRef] [PubMed]
- Miyahara, M.; Butson, R.; Cutfield, R.; Clarkson, J.E. A pilot study of family-focused tele-intervention for children with developmental coordination disorder: Development and lessons learned. Telemed J. E-Health 2009, 15, 707–712. [Google Scholar] [CrossRef]
- Nanclares-Nogues, V.; Lin, E.; Rolland, C.; Cupoli, J.M.; Msall, M.E. Enhancing multidisciplinary community supports for minority preschool children with autistic spectrum disorders: Promoting family centered and evidence based practices. Int. Pub. Health J. 2010, 2, 69–82. [Google Scholar]
- O’Donnell, L.A.; Weintraub, M.J.; Ellis, A.J.; Axelson, D.A.; Kowatch, R.A.; Schneck, C.D.; Miklowitz, D.J. A Randomized comparison of two psychosocial interventions on family functioning in adolescents with bipolar disorder. Fam. Process. 2020, 59, 376–389. [Google Scholar] [CrossRef]
- Pineda, J.; Dadds, M.R. Family intervention for adolescents with suicidal behavior: A randomized controlled trial and mediation analysis. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 851–862. [Google Scholar] [CrossRef]
- Poggioli, M.; Minichilli, F.; Bononi, T.; Meghi, P.; Andre, P.; Crecchi, A.; Rossi, B.; Carboncini, M.C.; Ottolini, A.; Bonfiglio, L. Effects of a home-based family-centred early habilitation program on neurobehavioural outcomes of very preterm born infants: A retrospective cohort study. Neural. Plast. 2016, 2016, 4323792. [Google Scholar] [CrossRef] [PubMed]
- Reid, N.; Dawe, S.; Harnett, P.; Shelton, D.; Hutton, L.; O’Callaghan, F. Feasibility study of a family-focused intervention to improve outcomes for children with FASD. Res. Dev. Disabil. 2017, 67, 34–46. [Google Scholar] [CrossRef] [Green Version]
- Samadi, S.A.; McConkey, R.; Kelly, G. Enhancing parental well-being and coping through a family-centred short course for Iranian parents of children with an autism spectrum disorder. Autism 2013, 17, 27–43. [Google Scholar] [CrossRef] [PubMed]
- Sgandurra, G.; Bartalena, L.; Cecchi, F.; Cioni, G.; Giampietri, M.; Greisen, G.; Herskind, A.; Inguaggiato, E.; Lorentzen, J.; Nielsen, J.B.; et al. A pilot study on early home-based intervention through an intelligent baby gym (CareToy) in preterm infants. Res. Dev. Disabil. 2016, 53, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Sgandurra, G.; Lorentzen, J.; Inguaggiato, E.; Bartalena, L.; Beani, E.; Cecchi, F.; Dario, P.; Giampietri, M.; Greisen, G.; Herskind, A.; et al. A randomized clinical trial in preterm infants on the effects of a home-based early intervention with the ‘CareToy System’. PLoS ONE 2017, 12, e0173521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storbeck, C.; Pittman, P. Early intervention in South Africa: Moving beyond hearing screening. Int. J. Audiol. 2008, 47, S36–S43. [Google Scholar] [CrossRef]
- Stumpf, E.; Breitenbach, E. Dolphin-assisted therapy with parental involvement for children with severe disabilities: Further evidence for a family-centered theory for effectiveness. Anthrozoos 2014, 27, 95–109. [Google Scholar] [CrossRef]
- Tompson, M.C.; Sugar, C.A.; Langer, D.A.; Asarnow, J.R. A randomized clinical trial comparing family-focused treatment and individual supportive therapy for depression in childhood and early adolescence. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 515–523. [Google Scholar] [CrossRef]
- Wade, S.L.; Michaud, L.; Brown, T.M. Putting the pieces together: Preliminary efficacy of a family problem-solving intervention for children with traumatic brain injury. J Head Trauma Rehabil. 2006, 21, 57–67. [Google Scholar] [CrossRef]
- Willis, C.; Nyquist, A.; Jahnsen, R.; Elliott, C.; Ullenhag, A. Enabling physical activity participation for children and youth with disabilities following a goal-directed, family-centred intervention. Res. Devel. Disabil. 2018, 77, 30–39. [Google Scholar] [CrossRef]
- Wong, S.Y.; Lai, A.C.; Martinson, I.; Wong, T.K.S. Effects of an education programme on family participation in the rehabilitation of children with developmental disability. JOID 2006, 10, 165–189. [Google Scholar] [CrossRef] [PubMed]
- Beharie, N.; Kalogerogiannis, K.; McKay, M.M.; Paulino, A.; Miranda, A.; Rivera-Rodriguez, A.; Torres, E.; Ortiz, A. The HOPE family project: A family-based group intervention to reduce the impact of homelessness on hiv/sti and drug risk behaviors. Soc. Work. Groups 2010, 34, 61–78. [Google Scholar] [CrossRef]
- Gopalan, G.; Chacko, A.; Franco, L.; Dean-assael, K.M.; Rotko, L.E.; Marcus, S.M.; Hoagwood, K.E.; McKay, M.M. Multiple family groups for children with disruptive behavior disorders: Child outcomes at 6-month follow-up. J. Child Fam. Stud. 2015, 24, 2721–2733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulkerson, J.A.; Friend, S.; Flattum, C.; Horning, M.; Draxten, M.; Neumark-Sztainer, D.; Gurvich, O.; Story, M.; Garwick, A.; Kubik, M.Y. Promoting healthful family meals to prevent obesity: HOME Plus, a randomized controlled trial. Int. J. Behav. 2015, 12, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pittson, H.; Wallace, L. Weight management programme for children. Prim. Health Care. 2010, 20, 16–21. Available online: https://www-proquest-com.ezproxy.otago.ac.nz/scholarly-journals/weight-management-programme-children/docview/757468711/se-2?accountid=14700 (accessed on 26 September 2021). [CrossRef]
- Feinberg, L.; Reinhard, S.C.; Houser, A.; Choula, R. Valuing the Invaluable: 2011 Update: The Growing Contributions and Costs of Family Caregiving; AARP Public Policy Institute: Washington, DC, USA, 2011. [Google Scholar]
- The National Alliance for Caregiving & AARP Public Policy Institute. Caregiving in the U.S 2015. Available online: https://www.aarp.org/content/dam/aarp/ppi/2015/caregiving-in-the-united-states-2015-report-revised.pdf (accessed on 26 September 2021).
- The National Alliance for Caregiving & AARP Public Policy Institute. Caregiving in the U.S. 2020. Available online: https://www.caregiving.org/caregiving-in-the-us-2020/ (accessed on 26 September 2021).
- Kracht, C.L.; Sisson, S.B. Sibling influence on children’s objectively measured physical activity: A meta-analysis and systematic review. BMJ SEM. 2018, 4, e000405. [Google Scholar] [CrossRef] [Green Version]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? a systematic review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef]
- O’Neil, M.E.; Palisano, R.J.; Westcott, S.L. Relationship of therapists’ attitudes, children’s motor ability, and parenting stress to mothers’ perceptions of therapists’ behaviors during early intervention. Phys. Ther. 2001, 81, 1412–1424. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.-W.K.; Barnard, A. Technology-dependent children and their families: A review. J. Adv. Nurs. 2004, 45, 36–46. [Google Scholar] [CrossRef] [Green Version]
- Dunst, C.J.; Trivette, C.M.; Hamby, D.W. Meta-analysis of family-centered helpgiving practices research. Ment. Retard. Dev. Disabil. Res. Rev. 2007, 13, 370–378. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search No. | Keywords (Not Mapped to Search Headings) |
|---|---|
| 1. | “family centered” OR “family centred” OR “family focused” OR “family focussed” OR “family-centered” OR “family-centred” OR “family-focused” OR “family-focussed” |
| 2. | Care |
| 3. | #1 AND #2 |
| 4. | Child* OR infant* OR adolescen* OR youth* OR young OR “young person” OR “young people” OR teen* OR juvenil* OR kid* OR baby OR babies OR preschool* OR toddler* OR pediatric OR paediatric* OR “school age*” OR kindergarten* |
| 5. | social OR mental OR “mental health” OR physical OR education* OR psycholog* OR intellectual |
| 6. | “special need*” OR “need*” OR disab* OR impair* |
| 7. | #5 AND #6 |
| 8. | disab* OR impair* |
| 9. | “developmental delay” OR “long term condition*” OR “health care need*” OR “healthcare need*” |
| 10. | #7 OR #8 OR #9 |
| 11. | #3 AND #4 AND #10 |
| Filters | Language: English dsDates: 2005–2020 |
| Inclusion Criteria | Definitions |
|---|---|
| Primary research | Studies directly collected data |
| Qualitative studies | Qualitative data collection methods (e.g., focus groups, individual interviews). dsQualitative data analysis methods (e.g., phenomenology, grounded theory, general inductive approach). |
| Mixed-method studies | Qualitative and quantitative methods and/or analysis methods. |
| Quantitative studies | Quantitative methodology including cross sectional, prospective and randomised controlled trials. |
| Search parameters | Only peer-reviewed research published in the English language from 2005 to 14 October 2020. |
| Implementation processes of family-centred care | The focus of the study includes the processes of implementation of a family-centred model of care and/or service delivery. |
| Children | Aged from birth up to 21 years of age, to include children that require additional learning support and are eligible under the Special Education Act 2020 in New Zealand [29] and the Individuals with Disabilities Education Act in the United States to attend special education and related services until the end the age of 21. [30] |
| Biopsychosocial needs | Persons effected by physical, social, environmental, psychological and/or emotional factors that hinder participation in society. |
| Exclusion Criteria | Definition |
| Peer-reviewed and non-peer-reviewed literature | Abstracts, proceedings, books, book chapters, commentaries, opinion pieces, reviews, protocols and thesis dissertations. |
| Indirect family-centred care interactions | Articles focusing on only interactions between or discussion regarding family members. |
| Family-centred care intervention not implemented | Articles that reviewed or discussed only the history, implications, rationale, ethics or theoretical understanding of family-centred care. For example, the study conclusions suggested the need for a model of family-centred care (adapted from [16]). dsArticles that focused on the assessment or the evaluation of a tool that measured the degree of family-centred-ness of a programme, intervention or setting. The focus of the study was not the implementation of a family-centred care model (adapted from [16]). |
| Insufficient family-centred care processes | Articles which do not describe who is involved in the decision making and/or goal-setting processes in the family-centred care model. |
| Terminology used in this study | Definition |
| Biopsychosocial needs | All biopsychosocial factors that hinder participation for children in society, including physical, social environmental, psychological and emotional factors. A broad definition of ‘disability’ to align with the biopsychosocial model of health, with the recognition that biopsychosocial needs which hinder participation are additional to the everyday needs of the child. |
| Family-centred care | Care for children and their families within services (such as health or education) that are planned around the whole family, not just for the individual child and in which all the family members were recognised as care recipients [31]. |
| Key attributes of family-centred care | (1) Family members are included in the delivery of the child’s treatment [9] or care, (2) Parents are co-decision makers in their child’s care [11], (3) There is family-professional collaboration [12]. |
| Implementation of family-centred care interventions | Implementation in this context refers to the different practical and theoretical elements comprised within each individual primary study that strive to make it family centred and how these processes were delivered and put into action. It is acknowledged that this differs from the common definition of ‘implementation’ science relating to the promotion of systematic uptake of research findings into routine practice to improve health services quality and effectiveness [32]. |
| Family-centred model of care original to the study | Model of care with family-centred characteristics created specifically for the intervention, not previously described in other literature. |
| Existing family-centred model of care | Model of family-centred care that had been previously defined and described in other literature. |
| Family-centred care model derived from theoretical backgrounds | Model of care that used a theoretical background to define the family-centred characteristics of the intervention. |
| Family-centred care adapted model | Model of family-centred care that used the framework of an existing family-centred model but was adapted to suit the population or environment of the new intervention. |
| Article | Study | Children | Primary Caregiver | Family Demographics | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref & Code | Year | Geography | Design | Aims | Ages | Gender | Ethnicity | BPS Need | Relation | Age (Years) | Ethnicity | Family Structure | Other Family |
| [36] dsA1 | 2016 | South Korea | Case report | Describe implementation | 10 & 8 years | M 50% | Physical disability, Leigh disease, CP | Mother | 33–44 | Nuclear | Siblings | ||
| [37] dsA2 | 2014 | South Korea | Case study | Effectiveness | 16 months | M 100% | Global dev delay. Proteus syndrome, infantile spasm | Mother | 31 | Nuclear | |||
| [38] dsA3 | 2015 | USA | Feasibility trial | Evaluate intervention | 5.4–12 years | M 52.5% | Obesity and low-income Latino families | 28.6–47 | Nuclear | Siblings | |||
| [39] dsA4 | 2015 | USA | multiple-baseline intervention | Describe implementation | 5–7 years | M 100% | Caucasian | ASD or language delay with sensory processing problems | Mother | Nuclear and Single parents | Siblings | ||
| [40] dsA5 | 2011 | Netherlands | Two-arm randomised trial | Describe implementation | 3–6 months CA | M 43.5% | Infants at high risk for dev disorders | ||||||
| [41] dsA6 | 2019 | Brazil | Pilot study | Effectiveness | 3–9 months | M 53% | Congenital Zika virus syndrome (CZS) | Mother | |||||
| [42] dsA7 | 2015 | USA | Retrospective analysis | Effectiveness | 8.4–15.2 years | M 42% | White 45%, Black 32%, Hispanic/Latino 18%, Other 5% | BMI 95th percentile for age and gender. Obesity related medical comorbidities. | |||||
| [43] dsA8 | 2016 | Australia | Single case experimental design | Effectiveness | 48–57 months | M 67% | Atypical sensory processing, behaviour and sensory challenges, ASD, global dev delay | Mother | 33–38 | Vietnamese, Indian, Australian-Asian | |||
| [44] dsA9 | 2011 | Netherlands | Two-arm randomised trial | Evaluate intervention | 3–6 months CA | M 43.5% | High risk for developmental delay. Motor disorder | Majority Mother | 24.3–36.7 years | ||||
| [45] dsA10 | 2015 | USA | RCT | Effectiveness | 5–12 years | M 49% | Latino | Obesity and low-income Latino families | Majority Mothers | 30.2–43 | Latino | ||
| [46] dsA11 | 2019 | USA | RCT | Effectiveness | 8–12, 13–16 years | M 51% | Non-Hispanic/White 84% | Type 1 diabetes | Majority Mothers | 32.4–51 | Mostly White, non-Hispanic | ||
| [47] dsA12 | 2019 | Korea | RCT | Effectiveness | 4.6–11.7 years | M 67% | Cerebral palsy, Aarthrogryposis, Down syndrome, Prader-Willi syndrome, Moyamoya disease, Dev delay | Mother | 39.3–40.1 | ||||
| [48] dsA13 | 2017 | USA | Randomised parallel-group clinical trial | Effectiveness | 8–16 years | M 50.9% | White (Non-Hispanic) 83.6% | T1D diagnosis | Majority Mothers | mean 41.8 | Non-Hispanic 87.9% | ||
| [49] dsA14 | 2009 | USA | Retrospective analysis of RCT | Effectiveness | 2–2.11 years | M 51% | African American 28%, European American 50%, Biracial 13% | High risk for problem behaviour and from low-income families | Mother | African America 28%, Euro American 50%, biracial 13%, other 9%, Hispanic Amer. 13% | Nuclear and Single parents | ||
| [50] dsA15 | 2014 | USA | Feasibility trial—pilot study | Evaluate intervention | 11–15 years | M 60% | African American 50%, White 50% | Referred to mental health services | Majority Mothers | 32.39–52.01 | African American 50% | Nuclear and Single parents/caregivers | Grandmother |
| [51] dsA16 | 2019 | Netherlands | Retrospective analysis of RCT | Effectiveness | <9 months CA | M 60.5% | High risk of CP | ||||||
| [52] dsA17 | 2016 | Taiwan | Prospective study | Effectiveness | 18–35 months | M 75% | Developmental delay. | Majority Mothers | 30–54 | Nuclear | |||
| [53] dsA18 | 2020 | Taiwan | Pilot randomised control trial | Effectiveness | 6 to 33 months | M 79.2% | Chinese | Motor delays | Grandparents and Parents | mean 39.5 | Nuclear | ||
| [54] dsA19 | 2012 | Germany | Report | Evaluate intervention | From birth | Preterm infants < 32 weeks gestation (GA), multiple preterms and neonates with congenital malformations or severe illness. | |||||||
| [55] dsA20 | 2014 | Taiwan | Pilot study | Effectiveness | 45–69 months | M 100% | Autistic disorder | Mother | 29–44 | Nuclear | |||
| [56] dsA21 | 2018 | USA | Study of implementation | Describe implementation | 2–10 years | M 78% | Caucasian 79%, Black or African American 15%, Asian/Pacific Islander 4%, one race + 1%, not reported 1%, non-Hispanic 92%, Hispanic 8% | Autism spectrum disorder, dev delay, intellectual disability. | |||||
| [57] dsA22 | 2020 | Northern Ireland | Implementation of intervention | Effectiveness | 3.4–11.8 years | M 79.2% | ASD | Nuclear and Single parents | |||||
| [58] dsA23 | 2012 | Australia | RCT | Evaluate intervention | 39–58 months | M 70% | Speech sound and/or language disorder. | Parents | |||||
| [59] dsA24 | 2009 | New Zealand | Pilot study | Describe intervention | 7–10 years | M 91% | Developmental coordination disorder (DCD) | Majority Mothers | |||||
| [60] dsA25 | 2013 | USA | Trial | Describe intervention | 2–6.11 years | Caucasian & Latino | Autism | Nuclear and Single parents | |||||
| [61] dsA26 | 2020 | USA | RCT | Effectiveness | 12.0–18.1 years | M 50% | Non-White 16.7%, Hispanic 9.7% | Bipolar disease I or II | Nuclear | ||||
| [62] dsA27 | 2013 | Australia | Preliminary RCT | Effectiveness | 12–17 years | M 27% | Anglo-Saxon 57.5%, Culturally linguistically diverse/Non-English Speaking 35%, Aboriginal 7.5% | Suicidal adolescents. | Mother | 39.67–50.61 years | Anglo-Saxon 57.5%, Culturally linguistically diverse/Non English Speaking Background 35%, Aboriginal 7.5% | Nuclear and Single parents | Siblings |
| [63] dsA28 | 2016 | Italy | retrospective cohort study | Effectiveness | 3–24 months CA | M 56% | Preterm infant gestational age at birth of <32 weeks | ||||||
| [64] dsA29 | 2017 | Australia | mixed methods single-case experimental des. | Evaluate intervention | 9–12 years | M 0% | Foetal alcohol spectrum disorder (FASD) | Parents | 43–57 | Siblings | |||
| [65] dsA30 | 2013 | Iran | Pre-post, cross-over design | Evaluate intervention | 3–17 years | M 70.3% | ASD | <30–50+ years | Single parent | Siblings | |||
| [66] dsA31 | 2016 | Denmark and Italy | Pilot study | Evaluate intervention | 3–9 months CA | M 61.9% | Pre-term infants, born between 28 + 0 and 32 + 6 (weeks + days) of gestational age. | ||||||
| [67] dsA32 | 2017 | Italy and Denmark | Multicentre RCT | Effectiveness | 3–8.9 months CA | M 46.3% | Pre-term infants born between 28 + 0 and 32 + 6 (weeks + days) of gestational age | ||||||
| [68] dsA33 | 2008 | South Africa | Descriptive research design | Evaluate intervention | 3–43 months | M 53% | Black 66%, white 22%, mixed race %, Asian/Indian 3% | Hearing loss | |||||
| [69] dsA34 | 2014 | Germany | Controlled pretest-post-test design | Evaluate intervention | 5–10 years | M 54.8% | Down syndrome, physical or mental retardation, diverse disabilities | ||||||
| [70] dsA35 | 2017 | USA | Two-site RCT | Effectiveness | 7–14 years | M 44% | Caucasion 51%, Latino/hispanic: 15%, African American 26%, other 8% | MDD, DD, or depressive disorder-not otherwise specified | Nuclear | ||||
| [71] dsA36 | 2006 | USA | Trial | Describe intervention | 5–16 years | M 65.6% | African American 18.8%, European American 81.3% | Traumatic Brain Injury | Mother | ||||
| [72] dsA37 | 2018 | Norway | Mixed methods pre-test post-test cohort design | Evaluate intervention | 6–17 years | M 53.3% | Range of disabilities leading to activity limitations and participation restrictions | Nuclear and Single parents/caregiver | |||||
| [73] dsA38 | 2006 | China | Pre-test/post-test control group | Effectiveness | <2–11 years | M 75% | Chinese | Developmental disability | Majority Mothers | <20–45 | Siblings | ||
| [74] dsA39 | 2011 | USA | Comparison two models | Evaluate intervention | 11–14 years | Parents and their children who live in family shelters. | |||||||
| [75] dsA40 | 2015 | USA | Block comparison design | Effectiveness | 7–11 years | M 68% | Latino 53 %, Black/African American 30 % | Disruptive behaviour disorders | Single parent | Siblings | |||
| [76] dsA41 | 2015 | USA | Two-group RCT | Effectiveness | 8–12-years. | M 52% | White 71%, Black 16%, Other 13% | BMI percentile above the 50th percentile | mean ~41 years | 80% White, 13% black, 7% other | |||
| [77] dsA42 | 2010 | UK | Pilot study | Evaluate intervention | 8–13 years | BMI > 91st percentile | 33 and 44 | ||||||
| Family-Centred Care Model Characteristics | Location | Temporal Features of Family-Centred Care Interventions | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref and Code | Origin | Recruitment | Preparation | Implemented by | Delivery Method | Primary Location | Secondary Location | Weeks | Days | Sessions | Mins | Min Range | Frequency |
| [36] dsA1 | Existing model | Word of mouth/Flier | Physical therapist | Facilitator to family | Hospital | 6 | 40 | Weekly | |||||
| [37] dsA2 | Existing model | Word of mouth | Occupational therapist | Combo: Facilitator to family and home prog. | Hospital | Home | 20 | 60 | Twice weekly | ||||
| [38] dsA3 | Original to study | Health service | Bilingual program coordinator, dietitians, paediatricians, chef, nutrition and exercise experts, bilingual culturally aware volunteers | Group | Community Centre | 16 | 120 | Weekly | |||||
| [39] dsA4 | Adapted from existing | Health service | Child and Family Studies Associate Professor | Combo: facilitator to family and independent home programme | Home | ||||||||
| [40] dsA5 | Original to study | Health service | Train facilitator | Paediatric Physical Therapists | Facilitator to family | Home | 60 | Twice weekly | |||||
| [41] dsA6 | Existing model | Health service | Train facilitator | physical therapist, occupational therapist, speech therapist, psychologist | Combo: Group and Facilitator to family | Home | 16 | 60–90 | Weekly | ||||
| [42] dsA7 | Original to study | Health service | Paediatrician, family counsellor, dietician, physical therapist, exercise specialist | Facilitator to family | Hospital clinic | Home (instruction) | 52 | Biweekly | |||||
| [43] dsA8 | Original to study | Health service | Occupational Therapist | Combo: Facilitator to family and Written material | Home | 4 | 60 | Weekly | |||||
| [44] dsA9 | Original to study | Health service | Train facilitator | Paediatric physical therapists | Facilitator to family | Home | 60 | Twice weekly | |||||
| [45] dsA10 | Adapted from existing | Health service | Registered dietitian, Physician, Promotora, Medical assistant | Combo: Facilitator to family and Group | Health centres | 10 | 5 | 120 | Every other week | ||||
| [46] dsA11 | Original to study | Health service | Train facilitator | Registered nurses, Certified diabetes educators, Motivational Interviewing Network of Trainees, Paediatric health psychologists | Group | Diabetes clinic | 36 | 4 | 75 | ||||
| [47] dsA12 | Existing model | Ad/Flier | Train facilitator | Physical Therapists | Facilitator to family | Home or Clinic | 6 | 40 | Weekly | ||||
| [48] dsA13 | Original to study | Ad/flier | Train facilitator | Registered nurses, Certified diabetes educators, Motivational Interviewing Network of Trainees, Pediatric health psychologists | Group | Healthcare facilities | Home (assignments) | 36 | 4 | 75 | Every 3 months | ||
| [49] dsA14 | Adapted from original | Health service | Train facilitator | Psychology Research staff, parent consultant | Facilitator to family | Home | |||||||
| [50] dsA15 | Theoretical framework | Health service | Train facilitator/make resources | School Mental Health clinicians | Combo: Facilitator to family and Written material | School clinic | Home | 6 | |||||
| [51] dsA16 | Original to study | Health service | Train facilitator | Paediatric physiotherapists | Facilitator to family | Home | 52 | Aim weekly (actually 3× month) | |||||
| [52] dsA17 | Existing model | Health service | Childcare and educationteacher, speech therapist, occupational therapist | Group | 6 | 6 | 120 | Weekly | |||||
| [53] dsA18 | Theoretical + Model | Health service | Paediatric physical therapist, social workers, local paraprofessional, physical therapist | Facilitator to family | Home visits | 12 | 5 | 60–90 | Every other week, once in last month | ||||
| [54] dsA19 | Adapted from existing | Not described | Train facilitator | Specialised nurses, social education workers, case managers, psychologists, Neonatologists | Facilitator to family | Hospital/NICU | Home | 12 | Variable | ||||
| [55] dsA20 | Existing model | Health prof/flier | Train facilitator and parent/s | Occupational therapist | Combo: Facilitator to family and DVD Resources | Home | 10 | Variable | |||||
| [56] dsA21 | Theoretical + Model | Health service | Train facilitator | Clinicians (neurodevelopmental disabilities), Care coordinator (registered nurse, clinical social worker) | Facilitator to family | Neurodevelopmental outpatient clinical setting | Care coordination from respective workplaces | 36 | 90 | Variable | |||
| [57] dsA22 | Original to study | Health service | Train facilitator | Psychologist | Combo: Facilitator to family and resources | Home | Community | 52 | Fortnightly | ||||
| [58] dsA23 | Theoretical framework | Not described | Create resources | Speech Language Therapists | Combo: Group and Facilitator to family | Clinic | Home (consolidation) | 9 | 45 | Weekly | |||
| [59] dsA24 | Adapted from existing | Ad/flier | Paediatric physiotherapist | Combo: Written material and Independent home programme | Home | 12 | |||||||
| [60] dsA25 | Existing model | Health service | Train facilitator | Professional therapist (medical centre) | Combo: Facilitator to family and independent home programme | Medical centre | Home | 12 | 60 | Every 3 weeks | |||
| [61] dsA26 | Original to study | Health prof/flier | Train facilitator | unspecified clinicians | Facilitator to family | Outpatient clinics of University hospitals | 39 | 21 | 60 | Weekly, every other week, 3 monthly | |||
| [62] dsA27 | Adapted from existing | Health service | Train facilitator | Accredited RAP facilitators, psychologists, social workers, registered nurses | Combo: Facilitator to family and written material | Outpatient mental health setting or at the family’s discretion in the home | 4 | 120 | Weekly, every other week | ||||
| [63] dsA28 | Existing model | Health service | Nursing staff, child neurologist, neonatologist, paediatric physiotherapist | Combo: Facilitator to family and independent home programme | NICU | Home | |||||||
| [64] dsA29 | Existing model | Health service | Train facilitator | Registered Psychologist | Combo: Facilitator to family and written material | Home | 27 | 60–120 | weekly, fortnightly | ||||
| [65] dsA30 | Existing model | Health service | Psychologist | Combo: Group and DVD resources and written material and home programme | Private school/clinic for students with special needs | Home (training materials) | 7 | 60–90 | |||||
| [66] dsA31 | Existing model | Health service | Create resources | Child neurologists, paediatric physical therapists | Independent home programme | Home | 4 | 30–45 | Daily | ||||
| [67] dsA32 | Adapted from existing | Health service | Rehabilitative staff | Independent home programme | Home | 4 | 30–45 | Daily | |||||
| [68] dsA33 | Existing model | Health service | Train facilitator | Parent advisors and deaf mentors, professionals from infant’s individualised team | Combo: Facilitator to family and written material | Home | 52 | 60–90 | Weekly | ||||
| [69] dsA34 | Theoretical framework | Not described | Speech therapists, occupational therapists, Physiotherapists, Dolphin trainer | Facilitator to family | Dolphinarium | 10 | 30 | Daily | |||||
| [70] dsA35 | Original to study | Health prof/flier | Train facilitator | Psychology prof, social worker | Combo: Written material and independent home programme | Home (assignments) | 16 | 15 | 50–60 | weekly | |||
| [71] dsA36 | Theoretical framework | Health service | Train facilitator | Clinical psychology graduate student | Combo: Facilitator to family and written material | Clinic or Home | Home (assignments) | 24 | 7 | 75–100 | Every other week | ||
| [72] dsA37 | Adapted from existing | Health service | Create resources | Occupational therapist, Physiotherapists, adapted physical activity specialist | Group | Health/sports Centre | Local community | 19 | 120–300 | 6 days per week | |||
| [73] dsA38 | Original to study | Not described | Create resources | Unspecified researchers | Combo: Group and facilitator to family and written material | In house rehab centre. | 10 | 10 | 120 | Weekly | |||
| [74] dsA39 | Adapted from existing | Health prof/flier | Train facilitator | Community coordinators, social work university researchers, peer community educators, childcare providers | Combo: Group and written material | Six shelters in New York City | 8 | ||||||
| [75] dsA40 | Original to study | Health service | Train facilitator | Clinician, Family partners advocates (previous parents) | Combo: Group and Home programme | Outpatient mental health agencies. | Home (assignments) | 16 | 16 | 90–120 | Weekly | ||
| [76] A41 | Theoretical framework | Health prof/flier | Registered dietitians, public health nurse | Combo: Group and written material | Recreation community centres | Home (tasks) | 40 | 10 | Monthly | ||||
| [77] dsA42 | Theoretical framework | Health service | Create resources | Steering group: programme developer, obesity service manager, paediatric, dietician, school nurse, health intelligence manager, GP, schoolteacher, child psychologist, and representatives from the child/adolescent mental health service and local council leisure services | Combo: Written material and group | Local further education college | 12 | 120 | Weekly | ||||
| Article Ref and Code | Outcome Measures | |||||||
|---|---|---|---|---|---|---|---|---|
| [36] A1 | Interviews | Canadian Occupational Performance Measure (COPM) | Response Class Matrix | |||||
| [37] A2 | Interviews | |||||||
| [38] A3 | Survey | Child weight | Child BMI | |||||
| [39] A4 | Individualised Behaviour Rating Scale Tool (IBRST) | |||||||
| [40] A5 | Neurological examination | Alberta Infant Motor Scale | The Paediatric Evaluation of Disability | |||||
| [41] A6 | Canadian Occupational Performance Measure (COPM) | Bayley Scales of Infant and Toddler Development | Affordances in the Home Environment for Motor Development-Infant Scale | Measure of Processes of Care (MPOC) | ||||
| [42] A7 | Child BMI | Child BMI z-score | ||||||
| [43] A8 | Mothers’ perceptions of the children’s behaviour = visual analogue scale (VAS) | |||||||
| [44] A9 | Time spent in different positions | Measures of family involvement. | ||||||
| [45] A10 | Child BMI changes | Child BMI z-score | Child blood pressure | Child fasting lipids | Child blood glucose—haemoglobin A1c | Child insulin | Child homeostasis model assessment-estimated insulin resistance | Parent weight |
| [46] A11 | QOL for children and their parents | Glycaemic control A1c data | ||||||
| [47] A12 | Family Empowerment Scale (FES) | Canadian Occupational Performance Measure (COPM) | ||||||
| [48] A13 | Diabetes-specific PedsQL | PedsQL Family Impact Module | PRISM barrier scores | Surveys | Percentage of patients meeting A1c target | |||
| [49] A14 | Eyberg Child Behaviour Inventor (ECBI) | Maternal depression: Centre for Epidemiological Studies on Depression Scale (CES-D) | Marital Adjustment Test | Cumulative risk index | ||||
| [50] A15 | Measurement of psychosocial variables | BMI | Standardised BMI | |||||
| [51] A16 | Family Empowerment Scale (FES) | Nijmeegse Ouderlijke Stress Index questionnaire, short version (NOSI-K) | Utrechtse Coping List | Vineland Adaptive Behaviour Scales (VABS), Dutch version | Infant and Toddler Quality of Life Questionnaire (ITQOL) | CBS-list Quality of Life | Paediatric Evaluation of Disability Index (PEDI) | Gross Motor Function Classification System (GMFCS). Factor analysis |
| [52] A17 | Pediatric Quality of Life Inventory (PaedsQL) Family Impact Module | the PedsQL Healthcare Satisfaction Module | Hospital Anxiety and Depression Scale | World Health Organisation Quality of Life brief assessment | ||||
| [53] A18 | Paediatric Evaluation of Disability Inventory Chinese Version (PEDI) | Peabody Developmental Motor Scale, 2nd edition | Disability-Adapted Infant–Toddler version of Home Observation for Measurement | Knowledge of Infant Development Inventory | Parental Stress Index-Short Form | |||
| [54] A19 | Economic impact length of stay | Re-hospitalisation rate for patients in—and outborn | Number of stays longer than average | Gestational age at discharge | ||||
| [55] A20 | Parenting Stress Index-Short Form | Vineland Adaptive Behaviour Scales | Functional Emotional Assessment Scale | |||||
| [56] A21 | Family goals outlined in the SPoC, and progress against those documented goals | The National Survey of Children with Special Health Care Needs (CAHMI) | Shared Plan of Care, (Family Experience of Care Coordination measurement set) | Family Empowerment (Family Empowerment Scales—about my child and about my family) | Family worry (Centre for Medical Home Improvement | |||
| [57] A22 | Qualitative interviews | Questionnaires on perceived outcomes and project quality | Rating scales specific to study | |||||
| [58] A23 | “Getting to know your child” questionnaire with contextual Factors of the ICF-CY | The Measures of Processes of Care (MPOC) | Satisfaction survey (developed for the study) | Goal Attainment Scaling GAS | Diagnostic Evaluation of Articulation and Phonology (DEAP) | The Risk Assessment and Prediction Tool (RAPT) | ||
| [59] A24 | Movement Assessment Battery for Children | Developmental Coordination Disorder Questionnaire | ||||||
| [60] A25 | Psychoeducational Profile Revised (PEP-R) | Vineland Adaptive Behaviour Scale (VABS) | Parental sense of competence scale (PSCS) | |||||
| [61] A26 | The Family Adaptability and Cohesion Evaluation Scale (FACES-II) | The Conflict Behaviour Questionnaire (CBQ) | The Mania Rating Scale (MRS; Chambers, 1985) | Depression Rating Scale of the K-SADS-PL | ||||
| [62] A27 | Adolescent Suicide Questionnaire—Revised (ASQ-R) | Adolescent and parental reports on the Strengths and Difficulties Questionnaire (SDQ) | Health of the Nation Outcomes Scale for Children and Adolescents (HoNOSCA) | Family Assessment Device (FAD) (McMaster Model of Family Functioning) | ||||
| [63] A28 | Bayley Scales of Infant Development 2nd Edition | |||||||
| [64] A29 | Survey | Semi-structured interviews | The 86-item Behaviour Rating Inventory of Executive Function (BRIEF) | The NEPSY, Second Edition (NEPSY-II) | The 64-item Youth Outcome Questionnaire—Self Report (Y-OQ SR) | |||
| [65] A30 | Post-course interviews | General Health Questionnaire | Coping Styles Questionnaire (CSQ) | Family functioning | The Short Form of the Parenting Stress Index (PSI-SF) | |||
| [66] A31 | The Infant Motor Profile (IMP) | Alberta Infant Motor Scale | Teller Acuity Cards | |||||
| [67] A32 | Infant Motor Profile (IMP) | Alberta Infant Motor Scale (AIMS) | Teller Acuity Cards | |||||
| [68] A33 | Surveys | HI HOPES data sheets | SKI-HI language development scale | |||||
| [69] A34 | Questionnaires | |||||||
| [70] A35 | Children’s Depression Rating Scale-Revised (CDRS-R) | Parent- and child-rated 5-point scales of overall satisfaction | Child Depression Inventory (CDI) | Social Adjustment Scale for Children -Self-Report (SAS-SR) | Multidimensional Anxiety Scale for Children | Child Behaviour Checklist | ||
| [71] A36 | Two-part satisfaction survey | Child Behaviour Checklist | Brief Symptom Inventory | Conflict Behaviour Questionnaire | ||||
| [72] A37 | Short structured interview with parents | Canadian Occupational Performance Measure (COPM) | Goal Attainment Scaling (GAS) | |||||
| [73] A38 | Knowledge Questionnaire | Maternal Self-Rating Scale | Short Form of the Questionnaire of Resources and Stress (QRS–F) | Community Activity Questionnaire (CAQ) | Parent Experience Survey (PES) | Parent–Child Interaction Assessment System | ||
| [74] A39 | The Within Family support subscale | Family Assessment Measure | Parenting Skills Questionnaire | Family Stress Scale | Monitoring the Future survey | Child Depression Inventory (CDI) | Brief Symptom Inventory | Sexual behaviour structured interview pre- and early adolescents |
| [75] A40 | Parent-report measures IOWA Connors Rating Scale (IOWA CRS) | Impairment Rating Scale (IRS) | Social Skills Rating System: Social Skills Subscale (SSRSSSS) | |||||
| [76] A41 | Child BMI z-score | Pubertal Development Scale | ||||||
| [77] A42 | Amended version of the Self-Perception Profile for Children (SPPC) | BMI | Physical activity survey | Family behaviours questionnaire developed by the programme | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrington, L.; Hale, L.; Freeman, C.; Qureshi, A.; Perry, M. Family-Centred Care for Children with Biopsychosocial Support Needs: A Scoping Review. Disabilities 2021, 1, 301-330. https://doi.org/10.3390/disabilities1040022
Carrington L, Hale L, Freeman C, Qureshi A, Perry M. Family-Centred Care for Children with Biopsychosocial Support Needs: A Scoping Review. Disabilities. 2021; 1(4):301-330. https://doi.org/10.3390/disabilities1040022
Chicago/Turabian StyleCarrington, Lizz, Leigh Hale, Claire Freeman, Ayesha Qureshi, and Meredith Perry. 2021. "Family-Centred Care for Children with Biopsychosocial Support Needs: A Scoping Review" Disabilities 1, no. 4: 301-330. https://doi.org/10.3390/disabilities1040022