
The Kinematics and Biomechanics for Non-Contiguous Anterior Cervical Discectomy and Fusion, Cervical Disc Arthroplasty, and Hybrid Cervical Surgery: A Systematic Review
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Definitions
2.4. Article Selection Process
2.5. Data Extraction
2.6. Bias and Quality Assessment
2.7. Certainty Assessment
2.8. Statistical Analysis
3. Results
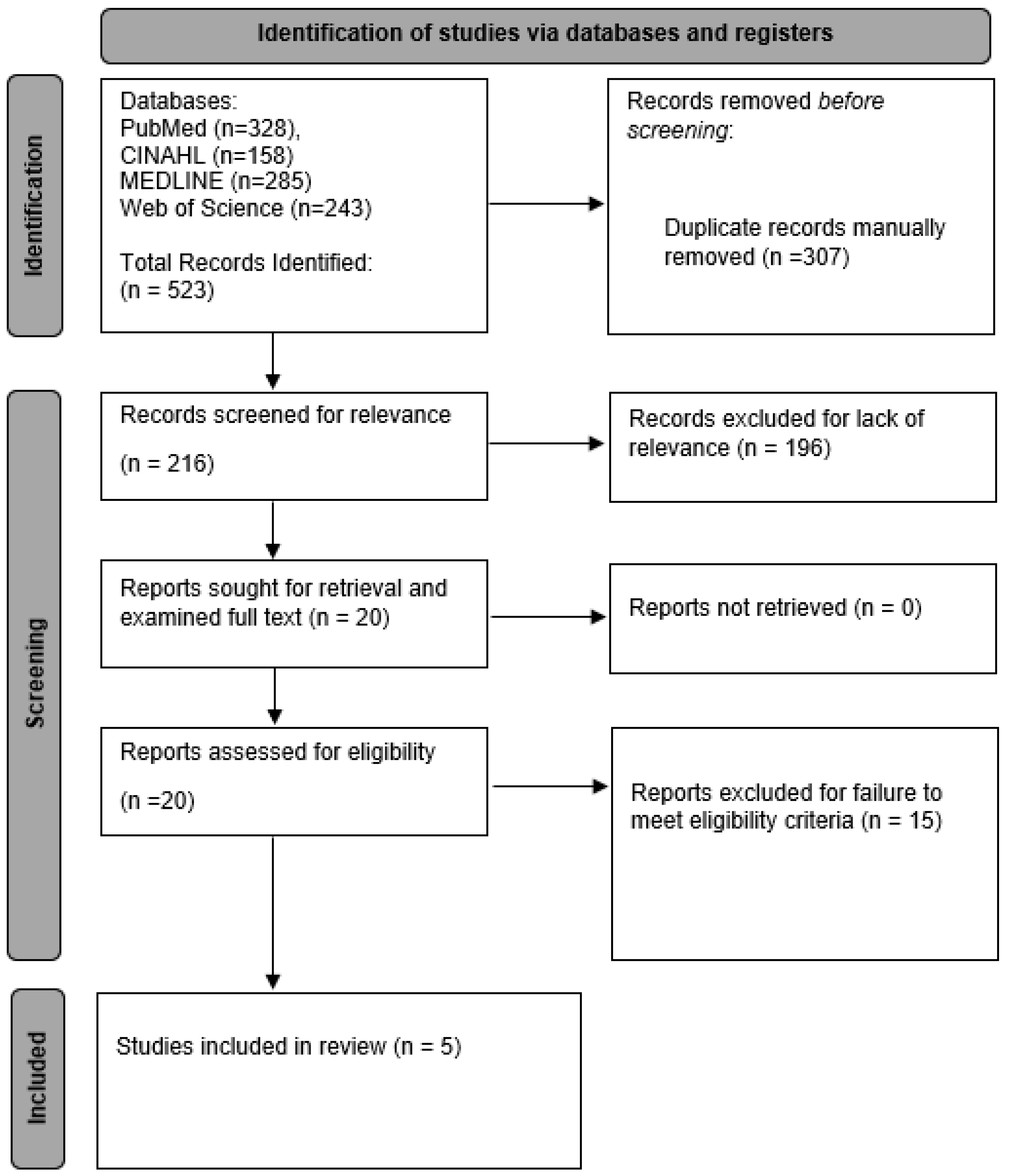
3.1. Study Selection and Characteristics
3.2. Methodology of Included Articles
3.3. Non-Contiguous Hybrid Cervical Surgery Motion
3.4. Non-Contiguous Hybrid Cervical Surgery Intervertebral Disc Pressure
3.5. Non-Contiguous Hybrid Cervical Surgery Facet Contact Force
3.6. Non-Contiguous Cervical Disc Arthroplasty Motion
3.7. Non-Contiguous Cervical Disc Arthroplasty Intervertebral Disc Pressure
3.8. Non-Contiguous Cervical Disc Arthroplasty Facet Contact Force
3.9. Non-Contiguous Anterior Cervical Discectomy and Fusion Motion
3.10. Non-Contiguous Anterior Cervical Discectomy and Fusion Intervertebral Disc Pressure
3.11. Non-Contiguous Anterior Cervical Discectomy and Fusion Facet Contact Force
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Safavi-Abbasi, S.; Reyes, P.M.; Abjornson, C.; Crawford, N.R. Feasibility and Biomechanics of Multilevel Arthroplasty and Combined Cervical Arthrodesis and Arthroplasty. Clin. Spine Surg. 2016, 29, E522–E531. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.D.; Coric, D.; Khachatryan, A.; Brady, B.L.; Lillehaugen, T.; McCormack, M.; Dolman, W.B.; Ditto, R. A real-world analysis of hybrid CDA and ACDF compared to multilevel ACDF. BMC Musculoskelet. Disord. 2023, 24, 191. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Meng, F.; Ding, Y.; Li, J.; Han, J.; Zhang, X.; Dong, W. Comprehensive Analysis of Hybrid Surgery and Anterior Cervical Discectomy and Fusion in Cervical Diseases: A Meta-Analysis. Medicine 2020, 99, e19055. [Google Scholar] [CrossRef]
- Wu, T.-K.; Wang, B.-Y.; Meng, Y.; Ding, C.; Yang, Y.; Lou, J.-G.; Liu, H. Multilevel cervical disc replacement versus multilevel anterior discectomy and fusion: A meta-analysis. Medicine 2017, 96, e6503. [Google Scholar] [CrossRef] [PubMed]
- Jia, Z.; Mo, Z.; Ding, F.; He, Q.; Fan, Y.; Ruan, D. Hybrid surgery for multilevel cervical degenerative disc diseases: A systematic review of biomechanical and clinical evidence. Eur. Spine J. 2014, 23, 1619–1632. [Google Scholar] [CrossRef]
- Brinjikji, W.; Luetmer, P.; Comstock, B.; Bresnahan, B.; Chen, L.; Deyo, R.; Halabi, S.; Turner, J.; Avins, A.; James, K.; et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. Am. J. Neuroradiol. 2015, 36, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Sun, S.; Zhang, T.; Kong, C.; Wang, W.; Lu, S. Biomechanical comparison of noncontiguous cervical disc arthroplasty and noncontiguous cervical discectomy and fusion in the treatment of noncontinuous cervical degenerative disc disease: A finite element analysis. J. Orthop. Surg. Res. 2020, 15, 36. [Google Scholar] [CrossRef]
- Sun, X.; Zhang, Q.; Cao, L.; Wang, J.; Huang, J.; Liu, Y.; Zhang, Y.; Song, Z.; Tang, W.; Chen, Y.; et al. Biomechanical effects of hybrid constructions in the treatment of noncontinuous cervical spondylopathy: A finite element analysis. J. Orthop. Surg. Res. 2023, 18, 57. [Google Scholar] [CrossRef]
- Wu, T.-K.; Meng, Y.; Liu, H.; Wang, B.-Y.; Hong, Y.; Rong, X.; Ding, C.; Chen, H. Biomechanical effects on the intermediate segment of noncontiguous hybrid surgery with cervical disc arthroplasty and anterior cervical discectomy and fusion: A finite element analysis. Spine J. 2019, 19, 1254–1263. [Google Scholar] [CrossRef]
- Wu, T.-K.; Meng, Y.; Wang, B.-Y.; Rong, X.; Hong, Y.; Ding, C.; Chen, H.; Liu, H. Biomechanics following skip-level cervical disc arthroplasty versus skip-level cervical discectomy and fusion: A finite element-based study. BMC Musculoskelet. Disord. 2019, 20, 49. [Google Scholar] [CrossRef]
- Finn, M.A.; Samuelson, M.M.; Bishop, F.; Bachus, K.N.; Brodke, D.S. Two-level noncontiguous versus three-level anterior cervical discectomy and fusion: A biomechanical comparison. Spine 2011, 36, 448–453. [Google Scholar] [CrossRef]
- Liu, B.; Zeng, Z.; Van Hoof, T.; Kalala, J.P.; Liu, Z.; Wu, B. Comparison of hybrid constructs with 2-level artificial disc replacement and 2-level anterior cervical discectomy and fusion for surgical reconstruction of the cervical spine: A kinematic study in whole cadavers. Med. Sci. Monit. 2015, 21, 1031–1037. [Google Scholar] [CrossRef]
- Lee, M.J.; Dumonski, M.; Phillips, F.M.; Voronov, L.I.; Renner, S.M.; Carandang, G.; Havey, R.M.; Patwardhan, A.G. Disc replacement adjacent to cervical fusion: A biomechanical comparison of hybrid construct versus two-level fusion. Spine 2011, 36, 1932–1939. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, B.W.; Hu, N.; Zorn, C.M.; McAfee, P.C. Biomechanical comparison of single- and two-level cervical arthroplasty versus arthrodesis: Effect on adjacent-level spinal kinematics. Spine J. 2010, 10, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Hollyer, M.A.; Gill, E.C.; Ayis, S.; Demetriades, A.K. The safety and efficacy of hybrid surgery for multilevel cervical degenerative disc disease versus anterior cervical discectomy and fusion or cervical disc arthroplasty: A systematic review and meta-analysis. Acta Neurochir. 2020, 162, 289–303. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, Y.; Jiang, W. A comparison of zero-profile anchored spacer (ROI-C) and plate fixation in 2-level noncontiguous anterior cervical discectomy and fusion- a retrospective study. BMC Musculoskelet. Disord. 2018, 19, 119. [Google Scholar] [CrossRef]
- Qizhi, S.; Lei, S.; Peijia, L.; Hanping, Z.; Hongwei, H.; Junsheng, C.; Jianmin, L. A Comparison of Zero-Profile Devices and Artificial Cervical Disks in Patients With 2 Noncontiguous Levels of Cervical Spondylosis. Clin. Spine Surg. 2016, 29, E61–E66. [Google Scholar] [CrossRef] [PubMed]
- Kan, L.; Kang, J.; Gao, R.; Chen, X.; Jia, L. Clinical and radiological results of two hybrid reconstructive techniques in noncontiguous 3-level cervical spondylosis. J. Neurosurg. Spine 2014, 21, 944–950. [Google Scholar] [CrossRef]
- Shi, S.; Zheng, S.; Li, X.-F.; Yang, L.-L.; Liu, Z.-D.; Yuan, W. Comparison of a Stand-Alone Anchored Spacer Versus Plate-Cage Construct in the Treatment of Two Noncontiguous Levels of Cervical Spondylosis: A Preliminary Investigation. World Neurosurg. 2016, 89, 285–292. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (Minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Bao, W.; Wang, Z.; Zhou, F.; Zou, J.; Jiang, W.; Yang, H.; Zhang, Z.; Zhu, X. Comparison of the clinical effects of zero-profile anchored spacer (ROI-C) and conventional cage-plate construct for the treatment of noncontiguous bilevel of cervical degenerative disc disease (CDDD): A minimum 2-year follow-up. Medicine 2018, 97, e9808. [Google Scholar] [CrossRef]
- Wang, H.-R.; Li, X.-L.; Dong, J.; Yuan, F.-L.; Zhou, J. Skip-level anterior cervical discectomy and fusion with self-locking stand-alone PEEK cages for the treatment of 2 noncontiguous levels of cervical spondylosis. J. Spinal Disord. Tech. 2013, 26, E286–E292. [Google Scholar] [CrossRef]
- Dong, L.; Xu, Z.; Chen, X.; Wang, D.; Li, D.; Liu, T.; Hao, D. The change of adjacent segment after cervical disc arthroplasty compared with anterior cervical discectomy and fusion: A meta-analysis of randomized controlled trials. Spine J. 2017, 17, 1549–1558. [Google Scholar] [CrossRef] [PubMed]
- Harada, G.K.; Tao, Y.; Louie, P.K.; Basques, B.A.; Galbusera, F.; Niemeyer, F.; Wilke, H.; Goldberg, E.; An, H.S.; Samartzis, D. Cervical spine MRI phenotypes and prediction of pain, disability and adjacent segment degeneration/disease after ACDF. J. Orthop. Res. 2021, 39, 657–670. [Google Scholar] [CrossRef]
- Carrier, C.S.; Bono, C.M.; Lebl, D.R. Evidence-based analysis of adjacent segment degeneration and disease after ACDF: A systematic review. Spine J. 2013, 13, 1370–1378. [Google Scholar] [CrossRef] [PubMed]
- Broida, S.E.; Murakami, K.; Abedi, A.; Meisel, H.-J.; Hsieh, P.; Wang, J.; Jain, A.; Buser, Z.; Yoon, S.T. Clinical risk factors associated with the development of adjacent segment disease in patients undergoing ACDF: A systematic review. Spine J. 2023, 23, 146–156. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, B.; Liu, H.; Wu, Y.; Zhu, Q. Cervical disc arthroplasty versus anterior cervical discectomy and fusion for incidence of symptomatic adjacent segment disease: A meta-analysis of prospective randomized controlled trials. Spine 2016, 41, 1493–1502. [Google Scholar] [CrossRef]


{kind=link}
| Author (Year) | Study Type | Total MINORS Score | Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Collection of Data | End Points Appropriate to Study Aim | Unbiased Assessment of Study End Point | Follow-Up Period Appropriate to Study Aim | Less Than 5% Lost to Follow Up | Prospective Calculation of the Study Size | Adequate Control Group | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analysis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sun et al. (2020) [7] | Comparative | 20 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 |
| Sun et al. (2023) [8] | Comparative | 20 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 |
| Wu, Meng, Liu et al. (2019) [9] | Comparative | 17 | 2 | 1 | 2 | 2 | 0 | 2 | 2 | 0 | 1 | 2 | 1 | 2 |
| Wu, Meng, Wang, et al. (2019) [10] | Comparative | 16 | 2 | 1 | 2 | 2 | 0 | 2 | 2 | 0 | 1 | 2 | 1 | 1 |
| Finn et al. (2011) [11] | Comparative | 20 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 |
| Author (Year) | Study Type | Method of Assessment | Model Demographics | Number of Models | Surgical Devices Utilized | Surgical Levels | Comparison Groups by Surgery Type |
|---|---|---|---|---|---|---|---|
| Sun et al. (2020) [7] | Comparative Prospective | FEM from human CT images | Male and female with mild cervical degenerative disease | 8 (4 male and 4 female) | NuVasive Helix ACP (NuVasive, Inc.; San Diego, CA, USA), CoRoent Contour (NuVasive, Inc.; San Diego, CA, USA), Prodisc-C (Synthes; West Chester, Switzerland) | C3–C4; C5–C6 | Two-level non-contiguous ACDF versus two-level non-contiguous CDA |
| Sun et al. (2023) [8] | Comparative Prospective | FEM from human CT images | Male and female with mild cervical degenerative disease | 12 (6 male and 6 female) | NuVasive Helix ACP (NuVasive, Inc.; San Diego, CA, USA), CoRoent Contour (NuVasive, Inc.; San Diego, CA, USA), Prodisc-C (Synthes; West Chester, Switzerland) | C3–C4; C3–C7 | Two-level non-contiguous CDA-ACDF variant of HCS versus two-level non-contiguous ACDF-CDA variant of HCS |
| Wu, Meng, Liu et al. (2019) [9] | Comparative Prospective | FEM from human CT images | Healthy male without cervical disease | 1 | Zero-P system (Synthes; West Chester, Switzerland), Prestige-LP artificial disc (Medtronic Sofamor Danek Inc; Memphis, TN, USA) | C3–C4; C3–C8 | Two-level non-contiguous CDA-ACDF variant of HCS versus two-level non-contiguous ACDF-CDA variant of HCS versus two-level non-contiguous ACDF |
| Wu, Meng, Wang, et al. (2019) [10] | Comparative Prospective | FEM from human CT images | Healthy male without cervical disease | 1 | Zero-P system (Synthes; West Chester, Switzerland), Prestige-LP artificial disc (Medtronic Sofamor Danek; Memphis, TN, USA) | C3–C4; C3–C9 | Two-level non-contiguous ACDF versus two-level non-contiguous CDA |
| Finn et al. (2011) [11] | Comparative Prospective | Cadaver | Fresh and frozen human cadaver | 7 | - | C4–C5; C6–C7 | Two-level non-contiguous ACDF versus three-level contiguous ACDF |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anastasio, A.T.; Baumann, A.N.; Fiorentino, A.; Sidloski, K.; Walley, K.C.; Muralidharan, A.; Conry, K.T.; Hoffmann, J.C. The Kinematics and Biomechanics for Non-Contiguous Anterior Cervical Discectomy and Fusion, Cervical Disc Arthroplasty, and Hybrid Cervical Surgery: A Systematic Review. Biomechanics 2023, 3, 443-456. https://doi.org/10.3390/biomechanics3040036
Anastasio AT, Baumann AN, Fiorentino A, Sidloski K, Walley KC, Muralidharan A, Conry KT, Hoffmann JC. The Kinematics and Biomechanics for Non-Contiguous Anterior Cervical Discectomy and Fusion, Cervical Disc Arthroplasty, and Hybrid Cervical Surgery: A Systematic Review. Biomechanics. 2023; 3(4):443-456. https://doi.org/10.3390/biomechanics3040036
Chicago/Turabian StyleAnastasio, Albert T., Anthony N. Baumann, Andrew Fiorentino, Katelyn Sidloski, Kempland C. Walley, Aditya Muralidharan, Keegan T. Conry, and Jacob C. Hoffmann. 2023. "The Kinematics and Biomechanics for Non-Contiguous Anterior Cervical Discectomy and Fusion, Cervical Disc Arthroplasty, and Hybrid Cervical Surgery: A Systematic Review" Biomechanics 3, no. 4: 443-456. https://doi.org/10.3390/biomechanics3040036