The Effect of Sitting Posture and Postural Activity on Low Back Muscle Stiffness


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Protocol
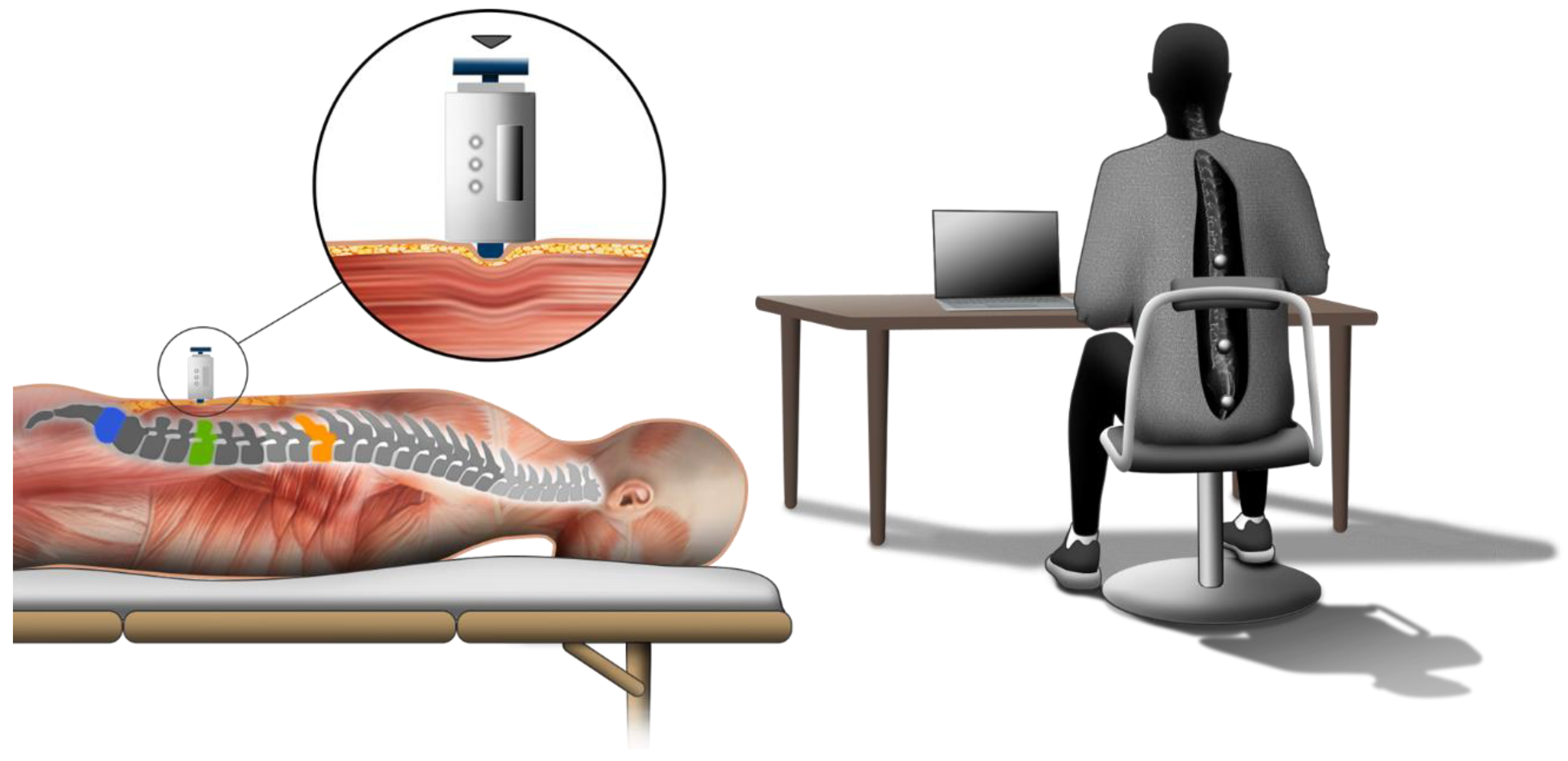
2.3. Stiffness Measurement
2.4. Acquisition and Analysis of Kinematic Data
2.5. Spinal Kinematics (Sitting Posture and Postural Activity)
2.6. Data Analysis and Statistics
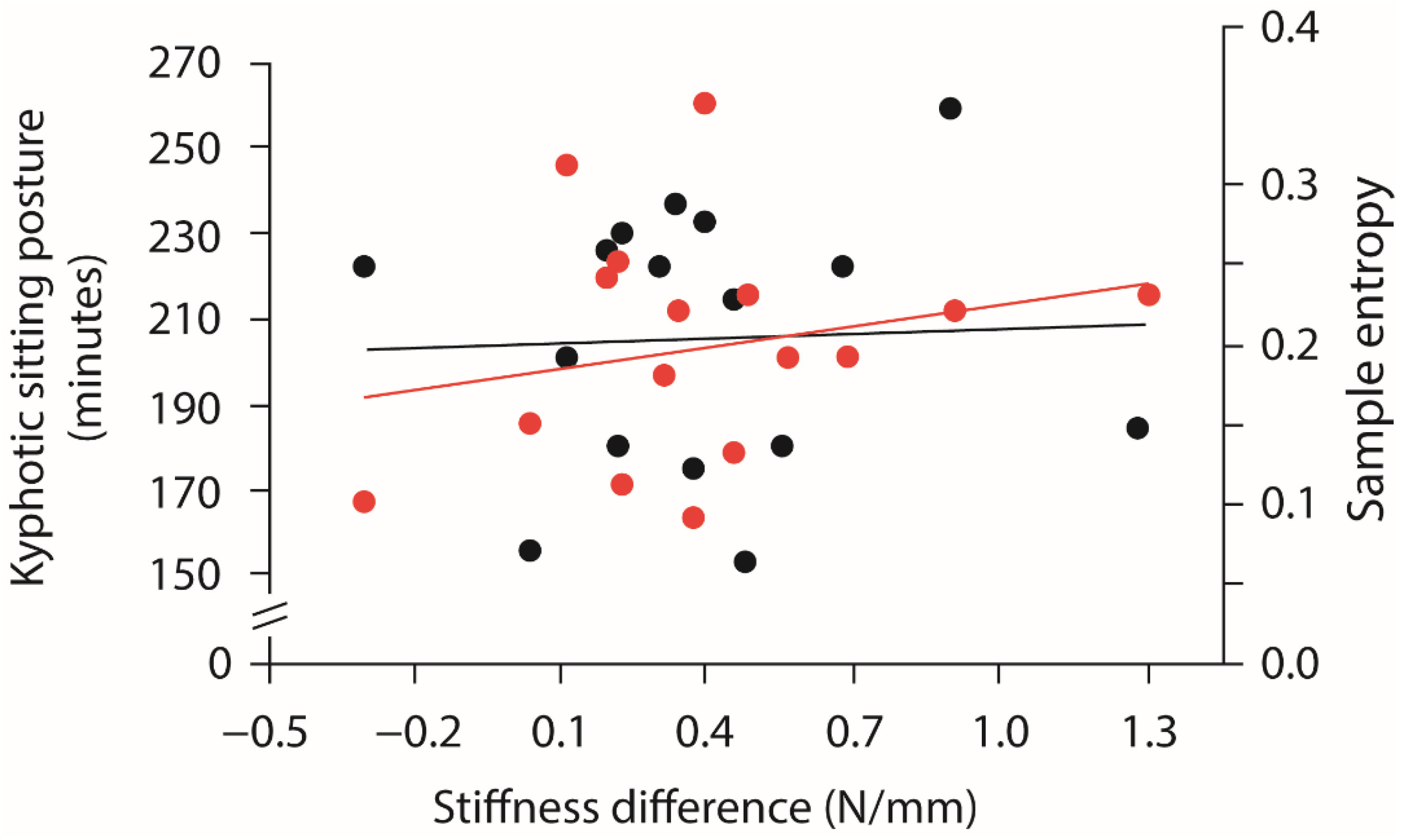
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lis, A.M.; Black, K.M.; Korn, H.; Nordin, M. Association between sitting and occupational LBP. Eur. Spine J. 2006, 16, 283–298. [Google Scholar] [CrossRef] [Green Version]
- Healy, G.N.; Matthews, C.; Dunstan, D.; Winkler, E.A.; Owen, N. Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 2003–06. Eur. Hear. J. 2011, 32, 590–597. [Google Scholar] [CrossRef]
- Clemes, S.; Patel, R.; Mahon, C.; Griffiths, P.L. Sitting time and step counts in office workers. Occup. Med. 2014, 64, 188–192. [Google Scholar] [CrossRef] [Green Version]
- Nolle, T. Mobile Berufe—Eine Untersuchung der Arbeitsbedingungen Mobile Berufe—Eine Untersuchung der Arbeitsbedingungen und der Ernährung im Hinblick auf Die Gesundheit. Ph.D. Dissertation, Technische Universität Dortmund, Dortmund, Germany, 2005. [Google Scholar]
- Schmücker, U.; Seifert, J.; Haasper, C.; Lob, G.; Matthes, G.; Stengel, D.; Ottersbach, C.; Frank, M.; Hinz, P.; Ekkernkamp, A.; et al. Unfälle, Erkrankungen und Verletzungen im Güterkraftverkehr. Unfallchirurg 2011, 115, 1022–1030. [Google Scholar] [CrossRef]
- Callaghan, J.P.; McGill, S.M. Low back joint loading and kinematics during standing and unsupported sitting. Ergonomics 2001, 44, 280–294. [Google Scholar] [CrossRef]
- van Dieën, J.H.; der Putten, E.P.W.-V.; Kingma, I.; de Looze, M.P. Low-level activity of the trunk extensor muscles causes electromyographic manifestations of fatigue in absence of decreased oxygenation. J. Electromyogr. Kinesiol. 2009, 19, 398–406. [Google Scholar] [CrossRef]
- Kett, A.R.; Sichting, F. Sedentary behaviour at work increases muscle stiffness of the back: Why roller massage has potential as an active break intervention. Appl. Ergon. 2020, 82, 102947. [Google Scholar] [CrossRef] [PubMed]
- Sammonds, G.M.; Fray, M.; Mansfield, N.J. Effect of long term driving on driver discomfort and its relationship with seat fidgets and movements (SFMs). Appl. Ergon. 2017, 58, 119–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, M.; McKinnon, C.; Viggiani, D.; Johnson, M.J.; Callaghan, J.P.; Albert, W.J. Biomechanical investigation of prolonged driving in an ergonomically designed truck seat prototype. Ergonomics 2017, 61, 367–380. [Google Scholar] [CrossRef] [PubMed]
- Waongenngarm, P.; van der Beek, A.J.; Akkarakittichoke, N.; Janwantanakul, P. Perceived musculoskeletal discomfort and its association with postural shifts during 4-h prolonged sitting in office workers. Appl. Ergon. 2020, 89, 103225. [Google Scholar] [CrossRef]
- Porter, J.M.; Gyi, D.E. The prevalence of musculoskeletal troubles among car drivers. Occup. Med. 2002, 52, 4–12. [Google Scholar] [CrossRef] [Green Version]
- Gupta, N.; Christiansen, C.S.; Hallman, D.M.; Korshøj, M.; Carneiro, I.G.; Holtermann, A. Is Objectively Measured Sitting Time Associated with Low Back Pain? A Cross-Sectional Investigation in the NOMAD study. PLoS ONE 2015, 10, e0121159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lunde, L.-K.; Koch, M.; Knardahl, S.; Veiersted, K.B. Associations of objectively measured sitting and standing with low-back pain intensity: A 6-month follow-up of construction and healthcare workers. Scand. J. Work. Environ. Health 2017, 43, 269–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waongenngarm, P.; Areerak, K.; Janwantanakul, P. The effects of breaks on low back pain, discomfort, and work productivity in office workers: A systematic review of randomized and non-randomized controlled trials. Appl. Ergon. 2018, 68, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Waongenngarm, P.; Rajaratnam, B.; Janwantanakul, P. Perceived body discomfort and trunk muscle activity in three prolonged sitting postures. J. Phys. Ther. Sci. 2015, 27, 2183–2187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claus, A.P.; Hides, J.; Moseley, L.; Hodges, P. Different Ways to Balance the Spine. Spine 2009, 34, E208–E214. [Google Scholar] [CrossRef] [Green Version]
- Hendershot, B.; Bazrgari, B.; Muslim, K.; Toosizadeh, N.; Nussbaum, M.; Madigan, M. Disturbance and recovery of trunk stiffness and reflexive muscle responses following prolonged trunk flexion: Influences of flexion angle and duration. Clin. Biomech. 2011, 26, 250–256. [Google Scholar] [CrossRef]
- Korakakis, V.; O’Sullivan, K.; O’Sullivan, P.B.; Evagelinou, V.; Sotiralis, Y.; Sideris, A.; Sakellariou, K.; Karanasios, S.; Giakas, G. Physiotherapist perceptions of optimal sitting and standing posture. Musculoskelet. Sci. Pract. 2019, 39, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.Y.; Grunseit, A.; Chey, T.; Stamatakis, E.; Brown, W.J.; Matthews, C.; Bauman, A.E.; van der Ploeg, H. Daily Sitting Time and All-Cause Mortality: A Meta-Analysis. PLoS ONE 2013, 8, e80000. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Role of Low Energy Expenditure and Sitting in Obesity, Metabolic Syndrome, Type 2 Diabetes, and Cardiovascular Disease. Diabetes 2007, 56, 2655–2667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janwantanakul, P.; Pensri, P.; Jiamjarasrangsri, V.; Sinsongsook, T. Prevalence of self-reported musculoskeletal symptoms among office workers. Occup. Med. 2008, 58, 436–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, M.; Shirai, Y.; Nakayama, Y.; Gembun, Y.; Kaneda, K. An Epidemiologic Study of Occupational Low Back Pain in Truck Drivers. J. Nippon. Med. Sch. 2000, 67, 186–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manchikanti, L.; Singh, V.; Datta, S.; Cohen, S.P.; Hirsch, J.A. Comprehensive review of epidemiology, scope, and impact of spinal pain. Pain Physician 2009, 12, 35–70. [Google Scholar] [CrossRef] [PubMed]
- Hartvigsen, J.; Hancock, M.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Mörl, F.; Bradl, I. Lumbar posture and muscular activity while sitting during office work. J. Electromyogr. Kinesiol. 2013, 23, 362–368. [Google Scholar] [CrossRef]
- Nairn, B.C.; Chisholm, S.R.; Drake, J.D. What is slumped sitting? A kinematic and electromyographical evaluation. Man. Ther. 2013, 18, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, J.P.; Dunk, N.M. Examination of the flexion relaxation phenomenon in erector spinae muscles during short duration slumped sitting. Clin. Biomech. 2002, 17, 353–360. [Google Scholar] [CrossRef]
- O’Sullivan, P.; Dankaerts, W.; Burnett, A.; Chen, D.; Booth, R.; Carlsen, C.; Schultz, A. Evaluation of the Flexion Relaxation Phenomenon of the Trunk Muscles in Sitting. Spine 2006, 31, 2009–2016. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Zuriaga, D.; Adams, M.; Dolan, P. Is Activation of the Back Muscles Impaired by Creep or Muscle Fatigue? Spine 2010, 35, 517–525. [Google Scholar] [CrossRef]
- Howarth, S.J.; Kingston, D.; Brown, S.; Graham, R.B. Viscoelastic creep induced by repetitive spine flexion and its relationship to dynamic spine stability. J. Electromyogr. Kinesiol. 2013, 23, 794–800. [Google Scholar] [CrossRef]
- Abboud, J.; Nougarou, F.; Descarreaux, M. Muscle Activity Adaptations to Spinal Tissue Creep in the Presence of Muscle Fatigue. PLoS ONE 2016, 11, e0149076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solomonow, M. Neuromuscular manifestations of viscoelastic tissue degradation following high and low risk repetitive lumbar flexion. J. Electromyogr. Kinesiol. 2012, 22, 155–175. [Google Scholar] [CrossRef] [PubMed]
- McGill, S.M.; Hughson, R.L.; Parks, K. Lumbar erector spinae oxygenation during prolonged contractions: Implications for prolonged work. Ergonomics 2000, 43, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Kell, R.T.; Bhambhani, Y. Relationship between erector spinae muscle oxygenation via in vivo near infrared spectroscopy and static endurance time in healthy males. Eur. J. Appl. Physiol. 2008, 102, 243–250. [Google Scholar] [CrossRef]
- Hill, D.K. Tension due to interaction between the sliding filaments in resting striated muscle the effect of stimulation. J. Physiol. 1968, 199, 637–684. [Google Scholar] [CrossRef]
- Proske, U.; Morgan, D.L. Do cross-bridges contribute to the tension during stretch of passive muscle? J. Muscle Res. Cell Motil. 1999, 20, 433–442. [Google Scholar] [CrossRef]
- Fenety, A.; Walker, J.M. Short-Term Effects of Workstation Exercises on Musculoskeletal Discomfort and Postural Changes in Seated Video Display Unit Workers. Phys. Ther. 2002, 82, 578–589. [Google Scholar] [CrossRef] [Green Version]
- Thorp, A.A.; Kingwell, B.A.; Owen, N.; Dunstan, D. Breaking up workplace sitting time with intermittent standing bouts improves fatigue and musculoskeletal discomfort in overweight/obese office workers. Occup. Environ. Med. 2014, 71, 765–771. [Google Scholar] [CrossRef]
- O’Sullivan, K.; O’Sullivan, L.; O’Sullivan, P.; Dankaerts, W. Investigating the effect of real-time spinal postural biofeedback on seated discomfort in people with non-specific chronic low back pain. Ergonomics 2013, 56, 1315–1325. [Google Scholar] [CrossRef]
- Van Dieën, J.H.; De Looze, M.P.; Hermans, V. Effects of dynamic office chairs on trunk kinematics, trunk extensor EMG and spinal shrinkage. Ergonomics 2001, 44, 739–750. [Google Scholar] [CrossRef]
- Wang, H.; Weiss, K.J.; Haggerty, M.C.; Heath, J.E. The effect of active sitting on trunk motion. J. Sport Health Sci. 2014, 3, 333–337. [Google Scholar] [CrossRef] [Green Version]
- Kuster, R.P.; Bauer, C.M.; Baumgartner, D. Is active sitting on a dynamic office chair controlled by the trunk muscles? PLoS ONE 2020, 15, e0242854. [Google Scholar] [CrossRef] [PubMed]
- Reenalda, J.; Van Geffen, P.; Nederhand, M.; Jannink, M.; Ijzerman, M.; Rietman, H. Analysis of healthy sitting behavior: Interface pressure distribution and subcutaneous tissue oxygenation. J. Rehabil. Res. Dev. 2009, 46, 577. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simons, G.D.; Mense, S. Understanding and measurement of muscle tone as related to clinical muscle pain. Pain 1998, 75, 1–17. [Google Scholar] [CrossRef]
- Wilke, J.; Vogt, L.; Pfarr, T.; Banzer, W. Reliability and validity of a semi-electronic tissue compliance meter to assess muscle stiffness. J. Back Musculoskelet. Rehabil. 2018, 31, 991–997. [Google Scholar] [CrossRef]
- Korakakis, V.; Sideris, V.; Giakas, G. Sitting bodily configuration: A study investigating the intra-tester reliability of positioning subjects into a predetermined sitting posture. Man. Ther. 2014, 19, 197–202. [Google Scholar] [CrossRef]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [Green Version]
- Søndergaard, K.H.; Olesen, C.G.; Søndergaard, E.K.; de Zee, M.; Madeleine, P. The variability and complexity of sitting postural control are associated with discomfort. J. Biomech. 2010, 43, 1997–2001. [Google Scholar] [CrossRef]
- Lubetzky, A.V.; Harel, D.; Lubetzky, E. On the effects of signal processing on sample entropy for postural control. PLoS ONE 2018, 13, e0193460. [Google Scholar] [CrossRef] [Green Version]
- Akkarakittichoke, N.; Janwantanakul, P. Seat Pressure Distribution Characteristics during 1 Hour Sitting in Office Workers With and Without Chronic Low Back Pain. Saf. Health Work 2017, 8, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Crenshaw, A.; Djupsjöbacka, M.; Svedmark, A. Oxygenation, EMG and position sense during computer mouse work. Impact of active versus passive pauses. Eur. J. Appl. Physiol. 2006, 97, 59–67. [Google Scholar] [CrossRef]
- Gregory, D.E.; Dunk, N.M.; Callaghan, J.P. Stability Ball Versus Office Chair: Comparison of Muscle Activation and Lumbar Spine Posture During Prolonged Sitting. Hum. Factors J. Hum. Factors Ergon. Soc. 2006, 48, 142–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kingma, I.; van Dieen, J. Static and dynamic postural loadings during computer work in females: Sitting on an office chair versus sitting on an exercise ball. Appl. Ergon. 2009, 40, 199–205. [Google Scholar] [CrossRef]
- Creze, M.; Timoh, K.N.; Gagey, O.; Rocher, L.; Bellin, M.-F.; Soubeyrand, M. Feasibility assessment of shear wave elastography to lumbar back muscles. Clin. Anat. 2017, 30, 774–780. [Google Scholar] [CrossRef]
- Masaki, M.; Aoyama, T.; Murakami, T.; Yanase, K.; Ji, X.; Tateuchi, H.; Ichihashi, N. Association of low back pain with muscle stiffness and muscle mass of the lumbar back muscles, and sagittal spinal alignment in young and middle-aged medical workers. Clin. Biomech. 2017, 49, 128–133. [Google Scholar] [CrossRef] [Green Version]
- Chan, S.-T.; Fung, P.-K.; Ng, N.-Y.; Ngan, T.-L.; Chong, M.-Y.; Tang, C.-N.; He, J.-F.; Zheng, Y.-P. Dynamic changes of elasticity, cross-sectional area, and fat infiltration of multifidus at different postures in men with chronic low back pain. Spine J. 2012, 12, 381–388. [Google Scholar] [CrossRef]
- Crommert, M.E.; Lacourpaille, L.; Heales, L.J.; Tucker, K.; Hug, F. Massage induces an immediate, albeit short-term, reduction in muscle stiffness. Scand. J. Med. Sci. Sports 2014, 25, e490–e496. [Google Scholar] [CrossRef] [PubMed]
- Van Deursen, L.L.; Patijn, J.; Durinck, J.R.; Brouwer, R.; Van Erven-Sommers, J.R.; Vortman, B.J. Sitting and low back pain: The positive effect of rotatory dynamic stimuli during prolonged sitting. Eur. Spine J. 1999, 8, 187–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sihawong, R.; Janwantanakul, P.; Jiamjarasrangsi, W. A prospective, cluster-randomized controlled trial of exercise program to prevent low back pain in office workers. Eur. Spine J. 2014, 23, 786–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kett, A.R.; Sichting, F.; Milani, T.L. The Effect of Sitting Posture and Postural Activity on Low Back Muscle Stiffness. Biomechanics 2021, 1, 214-224. https://doi.org/10.3390/biomechanics1020018
Kett AR, Sichting F, Milani TL. The Effect of Sitting Posture and Postural Activity on Low Back Muscle Stiffness. Biomechanics. 2021; 1(2):214-224. https://doi.org/10.3390/biomechanics1020018
Chicago/Turabian StyleKett, Alexander R., Freddy Sichting, and Thomas L. Milani. 2021. "The Effect of Sitting Posture and Postural Activity on Low Back Muscle Stiffness" Biomechanics 1, no. 2: 214-224. https://doi.org/10.3390/biomechanics1020018