
Blastocystis sp. Infection: Prevalence and Clinical Aspects among Patients Attending to the Laboratory of Parasitology–Mycology of Fann University Hospital, Dakar, Senegal
 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Socio-Demographic Characteristics of Study Participants
2.2. Clinical Characteristics of Study Patients
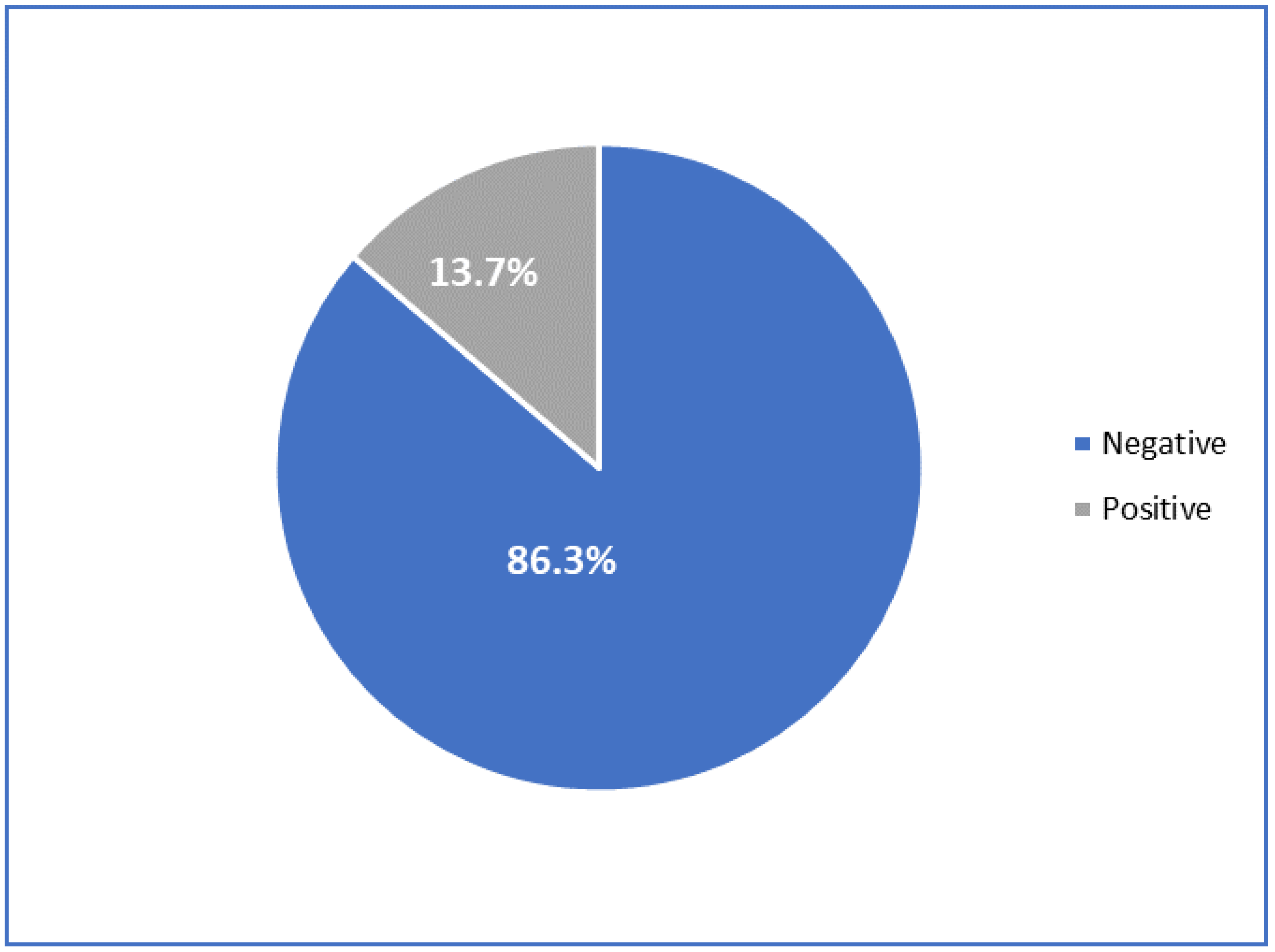
2.3. Prevalence of Blastocystis sp. Infection
2.4. Prevalence of Blastocystis sp. according to Socio-Demographic and Clinical Characteristics of Study Participants
3. Discussion
4. Materials and Methods
4.1. Study Design and Population
4.2. Data Collection
4.3. Parasitological Examination
4.4. Data Analysis
4.5. Ethics Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nithyamathi, K.; Chandramathi, S.; Kumar, S. Predominance of Blastocystis sp. infection among school children in Peninsular Malaysia. PLoS ONE 2016, 25, e0136709. [Google Scholar] [CrossRef]
- Osman, M.; El Safadi, D.; Cian, A.; Benamrouz, S.; Nourrisson, C.; Poirier, P.; Pereira, B.; Razakandrainibe, R.; Pinon, A.; Lambert, C.; et al. Prevalence and risk factors for intestinal protozoan infections with Cryptosporidium, Giardia, Blastocystis and Dientamoeba among schoolchildren in Tripoli, Lebanon. PLoS Negl. Trop. Dis. 2016, 10, e0004496. [Google Scholar]
- El Safadi, D.; Gaayeb, L.; Meloni, D.; Cian, A.; Poirier, P.; Wawrzyniak, I.; Delbac, F.; Dabboussi, F.; Delhaes, L.; Seck, M.; et al. Children of Senegal River Basin show the highest prevalence of Blastocystis sp. ever observed worldwide. BMC Infect. Dis. 2014, 25, 164. [Google Scholar]
- Stensvold, C.R.; Christiansen, D.B.; Olsen, K.E.; Nielsen, H.V. Blastocystis sp. subtype 4 is common in Danish Blastocystis- positive patients presenting with acute diarrhea. Am. J. Trop. Med. Hyg. 2011, 84, 883–885. [Google Scholar] [CrossRef] [PubMed]
- Abu-Madi, M.; Aly, M.; Behnke, J.M.; Clark, C.G.; Balkhy, H. The distribution of Blastocystis subtypes in isolates from Qatar. Parasit Vectors 2015, 17, 465. [Google Scholar] [CrossRef] [Green Version]
- Walker, C.L.; Aryee, M.J.; Boschi-Pinto, C.; Black, R.E. Estimating diarrhea mortality among young children in low and middle income countries. PLoS ONE 2012, 7, 29151. [Google Scholar]
- Keogh, M.B.; Castro-Alférez, M.; Polo-López, M.I.; Calderero, I.F.; Al-Eryani, Y.A.; Joseph-Titus, C.; Fernandez-Ibanez, P. Capability of 19-L polycarbonate plastic water cooler containers for efficient solar water disinfection (SODIS): Field case studies in India, Bahrain and Spain. Sol. Energy 2015, 116, 1–11. [Google Scholar] [CrossRef]
- Poirier, P.; Wawrzyniak, I.; Vivarès, C.P.; Delbac, F.; El Alaoui, H. New insights into Blastocystis spp.: A potential link with irritable bowel syndrome. PLoS Pathog. 2012, 8, 1002545. [Google Scholar] [CrossRef] [Green Version]
- Ocana-Losada, C.; Cuenca-Gomez, J.A.; Cabezas-Fernandez, M.T.; Vazquez-Villegas, J.; Soriano-Perez, M.J.; Cabeza-Barrera, I.; Salas-Coronas, J. Clinical and epidemiological characteristics of intestinal parasite infection by Blastocystis hominis. Rev. Clínica Española 2018, 218, 115–120. [Google Scholar] [CrossRef]
- Stensvold, C.R.; Lewis, H.C.; Hammerum, A.M.; Porsbo, L.J.; Nielsen, S.S.; Olsen, K.E.; Arendrup, M.C.; Nielsen, H.V.; Mølbak, K. Blastocystis: Unravelling potential risk factors and clinical significance of a common but neglected parasite. Epidemiol. Infect. 2009, 137, 1655–1663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaicharoen, R.; Sripochang, S.; Sermsart, B.; Pidetcha, P. Prevalence of Blastocystis hominis infection in asymptomatic individuals from Bangkok, Thailand. Southeast Asian J. Trop Med. Public Health 2005, 36, 17–20. [Google Scholar]
- Stensvold, C.R.; Suresh, G.K.; Tan, K.S.; Thompson, R.C.; Traub, R.J.; Viscogliosi, E.; Yoshikawa, H.; Clark, C.G. Terminology for Blastocystis subtypes-a consensus. Trends Parasitol. 2007, 23, 93–96. [Google Scholar] [CrossRef]
- Ghosh, K.; Ayyaril, M.; Nirmala, V. Acute GVHD involving the gastrointestinal tract and infestation with Blastocystis hominis in a patient with chronic myeloid leukaemia following allogeneic bone marrow transplantation. Bone Marrow Transplant. 1998, 22, 1115–1117. [Google Scholar] [CrossRef] [Green Version]
- Rao, K.; Sekar, U.; Iraivan, K.T.; Abraham, G.; Soundararajan, P. Blastocystis hominis-an emerging cause of diarrhoea in renal transplant recipients. J. Assoc. Physicians India 2003, 51, 719–721. [Google Scholar]
- Graczyk, T.K.; Shiff, C.K.; Tamang, L.; Munsaka, F.; Beitin, A.M.; Moss, W.J. The association of Blastocystis hominis and Endolimax nana with diarrheal stools in Zambian school-age children. Parasitol. Res. 2005, 98, 38–43. [Google Scholar] [CrossRef]
- M’bondoukwé, N.P.; Kendjo, E.; Mawili-Mboumba, D.P.; Koumba Lengongo, J.V.; Offouga Mbouoronde, C.; Nkoghe, D.; Touré, F.; Bouyou-Akotet, M.K. Prevalence of and risk factors for malaria, filariasis, and intestinal parasites as single infections or co-infections in different settlements of Gabon, Central Africa. Infect. Dis. Poverty 2018, 30, 6. [Google Scholar] [CrossRef] [Green Version]
- Sylla, K.; Tine, R.K.; Sow, D.; Lelo, S.; Ndiaye, L.A.; Faye, B.T.; Ndiaye, M.; Dieng, T.; Faye, B.; Gaye, O. Epidemiological profile of intestinal parasitic infection among preschool and school children living in a rural community in Senegal: A cross sectional survey. J. Bacteriol. Parasitol. 2018, 9, 2. [Google Scholar] [CrossRef]
- Sow, D.; Sylla, K.; Dieng, T.; Tine, R.C.; Ndiaye, M.; Faye, B.; Ndiaye, J.L.; Ndiaye, D.; Gaye, O.; Dieng, Y. Infection par Blastocystis hominis au Sénégal: Aspects épidémiologiques, cliniques et parasitologiques des cas diagnostiqués au CHNU de Fann à Dakar. Rev. CAMES Santé 2015, 3, 2. [Google Scholar]
- Trabelsi, S.; Ali, I.B.; Khaled, S. Clinical and epidemiological characteristics of blastocystis hominis. Tunis Med. 2010, 88, 190–192. [Google Scholar]
- Niang, T.M. Evalution d’un Nouveau Kit Pour la Detection de Parasites Intestinaux. Ph.D. Thesis, University Cheikh Anta Dakar, Dakar, Senegal, 2013; 140p. Available online: http://bibnum.ucad.sn/viewer.php?c=thm&d=THM%5f48541 (accessed on 19 October 2022).
- El Safadi, D.; Cian, A.; Nourrisson, C.; Pereira, B.; Morelle, C.; Bastien, P.; Bellanger, A.P.; Botterel, F.; Candolfi, E.; Desoubeaux, G.; et al. Prevalence, risk factors for infection and subtype distribution of the intestinal parasite Blastocystis sp. from a large-scale multi-center study in France. BMC Infect. Dis. 2016, 26, 451. [Google Scholar] [CrossRef] [Green Version]
- Becker, S.L.; Lohourignon, L.K.; Speich, B.; Rinaldi, L.; Knopp, S.; N’goran, E.K.; Cringoli, G.; Utzinger, J. Comparison of the Flotac-400 dual technique and the formalin-ether concentration technique for diagnosis of human intestinal protozoon infection. J. Clin. Microbiol. 2011, 49, 2183–2190. [Google Scholar] [CrossRef] [Green Version]
- Poulsen, C.S.; Efunshile, A.M.; Nelson, J.A.; Stensvold, C.R. Epidemiological Aspects of Blastocystis Colonization in Children in Ilero, Nigeria. Am. J. Trop. Med. Hyg. 2016, 95, 175–179. [Google Scholar] [CrossRef] [Green Version]
- Forsell, J.; Granlund, M.; Samuelsson, L.; Koskiniemi, S.; Edebro, H.; Evengard, B. High occurrence of Blastocystis sp. subtypes 1–3 and Giardia intestinalis assemblage B among patients in Zanzibar, Tanzania. Parasit. Vectors 2016, 9, 370. [Google Scholar] [CrossRef] [Green Version]
- Pinel, C.; Réjasse, C.; Picot, S.; Brenier-Pinchart, M.P.; Grillot, R.; Ambroise-Thomas, P. Blastocystis hominis: Epidemiological and clinical remarks from more than 3500 stool examinations. Ann. Biol. Clin. 1999, 57, 601–604. [Google Scholar]
- Poirier, P.; Wawrzyniak, I.; Albert, A.; El Alaoui, H.; Delbac, F.; Livrelli, V. Development and evaluation of a real-time PCR assay for detection and quantification of blastocystis parasites in human stool samples: Prospective study of patients with hematological malignancies. J. Clin. Microbiol. 2011, 49, 975–983. [Google Scholar] [CrossRef] [Green Version]
- Wong, K.H.; Ng, G.C.; Lin, R.T.; Yoshikawa, H.; Taylor, M.B.; Tan, K.S. Predominance of subtype 3 among Blastocystis isolates from a major hospital in Singapore. Parasitol. Res. 2008, 102, 663–670. [Google Scholar] [CrossRef]
- Abdulsalam, A.M.; Ithoi, I.; Al-Mekhlafi, H.M.; Khan, A.H.; Ahmed, A.; Surin, J.; Mak, J.W. Prevalence, predictors and clinical significance of Blastocystis sp. in Sebha, Libya. Parasit. Vectors 2013, 6, 86. [Google Scholar] [CrossRef] [Green Version]
- Dacal, E.; Saugar, J.M.; de Lucio, A.; Hernández-de-Mingo, M.; Robinson, E.; Köster, P.C.; Aznar-Ruiz-de-Alegría, M.L.; Espasa, M.; Ninda, A.; Gandasegui, J.; et al. Prevalence and molecular characterization of Strongyloides stercoralis, Giardia duodenalis, Cryptosporidium spp., and Blastocystis spp. isolates in school children in Cubal, Western Angola. Parasit. Vectors 2018, 11, 67. [Google Scholar] [CrossRef]
- Bart, A.; Wentink-Bonnema, E.M.; Gilis, H.; Verhaar, N.; Wassenaar, C.J.; van Vugt, M.; Goorhuis, A.; Van Gool, T. Diagnosis and subtype analysis of Blastocystis sp. in 442 patients in a hospital setting in the Netherlands. BMC Infect. Dis. 2013, 23, 389. [Google Scholar]
- Kain, K.C.; Noble, M.A.; Freeman, H.; Barteluk, R.L. Epidemiology and clinical features associated with Blastocystis hominis infection. Diagn. Microbiol. Infect. Dis. 1987, 8, 235–244. [Google Scholar] [CrossRef]
- Cirioni, O.; Giacometti, A.; Drenaggi, D.; Ancarani, F.; Scalise, G. Prevalence and clinical relevance of Blastocystis hominis in diverse patient cohorts. Eur. J. Epidemiol. 1999, 15, 389–393. [Google Scholar] [CrossRef]
- Sebaa, S. Contribution A L’etude De La Place Des Parasites Protozoaires Dans L’etiologie Des Enterites Chez La Population Humaine En Milieu Hospitalier Et Non Hospitalier Issues Des Zones Urbaines Et Rurales Via Les Sources Animales. Ph.D Thesis, University de Djelfa, Djelfa, Algeria, 2020; 231p. Available online: http://dspace.univ-djelfa.dz:8080/xmlui/handle/123456789/3403 (accessed on 19 October 2022).
- Al-Fellani, M.A.; Khan, A.H.; Al-Gazoui, R.M.; Zaid, M.K.; Al-Ferjani, M.A. Prevalence and Clinical Features of Blastocystis hominis Infection among Patients in Sebha, Libya. Sultan Qaboos Univ. Med. J. 2007, 7, 35–40. [Google Scholar]
- Beyhan, Y.E.; Yilmaz, H.; Cengiz, Z.T.; Ekici, A. Clinical significance and prevalence of Blastocystis hominis in Van, Turkey. Saudi Med. J. 2015, 36, 1118–1121. [Google Scholar] [CrossRef]
- Vassalos, C.M.; Spanakos, G.; Vassalou, E.; Papadopoulou, C.; Vakalis, N. Differences in clinical significance and morphologic features of Blastocystis sp subtype 3. Am. J. Clin. Pathol. 2010, 133, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Leder, K.; Hellard, M.E.; Sinclair, M.I.; Fairley, C.K.; Wolfe, R. No correlation between clinical symptoms and Blastocystis hominis in immunocompetent individuals. J. Gastroenterol. Hepatol. 2005, 20, 1390–1394. [Google Scholar] [CrossRef]
- Kumarasamy, V.; Roslani, A.C.; Rani, K.U.; Kumar Govind, S. Advantage of using colonic washouts for Blastocystis detection in colorectal cancer patients. Parasit. Vectors 2014, 3, 162. [Google Scholar] [CrossRef] [Green Version]
- Agholi, M.; Hatam, G.R.; Motazedian, M.H. HIV/AIDS-associated opportunistic protozoal diarrhea. AIDS Res. Hum. Retrovir. 2013, 29, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Rivero-Rodriguez, Z.; Hernandez, A.; Bracho, A.; Salazar, S.; Villalobos, R. Prevalence of intestinal microsporidia and other intestinal parasites in HIV positive patients from Maracaibo, Venezuela. Biomedica 2013, 33, 538–545. [Google Scholar]
- Taşova, Y.; Sahin, B.; Koltaş, S.; Paydaş, S. Clinical significance and frequency of Blastocystis hominis in Turkish patients with hematological malignancy. Acta Med. Okayama 2000, 54, 133–136. [Google Scholar]
- Suresh, K.; Smith, H. Comparison of methods for detecting Blastocystis hominis. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 23, 509–511. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Frequency (n) | Percentage (%) | 95% CI |
|---|---|---|---|
| Year | |||
| 2016 | 672 | 20.6 | 19.1–22.2 |
| 2017 | 801 | 24.5 | 22.8–26.3 |
| 2018 | 804 | 24.6 | 22.9–26.3 |
| 2019 | 616 | 18.8 | 17.4–20.4 |
| 2020 | 371 | 11.4 | 10.2–12.6 |
| Age group | |||
| <15 years | 1365 | 41.8 | 39.6–44.1 |
| [15–30] | 703 | 21.5 | 19.9–23.2 |
| [30–45] | 545 | 16.7 | 15.3–18.2 |
| ≥45 years | 651 | 20 | 18.4–21.5 |
| Gender | |||
| Female | 1600 | 49.1 | 46.6–51.5 |
| Male | 1664 | 50.9 | 48.5–53.5 |
| Season | |||
| Rainy | 2475 | 78.8 | 72.8–78.8 |
| Dry | 789 | 24.2 | 22.5–25.9 |
| Total | 3264 | 100 |
| Clinical Symptom | Frequency (n) | Percentage (%) |
|---|---|---|
| Constipation | 16 | 0.9 |
| Acute febrile diarrhea | 82 | 4.7 |
| Acute non-febrile diarrhea | 285 | 16.4 |
| Chronic diarrhea (HIV-positive) | 157 | 9.1 |
| Chronic diarrhea (HIV-negative) | 400 | 23 |
| Abdominal pain | 364 | 20.9 |
| Hypereosinophily | 5 | 0.3 |
| Malnutrition | 6 | 0.3 |
| Clinical anemia | 25 | 1.4 |
| Anal pruritus | 15 | 0.8 |
| Dysenteric syndrome | 60 | 3.5 |
| Fever | 143 | 8.2 |
| Dyspeptic disorders | 145 | 8.2 |
| Urticaria | 20 | 1.2 |
| Vomiting | 14 | 0.8 |
| Total | 1737 | 100 |
| Frequency (n) | Percentage (%) | 95% CI | |
|---|---|---|---|
| Parasitism | |||
| Mono-parasitism | 351 | 78.6 | 70.5–87.2 |
| Di-parasitism | 96 | 21.5 | 17.4–26.2 |
| Poly-parasitism | 16 | 3.6 | 2.1–5.8 |
| Type of parasite | |||
| Protozoa | 441 | 98.6 | 89.6–99.9 |
| Protozoa—Helminth | 6 | 1.6 | 0.4–2.9 |
| Parasite form | |||
| Vacuolar | 392 | 87.7 | 79.2–96.8 |
| Granular | 55 | 12.3 | 9.3–16 |
| Parasites Species | Frequency (n) | Percentage (%) |
|---|---|---|
| Di-parasitism | ||
| Blastocystis sp. + Cyst Entamoeba coli | 36 | 8.1 |
| Blastocystis sp. + Cyst Endolimax nana | 18 | 4 |
| Blastocystis sp. + Trophozoite Entamoeba coli | 13 | 2.9 |
| Blastocystis sp. + Cyst Giardia intestinalis | 12 | 2.7 |
| Blastocystis sp. + Ascaris lumbricoïdes | 3 | 0.8 |
| Blastocystis sp. + Trichuris trichiura | 1 | 0.2 |
| Blastocystis sp. + Teania | 1 | 0.2 |
| Polyparasitism | ||
| Blastocystis sp. + Trophozoite E. coli + Cyst E. coli | 6 | 1.3 |
| Blastocystis sp. + Cyst E. nana + Cyst E. coli | 2 | 0.4 |
| Blastocystis sp. + Pseudolimax Butschili + Cyst E. coli | 2 | 0.5 |
| Blastocystis sp. + Trophozoite E. coli + Cyst E. coli + Trichomonas. intestinalis | 1 | 0.2 |
| Blastocystis sp. + Cyst G. intestinalis + Cyst E. coli | 1 | 0.2 |
| Blastocystis sp. + T. intestinalis + Cyst E. coli | 1 | 0.2 |
| Variable | Frequency (n) | Percentage (%) | 95% CI | p Value |
|---|---|---|---|---|
| Year | ||||
| 2016 | 80 | 8.9 | 6.8–11.5 | |
| 2017 | 150 | 18.7 | 15.8–21.9 | |
| 2018 | 89 | 11.1 | 8.8–13.6 | |
| 2019 | 86 | 13.9 | 11.2–17.2 | |
| 2020 | 62 | 16.7 | 12.8–21.4 | <10−3 |
| Age group | ||||
| <15 years | 191 | 13.9 | 12.1–16.1 | |
| [15–30] | 92 | 13.1 | 10.5–16.1 | |
| [30–45] | 68 | 12.5 | 9.6–15.8 | |
| ≥45 years | 96 | 14.7 | 11.9–18 | 0.65 |
| Gender | ||||
| Female | 204 | 12.7 | 11.1–14.6 | |
| Male | 243 | 14.6 | 12.8–15.5 | 0.12 |
| Season | ||||
| Rainy | 124 | 15.7 | 13.1–18.7 | |
| Dry | 323 | 13.1 | 11.6–15.5 | 0.06 |
| Symptom | ||||
| Asymptomatic | 246 | 16.1 | 14.2–18.2 | |
| Symptomatic | 201 | 11.6 | 10–13.2 | <10−3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sylla, K.; Sow, D.; Lelo, S.; Dieng, T.; Tine, R.C.; Faye, B. Blastocystis sp. Infection: Prevalence and Clinical Aspects among Patients Attending to the Laboratory of Parasitology–Mycology of Fann University Hospital, Dakar, Senegal. Parasitologia 2022, 2, 292-301. https://doi.org/10.3390/parasitologia2040024
Sylla K, Sow D, Lelo S, Dieng T, Tine RC, Faye B. Blastocystis sp. Infection: Prevalence and Clinical Aspects among Patients Attending to the Laboratory of Parasitology–Mycology of Fann University Hospital, Dakar, Senegal. Parasitologia. 2022; 2(4):292-301. https://doi.org/10.3390/parasitologia2040024
Chicago/Turabian StyleSylla, Khadime, Doudou Sow, Souleye Lelo, Thérèse Dieng, Roger Clément Tine, and Babacar Faye. 2022. "Blastocystis sp. Infection: Prevalence and Clinical Aspects among Patients Attending to the Laboratory of Parasitology–Mycology of Fann University Hospital, Dakar, Senegal" Parasitologia 2, no. 4: 292-301. https://doi.org/10.3390/parasitologia2040024