
IgM-Associated Cryoglobulinaemia

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Clonal IgM Disorders
3. Clinical Characteristics
4. Diagnostic Evaluation
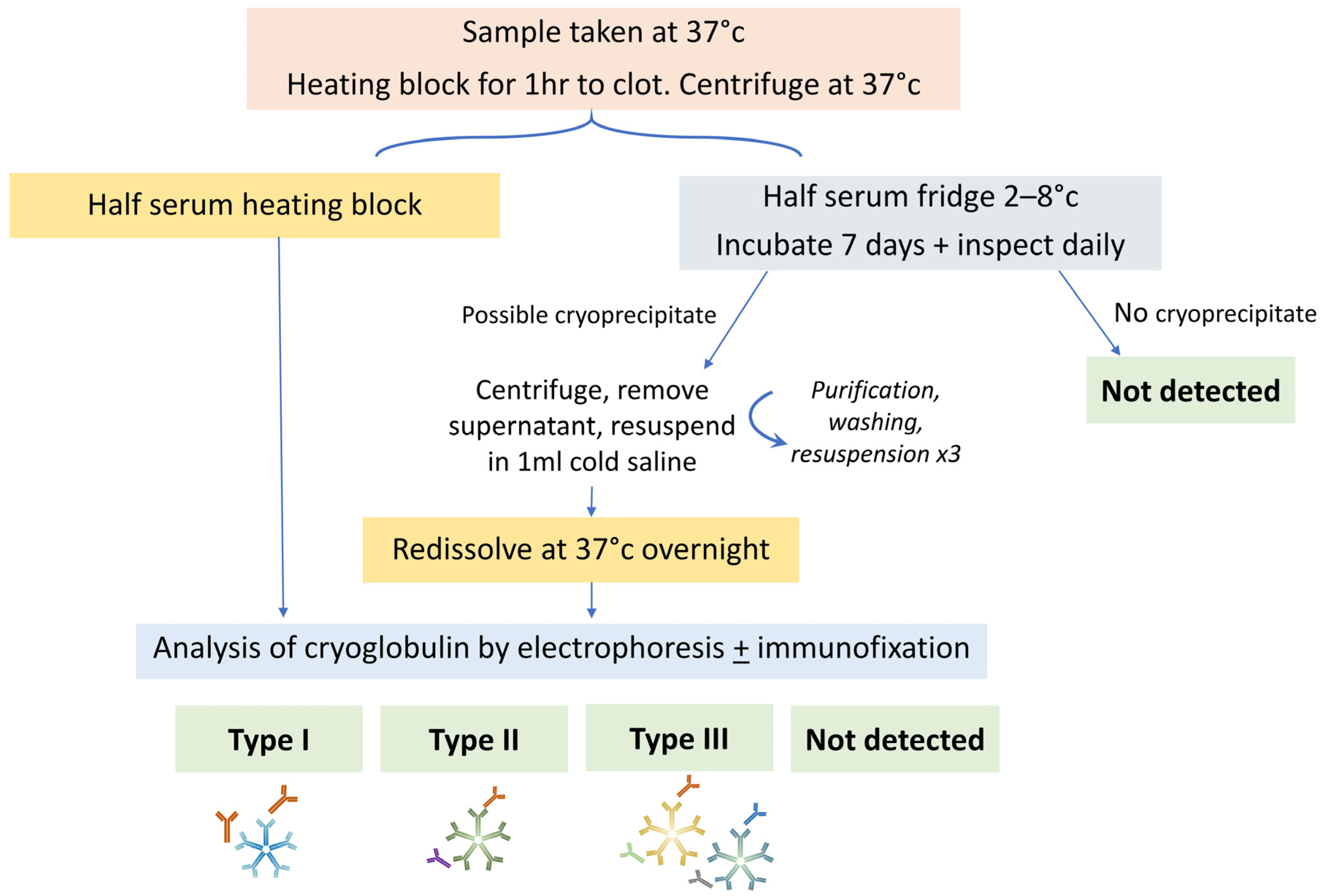
4.1. Cryoglobulin Detection
4.2. Organ Involvement
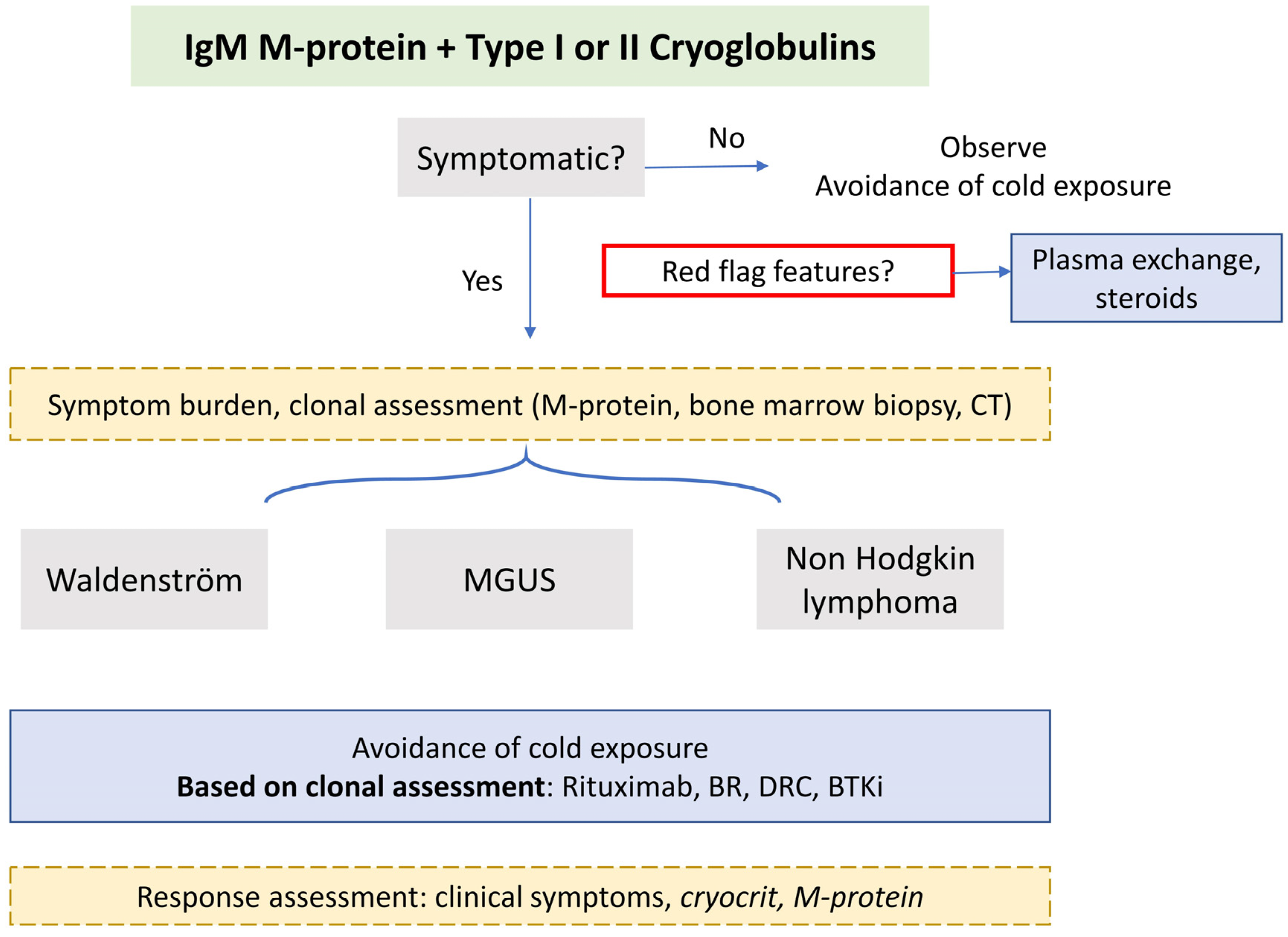
5. Management
5.1. Red Flag Symptoms
5.2. Symptomatic Disease
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wintrobe, N.; Buell, M. Hypreproteinemia Associated with Multiple Myeloma with Report of Case in Which Extraordinary Hyperproteinemia Was Associated with Thrombosis of Retinal Veins and Symptom Suggesting Raynauds Disease; Bull Johns Hopkins Hospital: Baltimore, MD, USA, 1933. [Google Scholar]
- Brouet, J.C.; Clauvel, J.P.; Danon, F.; Klein, M.; Seligmann, M. Biologic and clinical significance of cryoglobulins. A report of 86 cases. Am. J. Med. 1974, 57, 775–788. [Google Scholar] [CrossRef] [PubMed]
- Kolopp-Sarda, M.N.; Nombel, A.; Miossec, P. Cryoglobulins Today: Detection and Immunologic Characteristics of 1675 Positive Samples from 13,439 Patients Obtained Over Six Years. Arthritis Rheumatol. 2019, 71, 1904–1912. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [Green Version]
- Khwaja, J.; D’Sa, S.; Minnema, M.C.; Kersten, M.J.; Wechalekar, A.; Vos, J.M. IgM monoclonal gammopathies of clinical significance: Diagnosis and management. Haematologica 2022, 107, 2037–2050. [Google Scholar] [CrossRef] [PubMed]
- Gkalea, V.; Fotiou, D.; Dimopoulos, M.A.; Kastritis, E. Monoclonal Gammopathy of Thrombotic Significance. Cancers 2023, 15, 480. [Google Scholar] [CrossRef] [PubMed]
- Tzioufas, A.G.; Boumba, D.S.; Skopouli, F.N.; Moutsopoulos, H.M. Mixed monoclonal cryoglobulinemia and monoclonal rheumatoid factor cross-reactive idiotypes as predictive factors for the development of lymphoma in primary Sjögren’s syndrome. Arthritis Rheum. 1996, 39, 767–772. [Google Scholar] [CrossRef]
- Theander, E.; Henriksson, G.; Ljungberg, O.; Mandl, T.; Manthorpe, R.; Jacobsson, L.T. Lymphoma and other malignancies in primary Sjögren’s syndrome: A cohort study on cancer incidence and lymphoma predictors. Ann. Rheum. Dis. 2006, 65, 796–803. [Google Scholar] [CrossRef]
- Monti, G.; Pioltelli, P.; Saccardo, F.; Campanini, M.; Candela, M.; Cavallero, G.; De Vita, S.; Ferri, C.; Mazzaro, C.; Migliaresi, S.; et al. Incidence and characteristics of non-Hodgkin lymphomas in a multicenter case file of patients with hepatitis C virus-related symptomatic mixed cryoglobulinemias. Arch. Intern. Med. 2005, 165, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Marasca, R.; Vaccari, P.; Luppi, M.; Zucchini, P.; Castelli, I.; Barozzi, P.; Cuoghi, A.; Torelli, G. Immunoglobulin gene mutations and frequent use of VH1-69 and VH4-34 segments in hepatitis C virus-positive and hepatitis C virus-negative nodal marginal zone B-cell lymphoma. Am. J. Pathol. 2001, 159, 253–261. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.-L.; Cao, X.-X.; Shen, K.-N.; Han, H.-X.; Zhang, C.-L.; Qiu, Y.; Zhao, H.; Gao, X.-M.; Feng, J.; Zhang, L.; et al. Clinical characteristics and treatment outcome of type I cryoglobulinemia in Chinese patients: A single-center study of 45 patients. Ann. Hematol. 2020, 99, 1735–1740. [Google Scholar] [CrossRef]
- Néel, A.; Perrin, F.; Decaux, O.; Dejoie, T.; Tessoulin, B.; Halliez, M.; Mahé, B.; Lamy, T.; Fakhouri, F.; Jego, P.; et al. Long-term outcome of monoclonal (type 1) cryoglobulinemia. Am. J. Hematol. 2014, 89, 156–161. [Google Scholar] [CrossRef]
- Harel, S.; Mohr, M.; Jahn, I.; Aucouturier, F.; Galicier, L.; Asli, B.; Malphettes, M.; Szalat, R.; Brouet, J.-C.; Lipsker, D.; et al. Clinico-biological characteristics and treatment of type I monoclonal cryoglobulinaemia: A study of 64 cases. Br. J. Haematol. 2015, 168, 671–678. [Google Scholar] [CrossRef]
- Terrier, B.; Krastinova, E.; Marie, I.; Launay, D.; Lacraz, A.; Belenotti, P.; de Saint-Martin, L.; Quemeneur, T.; Huart, A.; Bonnet, F.; et al. Management of noninfectious mixed cryoglobulinemia vasculitis: Data from 242 cases included in the CryoVas survey. Blood 2012, 119, 5996–6004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gemignani, F.; Brindani, F.; Alfieri, S.; Giuberti, T.; Allegri, I.; Ferrari, C.; Marbini, A. Clinical spectrum of cryoglobulinaemic neuropathy. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1410–1414. [Google Scholar] [CrossRef] [Green Version]
- Monti, G.; Galli, M.; Invernizzi, F.; Pioltelli, P.; Saccardo, F.; Monteverde, A.; Pietrogrande, M.; Renoldi, P.; Bombardieri, S.; Bordin, G. Cryoglobulinaemias: A multi-centre study of the early clinical and laboratory manifestations of primary and secondary disease. GISC. Italian Group for the Study of Cryoglobulinaemias. QJM Int. J. Med. 1995, 88, 115–126. [Google Scholar]
- Hira-Kazal, R.; Sayar, Z.; Kothari, J.; Ayrton, P.; Berney, S.; Maher, J. Cryoglobulinaemia identified by repeated analytical failure of laboratory tests. Lancet 2014, 383, 382. [Google Scholar] [CrossRef]
- Terrier, B.; Karras, A.; Kahn, J.E.; Le Guenno, G.; Marie, I.; Benarous, L.; Lacraz, A.; Diot, E.; Hermine, O.; de Saint-Martin, L.; et al. The spectrum of type I cryoglobulinemia vasculitis: New insights based on 64 cases. Medicine 2013, 92, 61–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaidan, M.; Terrier, B.; Pozdzik, A.; Frouget, T.; Rioux-Leclercq, N.; Combe, C.; Lepreux, S.; Hummel, A.; Noël, L.-H.; Marie, I.; et al. Spectrum and Prognosis of Noninfectious Renal Mixed Cryoglobulinemic GN. J. Am. Soc. Nephrol. 2016, 27, 1213–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Sa, S.; Kersten, M.J.; Castillo, J.J.; Dimopoulos, M.; Kastritis, E.; Laane, E.; Leblond, V.; Merlini, G.; Treon, S.P.; Vos, J.M.; et al. Investigation and management of IgM and Waldenström-associated peripheral neuropathies: Recommendations from the IWWM-8 consensus panel. Br. J. Haematol. 2017, 176, 728–742. [Google Scholar] [CrossRef]
- Kolopp-Sarda, M.N.; Azevedo, P.M.; Miossec, P. IgG subclasses in cryoglobulins: Link to composition and clinical manifestations. Arthritis Res. Ther. 2020, 22, 267. [Google Scholar] [CrossRef]
- Nemni, R.; Corbo, M.; Fazio, R.; Quattrini, A.; Comi, G.; Canal, N. Cryoglobulinaemic neuropathy. A clinical, morphological and immunocytochemical study of 8 cases. Brain 1988, 111 Pt 3, 541–552. [Google Scholar] [CrossRef] [PubMed]
- Vallat, J.M.; Desproges-Gotteron, R.; Leboutet, M.J.; Loubet, A.; Gualde, N.; Treves, R. Cryoglobulinemic neuropathy: A pathological study. Ann. Neurol. 1980, 8, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Ciompi, M.; Marini, D.; Siciliano, G.; Melchiorre, D.; Bazzichi, L.; Sartucci, F.; Murri, L. Cryoglobulinemic peripheral neuropathy: Neurophysiologic evaluation in twenty-two patients. Biomed. Pharmacother. 1996, 50, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Sidana, S.; Rajkumar, S.V.; Dispenzieri, A.; Lacy, M.Q.; Gertz, M.A.; Buadi, F.K.; Hayman, S.R.; Dingli, D.; Kapoor, P.; Gonsalves, W.I.; et al. Clinical presentation and outcomes of patients with type 1 monoclonal cryoglobulinemia. Am. J. Hematol. 2017, 92, 668–673. [Google Scholar] [CrossRef]
- Motyckova, G.; Murali, M. Laboratory testing for cryoglobulins. Am. J. Hematol. 2011, 86, 500–502. [Google Scholar] [CrossRef]
- Pratt, G.; El-Sharkawi, D.; Kothari, J.; D’Sa, S.; Auer, R.; McCarthy, H.; Krishna, R.; Miles, O.; Kyriakou, C.; Owen, R. Diagnosis and management of Waldenström macroglobulinaemia-A British Society for Haematology guideline. Br. J. Haematol. 2022, 197, 171–187. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, F.; Monti, G. Colchicine and mixed cryoglobulinemia. Arthritis Rheum. 1993, 36, 722–723. [Google Scholar] [CrossRef]
- De Vita, S.; Quartuccio, L.; Isola, M.; Mazzaro, C.; Scaini, P.; Lenzi, M.; Campanini, M.; Naclerio, C.; Tavoni, A.; Pietrogrande, M.; et al. A randomized controlled trial of rituximab for the treatment of severe cryoglobulinemic vasculitis. Arthritis Rheum. 2012, 64, 843–853. [Google Scholar] [CrossRef] [Green Version]
- Nehme-Schuster, H.; Korganow, A.S.; Pasquali, J.L.; Martin, T. Rituximab Inefficiency during Type I Cryoglobulinaemia; Rheumatology: Oxford, UK, 2005; Voluem 44, pp. 410–411. [Google Scholar]
- Sène, D.; Ghillani-Dalbin, P.; Amoura, Z.; Musset, L.; Cacoub, P. Rituximab may form a complex with IgMkappa mixed cryoglobulin and induce severe systemic reactions in patients with hepatitis C virus-induced vasculitis. Arthritis Rheum. 2009, 60, 3848–3855. [Google Scholar] [CrossRef]
- Khwaja, J.; Uppal, E.; Baker, R.; Trivedi, K.; Rismani, A.; Gupta, R.; Proctor, I.; Kyriakou, C.; D’Sa, S. Bortezomib-based therapy is effective and well tolerated in frontline and multiply pre-treated Waldenström macroglobulinaemia including BTKi failures: A real-world analysis. EJHaem 2022, 3, 1330–1334. [Google Scholar] [CrossRef]
- Ferri, C.; Sebastiani, M.; Giuggioli, D.; Cazzato, M.; Longombardo, G.; Antonelli, A.; Puccini, R.; Michelassi, C.; Zignego, A.L. Mixed cryoglobulinemia: Demographic, clinical, and serologic features and survival in 231 patients. Semin. Arthritis Rheum. 2004, 33, 355–374. [Google Scholar] [CrossRef] [PubMed]
- Hermine, O.; Lefrère, F.; Bronowicki, J.-P.; Mariette, X.; Jondeau, K.; Eclache-Saudreau, V.; Delmas, B.; Valensi, F.; Cacoub, P.; Brechot, C.; et al. Regression of splenic lymphoma with villous lymphocytes after treatment of hepatitis C virus infection. N. Engl. J. Med. 2002, 347, 89–94. [Google Scholar] [CrossRef]
- Saadoun, D.; Resche Rigon, M.; Sene, D.; Terrier, B.; Karras, A.; Perard, L.; Schoindre, Y.; Coppéré, B.; Blanc, F.; Musset, L.; et al. Rituximab plus Peg-interferon-alpha/ribavirin compared with Peg-interferon-alpha/ribavirin in hepatitis C-related mixed cryoglobulinemia. Blood 2010, 116, 326–334. [Google Scholar] [CrossRef]
- Dammacco, F.; Tucci, F.A.; Lauletta, G.; Gatti, P.; De Re, V.; Conteduca, V.; Sansonno, S.; Russi, S.; Mariggiò, M.A.; Chironna, M.; et al. Pegylated interferon-alpha, ribavirin, and rituximab combined therapy of hepatitis C virus-related mixed cryoglobulinemia: A long-term study. Blood 2010, 116, 343–353. [Google Scholar] [CrossRef] [Green Version]
- Pozzato, G.; Mazzaro, C.; Artemova, M.; Abdurakhmanov, D.; Grassi, G.; Crosato, I.; Mauro, E.; Ghersetti, M.; Zorat, F.; Bomben, R.; et al. Direct-acting antiviral agents for hepatitis C virus-mixed cryoglobulinaemia: Dissociated virological and haematological responses. Br. J. Haematol. 2020, 191, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Arcaini, L.; Besson, C.; Frigeni, M.; Fontaine, H.; Goldaniga, M.; Casato, M.; Visentini, M.; Torres, H.A.; Loustaud-Ratti, V.; Peveling-Oberhag, J.; et al. Interferon-free antiviral treatment in B-cell lymphoproliferative disorders associated with hepatitis C virus infection. Blood 2016, 128, 2527–2532. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.J.; Kim, W.S.; Kim, S.J.; Lee, J.J.; Yang, D.H.; Kim, J.S.; Lee, S.R.; Lee, G.W.; Kim, H.J.; Kim, H.Y.; et al. Phase II trial of rituximab plus CVP combination chemotherapy for advanced stage marginal zone lymphoma as a first-line therapy: Consortium for Improving Survival of Lymphoma (CISL) study. Ann. Hematol. 2012, 91, 543–551. [Google Scholar] [CrossRef]
- Rummel, M.J.; Niederle, N.; Maschmeyer, G.; Banat, G.A.; von Grünhagen, U.; Losem, C.; Kofahl-Krause, D.; Heil, G.; Welslau, M.; Balser, C.; et al. Bendamustine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: An open-label, multicentre, randomised, phase 3 non-inferiority trial. Lancet 2013, 381, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Laribi, K.; Tempescul, A.; Ghnaya, H.; Denizon, N.; Besançon, A.; Anghel, A.; Farhi, J.; Truong, C.; Lemaire, P.; Poulain, S.; et al. The bendamustine plus rituximab regimen is active against primary nodal marginal zone B-cell lymphoma. Hematol. Oncol. 2017, 35, 536–541. [Google Scholar] [CrossRef]
- Lauletta, G.; Russi, S.; Pavone, F.; Vacca, A.; Dammacco, F. Direct-acting antiviral agents in the therapy of hepatitis C virus-related mixed cryoglobulinaemia: A single-centre experience. Arthritis Res. Ther. 2017, 19, 74. [Google Scholar] [CrossRef] [Green Version]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khwaja, J.; Salter, S.J.; D’Sa, S. IgM-Associated Cryoglobulinaemia. Hemato 2023, 4, 240-249. https://doi.org/10.3390/hemato4030019
Khwaja J, Salter SJ, D’Sa S. IgM-Associated Cryoglobulinaemia. Hemato. 2023; 4(3):240-249. https://doi.org/10.3390/hemato4030019
Chicago/Turabian StyleKhwaja, Jahanzaib, Simon J. Salter, and Shirley D’Sa. 2023. "IgM-Associated Cryoglobulinaemia" Hemato 4, no. 3: 240-249. https://doi.org/10.3390/hemato4030019