1. Case Presentation
In October 2019, a 70-year-old male with a medical history of hypertension, COPD, and pulmonary fibrosis presented to the emergency department with fever and abdominal pain. The pain was accompanied by a feeling of general weakness. He stated the pain had begun 10 days before and that he had previously presented it to the emergency department of another hospital; he was dismissed with the diagnosis of acute gastritis. His abdomen was tender with right-sided and lower quadrant pain upon palpation. No skin abnormalities were noted.
His temperature was up to 38°. His blood pressure was 145/90 mmHg with a pulse rate of 101/min. The complete blood count including platelets and leukocytes was normal and kidney function was within the normal range, while the PCR and LDH increased (304 mg/L and 352 UI/L, respectively) and coagulation tests showed an increased INR of 1.54 and aPTT of 53.
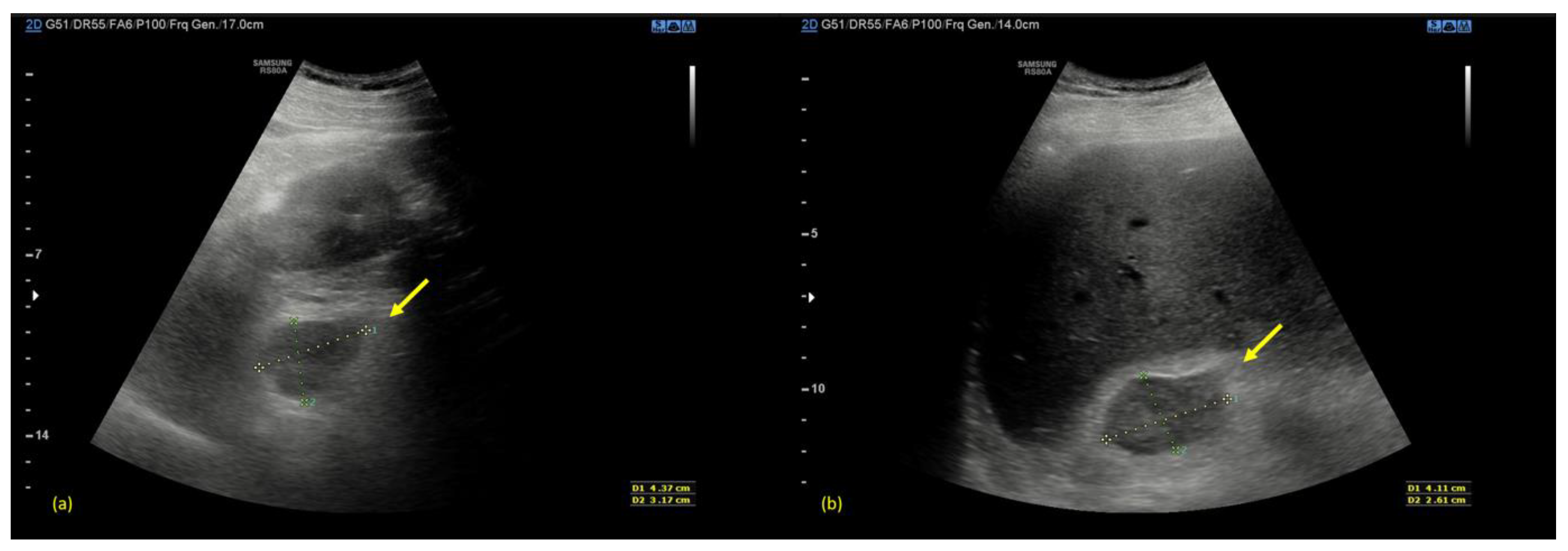
An urgent ultrasonography scan (US) was performed with a convex transducer that revealed an enlargement of both adrenal glands with inhomogeneous echogenicity (
Figure 1).
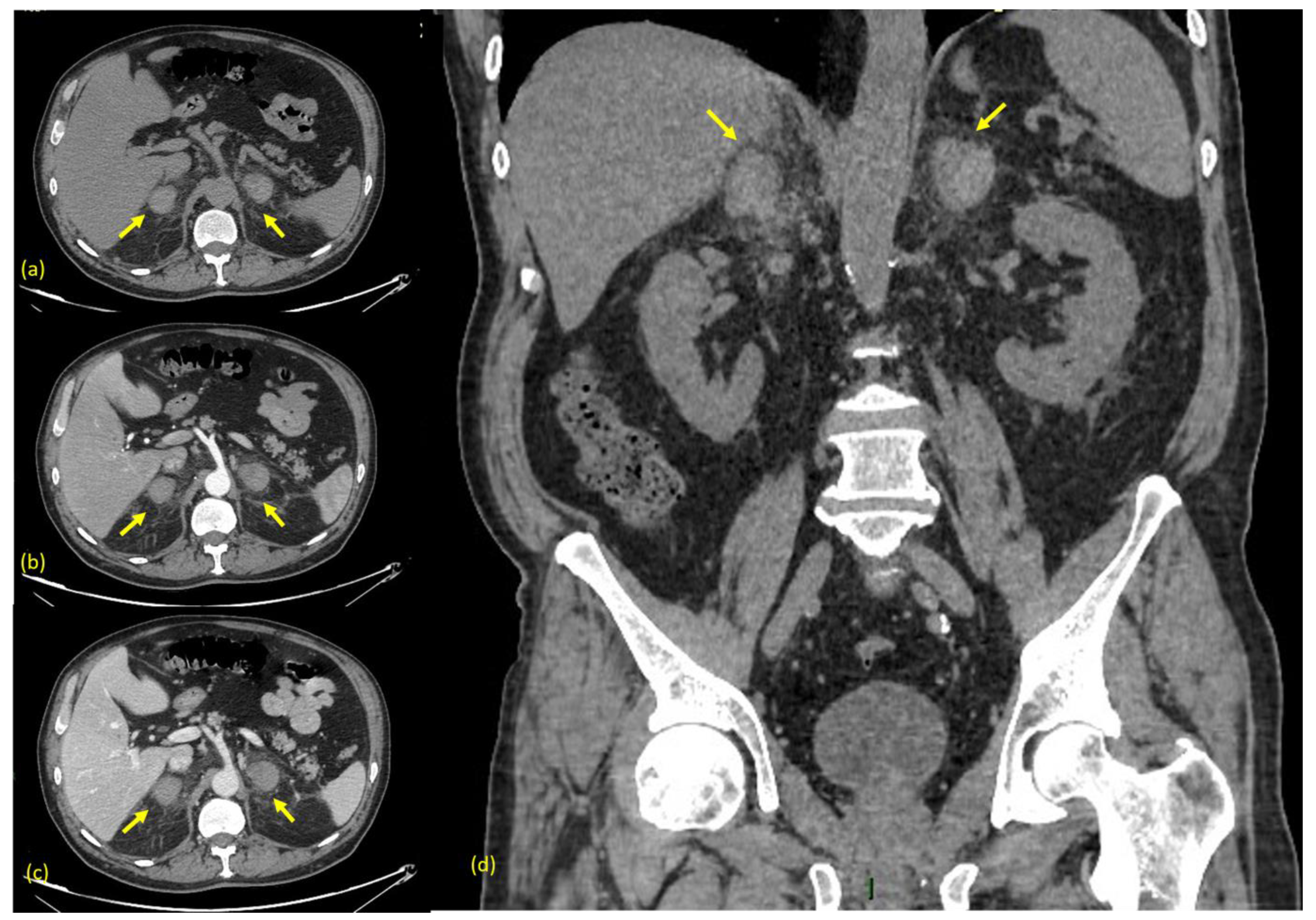
Therefore, he was immediately subjected to a computed tomography (CT) scan of the abdomen before and after the administration of contrast medium (Omnipaque 350 mgI/mL, 130 mL, 3 mL/s), with a 1.25 mm slice width, 120 kV, and 7 mAs. The non-contrast phase demonstrated slightly hyperdense round masses with fuzzy margins and a diffuse swelling of both adrenal glands, associated with inflammatory changes in the surrounding retroperitoneal fat, confirming the presence of a bilateral adrenal hemorrhage (
Figure 2a). After the intravenous contrast, no enhancement was revealed (with density values of 45–55 HU both in pre-contrast and post-contrast phases) and no ”blushes” were revealed, suggesting no evidence of active bleeding (
Figure 2b–d).
In the suspicion of meningococcal infection, intravenous antibiotic therapy with ceftriaxone immediately started, and blood culture and serology were performed, which then produced a negative result.
He was then hospitalized, antibiotic therapy was suspended, and adrenal insufficiency was confirmed. His adrenocorticotropin (ACTH) measurement was 185 pg/mL with high cortisol levels up to 65 ng/mL. The 24 h urine tests were in the normal range, except for a slight reduction in metanephrine (<11 mg/24 h). Replacement therapy with hydrocortisone started, initially intravenously and subsequently orally at the minimum effective dose. On subsequent days, he was able to maintain normal electrolyte levels, and he was discharged after 10 days of hospitalization.
During hospitalization, additional tests were performed, including a serum protein electrophoresis and immunofixation, which demonstrated an IgG lambda monoclonal gammopathy.
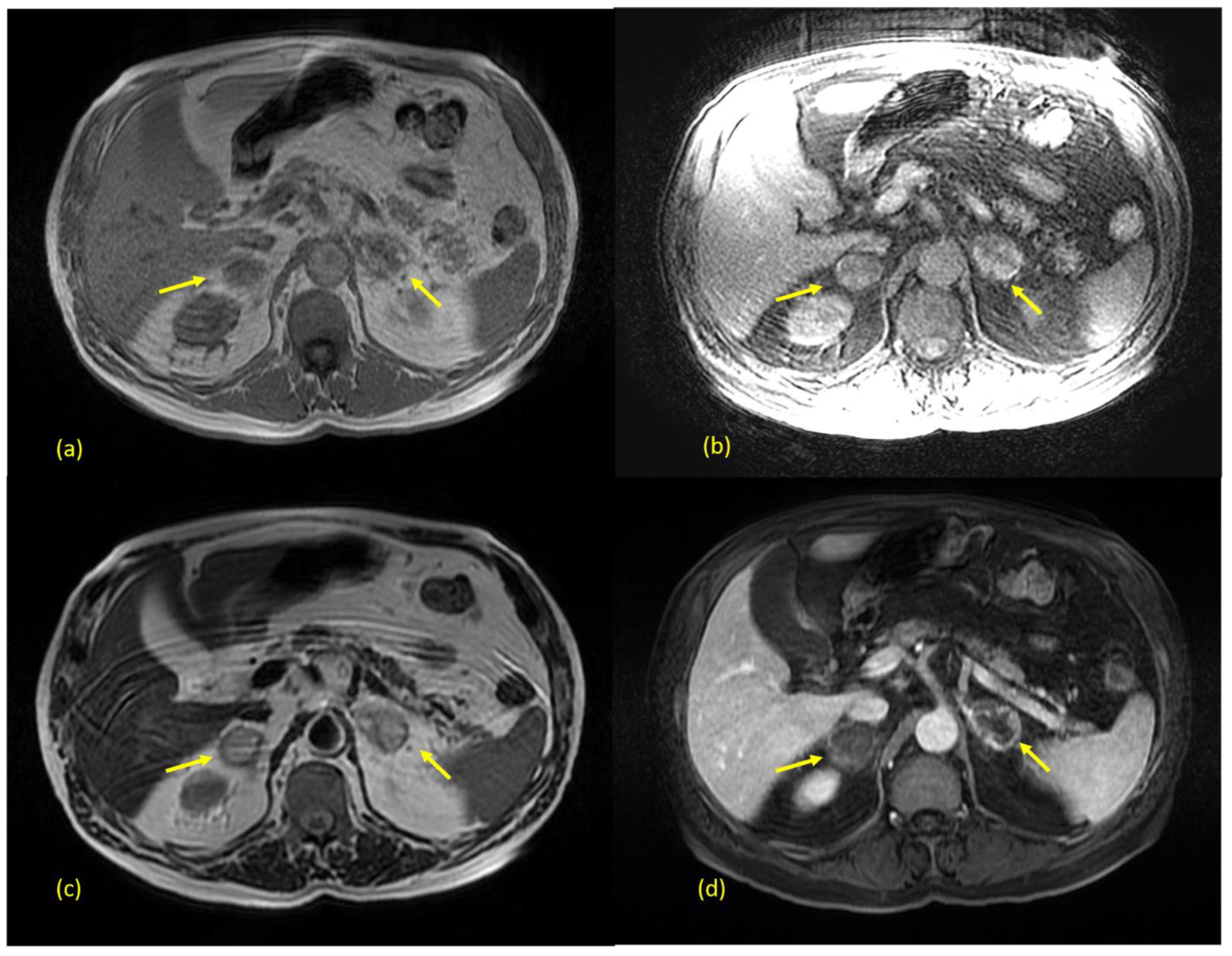
Three days after discharge, magnetic resonance imaging (MRI) was performed using a 1.5 T device, with ssFSE, LAVA, FSPGR 2D, and 3D sequences (some of which deteriorated by motion artifacts), before and after the administration of a paramagnetic contrast medium (Prohance, 0.2 mL/Kg), with a slice width between 2 and 6 mm. The MRI confirmed the enlargement of adrenal glands and showed the hyperintensity of the central adrenal region both on T1- and T2-weighted images, which is suggestive of subacute stage hematoma (>7 days to 7 weeks after onset), in association with peripheral residual parenchyma (
Figure 3a–d).
2. Discussion
The Waterhouse-Friderichsen syndrome (WFS), also known as
Purpura fulminans, is a rare but usually fatal event. First described in 1911 by Rupert Waterhouse and Carl Friderichsen, it consists of the acute hemorrhage of the adrenal glands, most frequently observed in the pediatric population rather than adult populations; it is commonly related to several infections, among which infections from
Neisseria meningitidis represents the majority of the cases [
1]. In addition to this, throughout the years, many other etiologies have been demonstrated, such as sepsis due to different organisms or non-infectious diseases such as thromboembolism [
2], the administration of anticoagulants [
3], antiphospholipid syndrome [
4], traumas, tumors, and cardiovascular dysfunction [
5]. As for infections, several other microorganisms have been identified as possible causes of this adrenal disease, the most common of which include bacteria such as
Neisseria Gonorrhoeae,
Streptococcus pneumoniae, group A
Streptococcus,
Staphylococcus aureus,
Haemophilus influenzae,
Pseudomonas aeruginosa, and
Escherichia coli but also viruses such as
Varicella-Zoster virus,
Epstein–Barr virus,
Cytomegalovirus, and
Parvovirus [
6,
7,
8,
9,
10]. Even if the pathophysiology of Waterhouse Friderichsen Syndrome is not completely clear, numerous theories have been assumed, and one of the most important theories suggests endotoxin-mediated damage. Endotoxins can cause the transcription of several genes that transcribe for inflammatory cytokines involved in fibrinolysis and coagulation [
11]. Another theory that could explain cases in which a clear cause cannot be identified is an increased synthesis of cortisol and adrenaline by the adrenal gland, which usually occurs in any stressful condition: cortisol tends to increase adrenal blood flows and the pressure within the vessels while adrenaline, on the other hand, induces platelet aggregation in the adrenaline veins, increasing the risk of hemorrhaging [
12,
13].
As far as the symptoms are concerned, patients with adrenal hemorrhage usually have a non-specific clinical presentation, such as abdominal pain, vomiting, fever, hypotension, headache, aching joints, and lethargy [
14]. The majority of them can develop a skin rash and, in the most severe cases, convulsions, cardiovascular collapse, and consequent shock.
As for the laboratory tests, they often show leukocytosis and coagulation abnormalities; metabolic acidosis can be associated and, as a consequence of the adrenal damage, hyperkalemia, hyponatremia, and hypoglycemia can also be present.
It comes as a consequence that, due to the non-specificity of both clinical presentation and laboratory findings, a clinical diagnosis of WFS can be very challenging.
If clinically suspected, an urgent CT scan of the abdomen is strongly suggested as the “gold standard” in the diagnosis of adrenal hemorrhage. It usually shows adrenal hematomas that characteristically appear round or oval, often with surrounding strandings of the periadrenal fat. In rare cases, if arterial active bleeding is occurring, a post-contrast blush might be also detected [
15,
16]. A condition named “adrenal congestion”, which consists in thickening of adrenal glands and the stranding of the periadrenal fat, can be occasionally detected before the hemorrhage [
17]. When clinical and laboratory findings are non-specific, as they were in our case, the CT scan may be preceded by a US scan, which can show an increased volume of both the adrenal glands with diffuse or inhomogeneous echogenicity due to the presence of hematomas [
18].
Due to the potentially lethal outcome, the antibiotic administration should start as soon as possible. In his writings, Friderichsen also emphasized the need for corticosteroid administration [
1], which is currently not recommended by some authors, who claim that patients with WFS often present high cortisol blood levels and that adrenal insufficiency occurs very rarely. On the other hand, some studies report cases of dramatic clinical improvements after the administration of corticosteroids [
19].
3. Radiological Management
In the management of a patient presenting abdominal pain, ultrasonography (US) is usually the first modality to be performed. The pattern of echogenicity of an adrenal hematoma depends on the time since the onset.
During the first days, a hematoma has the look of a mass with inhomogeneous echogenicity. As days go by, the hematoma tends to liquefy, starting to show peripheral heterogeneous echogenicity with a hypoechoic core. Eventually, it tends to become anechoic and appears similar to a pseudocyst. Color Doppler US can be helpful for confirming the absence of vascular signals [
20].
Computed Tomography (CT) is the most important tool in the diagnosis of adrenal bleeding. Adrenal hematomas can typically be detected in the non-contrast phase, where they appear as round to ovoid lesions, usually associated with periadrenal fat stranding and, sometimes, the involvement of the peri-nephric space. The acquisition of post-contrast phases (arterial, venous, and excretory) is crucial to detect any presence of active bleeding, seen as an arterial “blush” [
15].
As for the CT density values of an adrenal hematoma, they depend on its stage. In the acute stage, a hematoma usually contains high attenuation areas (between 50 and 90 HU); as time goes on, its size and attenuation values decrease and, in some cases, a complete resolution can be seen.
The typical appearance of a chronic hematoma is a hypodense mass with internal calcifications [
16]. An “adrenal congestion”, which consists in the thickening of the adrenal glands and stranding of the periadrenal fat, can be occasionally detected before the hemorrhage [
17].
A magnetic Resonance Imaging (MRI) scan is the most accurate diagnostic modality and is considered the gold standard in follow-up. It can differentiate acute from chronic hematomas and can also ascertain the presence of an underlying tumor [
20].
In the acute stage (within the first week), a hematoma has the look of an isointense or mildly hypointense mass on T1 weighted sequences, which becomes strongly hypointense on T2-weighted sequences.
In the subacute stage (between 1 to 7 weeks), it usually shows hyperintensity both on T1- and T2-weighted sequences.
Finally, in the chronic stage, (after more than 7 weeks), it typically shows a thin hypointensity edge on both T1- and T2-weighted sequences, which is correlated to hemosiderin’s presence and to the formation of a thin fibrous capsule [
21].
In the differential diagnosis, it is always important to take into consideration other types of lesions. The most benign lesions include cysts, usually seen in syndromic diseases such as adult polycystic kidney disease [
22]. A cyst can be identified with ultrasonography scans as an anechoic and avascular formation with posterior beam enhancements, and it appears as a round fluid lesion on CT with no enhancements after contrast.
On the other hand, adrenal tumors are usually solid and well-vascularized lesions; therefore, they tend to show enhancement after contrast even if they may have central areas with no enhancement due to necrosis, and the most malignant can be associated with the presence of metastasis in other organs. The most common adrenal tumors include adenomas, myelolipomas, pheochromocytomas, neuroblastomas, and metastasis [
23].
Sometimes, on a non-contrast CT, it can be difficult to distinguish an adrenal cyst from an adenoma, as they can both show fluid density (between 10 and −10 HU), but after contrast, an adenoma will show enhancements while a cyst will not.
A rarer but interesting condition is congenital adrenal hyperplasia, usually seen in infants, which presents with a bilateral enlargement of both adrenal glands with a typical “cerebriform” pattern on ultrasonography scans, together with typical clinical and laboratory features [
24].
In some rare cases, it may not be easy to distinguish a rim-calcified chronic adrenal hematoma from an aneurysm of the splenic artery [
25].
In addition to that, clinical and laboratory findings should always be taken into consideration as they can provide guidance in the radiological diagnosis.
4. Conclusions
The Waterhouse-Friderichsen syndrome is a very uncommon disorder but with high morbidity and mortality, and it is frequently connected to a lack of awareness or education regarding its management. An accurate, timely, and multidisciplinary approach is vitally important and can dramatically improve the chances of survival since the prognosis depends on the timeliness of diagnosis and the consequent treatment.
This case report aims raise awareness about the need of considering the Waterhouse-Friderichsen syndrome in the differential diagnosis of patients presenting with acute abdominal pain and, at the same time, to highlight the extreme importance of multimodality imaging both in the early diagnosis and in the follow-up of this rare disease in order to implement early and appropriate treatment, reduce hospitalization, and, in some cases, obtain a complete recovery of the adrenal function, allowing the preservation of the patient’s quality of life.
Author Contributions
Conceptualization: M.L.A., A.D.C., C.D., M.C., A.P., L.F., M.P. and F.F.; methodology: M.L.A., A.D.C., C.D., M.C. and F.O.; resources: A.P., L.F., M.P., F.F. and T.P.; data curation: M.L.A., A.D.C., C.D., M.C., A.P., L.F., M.P. and F.F.; writing—original draft preparation: M.L.A., A.D.C., C.D., M.C. and F.O.; writing—review and Editing: M.L.A., A.D.C., C.D. and F.O.; visualization: M.L.A., A.D.C., C.D., M.C. and F.O.; supervision: A.P., F.F. and T.P.; project administration: A.P., L.F., M.P., F.F. and T.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Fondazione Policlinico Gemelli (protocol code 0025817/22, 3 August 2022).
Informed Consent Statement
Patient consent was waived since the study’s data were anonymized.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available due to privacy restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Waterhouse, R. A Case of Suprarenal Apoplexy. Lancet 1911, 177, 577–578. [Google Scholar] [CrossRef]
- Rosenberger, L.H.; Smith, P.W.; Sawyer, R.G.; Hanks, J.B.; Adams, R.B.; Hedrick, T.L. Bilateral ad-renal hemorrhage: The unrecognized cause of hemodynamic collapse associated with heparin-induced thrombocytopenia. Crit. Care Med. 2011, 39, 833–838. [Google Scholar] [CrossRef] [Green Version]
- Alidoost, M.; Soomro, R.; Gubeladze, A.; Morabia, A.; Holland, S.; Asif, A.; Hossain, M.A. Rivaroxaban Related Bilateral Adrenal Hemorrhage: A Rare Complications of Direct Oral Anticoagulants—A Case Reports. Am. J. Case Rep. 2019, 20, 1607–1611. [Google Scholar] [CrossRef] [PubMed]
- Espinosa, G.; Santos, E.; Cervera, R.; Piette, J.C.; de la Red, G.; Gil, V.; Font, J.; Couch, R.; Ingelmo, M.; Asherson, R.A. Adrenal involvement in the an-tiphospholipid syndrome: Clinical and immunologic characteristics of 86 patients. Medicine 2003, 82, 106–118. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, D.; Harris, M.D.; Foweraker, J.; Gresham, G.A. Waterhouse-Friderichsen syndrome as a result of non-meningococcal infection. J. Clin. Pathol. 2004, 57, 208–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicho, R.; Jimenez, P.; Leon, C.; Sanchez, J.A.; Sancho, H. Waterhouse-Friderichsen syndrome secondary to Escherichia coli septicaemia. Int. J. Intensive Care 2004, 11, 133–135. [Google Scholar]
- Adem, P.V.; Montgomery, C.P.; Husain, A.N.; Koogler, T.K.; Arangelovich, V.; Humilier, M.; Boyle-Vavra, S.; Daum, R.S. Staphylococcus aureus sepsis and the Waterhouse-Friderichsen syndrome in children. N. Engl. J. Med. 2005, 353, 1245–1251. [Google Scholar] [CrossRef]
- Ventura Spagnolo, E.; Mondello, C.; Roccuzzo, S.; Stassi, C.; Cardia, L.; Grieco, A.; Raffino, C. A unique fatal case of Waterhouse-Friderichsen syndrome caused by Proteus mirabilis in an immunocompetent subject: Case report and literature analysis. Medicine 2019, 98, e16664. [Google Scholar] [CrossRef] [PubMed]
- McGowan-Smyth, S. Bilateral adrenal haemorrhage leading to adrenal crisis. BMJ Case Rep. 2014, 2014, bcr2014204225. [Google Scholar] [CrossRef] [PubMed]
- Margaretten, W.; Nakai, H.; Landing, B.H. Septicemic adrenal hemorrhage. Am. J. Dis. Child. 1963, 105, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Fox, B. Disseminated intravascular coagulation and the Waterhouse-Friderichsen syndrome. Arch. Dis. Child. 1971, 46, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Vella, A.; Nippoldt, T.B.; Morris, J.C. Adrenal Hemorrhage: A 25-Year Experience at the Mayo Clinic. Mayo Clin. Proc. 2001, 76, 161–168. [Google Scholar] [CrossRef]
- Karki, B.R.; Sedhai, Y.R.; Bokhari, S.R.A. Waterhouse-Friderichsen Syndrome; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Chernyak, V.; Patlas, M.N.; Menias, C.O.; Soto, J.A.; Kielar, A.Z.; Rozenblit, A.M.; Romano, L.; Katz, D.S. Traumatic and non-traumatic adrenal emergencies. Emerg. Radiol. 2015, 22, 697–704. [Google Scholar] [CrossRef]
- Addeo, G.; Cozzi, D.; Danti, G.; Bertelli, E.; Ferrari, R.; Pradella, S.; Trinci, M.; Miele, V. Multi-detector computed tomography in the diagnosis and characterization of adrenal gland traumatic injuries. Gland Surg. 2019, 8, 164–173. [Google Scholar] [CrossRef]
- Munoz Corsini, L.; Delgado Arnaiz, C.; Garcia del Valle, S.; Reboto Cortes, P.; Lopez del Castillo, A. Postoperative bilateral adrenal hemorrhage: Correlation between clinical and radiological signs. J. Clin. Anesth. 2008, 20, 605–608. [Google Scholar] [CrossRef] [PubMed]
- Tan, G.; Sutherland, T. Adrenal Congestion Preceding Adrenal Hemorrage on CT Imaging: A Case Series. Abdom. Radiol. 2016, 41, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Chira, R.I.; Chira, A.; Manzat-Saplacan, R.M.; Nagy, G.; Valea, A.; Silaghi, A.C.; Mircea, P.A.; Valean, S. Adrenal glands transabdominal ultrasonography—Pictorial essay. Med. Ultrason. 2017, 19, 318–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahangir-Hekmat, M.; Taylor, H.C.; Levin, H.; Wilbur, M.; Llerena, L.A. Adrenal insufficiency attributable to adrenal hemorrhage: Long-term follow-up with reference to glucocorticoid and mineralocorticoid function and replacement. Endocr. Pract. 2004, 10, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Dahnert, W. Radiology Review Manual; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; ISBN 9781609139438. [Google Scholar]
- Jordan, E.; Poder, L.; Courtier, J.; Sai, V.; Jung, A.; Coakley, F. Imaging of Nontraumatic Adrenal Hemorrage. Am. J. Roentgenol. 2012, 199, W91–W98. [Google Scholar] [CrossRef] [PubMed]
- Bastide, C.; Boyer, L.; Djellouli, N.; Baguet, J.C.; Viallet, J.F. Bilateral adrenal cysts and hepatorenal polycystic disease. Presse Med. 1997, 26, 711–712. [Google Scholar]
- Jossart, G.H.; Burpee, S.E.; Gagner, M. Surgery of the Adrenal Gland; Springer: Berlin/Heidelberg, Germany, 2000; ISBN B00A9YH2QM. [Google Scholar]
- Hernanz-Schulman, M.; Brock, J.; Russell, W. Sonographic Findings in Infants with Congenital Adrenal Hyperplasia. Pediatr. Radiol. 2002, 32, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Khosa, F.; Krinsky, G.; Macari, M.; Yucel, E.K.; Berland, L.L. Managing Incidental Findings on Abdominal and Pelvic CT and MRI, Part 2: White Paper of the ACR Incidental Findings Committee II on Vascular Findings. J. Am. Coll. Radiol. 2013, 10, 789–794. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 
{kind=link}
{kind=link}
{kind=link}


