
Violence and Child Mental Health Outcomes in Iraq: Mapping Vulnerable Areas

School of Applied Sciences, The University of Mississippi, Oxford, MS 38677, USA
Psychiatry Int. 2024, 5(1), 39-52; https://doi.org/10.3390/psychiatryint5010004
Submission received: 16 October 2023
/
Revised: 3 January 2024
/
Accepted: 18 January 2024
/
Published: 22 January 2024
Abstract
:Few studies have been conducted in Iraq regarding the association of violence at multiple ecological levels and child mental health outcomes. Therefore, the study objectives were (1) to conduct a nationwide analysis to explore violence at multiple socio-ecological levels and children’s mental health outcomes, and (2) to identify the most vulnerable children according to the spatial distribution of Iraqi governorates. This cross-sectional study used the 2018 Iraq Multiple Indicator Cluster Survey (MICS 6), which included 12,358 mothers or caretakers who provided complete information regarding their parenting and disciplinary practices for their children between the ages of 5 and 14. Logistic regression was employed to examine the factors associated with children’s depression and anxiety. This study showed that 22% of children had depression, while 38% experienced anxiety. Notably, children residing in Iraq’s south/central regions, specifically in areas, like Nainawa, Najaf, and Basrah, exhibited notably higher anxiety and depression. The research also showed that living in unsafe neighborhoods, women’s acceptance of domestic violence, and the use of severe physical punishment as corporal discipline were all associated with the development of anxiety and depression. This study addresses the scarcity of information on children’s mental health outcomes in Iraq at national and governorate levels, emphasizing the need for urgent national-level policy discussions to achieve key Sustainable Development Goals related to ending all forms of violence against children by 2030.
Keywords:
child abuse; violence; domestic violence; corporal punishment; depression; anxiety; spatial; Iraq1. Introduction
1.1. Background
Children’s mental health is a fundamental component of their overall well-being, with far-reaching implications for their development. Therefore, the prevalence of mental health problems such as depression and anxiety in children is a global health concern [1,2]. A recent meta-analysis showed that the prevalence of depression and anxiety symptoms was 25.2% and 20.5% among children and adolescents globally [1]. Therefore, understanding the factors contributing to these conditions is important for effective intervention and policy development.
More specifically, it is crucial to explore the prevalence and determinants of mental health outcomes among Iraqi children due to the enduring impact of conflict, displacement, and societal instability in this Middle Eastern country. Conflict and instability have exposed Iraqi children and their families to a range of traumatic experiences, including violence, which can significantly contribute to the high prevalence of mental health problems [3,4,5,6,7]. Additionally, limited access to quality healthcare and psychosocial support further exacerbates the situation [8]. Social and cultural factors, such as stigma surrounding mental health, can also hinder access to care and contribute to the persistence of mental health problems [9,10]. Addressing the mental health needs of children in Iraq requires a comprehensive understanding of the determinants to design multifaceted approaches that encompasses not only clinical interventions but also efforts to promote stability, security, and community support.
Children’s mental health may be impacted by exposure to neighborhood violence and the resulting feeling of a loss of safety. Anxiety, depression, and post-traumatic stress disorder (PTSD) are just a few of the negative mental health outcomes that can result from exposure to violence and instability [11]. As a result of the perceived threat, children growing up in such settings frequently experience an increased state of alertness, which may have long-term effects on their emotional well-being [12]. As children try to deal with the unpredictability and danger that surround them, living in an unsafe community might lead to the development of anxiety disorders and depressive symptoms.
On the other hand, witnessing or experiencing domestic violence can have profound and lasting effects on a child’s mental health. Children grow up surrounded by domestic violence between caretakers often internalize feelings of helplessness, guilt, and fear. Witnessing such violence can distort their understanding of healthy relationships and coping mechanisms, leading to an increased likelihood of developing anxiety and depression. [13]. Adding to that, women’s acceptance of domestic violence may normalize this harmful behavior, creating an environment where children are more likely to witness such violence and endure its psychological consequences [14].
However, the prevalence and determinants of domestic violence acceptance among women vary across and within different countries. For example, a global study showed that the prevalence of women’s acceptance to domestic violence varied from 2% in Argentina to 90% in Afghanistan [15]. Many Iraqi women might justify, accept, and be reluctant to report domestic violence incidents to Iraqi authorities or discuss this issue openly for various reasons, including social stigma, fear of family and tribe retaliation, limited education and employment opportunities, inadequate legal protection for abused women’s rights, feelings of hopelessness and fear arising from political, social, and economic instability, and the submissive and accepting behavior of the women themselves [16,17,18]. Hence, it is essential to explore how the acceptance of domestic violence by Iraqi women contributes to the perpetuation of this destructive cycle. Examining these factors through a social-ecological model is vital to comprehensively understand their impact on children’s mental well-being.
Severe corporal punishment, characterized by harsh physical discipline, can also contribute to the development of negative mental health outcomes in children [19,20]. Children subjected to such punitive measures often experience feelings of shame, humiliation, and fear [20]. Instead of learning constructive ways to manage their behaviors, they may internalize a belief that violence is an acceptable solution to problems. This distorted perspective can lead to heightened levels of stress, anxiety, and low self-esteem as children struggle with the emotional effect of punitive discipline [19,20]. However, the acceptability and prevalence of corporal punishment vary across cultures and regions. Some studies may reflect the specific cultural norms and contexts in which they were conducted, making it challenging to generalize findings to diverse populations with different cultural perspectives on discipline [21,22].
It is important to highlight that Iraq lacks the legal protections for survivors of domestic violence. For instance, Article 41 of the Penal Code (No. 111 of 1969) legalizes “The punishment of a wife by her husband, the disciplining by parents and teachers of children under their authority within certain limits prescribed by law or by custom” [23,24]. Efforts by Iraqi legislators to pass a draft law against domestic violence and violence against children were suspended by Iraqi parliament members throughout 2019 and 2020 [24]. The absence of law that protects the rights of the abused women and children means that violence victims cannot report these incidents and expose the perpetrators. Furthermore, Iraq lacks proper shelters that can provide protection for domestic violence victims [25].
In light of these complexities and variations in research findings, it is crucial to approach the topic of corporal punishment and children’s mental health with a balanced perspective. While numerous studies suggest a link between severe corporal punishment and negative mental health outcomes, it is also essential to acknowledge that not all research findings are consistent, and further investigation is needed to fully understand the details of this relationship.
Therefore, it is important to recognize that these factors often do not exist in isolation; children may experience a combination of community violence, domestic violence, and severe corporal punishment. Early intervention is crucial in breaking the cycle of adversity and mental health struggles. As such, the objectives of this study were (1) to conduct a nationwide analysis to explore violence at multiple socio-ecological levels and children’s mental health outcomes, and (2) to identify the most vulnerable children according to the spatial distribution of Iraqi governorates.
1.2. Theoretical Framework
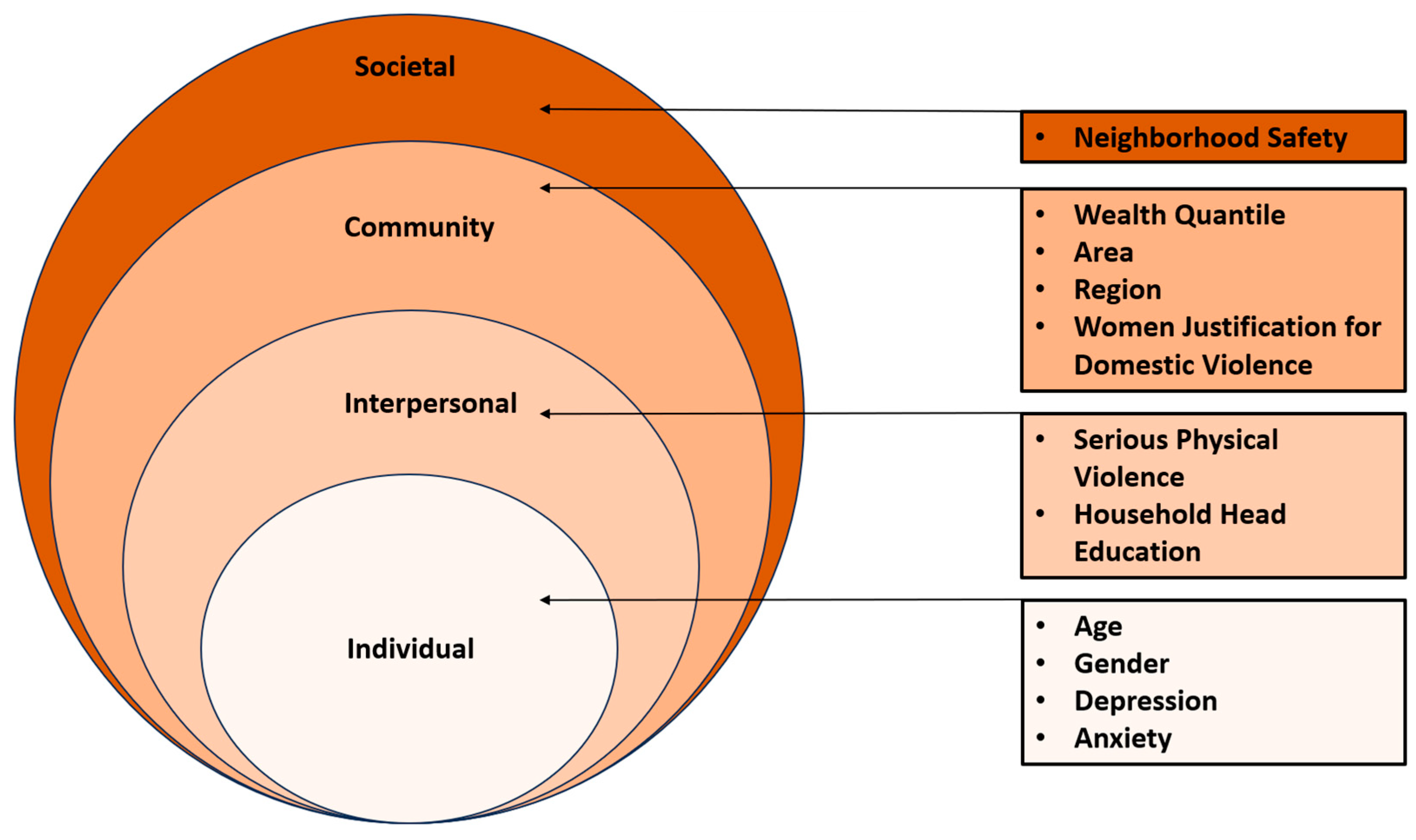
The social ecological model (SEM), initially proposed by Bronfenbrenner and Morris in 1998, serves as a theoretical lens through which to examine how individual, interpersonal, and environmental factors intersect to shape health outcomes [26]. This model outlines relations across four distinct levels: the individual, interpersonal, community, and societal levels. Within the context of children’s mental health, SEM emphasizes that adverse outcomes cannot be attributed to a single isolated factor but rather emerge from the complex relationship of factors operating at these multiple ecological levels [26].
In accordance with the SEM framework, this study delves into the role of violence across various ecological levels as determinants of adverse mental health outcomes among Iraqi children. This study builds upon prior research and applies SEM to investigate how individual, interpersonal, community, and societal factors collectively are associated with depression and anxiety among this vulnerable population [27,28]. Figure 1 shows the study variables according to SEM.
2. Materials and Methods
The objectives of this study were (1) to conduct a nationwide analysis to explore the factors associated with depression and anxiety among Iraqi children according to social ecological framework, and (2) to identify the most vulnerable children according to the spatial distribution of Iraqi governorates.
2.1. The Survey
Iraq Multiple Indicator Cluster Survey (MICS) was used in this study. MICS, an international multipurpose household survey created in the 1990s, aims to assist nations in gathering internationally comparable data on a wide range of variables pertaining to the situation of women and children. MICS measures important indicators that enable nations to produce statistics for use in national development goals, programs, and policies. The Sustainable Development Goals (SDGs) and other international commitments have been tracked using MICS recently.
With cooperation from UNICEF, the Iraqi government released the findings of the Multiple Indicator Cluster Survey (MICS 6) before the end of 2018 [29]. The country’s progress toward the SDG targets must be driven by these survey criteria. The sample method for the Iraq MICS 2018 was created to produce estimates for a wide range of indicators covering the well-being of women and children at many levels, including national, regional, and governorate-specific levels, embracing both urban and rural sectors. Estimates were prepared for the 18 governorates, namely, Dohuk, Nainawa, Sulaimaniya, Kirkuk, Erbil, Diala, Anbar, Baghdad, Babil, Karbalah, Wasit, Salahaddin, Najaf, Qadisyah, Muthana, Thiqar, Musan, and Basrah [30].
Mothers or caretakers, 12,382 in total, were specifically included in our study, and they provided detailed information about their parenting and disciplinary methods for children between the ages of 5 and 14. More specifically, mothers or caretakers of those children were asked a series of questions on the methods adults in the household used to discipline the child during the past month and if the respondent believe that physical punishment is a necessary part of child-rearing. Children between the ages of 15 and 17 were not covered by this survey section [29].
2.2. Study Variables
In this study, the outcome variables were two binary variables that were coded to measure negative mental outcomes among Iraqi children, based on the mothers or caretakers’ perception. Our first measure, depressive symptoms, is based on whether the mothers or caretakers reported that, over the past month, the child seemed very sad or depressed at least once a week (yes vs. no). Anxiety is based on whether the mothers or caretakers reported that, over the past month, the child seemed very anxious, nervous, or worried at least once a week (yes vs. no). This methodology is consistent with the approach used by Logan et al. [31].
The rest of the study variables were selected to align with the four levels of the SEM. Individual-level factors were child age (5–9, 10–14) and child sex (male, female). Interpersonal-level variables included parental discipline using serious physical violence, measured using a series of categorical dummy variables based on a hierarchy of severity logic, whereby more than one disciplinary method is reported by mothers or caretakers. Serious physical discipline includes adults in the household who reported disciplining their child by shaking the child, hitting the child with an object (e.g., a belt), hitting the child in the face, the head, or the ear, and/or beating the child as hard as possible, coded as yes vs. no. Also, interpersonal-level variables included household head education (pre-primary or none, primary, lower secondary, upper secondary and beyond).
Community-level variables were area (urban, rural), region (Kurdistan, South/Central Iraq), wealth index (poorest, second, middle, fourth, richest), and domestic violence acceptance among women. This was a binary variable with two responses (yes), indicating acceptance and (no) indicating opposition. Domestic violence acceptance among women was assessed using a set of fixed-response yes/no questions related to different circumstances, in which a husband might be perceived justified in hitting or beating his wife. These circumstances included (1) the wife going out without informing the husband, (2) neglecting the children, (3) engaging in arguments with the husband, (4) refusing to have sex with the husband, (5) burning the food, (6) the husband feeling that she is wasteful, and (7) exposing household secrets. Domestic violence acceptance among women was categorized as yes if at least one of the seven situations was endorsed with an affirmative answer and as no if none of the situations were endorsed. This categorization was introduced by other researchers [32,33].
The societal-level variable that was included in this study pertained to the perceived safety within one’s neighborhood, specifically focusing on the sense of security while walking alone in the neighborhood after nightfall. Respondents had a range of response options, including (1) feeling “very safe”, (2) “safe”, (3) “unsafe”, (4) “very unsafe”, and (7) “never do this”. In line with prior research, the safety variable responses were transformed into a binary format, as per the method established by Emerson and Llewellyn in 2023 [34]. “Very safe” and “safe” were consolidated as “safe”, while “unsafe”, “very unsafe”, and “never do this” were combined as “unsafe”.
2.3. Statistical Analysis
The first step of the analysis was carried out by conducting a descriptive analysis to estimate the prevalence of depression and anxiety among children along with the rest of the study variables. Subsequently, multivariate logistic regression models predicting children’s anxiety and depression were built adjusting for the study variables according to the four levels of SEM (see Figure 1, Table 1 and Table 2). The data compilations and analyses were conducted using IBM® SPSS® Statistics version 27. The significance level was set at p < 0.05. The adjusted odds ratios (AOR) and the 95% confidence intervals (95% CI) were reported for each independent variable (see Table 2).
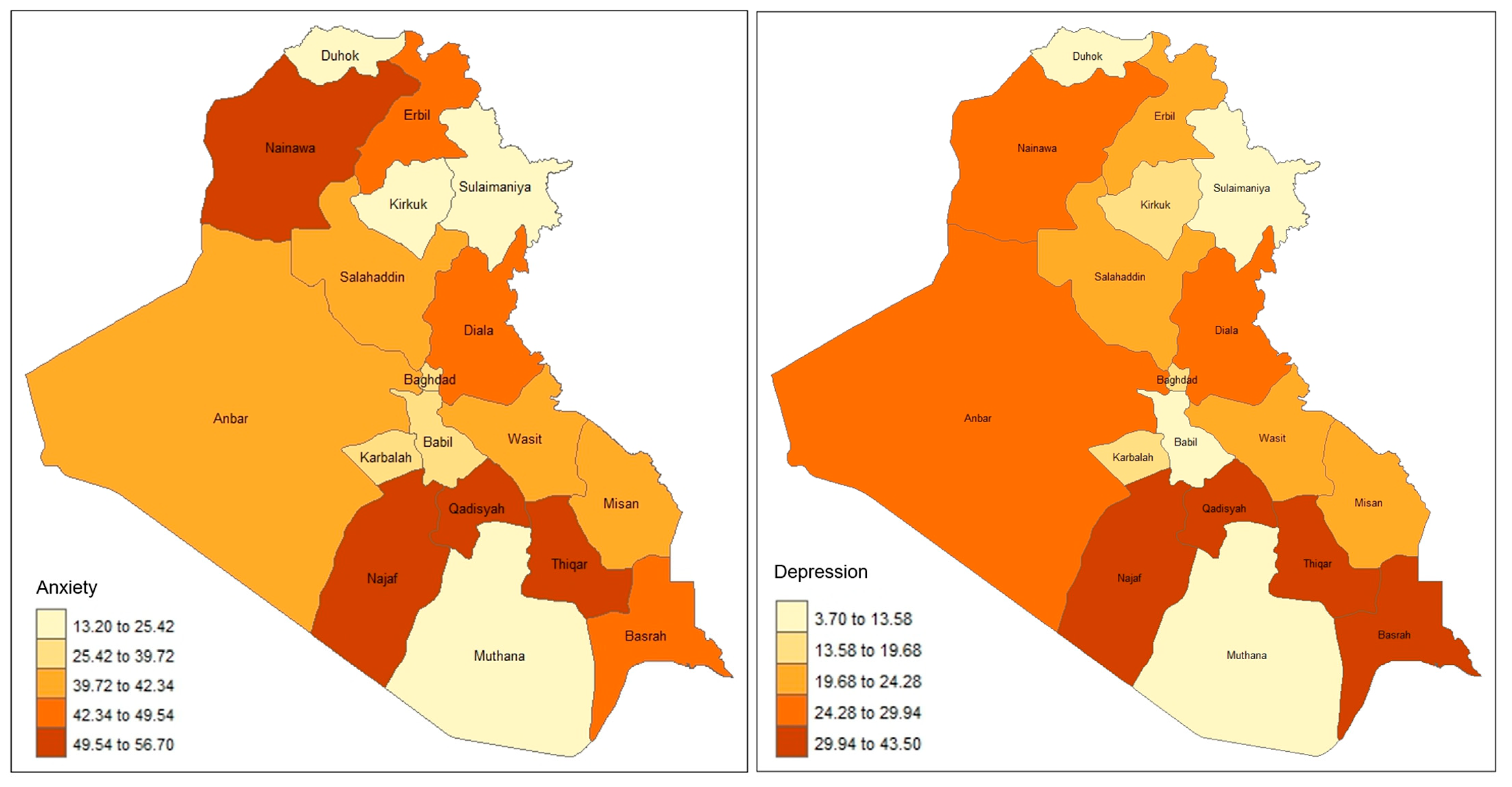
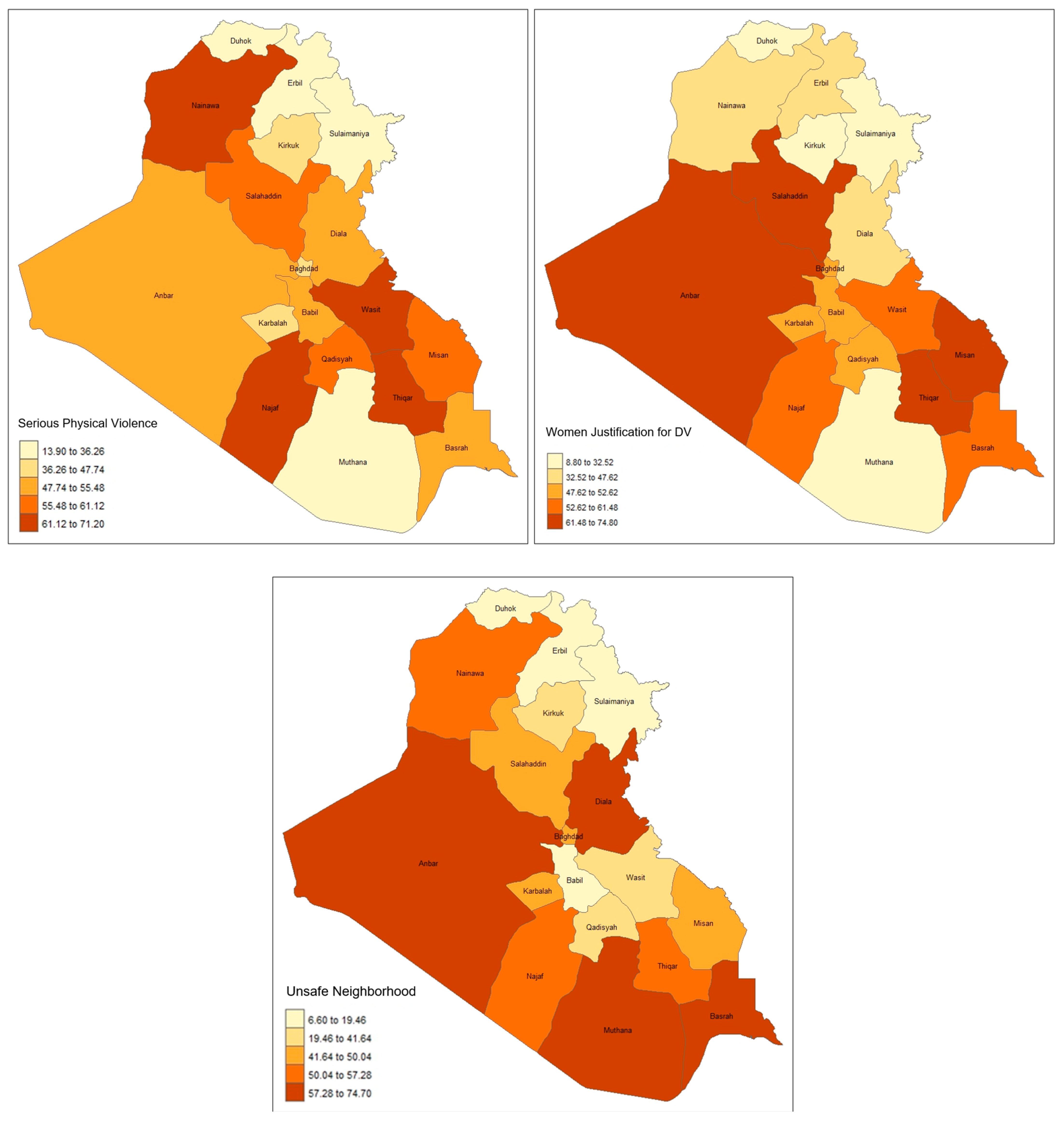
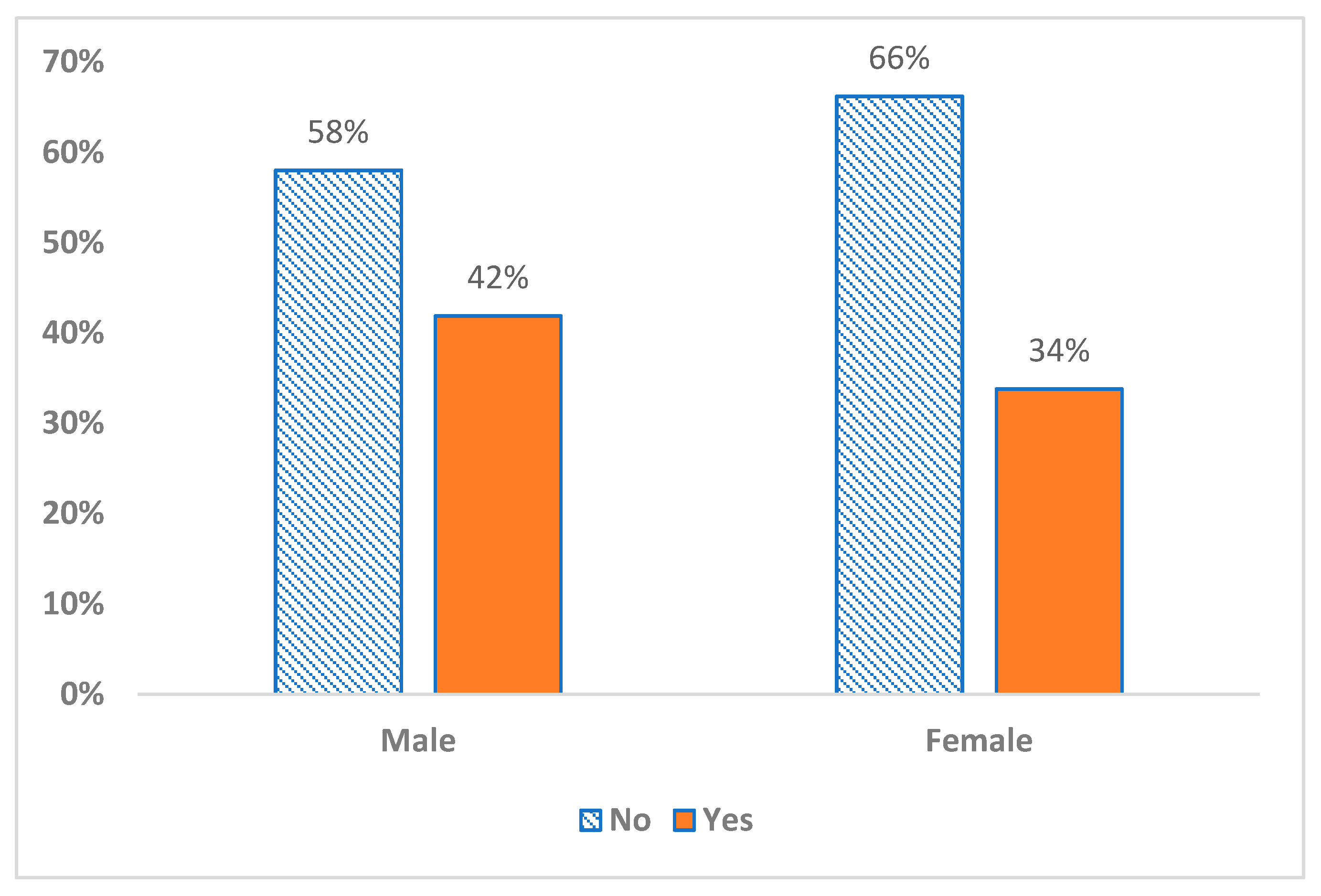
To investigate the spatial distribution of the important study variables, R software (R-4.3.2) was used to create maps showing the 18 Iraqi governorates. The mapped variables include children’s anxiety, children’s depression, children’s discipline practices using serious physical violence, domestic violence acceptance, and neighborhood safety (see Figure 2). Also, Figure A1 shows the percentage of female and male children affected by anxiety and depression.
3. Results
3.1. Descriptive Analysis
Table 1 provides an overview of the study sample’s key characteristics. Notably, 22% of the children had symptoms of depression, while 38% showed signs of anxiety. Children 5–9 years old were 57% vs. 43.3% for 10–14 children. Male children were 51.7% vs. 48.3% female children. The use of severe physical violence to discipline children by adults in the household was reported in 47.5% of cases, while 48.4% of women justified domestic violence. Additionally, 36% of household heads had primary education. The majority of mothers or caretakers resided in urban areas, making up 67% of the total sample. Regarding wealth, the poorest quintile comprised 25% of the total population studied. When it came to neighborhood safety, 44% of mothers or caretakers expressed feeling unsafe walking in their neighborhood after dark. For a more comprehensive breakdown of sociodemographic characteristics, please refer to Table 1. Also, Figure A1 in the Appendix A shows the percentage of female and male children affected by anxiety and depression to better understand the gender vulnerability.
Figure 2 illustrates the spatial distribution of key study variables across Iraq’s 18 governorates. The prevalence of children anxiety was notably higher than the national prevalence, ranging from 50% to 57%, in Najaf, Thiqar, Qadisyah, and Nainawa. Similarly, children’s depression exhibited higher prevalence, ranging from 30% to 44%, in Najaf, Thiqar, Qadisyah, and Basrah.
The governorates with the highest prevalence of reported severe physical violence (61% to 71%) were Najaf, Thiqar, Wasit, and Nainawa. On the other hand, women’s acceptance of domestic violence was more prevalent in the south/central region of Iraq, particularly in Anbar, Salahaddin, Thiqar, and Misan governorates (62–75%), but notably lower in the Kurdistan region, specifically Dohuk, Sulaimaniya, and Erbil governorates (9–33%). Regarding unsafe neighborhoods, Anbar, Diala, Muthana, and Basrah governorates showed the highest prevalence (57–75%), while Dohuk, Sulaimaniya, Erbil, and Babil governorates showed the lowest prevalence (7–20%) (refer to Figure 2 for further details).
3.2. Logistic Regression Analyses
Table 2 presents the results of two logistic regression analysis models, one for predicting children’s depression and the other for predicting children’s anxiety. These models assessed the associations between study variables according to the SEM.
In the model predicting children’s depression, individual-level variables (older age “10–14 vs. 5–9” and serious physical violence) were found to be significantly associated with children’s depression (AOR = 1.15, 95% CI: 1.06, 1.26 and AOR = 1.51, 95% CI: 1.37, 1.67), respectively. Moreover, at the interpersonal level, women’s justification for domestic violence (AOR = 1.27, 95% CI: 1.15, 1.41) demonstrated a significant association with children’s depression. Several community-level factors also showed significant associations with children’s depression, including the wealth index, mainly the middle (AOR = 0.79, 95% CI: 0.68, 0.92), fourth (AOR = 0.75, 95% CI: 0.64, 0.89), and richest (AOR = 0.59, 95% CI: 0.47–0.73) compared to the poorest quantile. Also, we observed the levels of the south/central region compared to Kurdistan (AOR = 1.91, 95% CI: 1.51, 2.38) and urban vs. rural (AOR = 0.74, 95% CI: 0.66, 0.83). Additionally, the societal-level indicator, “neighborhood safety,” was found to be significantly associated with children’s depression (AOR = 1.18, 95% CI: 1.07, 1.30). For a detailed breakdown of these results, please refer to Table 2.
In the model predicting children’s anxiety, individual-level variables (gender and serious physical violence) demonstrated associations with children’s anxiety. Furthermore, at the interpersonal level, women’s justification for domestic violence (AOR = 1.54, 95% CI: 1.06, 1.26) exhibited a significant association with children’s anxiety. Several community-level factors also showed a significant association with children’s anxiety, including the wealth index, south/central region compared to Kurdistan (AOR = 1.55, 95% CI: 1.31, 1.83) and urban vs. rural (AOR = 0.79, 95% CI: 0.72, 0.87). Notably, the societal-level indicator, “neighborhood safety,” displayed a significant association with children’s anxiety (AOR = 1.09, 95% CI: 1.00, 1.19). For a detailed breakdown of these findings, please refer to Table 2.
4. Discussion
The objectives of this study were (1) to conduct a nationwide analysis to explore how violence at multiple socio-ecological levels is associated with children’s depression and anxiety, and (2) to identify the most vulnerable children according to the spatial distribution of Iraqi governorates. The study revealed that nationwide, the prevalence of children with depression and anxiety was 22% and 38%, respectively. Yet, children living in south/central regions of Iraq showed a higher prevalence of depression and anxiety, namely Najaf, Thiqar, and Qadisyah, where the prevalence was 30–44% and 50–57%, respectively. Similar spatial patterns emerged when exploring the prevalence of violence exposure across various levels. Furthermore, the presence of violence exposure across multiple levels was significantly associated with a higher likelihood of children experiencing depression and anxiety.
Significant associations were found through the regression analyses. Particularly, exposure to interpersonal-level violence, such as using serious physical violence to raise a child, is associated with a child’s development of anxiety and depression. According to research, children who experience such harsh and aggressive disciplinary measures have a greatly increased probability of developing anxiety and depressive illnesses [35,36]. The fear, stress, and powerlessness that come with experiencing severe physical abuse can impair a child’s sense of safety and security, making it more difficult for them to build healthy relationships and deal with the difficulties of life [37]. It is crucial to highlight that Iraq currently lacks comprehensive legal safeguards to protect children from exposure to violence. Inconsistent with the principles of Sustainable Development Goal 16.2, which seeks to end all forms of violence against children, existing Iraqi legislation permits parents to discipline their children using physical punishment, as described in Article 41 (1) of the Iraqi Penal Code [23,24,38,39]. As part of Iraq’s commitment to the SDGs, it is essential to revisit and amend these legal provisions, ensuring the protection and well-being of our children.
At the community level, violence exposure like the justification of domestic violence by women showed a significant association with a child’s depression and anxiety. When women tolerate or justify domestic violence, it can create a hostile and unsafe environment for children [40]. One significant aspect that warrants further exploration is the cultural context surrounding women’s acceptance or justification of domestic violence within Iraqi society. Our study acknowledges the role of such attitudes, emphasizing how women’s tolerance or justification of domestic violence can perpetuate a hostile and unsafe environment for children. Witnessing such attitudes can have a profound impact on a child’s emotional well-being [13,41]. Moreover, communities that approve domestic violence may normalize harmful behaviors, making it more challenging for children to seek help or support. Therefore, addressing and challenging these harmful norms and attitudes are crucial to promoting the mental health and well-being of Iraqi children and breaking the cycle of violence. To comprehensively understand and address the complexities of children’s mental health in Iraq, it is essential to integrate a culturally sensitive approach that acknowledges and challenges harmful norms and attitudes surrounding domestic violence.
Significant associations between other community-level variables and children’s depression and anxiety were found. For example, living in south or central Iraq and coming from low-income families have been associated with an increased likelihood of developing childhood anxiety and depression. These factors might create a situation in which there may be limited access to mental health treatments and educational opportunities. Living in a community with poor infrastructure and economic possibilities can also make it difficult to access support networks for mental health, which can increase social isolation and the likelihood that children will experience sadness and anxiety [42,43]. It is critical to address these local inequalities if we are to improve the outcomes for Iraqi children’s mental health in these situations.
At the societal level, living in an “unsafe neighborhood” was associated with a significantly higher likelihood of depression and anxiety among children. Living in an environment characterized by violence and a lack of safety measures can have profound effects on a child’s mental health. Children in these neighborhoods often face chronic stressors, such as fear for their physical safety and limited outdoor play opportunities. These stressors can contribute to the development of symptoms associated with depression and anxiety [44]. Studies showed that community violence had direct adverse consequences for youth depression [45,46]. Recognizing that Iraq has suffered decades of political and social disorder, which has the potential to significantly impact the mental well-being of its children, it is imperative to integrate mental health awareness programs into the school curriculum [3,4,5,6,7]. These programs aim to assist Iraqi children in addressing and coping with their mental health needs, fostering the growth of a resilient and healthy generation that will shape the future of Iraq.
It is important to interpret the results of this study with certain limitations in mind. First off, due to its cross-sectional design, this study is unable to determine the causal pathways of development for depression and anxiety. When dealing with sensitive topics like violence exposure and mental health outcomes, the dependence on self-reported data collecting poses possible biases. Future studies are needed to investigate this association using longitudinal data. For instance, it might be beneficial to follow-up children until they reach 18 years of age to observe any recurring violent behaviors and maintain a strong correlation with patterns of repeated misconduct. Additionally, assessing neighborhood safety could involve evaluating threats, experiences, or instances of attempted sexual abuse. When evaluating the household head and mother, it is noteworthy to document any prior experiences they may have had during their childhood of receiving similar punitive and abusive discipline. Such information could offer significant insights into the normalization of violence within daily routines.
5. Conclusions
This study offers critical insights into the factors associated with the development of depression and anxiety among children in Iraq. By addressing the existing gaps in understanding children’s mental health outcomes at both national and governorate levels, this research highlights the urgency for actionable policy interventions. The future directions of this research could be to expand the focus and investigate the factors associated with the development of conduct disorders, cognitive deficits, or somatic symptom disorders among Iraqi children. Considering this study’s findings, we advocate for the formulation and implementation of targeted strategies aimed at assessing and treating mental illnesses in children. Furthermore, there is a need to prioritize initiatives that address family and community violence comprehensively. To achieve the key Sustainable Development Goals related to ending all forms of violence against children by 2030, we recommend specific measures, including but not limited to establishing community-based support systems, enhancing mental health service accessibility, and fostering collaborations among stakeholders at various levels. This calls for efforts from policymakers, healthcare providers, educators, and community leaders to ensure the holistic well-being and safety of children in Iraq.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study, due to the authors used secondary data analysis from a publicly available dataset for the manuscript. There is no identifying information in the dataset the authors used.
Informed Consent Statement
Patient consent was waived due to the authors used secondary data analysis from a publicly available dataset for the manuscript. There is no identifying information in the dataset the authors used.
Data Availability Statement
The data presented in this study are available on request from the United Nations Children’s Fund (UNICEF), MICS surveys: https://mics.unicef.org/surveys.
Conflicts of Interest
The author declares no conflict of interest.
Appendix A
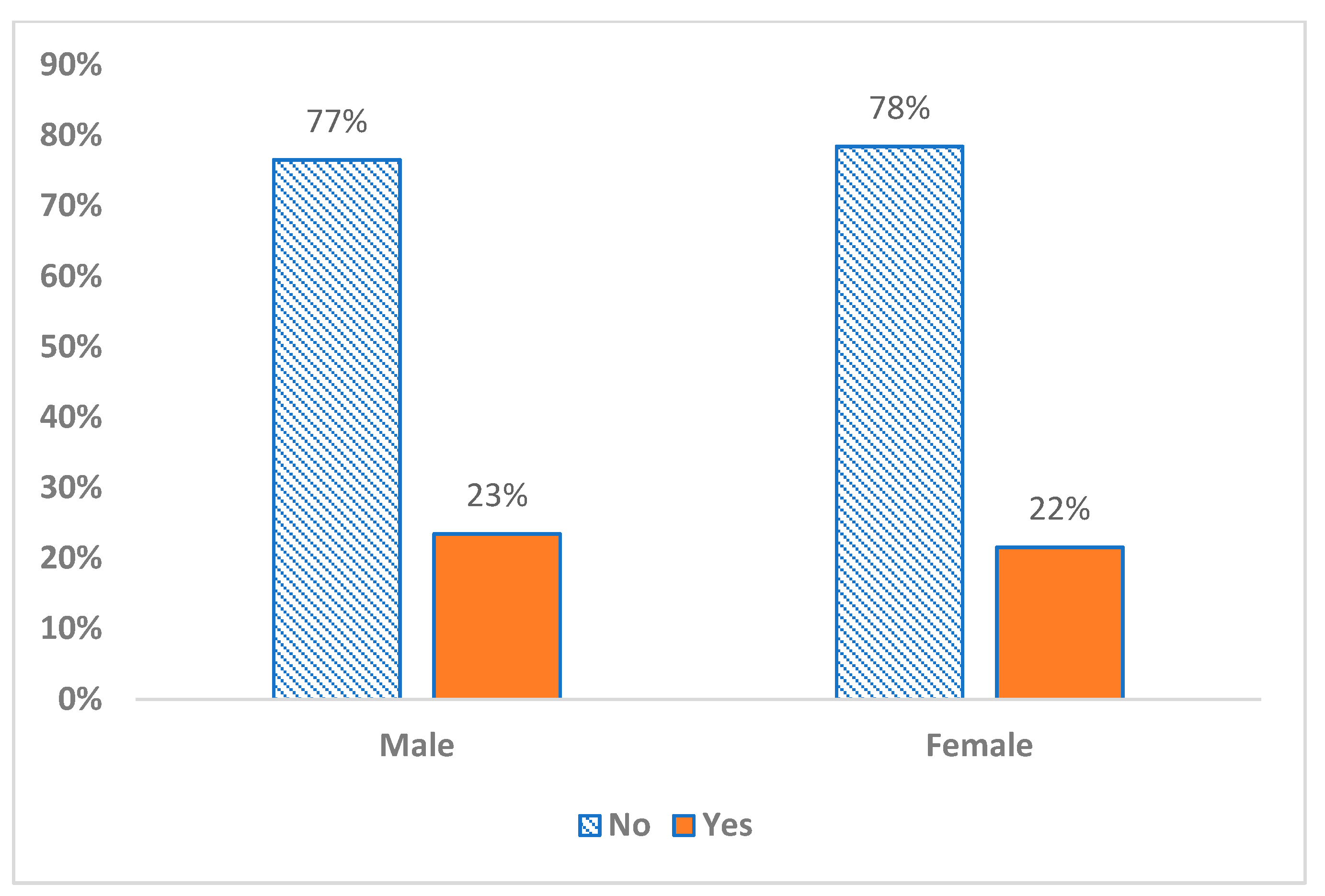
Figure A1.
The percentage of female and male subjects affected by anxiety (upper graph) and depression (lower graph).
Figure A1.
The percentage of female and male subjects affected by anxiety (upper graph) and depression (lower graph).


References
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19: A Meta-analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health of Adolescents. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health (accessed on 19 July 2023).
- Gialloreti, L.E.; Basa, F.B.; Moramarco, S.; Salih, A.O.; Alsilefanee, H.H.; Qadir, S.A.; Bezenchek, A.; Incardona, F.; Di Giovanni, D.; Khorany, R.; et al. Supporting Iraqi Kurdistan Health Authorities in Post-conflict Recovery: The Development of a Health Monitoring System. Front. Public Health 2020, 8, 7. [Google Scholar] [CrossRef]
- World Health Organization. Social Determinants of Health in Countries in Conflict: A Perspective from the Eastern Mediterranean. Available online: https://applications.emro.who.int/dsaf/dsa955.pdf (accessed on 25 July 2023).
- Murthy, R.S.; Lakshminarayana, R. Mental health consequences of war: A brief review of research findings. World Psychiatry 2006, 5, 25–30. [Google Scholar] [PubMed]
- Green, P.; Ward, T. The Transformation of Violence in Iraq. Br. J. Criminol. 2009, 49, 609–627. [Google Scholar] [CrossRef]
- Kaiser, J.; Hagan, J. Crimes of Terror, Counterterrorism, and the Unanticipated Consequences of a Militarized Incapacitation Strategy in Iraq. Soc. Forces 2018, 97, 309–346. [Google Scholar] [CrossRef]
- United Nations Children’s Fund. 2022 UNICEF Iraq’s Humanitarian Appeals. Available online: https://www.unicef.org/iraq/2022-unicef-iraqs-humanitarian-appeals (accessed on 5 September 2023).
- Corrigan, P.W.; Watson, A.C. Understanding the impact of stigma on people with mental illness. World Psychiatry 2002, 1, 16–20. [Google Scholar] [PubMed]
- Sadik, S.; Bradley, M.; Al-Hasoon, S.; Jenkins, R. Public perception of mental health in Iraq. Int. J. Ment. Health Syst. 2010, 4, 26. [Google Scholar] [CrossRef]
- Nelson, C.A.; Scott, R.D.; Bhutta, Z.A.; Harris, N.B.; Danese, A.; Samara, M. Adversity in childhood is linked to mental and physical health throughout life. BMJ 2020, 371, m3048. [Google Scholar] [CrossRef]
- United Nations. Hidden Scars: How Violence Harms the Mental Health of Children. Available online: https://violenceagainstchildren.un.org/sites/violenceagainstchildren.un.org/files/documents/publications/final_hidden_scars_lhow_violence_harms_the_mental_health_of_children.pdf (accessed on 7 September 2023).
- Moylan, C.A.; Herrenkohl, T.I.; Sousa, C.; Tajima, E.A.; Herrenkohl, R.C.; Russo, M.J. The Effects of Child Abuse and Exposure to Domestic Violence on Adolescent Internalizing and Externalizing Behavior Problems. J. Fam. Violence 2010, 25, 53–63. [Google Scholar] [CrossRef]
- Moffitt, T.E. Childhood exposure to violence and lifelong health: Clinical intervention science and stress-biology research join forces. Dev. Psychopathol. 2013, 25, 1619–1634. [Google Scholar] [CrossRef]
- Tran, T.D.; Nguyen, H.; Fisher, J. Attitudes towards Intimate Partner Violence against Women among Women and Men in 39 Low- and Middle-Income Countries. PLoS ONE 2016, 11, e0167438. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.; Garg, S. Addressing domestic violence against women: An unfinished agenda. Indian J. Community Med. 2008, 33, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Rakovec-Felser, Z. Domestic Violence and Abuse in Intimate Relationship from Public Health Perspective. Health Psychol. Res. 2014, 2, 1821. [Google Scholar] [CrossRef] [PubMed]
- Al-Atrushi, H.H.; Al-Tawil, N.G.; Shabila, N.P.; Al-Hadithi, T.S. Intimate partner violence against women in the Erbil city of the Kurdistan region, Iraq. BMC Womens Health 2013, 13, 37. [Google Scholar] [CrossRef] [PubMed]
- Wiggers, M.; Paas, F. Harsh Physical Discipline and Externalizing Behaviors in Children: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 14385. [Google Scholar] [CrossRef]
- World Health Organization. Corporal Punishment and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/corporal-punishment-and-health (accessed on 7 September 2023).
- Lansford, J.E.; Dodge, K.A. Cultural Norms for Adult Corporal Punishment of Children and Societal Rates of Endorsement and Use of Violence. Parent. Sci. Pract. 2008, 8, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Naudin, C.; Gatti, V.; Kounou, K.B.; Bagnéken, C.-O.; Ntjam, M.-C.; Clément, M.-È.; Brodard, F. Physically Violent Parental Practices: A Cross-Cultural Study in Cameroon, Switzerland, and Togo. J. Child Adolesc. Trauma 2023, 16, 959–971. [Google Scholar] [CrossRef] [PubMed]
- International Labour Organization. Database of National Labour, Social Security and Related Human Rights Legislation: Raq (232) > Criminal and Penal Law (5). Available online: https://www.ilo.org/dyn/natlex/natlex4.detail?p_lang=en&p_isn=57206&p_country=IRQ&p_count=232&p_classification=01.04&p_classcount=5 (accessed on 15 September 2023).
- Equity Now. Discriminatory Laws: Iraq—Penal Code No. 111 of 1969. Available online: https://www.equalitynow.org/discriminatory_law/iraq_-_penal_code_no_111_of_1969/#:~:text=The%20Law%3A-,Article%2041%20of%20the%20Iraqi%20Penal%20Code%20No.,while%20exercising%20a%20legal%20right (accessed on 15 September 2023).
- Rueve, M.E.; Welton, R.S. Violence and mental illness. Psychiatry 2008, 5, 34–48. [Google Scholar]
- Bronfenbrenner, U.; Morris, P.A. The ecology of developmental processes. In Handbook of Child Psychology: Theoretical Models of Human Development, 5th ed.; Damon, W., Lerner, R.M., Eds.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 1998; pp. 993–1028. [Google Scholar]
- Billings, A.G.; Moos, R.H. Comparisons of children of depressed and nondepressed parents: A social-environmental perspective. J. Abnorm. Child Psychol. 1983, 11, 463–485. [Google Scholar] [CrossRef]
- Mian, N.D.; Wainwright, L.; Briggs-Gowan, M.J.; Carter, A.S. An Ecological Risk Model for Early Childhood Anxiety: The Importance of Early Child Symptoms and Temperament. J. Abnorm. Child Psychol. 2011, 39, 501–512. [Google Scholar] [CrossRef]
- United Nations Children’s Fund. Iraq: Multiple Indicator Cluster Survey 2018. Available online: https://mics.unicef.org/files?job=W1siZiIsIjIwMTkvMDMvMDEvMTkvMjMvMTgvNTg5L0VuZ2xpc2gucGRmIl1d&sha=aea1de7cc6f6ec09 (accessed on 25 September 2023).
- United Nations Children’s Fund. Iraq: Monitoring the Situation of Children and Women: Multiple Indicator Cluster Survey 2018; United Nations Children’s Fund: New York, NY, USA, 2019. [Google Scholar]
- Logan, M.W.; Pare, P.-P.; Dulisse, B. Parental Discipline and Child Psychosocial Outcomes in Iraq and Kurdistan: Evidence From a Nationally Representative Sample. J. Interpers. Violence 2022, 37, 1223–1247. [Google Scholar] [CrossRef] [PubMed]
- Lansford, J.E.; Deater-Deckard, K.; Bornstein, M.H.; Putnick, D.L.; Bradley, R.H. Attitudes justifying domestic violence predict endorsement of corporal punishment and physical and psychological aggression towards children: A study in 25 low- and middle-income countries. J. Pediatr. 2014, 164, 1208–1213. [Google Scholar] [CrossRef] [PubMed]
- Bhowmik, J.; Biswas, R.K. Married Women’s Attitude toward Intimate Partner Violence Is Influenced by Exposure to Media: A Population-Based Spatial Study in Bangladesh. Int. J. Environ. Res. Public Health 2022, 19, 3447. [Google Scholar] [CrossRef]
- Emerson, E.; Llewellyn, G. Exposure of Women with and without Disabilities to Violence and Discrimination: Evidence from Cross-sectional National Surveys in 29 Middle- and Low-Income Countries. J. Interpers. Violence 2023, 38, 7215–7241. [Google Scholar] [CrossRef] [PubMed]
- De Bellis, M.D.; Zisk, A. The biological effects of childhood trauma. Child. Adolesc. Psychiatr. Clin. N. Am. 2014, 23, 185–222. [Google Scholar] [CrossRef] [PubMed]
- Morelli, N.M.; Hong, K.; Garcia, J.; Elzie, X.; Alvarez, A.; Villodas, M.T. Everyday Conflict in Families at Risk for Violence Exposure: Examining Unique, Bidirectional Associations with Children’s Anxious- and Withdrawn-Depressed Symptoms. Res. Child Adolesc. Psychopathol. 2023, 51, 317–330. [Google Scholar] [CrossRef] [PubMed]
- Al Odhayani, A.; Watson, W.J.; Watson, L. Behavioural consequences of child abuse. Can. Fam. Physician 2013, 59, 831–836. [Google Scholar] [PubMed]
- End Corporal Punishment. Country Report for Iraq. Available online: https://endcorporalpunishment.org/reports-on-every-state-and-territory/iraq/ (accessed on 28 September 2023).
- United Nations. Violence against Children. Available online: https://sdgs.un.org/topics/violence-against-children (accessed on 28 September 2023).
- Lloyd, M. Domestic Violence and Education: Examining the Impact of Domestic Violence on Young Children, Children, and Young People and the Potential Role of Schools. Front. Psychol. 2018, 9, 2094. [Google Scholar] [CrossRef]
- Wathen, C.N.; Macmillan, H.L. Children’s exposure to intimate partner violence: Impacts and interventions. Paediatr. Child Health 2013, 18, 419–422. [Google Scholar]
- Knifton, L.; Inglis, G. Poverty and mental health: Policy, practice and research implications. BJPsych Bull. 2020, 44, 193–196. [Google Scholar] [CrossRef]
- Brandt, L.; Liu, S.; Heim, C.; Heinz, A. The effects of social isolation stress and discrimination on mental health. Transl. Psychiatry 2022, 12, 398. [Google Scholar] [CrossRef] [PubMed]
- Coley, R.L.; Lynch, A.D.; Kull, M. Early Exposure to Environmental Chaos and Children’s Physical and Mental Health. Early Child. Res. Q. 2015, 32, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Foell, A.; Pitzer, K.A.; Nebbitt, V.; Lombe, M.; Yu, M.; Villodas, M.L.; Newransky, C. Exposure to community violence and depressive symptoms: Examining community, family, and peer effects among public housing youth. Health Place 2021, 69, 102579. [Google Scholar] [CrossRef] [PubMed]
- Preuß, M.; Nieuwenhuijsen, M.; Marquez, S.; Cirach, M.; Dadvand, P.; Triguero-Mas, M.; Gidlow, C.; Grazuleviciene, R.; Kruize, H.; Zijlema, W. Low Childhood Nature Exposure is Associated with Worse Mental Health in Adulthood. Int. J. Environ. Res. Public Health 2019, 16, 1809. [Google Scholar] [CrossRef]
Figure 1.
Study variables predicting children’s anxiety and depression according to the Social Ecological Model.
Figure 1.
Study variables predicting children’s anxiety and depression according to the Social Ecological Model.

Figure 2.
Spatial distribution of study variables according to 18 Iraqi governorates. DV = Domestic violence.
Figure 2.
Spatial distribution of study variables according to 18 Iraqi governorates. DV = Domestic violence.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Descriptive statistics (N = 12,382).
| Characteristics | N | % | ||
|---|---|---|---|---|
| Individual | Depression | No | 9670 | 78.2 |
| Yes | 2688 | 21.8 | ||
| Anxiety | No | 7655 | 61.9 | |
| Yes | 4706 | 38.1 | ||
| Child Age | 5–9 | 7009 | 56.7 | |
| 10–14 | 5352 | 43.3 | ||
| Child Sex | Male | 6391 | 51.7 | |
| Female | 5970 | 48.3 | ||
| Interpersonal | Serious Physical Violence | No | 6474 | 52.5 |
| Yes | 5857 | 47.5 | ||
| Household Head Education | Pre-primary or none | 1417 | 11.4 | |
| Primary | 4409 | 35.6 | ||
| Lower secondary | 2957 | 23.9 | ||
| Upper secondary and beyond | 3600 | 29.1 | ||
| Community | Women Justification for Domestic Violence | No | 6438 | 51.6 |
| Yes | 5943 | 48.4 | ||
| Wealth Quintile | Poorest | 3047 | 24.6 | |
| Second | 2678 | 21.6 | ||
| Middle | 2393 | 19.3 | ||
| Fourth | 2221 | 17.9 | ||
| Richest | 2006 | 16.2 | ||
| Area | Urban | 8271 | 66.8 | |
| Rural | 4111 | 33.2 | ||
| Region | Kurdistan | 1609 | 13.0 | |
| South Central | 10,772 | 87.0 | ||
| Societal | Unsafe Neighborhood | No | 6946 | 56.1 |
| Yes | 5436 | 43.9 | ||
Table 2.
Multivariate logistic regression analysis modeling depression and anxiety among Iraqi children (N = 12,382).
Table 2.
Multivariate logistic regression analysis modeling depression and anxiety among Iraqi children (N = 12,382).
| Characteristics | Depression | Anxiety | ||||
|---|---|---|---|---|---|---|
| AOR 95% CI | p Value | AOR 95% CI | p Value | |||
| Individual | Child Age, Ref = (5–9) years | |||||
| 10–14 | 1.15 (1.06–1.26) | <0.001 | 0.94 (0.88–1.01) | 0.65 | ||
| Child Sex, Ref = Male | Female | 0.92 (0.8–1.01) | 0.54 | 0.73 (0.67–0.79) | <0.001 | |
| Interpersonal | Serious Physical Violence, Ref = No | Yes | 1.51 (1.37–1.67) | <0.001 | 1.85 (1.70–2.01) | <0.001 |
| Household Head Education, Ref = Pre-primary or none | ||||||
| Primary | 1.13 (0.95–1.34) | 0.308 | 1.04 (0.90–1.21) | 0.81 | ||
| Lower secondary | 1.12 (0.93–1.34) | 0.446 | 1.12 (0.95–1.31) | 0.32 | ||
| Upper secondary and beyond | 1.19 (0.98–1.43) | 0.174 | 1.15 (0.98–1.34) | 0.18 | ||
| Community | Women Justification for Domestic Violence, Ref = No | Yes | 1.28 (1.16–1.42) | <0.001 | 1.16 (1.06–1.26) | 0.001 |
| Wealth Quintile, Ref = Poorest | ||||||
| Second | 0.89 (0.77–1.02) | 0.109 | 1.01 (0.89–1.14) | 0.87 | ||
| Middle | 0.79 (0.68–0.92) | 0.002 | 0.97 (0.85–1.11) | 0.65 | ||
| Fourth | 0.75 (0.64–0.89) | 0.001 | 0.89 (0.77–1.02) | 0.1 | ||
| Richest | 0.59 (0.47–0.73) | <0.001 | 0.72 (0.60–0.86) | <0.001 | ||
| Region, Ref = Kurdistan | South Central | 1.87 (1.49–2.34) | <0.001 | 1.53 (1.30–1.81) | <0.001 | |
| Area, Ref = Rural | Urban | 1.35 (1.49–2.34) | <0.001 | 0.80 (0.72–0.88) | <0.001 | |
| Societal | Unsafe Neighborhood, Ref = No | Yes | 1.18 (1.07–1.30) | 0.001 | 1.09 (1.00–1.19) | 0.04 |
Ref = reference level, AOR= adjusted odds ratios, 95% CI = 95% confidence intervals.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Al Juboori, R. Violence and Child Mental Health Outcomes in Iraq: Mapping Vulnerable Areas. Psychiatry Int. 2024, 5, 39-52. https://doi.org/10.3390/psychiatryint5010004
AMA Style
Al Juboori R. Violence and Child Mental Health Outcomes in Iraq: Mapping Vulnerable Areas. Psychiatry International. 2024; 5(1):39-52. https://doi.org/10.3390/psychiatryint5010004
Chicago/Turabian StyleAl Juboori, Ruaa. 2024. "Violence and Child Mental Health Outcomes in Iraq: Mapping Vulnerable Areas" Psychiatry International 5, no. 1: 39-52. https://doi.org/10.3390/psychiatryint5010004