
Mental Health Peer-Led Cafés—A Complementary Approach to Traditional Crisis Care: A Protocol for a Systematic Scoping Review

Abstract
:1. Introduction
Rationale for Systematic Scoping Review Protocol
“Out of hours crisis cafés should be piloted and should be operated based on identified good practice.”([21] p. 99)
- To examine the breadth of the literature relating to peer-led cafés within mental health service provision;
- To identify the types of peer-led services used for those experiencing a mental health crisis/emotional distress;
- To explore the advantages and challenges of peer-led cafés within mental health service provision;
- To explore the possible governance structures associated with such peer-led cafés internationally;
- To identify whether such peer-led cafés have an impact on the mental health of those who utilise them;
- To describe what is known regarding the implementation of such peer-led cafés within mental health service provision;
- To identify recommendations that can be used to support the further development of peer-led cafés in an Irish context.
2. Methods and Analysis
2.1. Stage One: Identifying the Research Question
2.2. Stage Two: Identifying Relevant Studies
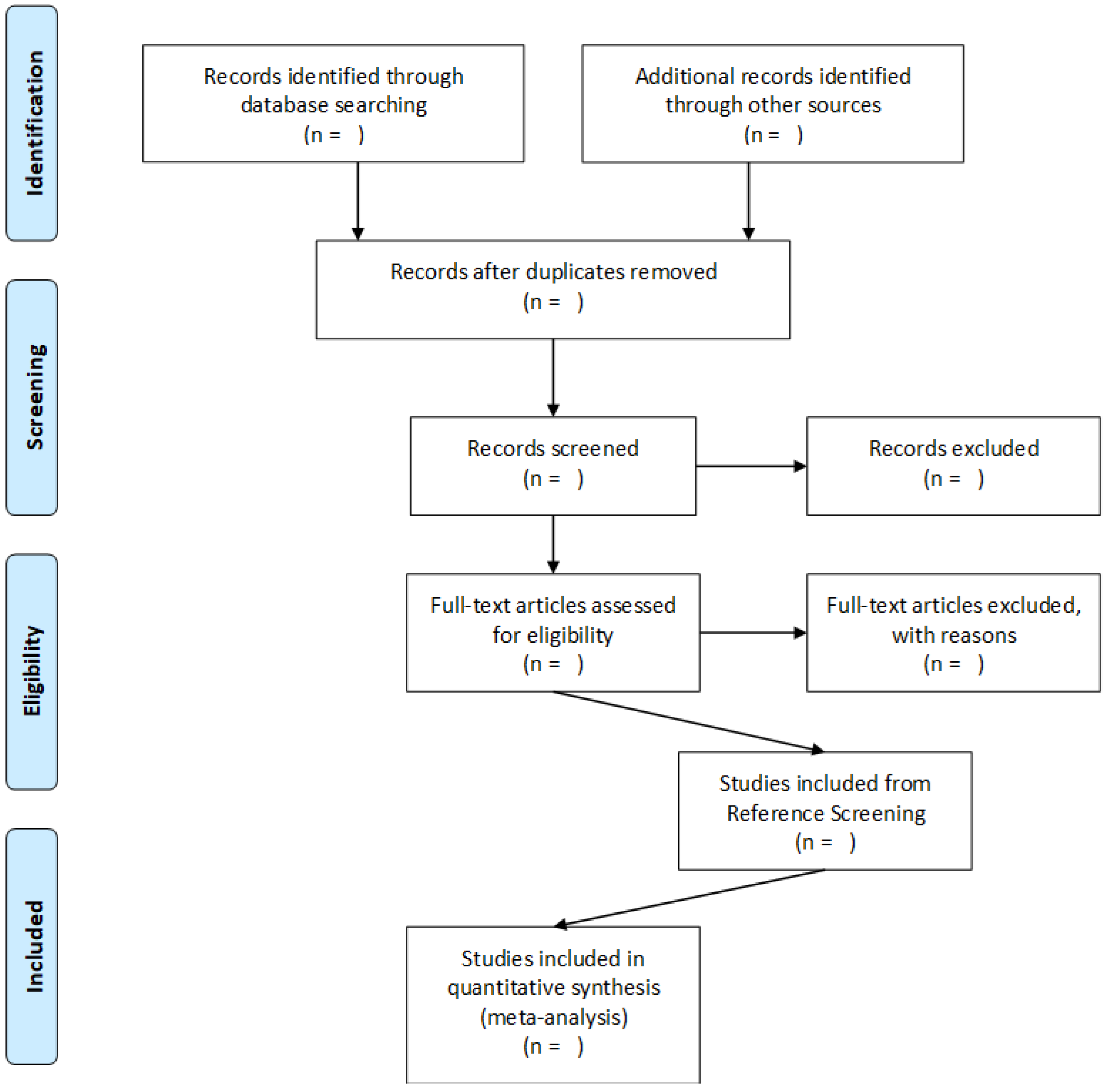
2.3. Stage Three: Study Selection
2.4. Stage Four: The Charting of the Data
- Authors, year of publication, country where the study was conducted, or the affiliation of the first author;
- Journal;
- Target audience;
- Format of the paper—dissertation, empirical, or report;
- Aim of the study;
- Study design;
- Methodological orientation—if known;
- Theoretical framework—if known;
- Method of data collection;
- Sampling;
- Type of peer-led centre;
- Advantages of peer-led centres;
- Challenges to peer-led centres;
- Mechanism of implementation of peer-led centre;
- Governance structure;
- Impact on mental health;
- Strengths and limitations of the study;
- Study recommendations.
2.5. Stage Five: The Collation, Summarisation, and Reporting of the Results
2.6. Ethics and Dissemination
3. Discussion
Strengths and Limitations
4. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Changing the Culture of Mental Health Service Delivery. Available online: https://www.mentalhealthreform.ie/news/changing-the-culture-of-mental-health-service-delivery (accessed on 27 September 2023).
- Kelly, B. Mental Health in Ireland: The Complete Guide for Patients, Families, Health Care Professionals and Everyone Who Wants to Be Well; The Liffey Press: Dublin, Ireland, 2017. [Google Scholar]
- From Vision to Action: An Analysis of the Implementation of a Vision for Change. Available online: https://www.lenus.ie/bitstream/handle/10147/112857/xFromVisiontoActionAnAnalysisoftheImplementationofAVisionforChange.pdf?sequence=3&isAllowed=y (accessed on 27 September 2023).
- Johansson, J.A.; Holmes, D. “Recovery” in mental health services, now and then: A poststructuralist examination of the despotic state machine’s effects. Nurs Inq. 2023. [CrossRef]
- Anthony, W.A. Recovery from mental illness: The guiding vision of the mental health service system in the 1990s. Psychosoc. Rehabil. J. 1993, 16, 11–23. [Google Scholar] [CrossRef]
- A Vision for Change: Report of the Expert Group on Mental Health Policy. Available online: https://www.hse.ie/eng/services/publications/mentalhealth/mental-health---a-vision-for-change.pdf (accessed on 27 September 2023).
- National Service Framework for Mental Health. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/198051/National_Service_Framework_for_Mental_Health.pdf (accessed on 20 March 2021).
- Norton, M. Implementing co-production in traditional statutory mental health services. Ment. Health Pract. 2019. [Google Scholar] [CrossRef]
- Norton, M.J. Peer support working: A question of ontology and epistemology. Int. J. Ment. Health Syst. 2023, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Peer Support Distance Working: Guidance on a Model of Peer Support Working during the COVID-19 Pandemic. Available online: https://www.researchgate.net/publication/342708755_Peer_Support_Distance_Working_Guidance_on_a_Model_of_Peer_Support_Working_during_the_Covid-19_Pandemic (accessed on 5 July 2022).
- The Early Peer Support Movement. Available online: https://cmwn.org/the-history-of-peer-support/the-early-peer-support-movement/#:~:text=Research%20suggests%20that%20peer%20support,and%20experiences%20to%20the%20public (accessed on 27 May 2023).
- Davidson, L.; Bellamy, C.; Guy, K.; Miller, R. Peer support among persons with severe mental illness: A review of evidence and experiences. World Psychiatry 2012, 11, 123–128. [Google Scholar] [CrossRef]
- Peer Support Workers: A Guidance Paper. Available online: https://www.lenus.ie/bitstream/handle/10147/576059/PeerSupportWorkersAGuidancePaper.pdf?sequence=6&isAllowed=y (accessed on 7 July 2022).
- Peer Support Workers in Mental Health Services: A Report on the Impact of Peer Support Workers in Mental Health Services. Available online: https://www.researchgate.net/publication/340716658_The_Impact_of_Peer_Support_Workers_in_Mental_Health_Services (accessed on 7 July 2022).
- National Service Plan 2022. Available online: https://www.hse.ie/eng/services/publications/serviceplans/hse-national-service-plan-2022.pdf (accessed on 7 July 2022).
- Coniglio, F.D.; Hancock, N.; Ellis, L.A. Peer support within Clubhouse: A grounded theory study. Community Ment. Health J. 2012, 48, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Biegel, D.E.; Pernice, F.; Chang, C.-W.; D’Anglo, L. Correlates of peer support in a Clubhouse setting. Community Ment. Health J. 2013, 49, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Chinman, M.; Shoai, R.; Cohen, A. Using organisational change strategies to guide peer support technicians implementation in the Veterans Administration. Psychiatr. Rehabil. J. 2010, 33, 269–277. [Google Scholar] [CrossRef]
- Kumar, A.; Azevedo, K.J.; Factor, A.; Hailu, E.; Ramirez, J.; Lindley, S.E.; Jain, S. Peer support in an outpatient program for veterans with posttraumatic stress disorder: Translating participant experiences into a recovery model. Psychol. Serv. 2019, 16, 415–424. [Google Scholar] [CrossRef]
- Development and Impact of Peer-Led Mental Health Support in the Community: A Review of Aras Follain and Gateway. Available online: https://www.researchgate.net/publication/342748517_Development_and_impact_of_peer-led_mental_health_support_in_the_community_A_review_of_Aras_Follain_and_Gateway (accessed on 7 July 2022).
- Sharing the Vision: A Mental Health Policy for Everyone. Available online: https://assets.gov.ie/76770/b142b216-f2ca-48e6-a551-79c208f1a247.pdf (accessed on 19 January 2021).
- Implementation Plan 2022–2024: Sharing the Vision—A Mental Health Policy for Everyone. Available online: https://www.hse.ie/eng/services/publications/mentalhealth/sharing-the-vision-implementation-plan-2022.pdf (accessed on 7 July 2022).
- Crisis Cafés. Available online: https://www.nhft.nhs.uk/crisis-cafe (accessed on 27 September 2023).
- Larkin, G.L.; Beautrais, A.L.; Spirito, A.; Kirrane, B.M.; Lippmann, M.J.; Milzman, D.P. Mental health and emergency medicine: A research agenda. Acad. Emerg. Med. 2009, 16, 1110–1119. [Google Scholar] [CrossRef]
- Hodgson, K. Nurse’s attitudes towards patients’ hospitalised for self-harm. Nurs. Stand. 2016, 30, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Crisis Café Kilkenny Feasibility Study. Available online: https://workhouseunion.com/wp-content/uploads/Crisis-Cafe-Kilkenny-Feasibility-Study-Online-Version.pdf (accessed on 26 March 2021).
- Croft, B.; Isvan, N. Impact of the 2nd story peer respite program on use of inpatient and emergency services. Psychiatr. Serv. 2015, 66, 632–637. [Google Scholar] [CrossRef]
- Norton, M.J. More than just a health care assistant: Peer support working within rehabilitation and recovery mental health services. Ir. J. Psychol. Med. 2022, 1–2. [Google Scholar] [CrossRef]
- Peer Support Services in Crisis Care. Available online: https://store.samhsa.gov/sites/default/files/pep22-06-04-001.pdf (accessed on 2 September 2023).
- Dalton-Locke, C.; Johnson, S.; Harju-Seppanen, J.; Lyons, N.; Rains, L.S.; Stuart, R.; Campbell, A.; Clark, J.; Clifford, A.; Courtney, L.; et al. Emerging models and trends in mental health crisis care in England: A national investigation of crisis care systems. BMC Health Serv. Res. 2021, 21, 1174. [Google Scholar] [CrossRef]
- Experiences of Wandworth Mental Health Recovery Cafés. Available online: https://www.healthwatchwandsworth.co.uk/sites/healthwatchwandsworth.co.uk/files/Final%20Report%20-%20HWW%20Recovery%20Cafe%20survey%20%28003%29.pdf (accessed on 2 September 2023).
- Strand, M.; Eng, L.S.; Gammon, D. Combining online and offline peer support groups in community mental health care settings: A qualitative study of service users’ experiences. Int. J. Ment. Health Syst. 2020, 14, 39. [Google Scholar] [CrossRef] [PubMed]
- Crisis Resolution Services: Model of Care. Available online: https://www.hse.ie/eng/services/list/4/mental-health-services/crs-moc.pdf (accessed on 27 May 2023).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Melnyk, B.M.; Fineout-Overholt, E.; Stillwell, S.B.; Williamson, K.M. The seven steps of evidence-based practice. Am. J. Nurs. 2010, 110, 51–53. [Google Scholar] [CrossRef]
- SPIDER: Mixed Methods Qualitative Research. Available online: https://researchguides.gonzaga.edu/qualitative/spider (accessed on 27 May 2023).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide; SAGE Publications Ltd.: London, UK, 2022. [Google Scholar]
- Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product from the ESRC Methods Programme. Available online: https://www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf (accessed on 18 February 2023).
- Cuskelly, K.; Norton, M.J.; Delaney, G. Examining the existing knowledge base for enablers of family recovery in mental health: A protocol for a scoping review of national and international literature. BMJ Open 2022, 12, e066484. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Population | Service users, and family members/carers |
| Intervention | Peer-led/Peer-run cafés |
| Comparison | Emergency departments |
| Outcome | Decreased mental distress, and decreased use of coercive treatment and hospitalisations |
| Inclusion | Exclusion |
|---|---|
| Peer-reviewed articles, reports, and dissertations | Any kind of literature review, discussion/editorial/periodical papers, case reports, and perspective papers |
| Quantitative, qualitative, and mixed method studies | |
| English language | Papers that are not written in the English language |
| Mental health | Addictions, physical health, and intellectual disabilities |
| General adult mental health | Child/Adolescent mental health, older adult, rehab and recovery mental health, mental health, and ID services |
| Any peer-led café | |
| Focussing on service-user-based experiences and outcomes | Examining service provider or family member perspectives of peer-led cafés |
| Focusses on structure, governance, and mechanism of action of peer-led cafés |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Norton, M.J. Mental Health Peer-Led Cafés—A Complementary Approach to Traditional Crisis Care: A Protocol for a Systematic Scoping Review. Psychiatry Int. 2023, 4, 370-379. https://doi.org/10.3390/psychiatryint4040033
Norton MJ. Mental Health Peer-Led Cafés—A Complementary Approach to Traditional Crisis Care: A Protocol for a Systematic Scoping Review. Psychiatry International. 2023; 4(4):370-379. https://doi.org/10.3390/psychiatryint4040033
Chicago/Turabian StyleNorton, Michael John. 2023. "Mental Health Peer-Led Cafés—A Complementary Approach to Traditional Crisis Care: A Protocol for a Systematic Scoping Review" Psychiatry International 4, no. 4: 370-379. https://doi.org/10.3390/psychiatryint4040033