

Development of Hindi-Translated Version of the Female Sexual Function Index for Evaluating Sexual Dysfunctions among Individuals with Anxiety, Depression, and Other Common Mental Health Conditions: Experiential Account and Preliminary Findings from India

Abstract
:1. Introduction
2. Aim and Objectives
2.1. Objectives
- To highlight the process of translation and pilot testing of the FSFI in Hindi;
- To share authors’ experience, perceived challenges, and possible way outs in developing the Hindi version of the FSFI.
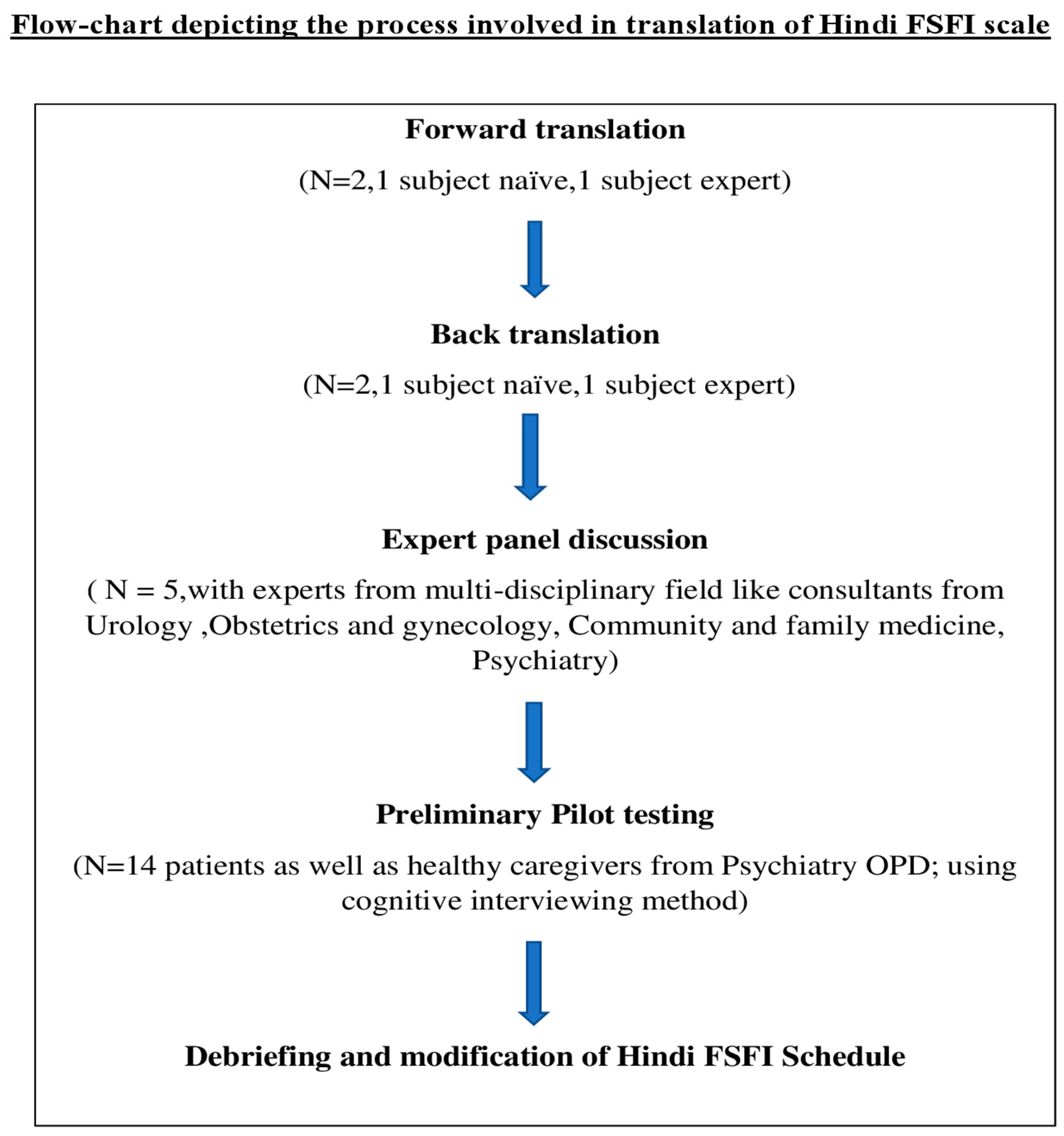
2.2. Materials and Methods
3. Results
3.1. Hindi Forward-Translation
3.2. English Back-Translation
3.3. Expert Panel Discussion on the Pre-Final Hindi Version of the FSFI
- Item 1: ‘Sambhog’ (intercourse) to replace ‘Yaun’ (sexual desire);
- Item 2: the word ‘star’ with word level in the parenthesis to be added to the pre-final Hindi version to capture the level/intensity of sexual desire (sambhog ki ichcha ka star);
- Item 5: it was suggested that ‘atmavishvas’ would be a better word than ‘ashwast’ to represent confidence in being sexually aroused;
- Item 7: to be better able to assess lubrication (wetness), ‘Geelapan’ should be preferred over ‘Cheeknai’, etc.
3.4. Preliminary Pilot Testing
3.5. Findings of the Cognitive Interview
3.6. Debriefing of the Findings of Cognitive Interviewing
- The authors discussed that the wordings of the Hindi FSFI questionnaire seem technical and complex; therefore, the general population may find it difficult to understand. Moreover, in India, we often use English words during routine conversations in Hindi to describe our experiences (excitement for uttejna, sex for Sambhog, etc.); the same pattern can be used in the questionnaire to make it more comprehensive and utilitarian. The latter will enhance the scale’s utility in research and clinics.
- The investigators agreed that the various terms or ideas being studied might appear overlapping or confusing to the participants; hence, as a part of general instruction, the following information may be added—“Participants are encouraged to refer to original definitions of various concepts or terms related to sexual functioning and as and when required they may clear their doubts from the investigator”.
- Notably, it was found that the scale lacked a definition of orgasm, which would otherwise be crucial for the participant’s understanding of this domain of sexual functioning. Hence, the same needs to be placed in the instruction section. Additionally, an alternative term for sexual excitement was adopted.
- It was also observed that the education status of the participants had a bearing on their responses to the questionnaire, with well-educated participants having a better understanding of questions and being less hesitant in responding. Therefore, this disparity needs to be addressed.
- Strikingly, it was deliberated that the responses from females who had never engaged in the penetrative sexual act relied upon sexual experiences from either sexual fantasy or self-stimulatory activities; hence, they faced difficulty understanding items that dealt with pain during the sexual act (such as Q17, 18, 19). Moreover, the relevance of the latter items for them was limited. Therefore, it was felt that the assessment of these items needs to be informed by the current sexual practices of the respondent and may be discussed separately at a later stage.
- Lastly, the opinion of an expert in sexual medicine, a knowledgeable bilingual translator, was also sought for accurate and better representative words for sexual stimulation. The expert opined that ‘yaun-uksav’ is a better word than yaun uttejna to assess sexual stimulation.
4. Discussion
4.1. Strength of the Current Procedure of FSFI-Hindi Tool Development
- Involvement of the bi-lingual translator at an early stage of the translation: We involved a bi-lingual translator early, i.e., at the stage of forward translation, who also has some understanding of female sexual functioning. The bi-lingual translator helped us identify the most suitable translation of the original FSFI. Literature suggests that the early involvement of bi-lingual translators who also know the subject matter in the scale translation improves the accuracy and robustness of the translation [15];
- A detailed description of the process of translation of FSFI: The greatest strength of the current research work lies in its procedural richness, which includes the detailed qualitative findings of various translation stages and how it informed us in refining the translated version of the FSFI. The in-depth cognitive interview process and its implications for the translated tool would notably be a valuable addition to the existing literature on this topic.
- Involving a comprehensive and representative expert panel: As the topic under study involves diverse, yet interrelated, disciplines, such as obstetricians and gynecologists, urologists, community medicine specialists, and mental health professionals, we had a representative experts panel who could provide a diverse and nuanced picture of the female sexual functioning. Research shows that the involvement of a multidisciplinary team to evaluate the translated version of the original scale is instrumental in developing a culturally valid and reliable assessment tool [15]. In addition, the multidisciplinary panel could inform us about the typical terminologies, grammar, key concepts, and culturally sensitive issues of female sexual practices and associated dysfunctions.
- Robust cognitive interview: We also performed sound cognitive interviews during the preliminary pilot testing of the developed Hindi FSFI. Data represent that researchers often do not conduct adequate pilot testing of the translated instrument; this can subsequently influence the validity and reliability of the tools [16]. Therefore, our approach was crucial in developing a robust Hindi FSFI. We involved persons with common mental disorders, with or without sexual dysfunctions, persons with severe mental illnesses, and healthy volunteers who could inform us about the validity of individual items in capturing the different domains of sexual functioning. Such an approach could widen the scope or utility of the Hindi FSFI across the populations in India.
- An iterative approach to final tool development: We followed a meticulous method to appropriately and timely update the subsequent versions (updating the item sentencing, semantics, voices, response categories, etc.) of the translated tool by considering the inputs of the key stakeholders. This approach concurs with guidelines/standards on the translation and adaptation of the original tools into a given language [15,16,21]. The latter becomes particularly critical when there is a profound stigma attached to the topic under study, and there is significant diversity among the females in reporting their sexual (dys)functioning. Moreover, such a technique is vital to consider the concepts, terminologies, and practices across the disciplines (e.g., for a female complaining of vaginismus to urologists vs. gynecologists vs. psychiatrist). Furthermore, we modified the instruction of the Hindi FSFI to make it relevant and valuable for our population. Researchers have highlighted that while developing the translated version of the original scale, the instructions of the original scale should also be looked at and handled as per the needs of the population or cultures to which it is to be applied [16,17].
4.2. Challenges Faced at Various Stages of the Development of the Hindi FSFI
- At the level of forward-translation and back-translation: Although we involved both lay translators as well as translators who were aware of the subject matter, the inherent limitation of the topic (of female sexual functioning) with much less discussion in day-to-day life, might have impacted initial Hindi forward-translation. Having a professional Hindi translator on board with some awareness about the subject could have been more helpful. In addition, although we obtained the initial two Hindi-forward translated versions vetted by a third bilingual translator, an alternative approach where the initial translators discussed their translations and came up with a consensus translation could have better informed us of the linguistic nuances of sexual functioning.
- At the level of the panel discussion: The panel meeting held was an attempt to reach researchers and clinicians who had maximal interactions on a routine basis with females presenting with sexual issues. However, despite the best efforts, there could be some shortcomings in the panels’ composition or discussions. One of the main limitations of the panel discussion was that none of the panelists was a sexual or psychosexual medicine expert or runs a dedicated sexual medicine clinic at the institute. Therefore, the opinion of the experts was personal and based on the prevalent practices of their disciplines. Hence, we might not have found the most familiar or accurate terminologies or phrases for a given sexual function domain.
- At the Level of Conducting a Cognitive Interview: While conducting the cognitive interview, we often found that participants faced or expressed stigma related to the topic being studied. Although recruitment was done after a few follow-ups when patients’ mental health problems were under control and a good working relationship between the patients and psychiatrist was established, the investigators faced difficulty building rapport with some of the participants. The participants were often concerned about the purpose of the study and confidentiality-related clauses. Such apprehension or uneasiness resulted in a high non-participation rate or hesitancy in their responses. In addition, it was often seen that participants would have difficulty understanding the differences between different subsets of questions, such as in Q12 (Over the past four weeks, when you had sexual stimulation or intercourse, how difficult was it for you to reach orgasm (climax)), most participants misunderstood the underlying theme as sexual capacity when it intended to assess the factor of orgasm (difficulty in the attainment of orgasm). Such challenges in understanding the questionnaire can be attributed to a lack of sexual knowledge, variations in the terminologies used in the Hindi language and regional dialects across Madhya Pradesh (Bundelkhandi or Bagheli), and either unawareness about the experience of orgasm or never being able to experience it. A qualitative study to identify the keywords, phrases, concepts, and ideas related to sexuality in the community could be a prudent approach to fill this gap before going for more detailed epidemiological research for tool development.
4.3. Limitations of the Current Study
4.4. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shifren, J.L.; Monz, B.U.; Russo, P.A.; Segreti, A.; Johannes, C.B. Sexual Problems and Distress in United States Women. Obstet. Gynecol. 2008, 112, 970–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briken, P.; Matthiesen, S.; Pietras, L.; Wiessner, C.; Klein, V.; Reed, G.M.; Dekker, A. Estimating the Prevalence of Sexual Dysfunction Using the New ICD-11 Guidelines. Dtsch. Arztebl. Int. 2020, 117, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Parish, W.L.; Laumann, E.O.; Pan, S.; Hao, Y. Sexual dysfunctions in urban china: A population-based national survey of men and women. J. Sex. Med. 2007, 4, 1559–1574. [Google Scholar] [CrossRef] [PubMed]
- Mishra, V.V.; Nanda, S.; Vyas, B.; Aggarwal, R.; Choudhary, S.; Saini, S.R. Prevalence of female sexual dysfunction among Indian fertile females. J. Midlife Health 2016, 7, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Shringirishi, M.; Gurnani, K.C.; Kumar, M. Female sexual dysfunction in generalized anxiety disorder. IP Indian J. Neurosci. 2020, 6, 192–196. [Google Scholar] [CrossRef]
- Roy, P.; Gupta, B.; Tripathi, A.; Nischal, A.; Dalal, P.K.; Kar, S. Sexual functioning in females with depression in remission receiving escitalopram. Indian J. Med. Res. 2019, 150, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Sathyanarayana Rao, T.S.; Darshan, M.S.; Tandon, A. An epidemiological study of sexual disorders in south Indian rural population. Indian J. Psychiatry 2015, 57, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.; Tharyan, P.; Kekre, N.; Singh, G.; Gopalakrishnan, G. Prevalence and risk factors for female sexual dysfunction in women attending a medical clinic in south India. J. Postgrad. Med. 2009, 55, 113. [Google Scholar] [CrossRef] [PubMed]
- Kingsberg, S.A.; Schaffir, J.; Faught, B.M.; Pinkerton, J.V.; Parish, S.J.; Iglesia, C.B.; Gudeman, J.; Krop, J.; Simon, J.A. Female Sexual Health: Barriers to Optimal Outcomes and a Roadmap for Improved Patient–Clinician Communications. J. Womens Health 2019, 28, 432–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, N.; Sharma, P.; Mishra, N. Female Sexual Dysfunction: Indian Perspective and Role of Indian Gynecologists. Indian J. Community Med. 2020, 45, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Keertish, N.; Sathyanarayana, M.T.; Kumar, B.G.; Singh, N.; Udagave, K. Pattern of Psychiatric Referrals in a Tertiary Care Teaching Hospital in Southern India. J. Clin. Diagn. Res. 2013, 7, 1689–1691. [Google Scholar] [CrossRef] [PubMed]
- Eisenach, N.; Zoorob, D.; Nazir, N.; Pedraza, R.; Swan, K. Translating Sexual Dysfunction: Does Language Impact Clinical Discussion of Painful Sex? Female Pelvic. Med. Reconstr. Surg. 2020, 26, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Inokuchi, T.; Watanabe, C.; Saito, T.; Kai, I. The Female Sexual Function Index (FSFI): Development of a Japanese version. J. Sex. Med. 2011, 8, 2246–2254. [Google Scholar] [CrossRef] [PubMed]
- Rehman, K.U.; Mahmood, M.A.; Sheikh, S.S.; Sultan, T.; Khan, M.A. The Female Sexual Function Index (FSFI): Translation, Validation, and Cross-Cultural Adaptation of an Urdu Version “FSFI–U”. Sex. Med. 2015, 3, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Widenfelt, B.M.; Treffers, P.D.A.; De Beurs, E.; Siebelink, B.M.; Koudijs, E. Translation and cross-cultural adaptation of assessment instruments used in psychological research with children and families. Clin. Child. Fam. Psychol. Rev. 2005, 8, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Guillemin, F.; Bombardier, C.; Beaton, D. Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. J. Clin. Epidemiol. 1993, 46, 1417–1432. [Google Scholar] [CrossRef] [PubMed]
- DuBay, M.; Watson, L.R.; Baranek, G.T.; Lee, H.; Rojevic, C.; Brinson, W.; Smith, D.; Sideris, J. Rigorous Translation and Cultural Adaptation of An Autism Screening Tool: First Years Inventory as A Case Study. J. Autism. Dev. Disord. 2021, 51, 3917–3928. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex Marital. Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef] [PubMed]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi. J. Anaesth 2017, 11, S80–S89. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Process of Translation and Adaptation of Instruments; WHO: Geneva, Switzerland, 2009; Available online: https://www.google.com/url?sa=i&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=0CAIQw7AJahcKEwjYt9GLvb3_AhUAAAAAHQAAAAAQAw&url=https%3A%2F%2Fwww.mhinnovation.net%2Fsites%2Fdefault%2Ffiles%2Ffiles%2FWHO%2520Guidelines%2520on%2520Translation%2520and%2520Adaptation%2520of%2520Instruments.docx&psig=AOvVaw375Tg94MkedcF5rscUyCkr&ust=1686650554847011 (accessed on 12 June 2023).
- van de Vijver, F.; Tanzer, N.K. Bias and equivalence in cross-cultural assessment: An overview. Eur. Rev. Appl. Psychol. 2004, 54, 119–135. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Stage of Translation | Key Aspects # | Characteristics of the Current Translation |
|---|---|---|
| Forward-translation |
|
|
| Backward-translation |
|
|
| Expert committee discussion |
|
|
| Preliminary pilot testing |
|
|
| Documentation |
|
|
| S.No | Age (Years) | Education | Residence | Diagnosis | Treatment | Side Effects |
|---|---|---|---|---|---|---|
| 1 | 20 yrs | Postgraduate | Urban | Panic disorder | Sertraline 100 mg CBT | Decreased libido |
| 2 | 35 yrs | Graduate | Urban | Healthy volunteer | ||
| 3 | 37 yrs | Graduate | Urban | Healthy volunteer | ||
| 4 | 37 yrs | Graduate | Urban | Adjustment disorder | Non-pharmacological | NA |
| 5 | 21 yrs | Pursuing graduation | Urban | Mixed Anxiety depressive illness | Desvenlafaxine 150 mg CBT | Nil |
| 6 | 32 yrs | Graduate | Urban | Anxiety disorder | Escitalopram 10 mg | nil |
| 7 | 25 yrs | Graduate | Urban | RDD with a current episode of moderate depression with PMDD | Lithium 900 mg Escitalopram 20 mg | nil |
| 8 | 33 yrs | Graduate | Urban | Anxiety disorder | Escitalopram 10 mg | nil |
| 9 | 50 yrs | Completed secondary education | Rural | RDD with GAD | Escitalopram 20 mg Propranolol | nil |
| 10 | 34 yrs | Graduate | Urban | Depressive disorder | Escitalopram 15 mg | nil |
| 11 | 32 yrs | Graduate | Urban | Healthy volunteer | ||
| 12 | 32 yrs | Graduate | Urban | Depressive disorder | Escitalopram 15 mg | nil |
| 13 | 32 yrs | Pursuing post-graduation | Urban | Cyclothymia with binge eating disorder | Oxcarbazepine 900 mg Atomoxetine | nil |
| 14 | 35 yrs | Graduate | Rural | BPAD | Lithium 900 mg | nil |
| 15 | 47 yr | Completed secondary education | Rural | Healthy volunteer | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jain, J.; Ghosh, S.; Gupta, S.; Vullanki, S.S. Development of Hindi-Translated Version of the Female Sexual Function Index for Evaluating Sexual Dysfunctions among Individuals with Anxiety, Depression, and Other Common Mental Health Conditions: Experiential Account and Preliminary Findings from India. Psychiatry Int. 2023, 4, 160-173. https://doi.org/10.3390/psychiatryint4020018
Jain J, Ghosh S, Gupta S, Vullanki SS. Development of Hindi-Translated Version of the Female Sexual Function Index for Evaluating Sexual Dysfunctions among Individuals with Anxiety, Depression, and Other Common Mental Health Conditions: Experiential Account and Preliminary Findings from India. Psychiatry International. 2023; 4(2):160-173. https://doi.org/10.3390/psychiatryint4020018
Chicago/Turabian StyleJain, Jyotsna, Sanjukta Ghosh, Snehil Gupta, and Sai Sreeja Vullanki. 2023. "Development of Hindi-Translated Version of the Female Sexual Function Index for Evaluating Sexual Dysfunctions among Individuals with Anxiety, Depression, and Other Common Mental Health Conditions: Experiential Account and Preliminary Findings from India" Psychiatry International 4, no. 2: 160-173. https://doi.org/10.3390/psychiatryint4020018