
Anxious Temperament Predicts Poor Acceptance of Self and Life in Bipolar Disorder during the COVID-19 Pandemic

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Methods
- A self-constructed questionnaire was applied to measure COVID-19 fears, using the mean index of three items:
- “How strongly do you rate your concerns and fears about the coronavirus?”
- “How strongly do you rate your fear of contracting the coronavirus?”
- “How strongly do you rate your fear of infecting others with the coronavirus?”
- A second self-constructed questionnaire assessed emotional distress due to social distancing by asking participants to rate their response to five items: “Social distancing makes me feel lonely/bored/frustrated/anxious/hopeless”. These items were intended to measure the impact of social distancing on the mental health of the participants. In addition, situational concerns were assessed by the following items:
- “I worry about my health.”
- “I worry about my relatives’ health.”
- “I fear for my job/company.”
- “I cope well with social distancing and manage to occupy myself.”
2.3. Statistical Analyses
3. Results
3.1. Sample Description
3.1.1. Differences in Resilience, COVID-19-Related Variables, and Temperament in Individuals with BD and HCs
3.1.2. Associations between Resilience and Both COVID-19-Related Variables and Temperament
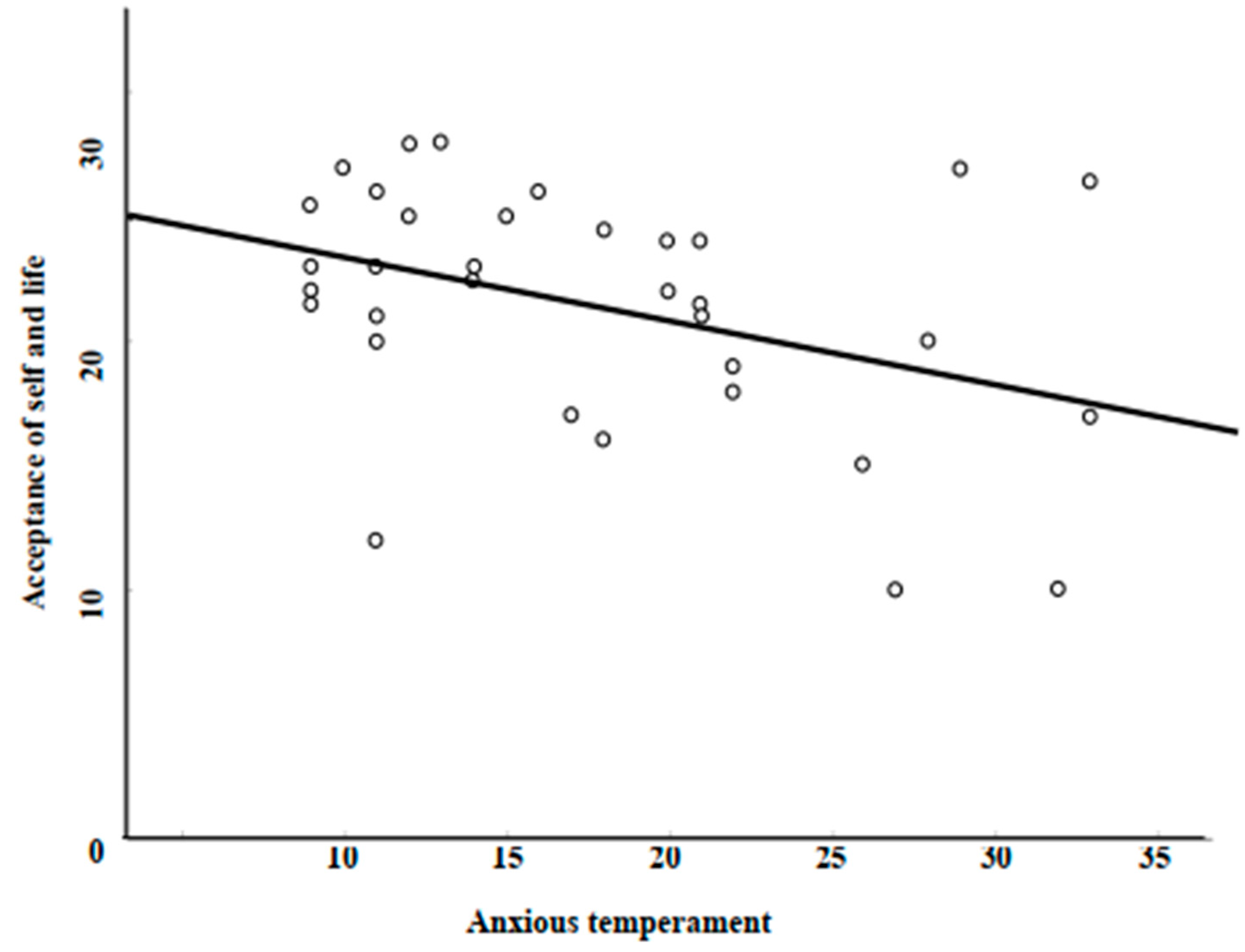
3.1.3. Predicting Resilience with Anxious Temperament
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kretchy, I.A.; Asiedu-Danso, M.; Kretchy, J.P. Medication management and adherence during the COVID-19 pandemic: Perspectives and experiences from low-and middle-income countries. Res. Soc. Adm. Pharm. 2020, 17, 2023–2026. [Google Scholar] [CrossRef]
- Adhanom, T. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 20 March 2022).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Fanaj, N.; Mustafa, S. Depression measured by PHQ-9 in Kosovo during the COVID-19 outbreak: An online survey. Psychiatr. Danub. 2021, 33, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.N.; Apostolidou, M.K.; Atsiova, M.B.; Filippidou, A.K.; Florou, A.K.; Gousiou, D.S.; Katsara, A.R.; Mantzari, S.N.; Padouva-Markoulaki, M.; Papatriantafyllou, E.I.; et al. Self-reported changes in anxiety, depression and suicidality during the COVID-19 lockdown in Greece. J. Affect. Disord. 2021, 279, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatr. 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatr. 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Maunder, R.G. Was SARS a mental health catastrophe? Gen. Hosp. Psychiatry 2009, 31, 316–317. [Google Scholar] [CrossRef]
- Bloom, N.; Fletcher, R.; Yeh, E. The impact of COVID-19 on US firms. NBER Work. Pap. 2021, 28314. [Google Scholar] [CrossRef]
- Zandifar, A.; Badrfam, R. Iranian mental health during the COVID-19 epidemic. Asian J. Psychiatry 2020, 51, 101990. [Google Scholar] [CrossRef]
- Chen, S.; Bonanno, G.A. Psychological adjustment during the global outbreak of COVID-19: A resilience perspective. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 51–54. [Google Scholar] [CrossRef]
- Zajenkowski, M.; Jonason, P.K.; Leniarska, M.; Kozakiewicz, Z. Who complies with the restrictions to reduce the spread of COVID-19?: Personality and perceptions of the COVID-19 situation. Pers. Individ. Diff. 2020, 166, 110199. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Yu, R.; Ren, J. The correlation between psychiatric disorders and COVID-19: A narrative review. Psychiatr. Danub. 2021, 33, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Lex, C.; Bäzner, E.; Meyer, T.D. Does stress play a significant role in bipolar disorder? A meta-analysis. J. Affect. Disord. 2017, 208, 298–308. [Google Scholar] [CrossRef]
- Van Rheenen, T.E.; Meyer, D.; Neill, E.; Phillipou, A.; Tan, E.J.; Toh, W.L.; Rossell, S.L. Mental health status of individuals with a mood-disorder during the COVID-19 pandemic in Australia: Initial results from the COLLATE project. J. Affect. Disord. 2020, 275, 69–77. [Google Scholar] [CrossRef]
- Asmundson, G.J.G.; Paluszek, M.M.; Landry, C.A.; Rachor, G.S.; McKay, D.; Taylor, S. Do pre-existing anxiety-related mood-disorders differentially impact COVID-19 stress responses and coping? J. Anxiety Disord. 2020, 74, 102271. [Google Scholar] [CrossRef] [PubMed]
- Dalkner, N.; Wagner-Skacel, J.; Ratzenhofer, M.; Fellendorf, F.; Lenger, M.; Maget, A.; Tmava-Berisha, A.; Pilz, R.; Queissner, R.; Hamm, C.; et al. Psychological symptoms during and after Austrian first lockdown in individuals with bipolar disorder? A follow-up control-group investigation. Int. J. Bipolar Disord. 2021, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Winkler, P.; Formanek, T.; Mlada, K.; Kagstrom, A.; Mohrova, Z.; Mohr, P.; Csemy, L. Increase in prevalence of current mental disorders in the context of COVID-19: Analysis of repeated nationwide cross-sectional surveys. Epidemiol. Psychiatr. Sci. 2020, 29, e173. [Google Scholar] [CrossRef]
- Yocum, A.K.; Zhai, Y.; McInnis, M.G.; Han, P. COVID-19 pandemic and lockdown impacts: A description in a longitudinal study of bipolar disorder. J. Affect. Disord. 2021, 282, 1226–1233. [Google Scholar] [CrossRef]
- Costa, M.; Pavlo, A.; Reis, G.; Ponte, K.; Davidson, L. COVID-19 Concerns among Persons with mental illness. Psychiatr. Serv. 2020, 71, 1188–1190. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental health and the COVID-19 pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Herrman, H.; Stewart, D.E.; Diaz-Granados, N.; Berger, E.L.; Jackson, B.; Yuen, T. What is resilience? Can. J. Psychiatry. 2011, 56, 258–265. [Google Scholar] [CrossRef] [Green Version]
- Palmiter, D.; Alvord, M.; Dorlen, R.; Comas-Diaz, L.; Luthar, S.S.; Maddi, S.R.; O’Neill, H.K.; Saakvitne, K.W.; Tedeschi, R.G. Building Your Resilience. American Association of Psychology 2012. Available online: https://www.apa.org/topics/resilience/building-your-resilience (accessed on 28 March 2022).
- Werner, E.E.; Bierman, J.M.; French, F.E. The Children of Kauai: A Longitudinal Study from the Prenatal Period to Age Ten; University of Hawaii Press: Honolulu, HI, USA, 1971. [Google Scholar]
- Petersen, L.; Lange, D.; Theocharidou, M. Who cares what it means? Practical reasons for using the word resilience with critical infrastructure operators. Reliab. Eng. Syst. Saf. 2020, 199, 06872. [Google Scholar] [CrossRef]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the resilience scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Leppert, K.; Koch, B.; Brähler, E.; Strauss, B. Die Resilienzskala (RS)—Überprüfung der Langform RS-25 und einer Kurzform RS-13. Klin. Diagn. Eval. 2008, 1, 226–243. [Google Scholar]
- Gong, Y.; Shi, J.; Ding, H.; Zhang, M.; Kang, C.; Wang, K.; Yu, Y.; Wei, J.; Wang, S.; Shao, N.; et al. Personality traits and depressive symptoms: The moderating and mediating effects of resilience in Chinese adolescents. J. Affect. Disord. 2020, 265, 611–617. [Google Scholar] [CrossRef]
- Poole, J.C.; Pusch, D.; Dobson, K.S. Childhood adversity and adult depression: The protective role of psychological resilience. Child Abus. Negl. 2017, 64, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Cohn, M.A.; Fredrickson, B.L.; Brown, S.L.; Mikels, J.A.; Conway, A.M. Happiness unpacked: Positive emotions increase life satisfaction by building resilience. Emotion 2009, 9, 361–368. [Google Scholar] [CrossRef]
- Choi, J.-W.; Cha, B.; Jang, J.; Park, C.-S.; Kim, B.-J.; Lee, C.-S.; Lee, S.-J. Resilience and impulsivity in euthymic patients with bipolar disorder. J. Affect. Disord. 2015, 170, 172–177. [Google Scholar] [CrossRef]
- Şenormancı, G.; Güçlü, O.; Özben, İ.; Karakaya, F.N.; Şenormancı, Ö. Resilience and insight in euthymic patients with bipolar disorder. J. Affect. Disord. 2020, 266, 402–412. [Google Scholar] [CrossRef]
- Uygun, E.; Cebeci, R.B.; Özsoy, E.; Başar, Ş.; Erim, B.R.; Erkoç, N.S. Investigation of the relationship between perceived social support and psychological resilience in bipolar disorder: A cross-sectional study. Anadolu Psikiyatr. Derg. 2020, 21, 37–44. [Google Scholar] [CrossRef]
- Bozikas, V.P.; Parlapani, E.; Ntouros, E.; Bargiota, S.I.; Floros, G.; Nazlidou, E.I.; Garyfallos, G. Resilience predicts social functioning in clinically stable patients with bipolar disorder. J. Nerv. Ment. Dis. 2018, 206, 567–574. [Google Scholar] [CrossRef]
- Wundt, W. Grundzüge der Physiologischen Psychologie, 5th ed.; Wilhelm Engelmann: Leipzig, Germany, 1903. [Google Scholar]
- Akiskal, H.S.; Brieger, P.; Mundt, C.; Angst, J.; Marneros, A. Temperament und affektive Störungen. In Universitätskolloquien zur Schizophrenie; Brieger, P., Ed.; Springer-Verlag: Berlin, Germany, 2002; pp. 293–299. [Google Scholar]
- Kraepelin, E. Psychiatrie: Ein Lehrbuch für Studierende und Ärzte; Barth: Leipzig, Germany, 1913. [Google Scholar]
- Matsumoto, S.; Akiyama, T.; Tsuda, H.; Miyake, Y.; Kawamura, Y.; Noda, T.; Akiskal, K.K.; Akiskal, H.S. Reliability and validity of TEMPS-A in a Japanese non-clinical population: Application to unipolar and bipolar depressives. J. Affect. Disord. 2005, 85, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, G.H.; Kahn, C.; Schiavo, C.E.; Goldchluk, A.; Herbst, L.; Piccione, M.; Saidman, N.; Ruggeri, H.; Silva, A.; Leal, J. Bipolar disorders and affective temperaments: A national family study testing the “endophenotype” and “subaffective” theses using the TEMPS-A Buenos Aires. J. Affect. Disord. 2008, 108, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Wittchen, H.U.; Wunderlich, U.; Gruschwitz, S.; Zaudig, M. SCID: Clinical Interview for DSM-IV (German Version); Verlag für Psychologie: Göttingen, Germany, 1997. [Google Scholar]
- Nussmayr, K. 15 Grafiken, die die Verbreitung des Coronavirus in Österreich und der Welt erklären. 2020. Available online: https://www.diepresse.com/5785804/15-grafiken-die-die-verbreitung-des-coronavirus-in-osterreich-und-der-welt-erklaren (accessed on 21 March 2022).
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry. 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kühner, C.; Bürger, C.; Keller, F.; Hautzinger, M. Reliability and validity of the Revised Beck Depression Inventory (BDI-II). Results from German samples. Nervenarzt 2007, 78, 651–656. [Google Scholar] [CrossRef]
- Altman, E.G.; Hedeker, D.; Peterson, J.L.; Davis, J.M. The Altman self-rating mania scale. Biol. Psychiatry 1997, 42, 948–955. [Google Scholar] [CrossRef]
- Blöink, R.; Brieger, P.; Akiskal, H.S.; Marneros, A. Factorial structure and internal consistency of the German TEMPS-A scale: Validation against the NEO-FFI questionnaire. J. Affect. Disord. 2005, 85, 77–83. [Google Scholar] [CrossRef]
- Cloninger, R.C. Temperament and Personality. Curr. Opin. Neurobiol. 1994, 4, 266–273. [Google Scholar] [CrossRef]
- Satici, S.A. Psychological vulnerability, resilience, and subjective well-being: The mediating role of hope. Pers. Individ. Differ. 2016, 102, 68–73. [Google Scholar] [CrossRef]
- Echezarraga, A.; Calvete, E.; González-Pinto, A.M.; Las Hayas, C. Resilience dimensions and mental health outcomes in bipolar disorder in a follow-up study. Stress Health 2018, 34, 115–126. [Google Scholar] [CrossRef]
- Killgore, W.D.S.; Taylor, E.C.; Cloonan, S.A.; Dailey, N.S. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 2020, 291, 113216. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, T.; Janssen, B.; Schrader, S.; Geerling, G. Depressive symptoms, resilience, and personality traits in dry eye disease. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Kaloeti, D.V.S.; Rahmandani, A.; Sakti, H.; Salma, S.; Suparno, S.; Hanafi, S. Effect of childhood adversity experiences, psychological distress, and resilience on depressive symptoms among Indonesian university students. Int. J. Adolesc. Youth 2019, 24, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Taylor, H.O.; Taylor, R.J.; Nguyen, A.W.; Chatters, L. Social isolation, depression, and psychological distress among older adults. J. Aging Health 2018, 30, 229–246. [Google Scholar] [CrossRef]
- Kesebir, S.; Yosmaoğlu, A. QEEG—spectral power density of brain regions in predicting risk, resistance and resilience for bipolar disorder: A comparison of first degree relatives and unrelated healthy subjects. Heliyon 2020, 6, e04100. [Google Scholar] [CrossRef]
- Moccia, L.; Janiri, D.; Pepe, M.; Dattoli, L.; Molinaro, M.; De Martin, V.; Chieffo, D.; Janiri, L.; Fiorillo, A.; Sani, G.; et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: An early report on the Italian general population. Brain Behav. Immun. 2020, 87, 75–79. [Google Scholar] [CrossRef]
- Wang, J.; Lloyd-Evans, B.; Giacco, D.; Forsyth, R.; Nebo, C.; Mann, F.; Johnson, S. Social isolation in mental health: A conceptual and methodological review. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 1451–1461. [Google Scholar] [CrossRef] [Green Version]
- Stefana, A.; Youngstrom, E.A.; Jun, C.; Hinshaw, S.; Maxwell, V.; Michalak, E.; Vieta, E. The COVID-19 pandemic is a crisis and opportunity for bipolar disorder. Bipolar Disord. 2020, 22, 641–643. [Google Scholar] [CrossRef]
- Hofer, A.; Mizuno, Y.; Wartelsteiner, F.; Fleischhacker, W.W.; Frajo-Apor, B.; Kemmler, G.; Mimura, M.; Pardeller, S.; Sondermann, C.; Suzuki, T.; et al. Quality of life in schizophrenia and bipolar disorder: The impact of symptomatic remission and resilience. Eur. Psychiatry 2017, 46, 42–47. [Google Scholar] [CrossRef]
- Leys, C.; Arnal, C.; Wollast, R.; Rolin, H.; Kotsou, I.; Fossion, P. Perspectives on resilience: Personality Trait or Skill? Eur. J. Trauma Dissociation 2020, 4, 100074. [Google Scholar] [CrossRef]
- Chmitorz, A.; Kunzler, A.; Helmreich, I.; Tüscher, O.; Kalisch, R.; Kubiak, T.; Wessa, M.; Lieb, K. Intervention studies to foster resilience—A systematic review and proposal for a resilience framework in future intervention studies. Clin. Psychol. Rev. 2018, 59, 78–100. [Google Scholar] [CrossRef] [PubMed]
- Bolos, A. Considerations on assisted resilience and individualized therapy in bipolar affective disorder, with a clinical case exemplification. Clujul Med. 2015, 88, 462–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marano, G.; Traversi, G.; Gesualdi, A.; Biffi, A.; Gaetani, E.; Sani, G.; Mazza, M. Mental health and coaching challenges facing the COVID-19 outbreak. Psychiatr. Danub. 2021, 33, 124–126. [Google Scholar] [PubMed]
- Hart Abney, B.G.; Lusk, P.; Hovermale, R.; Melnyk, B.M. Decreasing depression and anxiety in college youth using the Creating Opportunities for Personal Empowerment Program (COPE). J. Am. Psychiatr. Nurses Assoc. 2019, 25, 89–98. [Google Scholar] [CrossRef]


{kind=link}
| Group | |||||
|---|---|---|---|---|---|
| BD (n = 36) M (±SD) | HC (n = 39) M (±SD) | Statistics | p | η2 | |
| Age | 50.18 (13.06) | 34.09 (11.64) | U = 258.00 | 0.000 ** | |
| Sex (n) | χ2 = 8.25 | 0.004 ** | |||
| Male | 21 (58.3%) | 10 (25.6%) | |||
| Female | 15 (41.7%) | 29 (74.4%) | |||
| Education (n) | χ2 = 22.36 | <0.001 ** | |||
| Secondary school | 1 (2.8%) | 1 (2.6%) | |||
| High school | 5 (13.9%) | 6 (15.4%) | |||
| Apprenticeship | 13 (36.1%) | 0 (0.0%) | |||
| College | 7 (19.4%) | 4 (10.3%) | |||
| Bachelor’s degree | 7 (19.4%) | 19 (48.7%) | |||
| Master’s degree | 3 (8.3%) | 9 (23.1%) | |||
| Diagnosis | |||||
| BD 1 | 22 (61.1%) | ||||
| BD 2 | 14 (38.9%) | ||||
| Resilience | 69.31 (11.52) | 76.96 (9.76) | F = 6.71 | 0.012 * | 0.09 |
| “Acceptance of self and life” | 21.13 (4.84) | 23.01 (3.82) | F = 4.35 | 0.024 * | 0.06 |
| “Personal competence” | 48.18 (7.71) | 53.95 (6.55) | F = 6.80 | 0.011 * | 0.09 |
| BDI-II | 8.25 (7.81) | 4.06 (3.47) | U = 539.00 | 0.083 | |
| ASRM | 2.15 (3.02) | 0.49 (0.88) | U = 452.00 | 0.004 ** | |
| COVID-19 fears a | 3.31 (2.34) | 3.80 (1.88) | t = −1.02 | 0.311 | |
| Emotional distress due to social distancing b | 1.33 (0.84) | 1.15 (0.75) | t = 0.96 | 0.340 | |
| Situational concerns c | 1.65 (.93) | 1.51 (.67) | t = 0.73 | 0.467 | |
| TEMPS-A | |||||
| Depressive | 17.97 (7.84) | 10.72 (3.39) | F = 18.23 | <0.001 ** | 0.20 |
| Cyclothymic | 18.61 (5.98) | 9.97 (3.62) | F = 46.51 | <0.001 ** | 0.40 |
| Hyperthymic | 21.75 (5.72) | 22.21 (5.38) | F = 1.01 | 0.319 | 0.01 |
| Irritable | 16.28 (6.58) | 13.44 (5.26) | F = 4.55 | 0.036 * | 0.06 |
| Anxious | 18.14 (7.31) | 13.95 (5.61) | F = 7.80 | 0.007 ** | 0.10 |
| Resilience | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | “Acceptance of Self and Life” | “Personal Competence” | RS-13 Sum Score | |||||||||
| BD (n = 38) | HC (n = 36) | BD (n = 38) | HC (n = 36) | BD (n = 38) | HC (n = 36) | |||||||
| r | p | r | p | r | p | r | p | r | p | r | p | |
| COVID-19 fears a | −0.18 | 0.290 | −0.30 | 0.066 | −0.07 | 0.691 | −0.28 | 0.084 | −0.12 | 0.485 | −0.31 | 0.059 |
| Emotional distress due to social distancing b | −0.36 * | 0.033 | −0.30 | 0.064 | −0.28 | 0.106 | −0.44 ** | 0.005 | −0.33 | 0.050 | −0.42 * | 0.009 |
| Situational concerns c | −0.25 | 0.156 | −0.24 | 0.156 | −0.23 | 0.180 | −0.28 | 0.091 | −0.26 | 0.137 | −0.28 | 0.090 |
| BDI-II | −0.67 ** | <0.001 | −0.51 **d | 0.001 | −0.65 ** | <0.001 | −0.61 **d | <0.001 | −0.72 ** | <0.001 | −0.61 **d | <0.001 |
| TEMPS-A | ||||||||||||
| Depressive | −0.20 | 0.253 | −0.36 * | 0.029 | −0.10 | 0.571 | −0.13 | 0.449 | −0.15 | 0.397 | −0.23 | 0.175 |
| Cyclothymic | −0.24 | 0.166 | −0.41 * | 0.011 | 0.03 | 0.845 | −0.31 | 0.062 | −0.07 | 0.673 | −0.37 * | 0.024 |
| Hyperthymic | 0.08 | 0.649 | 0.31 d | 0.057 | 0.27 | 0.121 | 0.29 d | 0.070 | 0.21 | 0.219 | 0.32 *d | 0.045 |
| Irritable | −0.145 | 0.407 | −0.02 | 0.891 | −0.11 | 0.547 | −0.20 | 0.240 | −0.13 | 0.457 | −0.14 | 0.402 |
| Anxious | −0.35 * | 0.039 | −0.37 * | 0.024 | −0.15 | 0.380 | −0.23 | 0.165 | −0.25 | 0.154 | −0.30 | 0.069 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fleischmann, E.; Fellendorf, F.T.; Ortner, J.; Bengesser, S.A.; Ratzenhofer, M.; Pilz, R.; Lenger, M.; Birner, A.; Queissner, R.; Platzer, M.; et al. Anxious Temperament Predicts Poor Acceptance of Self and Life in Bipolar Disorder during the COVID-19 Pandemic. Psychiatry Int. 2022, 3, 236-247. https://doi.org/10.3390/psychiatryint3030019
Fleischmann E, Fellendorf FT, Ortner J, Bengesser SA, Ratzenhofer M, Pilz R, Lenger M, Birner A, Queissner R, Platzer M, et al. Anxious Temperament Predicts Poor Acceptance of Self and Life in Bipolar Disorder during the COVID-19 Pandemic. Psychiatry International. 2022; 3(3):236-247. https://doi.org/10.3390/psychiatryint3030019
Chicago/Turabian StyleFleischmann, Eva, Frederike T. Fellendorf, Jennifer Ortner, Susanne A. Bengesser, Michaela Ratzenhofer, René Pilz, Melanie Lenger, Armin Birner, Robert Queissner, Martina Platzer, and et al. 2022. "Anxious Temperament Predicts Poor Acceptance of Self and Life in Bipolar Disorder during the COVID-19 Pandemic" Psychiatry International 3, no. 3: 236-247. https://doi.org/10.3390/psychiatryint3030019