Resmetirom: Finally, the Light at the End of the NASH Tunnel?


Internal Medicine, Ospedale Civile di Baggiovara, Azienda Ospedaliero-Universitaria di Modena, 41126 Modena, Italy
Livers 2024, 4(1), 138-141; https://doi.org/10.3390/livers4010010
Submission received: 12 February 2024
/
Accepted: 18 February 2024
/
Published: 26 February 2024
{kind=link}
1. Introduction
Nonalcoholic steatohepatitis (NASH) is a double composite word that was first coined in 1980 by Ludwig and Colleagues [1]. These authors reported on a series of 20 individuals, predominantly women, who were moderately obese, often had type 2 diabetes and gallstones, and sought hepatological consultation owing to enlarged livers and mildly raised liver tests. Liver biopsy findings of these subjects exhibited fatty changes, lobular hepatitis, focal necrosis, inflammatory infiltrates (with mononuclear cells and/or neutrophils), and, in most instances, Mallory bodies; liver fibrosis was identified in most cases, and three patients had histological evidence consistent with liver cirrhosis. Ludwig and Colleagues concluded by stating that “currently, we know of no effective therapy” [1].
The absence of any effective management option, other than lifestyle changes, has lasted for forty-four years since the seminal paper by Ludwig and Colleagues was published [1], and innumerable NASH clinical trials have yielded disappointing results [2,3]. However, recently, Harrison et al. [4], based on an analysis conducted in approximately one thousand individuals, published a breakthrough article announcing that, irrespective of the oral dose used (i.e., 80 mg or 100 mg daily), resmetirom was better than placebo regarding the outcomes of resolved NASH (in 25.9 to 29.9% of individuals treated with resmetirom vs. 9.7% of those assigned to placebo) and improved liver fibrosis by ≥1 stage without any worsening of the NAFLD activity score (NAS), which is assessed by summing up scores of steatosis (0–3), lobular inflammation (0–3), and hepatocyte ballooning (0–2) [5] (in 24.2 to 25.9% of patients receiving resmetirom compared to 14.2% of those receiving placebo).
Interestingly, resmetirom also improved atherogenic dyslipidemia while exerting neutral effects on body weight, insulin resistance, and glycemia. Similarly, the drug affected neither the cardiovasculature (i.e., heart rate and blood pressure) nor the endocrine system, and the profile of undesired effects, which occurred more often with resmetirom than with placebo, comprised often transient, mild, gastrointestinal complaints (nausea, vomiting, and diarrhea) [4].
Given that resmetirom is a selective agonist of thyroid hormone receptor (THR) beta [6], the logical question is this: what has NASH to do with the thyroid? To answer this question, the histological features and pathogenic determinants of NASH need to be pinpointed first.
2. What Has NASH to Do with Thyroid?
Over time, what we now call “NASH” has been identified with different names, including “diabetic hepatitis”, “metabolic steatohepatitis”, “metabolic syndrome steatohepatitis”, and “metabolic dysfunction-associated steatohepatitis” (MASH) [7,8,9]. These names are clear evidence for the strong association of NASH with dysmetabolism. Histologically, the criteria used to diagnose NASH include, further to the presence of steatosis, mild-grade, sterile inflammation owing to metabolic dysfunction (i.e., “metaflammation”), injured hepatocytes (i.e., ballooning and Mallory bodies), and variable stages of fibrosis classified from F0 (absent) to F1–F2 (mild) to F3–F4 (advanced) [8,10].
Among the innumerable reasons explaining the failures of NASH trials before the advent of resmetirom, there is the scarcely appreciated notion that NASH is invariably accompanied by a complex picture of systemic metabolic dysfunction [11]. For example, each of the individual elementary components of NASH histology invariably recognizes metabolic determinants [12], strongly supporting the notion that, being a systemic condition owing to general metabolic dysfunction, NASH therefore requests a multidisciplinary and holistic approach [3].
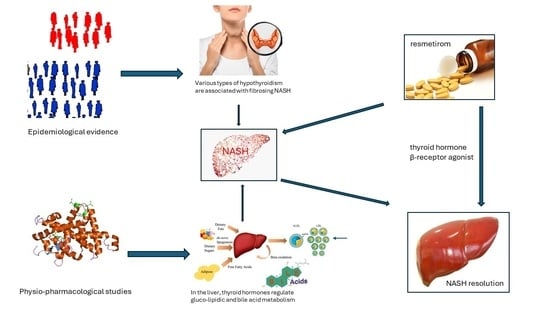
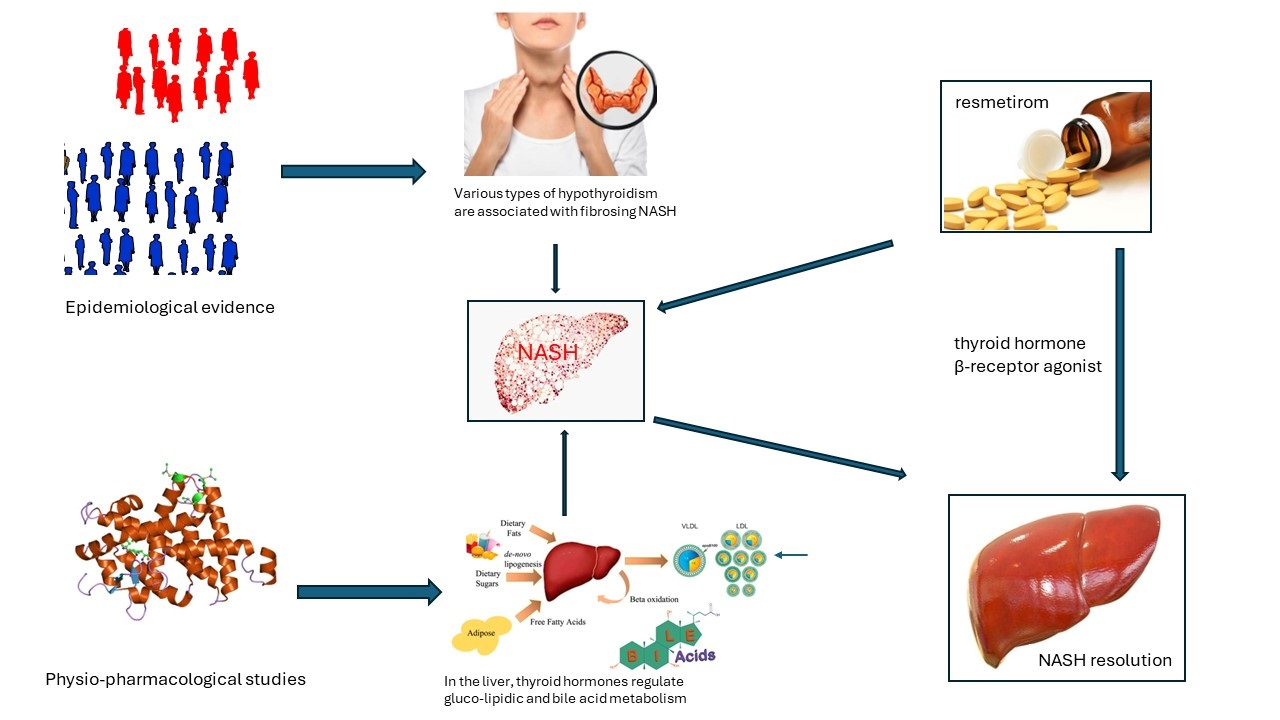
Pioneering studies highlighting the interconnections among endocrine derangements and the development of nonalcoholic fatty liver disease (NAFLD) and its progression to NASH [13,14] have laid the foundations for clearly differentiating “hypothyroidism-induced NAFLD” from other “primary” NAFLD forms [15,16]. This notion has universally been accepted by subsequent studies [17,18]. In parallel, strong epidemiological evidence has indicated that hypothyroidism is also tightly associated with the development and fibrotic progression of NAFLD and NASH [19,20,21,22]. This association has recently been found to be sex-specific and mediated by adipokines/mitokines [23].
Understanding the relationship between NASH and thyroid function in healthy states is critical for conceptualizing how hypothyroidism perturbs this relation [24,25]. In the liver, thyroid hormones (THs) regulate energy and metabolic homeostasis by modulating the export of lipids from the hepatocyte into the bile and the blood stream, as well as their oxidation and de novo lipogenesis [26]. Moreover, THs also control hepatic insulin sensitivity, suppress hepatic gluconeogenesis [26], and are involved in bile acid metabolism [27]. Among the various signals implicated in the cross-talks between the thyroid and the liver [high thyroid-stimulating hormone (TSH) levels, low TH levels, and chronic inflammation], it is the role of the THR that is deemed to be essential in the pathogenesis of hypothyroidism-induced NAFLD [6,26].
Their beneficial cardiometabolic effects (such as lowering LDL cholesterol, or reducing whole-body adiposity and body weight) explain why agonists of THRs (hence “thyromimetics”) were among the first anti-obesity agents [28]. However, this approach leads to undesired and ominous effects on the heart (e.g., tachycardia and sudden death) and musculo-skeletal system, prompting the research of safe thyromimetics that leverage the existence and different body distribution of THR isoforms: alpha and beta, which are found in the heart and liver, respectively [28].
Moreover, the use of non-selective agonists of THRs to treat NASH has raised concerns regarding the risks of accruing hepatic lipogenesis because of increased lipolysis in the adipose tissue; these concerns have prompted pioneering studies utilizing liver-targeted agonists of THR [29].
3. Safety and Efficacy of Resmetirom
On the grounds of the physio-pharmacological premises summarized above, investigators have developed an orally-active, small-molecule, liver-selective THR agonist—resmetirom (MGL-3196)—which has been shown to improve quality of life in patients through a reduced intrahepatic fat content (measured non-invasively with the magnetic-resonance-imaging-derived proton density fat fraction); moreover, it also reduces liver enzyme levels, improves non-invasive markers of liver fibrogenesis, and decreases liver stiffness, while eliciting a favorable cardiometabolic profile by reducing LDL cholesterol [30,31]. Preliminarily, investigators reported on the good safety and tolerability profile of resmetirom by showing that treatment-emergent adverse events (TEAEs) occurred in 86.5–86.1% of individuals receiving 100 mg resmetirom and in 88.4% of those assigned to 80 mg resmetirom versus 81.8% of those under placebo [31]. TEAEs occurring more often under resmetirom than placebo comprised mild gastrointestinal complaints (e.g., diarrhea and nausea) when treatment was initiated. Confronted with these adverse effects, there were beneficial effects versus placebo in terms of LDL reduction (−11.1%, −12.6%), decreased apolipoprotein B (−15.6%, −18.0%), triglycerides (−15.4%, −20.4%), 16-week hepatic fat (−34.9%, −38.6%) (p < 0.0001) and liver stiffness (−1.02, −1.70), and 52-week hepatic fat (−28.8, −33.9) with resmetirom at 80 mg and 100 mg, respectively [31].
4. Conclusions and Research Agenda
Over a 44-year period, investigators have progressed from a state of global uncertainty, if not frank impotence, regarding the pharmacological treatment of NASH to developing an innovative thyromimetic drug—resmetirom. Notable steps along this scientific journey have included pioneering recognition that systemic administration of iodothyronines curtailed body weight gain and resulted in reductions in triglyceridemia, cholesterolemia, and hepatic steatosis in high-fat-diet-fed rats [32] However, these compounds could not enter the clinical arena owing to their unacceptable cardiovascular effects. To avoid these effects, hepato-specific thyromimetics have been modeled, including resmetirom, which has proven effective in fibrosing NASH.
Future, independent studies should be conducted in the post-marketing phase to document any unprecedented side effects while ascertaining whether, as expected, reduced liver fibrosis will eventually result in a reduced risk of liver-related (e.g., cirrhosis, liver failure, hepatocellular carcinoma) and other extra-hepatic (e.g., cardio-metabolic) outcomes. Additionally, investigators should be encouraged to consider combination therapies, as predicted many years ago [33], and to perform sex-specific analyses of data [34].
In conclusion, the robustness of biological rationale, and findings in experimental and human studies concur in supporting the notion that resemetirom represents a breakthrough in drug treatment of NASH with fibrosis [35,36]. In this case, it seems unlikely that the light at the end of the tunnel is just the light of an oncoming train. Rather, the advent of resmetirom documents the successful multidisciplinary approach to complex medical topics achieved by integrating epidemiological evidence with pathophysiological and physio-pharmacological studies.
Funding
This research received no external funding.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Ludwig, J.; Viggiano, T.R.; McGill, D.B.; Oh, B.J. Nonalcoholic steatohepatitis: Mayo Clinic experiences with a hitherto unnamed disease. Mayo Clin. Proc. 1980, 55, 434–438. [Google Scholar]
- Ratziu, V.; Friedman, S.L. Why Do So Many Nonalcoholic Steatohepatitis Trials Fail? Gastroenterology 2023, 165, 5–10. [Google Scholar] [CrossRef]
- Tilg, H.; Byrne, C.D.; Targher, G. NASH drug treatment development: Challenges and lessons. Lancet Gastroenterol. Hepatol. 2023, 8, 943–954. [Google Scholar] [CrossRef]
- Harrison, S.A.; Bedossa, P.; Guy, C.D.; Schattenberg, J.M.; Loomba, R.; Taub, R.; Labriola, D.; Moussa, S.E.; Neff, G.W.; Rinella, M.E.; et al. A Phase 3, Randomized, Controlled Trial of Resmetirom in NASH with Liver Fibrosis. N. Engl. J. Med. 2024, 390, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Juluri, R.; Vuppalanchi, R.; Olson, J.; Unalp, A.; Van Natta, M.L.; Cummings, O.W.; Tonascia, J.; Chalasani, N. Generalizability of the nonalcoholic steatohepatitis Clinical Research Network histologic scoring system for nonalcoholic fatty liver disease. J. Clin. Gastroenterol. 2011, 45, 55–58. [Google Scholar] [CrossRef]
- Karim, G.; Bansal, M.B. Resmetirom: An Orally Administered, Smallmolecule, Liver-directed, β-selective THR Agonist for the Treatment of Non-alcoholic Fatty Liver Disease and Non-alcoholic Steatohepatitis. touchREV Endocrinol. 2023, 19, 60–70. [Google Scholar] [CrossRef]
- Lonardo, A.; Leoni, S.; Alswat, K.A.; Fouad, Y. History of Nonalcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2020, 21, 5888. [Google Scholar] [CrossRef] [PubMed]
- Neuschwander-Tetri, B.A.; Caldwell, S.H. Nonalcoholic steatohepatitis: Summary of an AASLD Single Topic Conference. Hepatology 2003, 37, 1202–1219. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J. Hepatol. 2023, 79, 1542–1556. [Google Scholar] [CrossRef]
- Scheen, A.J.; Luyckx, F.H.; Esser, N.; Lamproye, A.; Delwaide, J.; Paquot, N. Stéatohépatite non alcoolique (NASH): Un modèle d’inflammation métabolique («métaflammation») [Non-alcoholic steatohepatitis (NASH): A model of metabolic inflammation («metaflammation»)]. Rev. Med. Liege 2022, 77, 316–322. (In French) [Google Scholar]
- Lonardo, A.; Ballestri, S.; Mantovani, A.; Targher, G.; Bril, F. Endpoints in NASH Clinical Trials: Are We Blind in One Eye? Metabolites 2024, 14, 40. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Nascimbeni, F.; Romagnoli, D.; Lonardo, A. The independent predictors of non-alcoholic steatohepatitis and its individual histological features.: Insulin resistance, serum uric acid, metabolic syndrome, alanine aminotransferase and serum total cholesterol are a clue to pathogenesis and candidate targets for treatment. Hepatol. Res. 2016, 46, 1074–1087. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Carani, C.; Carulli, N.; Loria, P. ‘Endocrine NAFLD’ a hormonocentric perspective of nonalcoholic fatty liver disease pathogenesis. J. Hepatol. 2006, 44, 1196–1207. [Google Scholar] [CrossRef] [PubMed]
- Loria, P.; Carulli, L.; Bertolotti, M.; Lonardo, A. Endocrine and liver interaction: The role of endocrine pathways in NASH. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 236–247. [Google Scholar] [CrossRef]
- Ferrandino, G.; Kaspari, R.R.; Spadaro, O.; Reyna-Neyra, A.; Perry, R.J.; Cardone, R.; Kibbey, R.G.; Shulman, G.I.; Dixit, V.D.; Carrasco, N. Pathogenesis of hypothyroidism-induced NAFLD is driven by intra- and extrahepatic mechanisms. Proc. Natl. Acad. Sci. USA 2017, 114, E9172–E9180. [Google Scholar] [CrossRef]
- Lonardo, A.; Ballestri, S.; Mantovani, A.; Nascimbeni, F.; Lugari, S.; Targher, G. Pathogenesis of hypothyroidism-induced NAFLD: Evidence for a distinct disease entity? Dig. Liver Dis. 2019, 51, 462–470. [Google Scholar] [CrossRef]
- Liebe, R.; Esposito, I.; Bock, H.H.; Vom Dahl, S.; Stindt, J.; Baumann, U.; Luedde, T.; Keitel, V. Diagnosis and management of secondary causes of steatohepatitis. J. Hepatol. 2021, 74, 1455–1471. [Google Scholar] [CrossRef]
- Hutchison, A.L.; Tavaglione, F.; Romeo, S.; Charlton, M. Endocrine aspects of metabolic dysfunction-associated steatotic liver disease (MASLD): Beyond insulin resistance. J. Hepatol. 2023, 79, 1524–1541. [Google Scholar] [CrossRef]
- Mantovani, A.; Nascimbeni, F.; Lonardo, A.; Zoppini, G.; Bonora, E.; Mantzoros, C.S.; Targher, G. Association Between Primary Hypothyroidism and Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Thyroid 2018, 28, 1270–1284. [Google Scholar] [CrossRef]
- Guo, Z.; Li, M.; Han, B.; Qi, X. Association of non-alcoholic fatty liver disease with thyroid function: A systematic review and meta-analysis. Dig. Liver Dis. 2018, 50, 1153–1162. [Google Scholar] [CrossRef]
- Kim, D.; Kim, W.; Joo, S.K.; Bae, J.M.; Kim, J.H.; Ahmed, A. Subclinical Hypothyroidism and Low-Normal Thyroid Function Are Associated with Nonalcoholic Steatohepatitis and Fibrosis. Clin. Gastroenterol. Hepatol. 2018, 16, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Rahadini, A.A.D.; Rahadina, A. Association between hypothyroidism and liver fibrosis risk: A systematic review and meta-analysis. Clin. Exp. Hepatol. 2022, 8, 188–194. [Google Scholar] [CrossRef]
- Kouvari, M.; Valenzuela-Vallejo, L.; Axarloglou, E.; Verrastro, O.; Papatheodoridis, G.; Mingrone, G.; George, J.; Mantzoros, C.S. Thyroid function, adipokines and mitokines in metabolic dysfunction-associated steatohepatitis: A multi-centre biopsy-based observational study. Liver Int. 2024. epub ahead of print. [Google Scholar] [CrossRef]
- Seifert, J.; Chen, Y.; Schöning, W.; Mai, K.; Tacke, F.; Spranger, J.; Köhrle, J.; Wirth, E.K. Hepatic Energy Metabolism under the Local Control of the Thyroid Hormone System. Int. J. Mol. Sci. 2023, 24, 4861. [Google Scholar] [CrossRef]
- Marino, L.; Kim, A.; Ni, B.; Celi, F.S. Thyroid hormone action and liver disease, a complex interplay. Hepatology 2023. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Cevallos, P.; Murúa-Beltrán Gall, S.; Uribe, M.; Chávez-Tapia, N.C. Understanding the Relationship between Nonalcoholic Fatty Liver Disease and Thyroid Disease. Int. J. Mol. Sci. 2023, 24, 14605. [Google Scholar] [CrossRef] [PubMed]
- Wirth, E.K.; Puengel, T.; Spranger, J.; Tacke, F. Thyroid hormones as a disease modifier and therapeutic target in nonalcoholic steatohepatitis. Expert Rev. Endocrinol. Metab. 2022, 17, 425–434. [Google Scholar] [CrossRef]
- Arrese, M. Burning hepatic fat: Therapeutic potential for liver-specific thyromimetics in the treatment of nonalcoholic fatty liver disease. Hepatology 2009, 49, 348–351. [Google Scholar] [CrossRef]
- Cable, E.E.; Finn, P.D.; Stebbins, J.W.; Hou, J.; Ito, B.R.; van Poelje, P.D.; Linemeyer, D.L.; Erion, M.D. Reduction of hepatic steatosis in rats and mice after treatment with a liver-targeted thyroid hormone receptor agonist. Hepatology 2009, 49, 407–417. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Stepanova, M.; Taub, R.A.; Barbone, J.M.; Harrison, S.A. Hepatic Fat Reduction Due to Resmetirom in Patients With Nonalcoholic Steatohepatitis Is Associated With Improvement of Quality of Life. Clin. Gastroenterol. Hepatol. 2022, 20, 1354–1361.e7. [Google Scholar] [CrossRef]
- Harrison, S.A.; Taub, R.; Neff, G.W.; Lucas, K.J.; Labriola, D.; Moussa, S.E.; Alkhouri, N.; Bashir, M.R. Resmetirom for nonalcoholic fatty liver disease: A randomized, double-blind, placebo-controlled phase 3 trial. Nat Med. 2023, 29, 2919–2928. [Google Scholar] [CrossRef]
- Vergani, L. Lipid lowering effects of iodothyronines: In vivo and in vitro studies on rat liver. World J. Hepatol. 2014, 6, 169–177. [Google Scholar] [CrossRef]
- Corey, K.E.; Chalasani, N. Should combination therapy be the paradigm for future nonalcoholic steatohepatitis clinical trials? Hepatology 2011, 54, 1503–1505. [Google Scholar] [CrossRef]
- Burra, P.; Zanetto, A.; Germani, G. Sex bias in clinical trials in gastroenterology and hepatology. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 413–414. [Google Scholar] [CrossRef] [PubMed]
- Targher, G. Editorial: Resmetirom—A promising treatment option for NASH and liver fibrosis. Aliment Pharmacol. Ther. 2024, 59, 128–129. [Google Scholar] [CrossRef] [PubMed]
- Cusi, K. Selective Agonists of Thyroid Hormone Receptor Beta for the Treatment of NASH. N. Engl. J. Med. 2024, 390, 559–561. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lonardo, A. Resmetirom: Finally, the Light at the End of the NASH Tunnel? Livers 2024, 4, 138-141. https://doi.org/10.3390/livers4010010
AMA Style
Lonardo A. Resmetirom: Finally, the Light at the End of the NASH Tunnel? Livers. 2024; 4(1):138-141. https://doi.org/10.3390/livers4010010
Chicago/Turabian StyleLonardo, Amedeo. 2024. "Resmetirom: Finally, the Light at the End of the NASH Tunnel?" Livers 4, no. 1: 138-141. https://doi.org/10.3390/livers4010010