


Rapid Ovarian Reserve Decline in a Woman with Pericentric Inv(9) Variant

Abstract
:1. Introduction
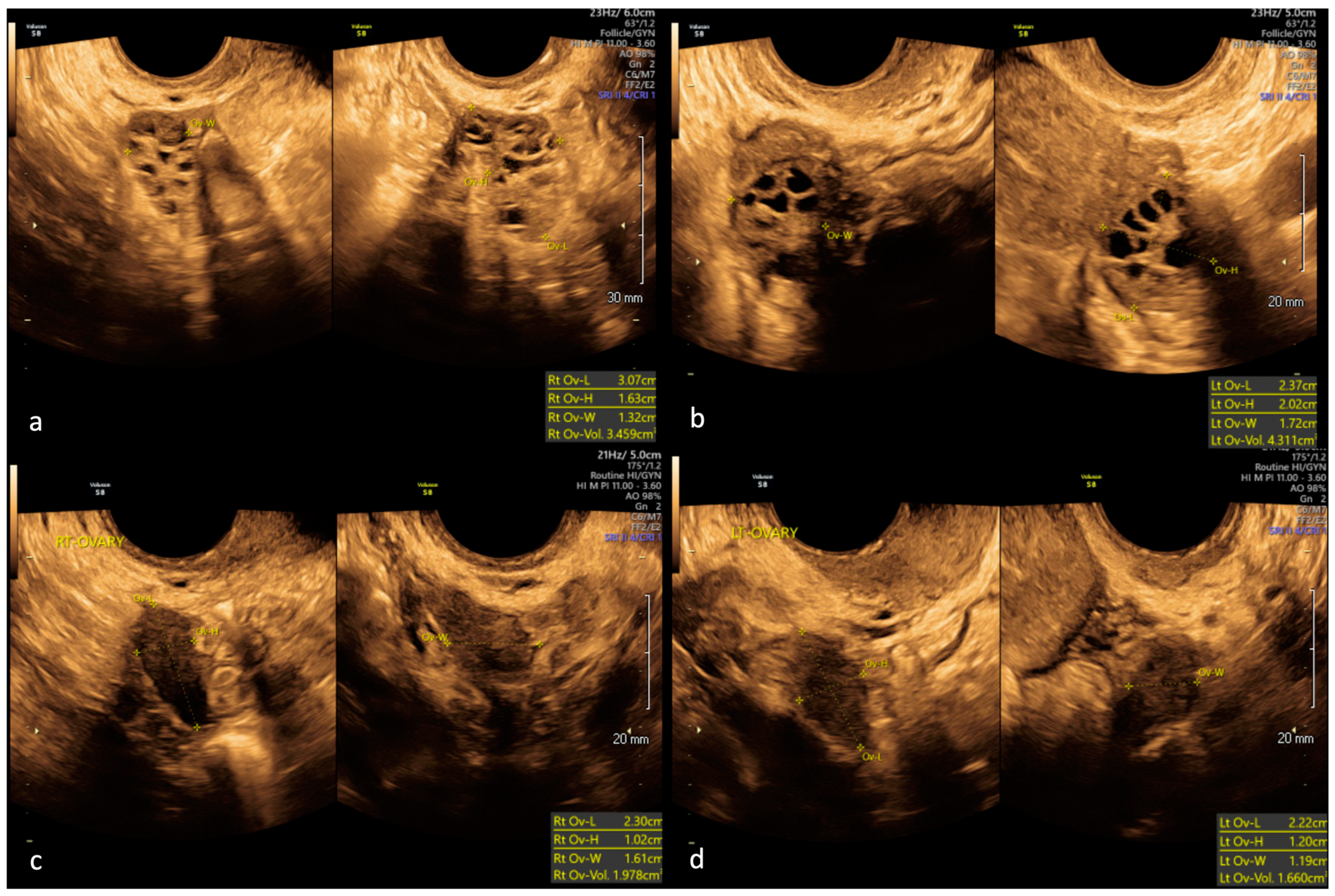
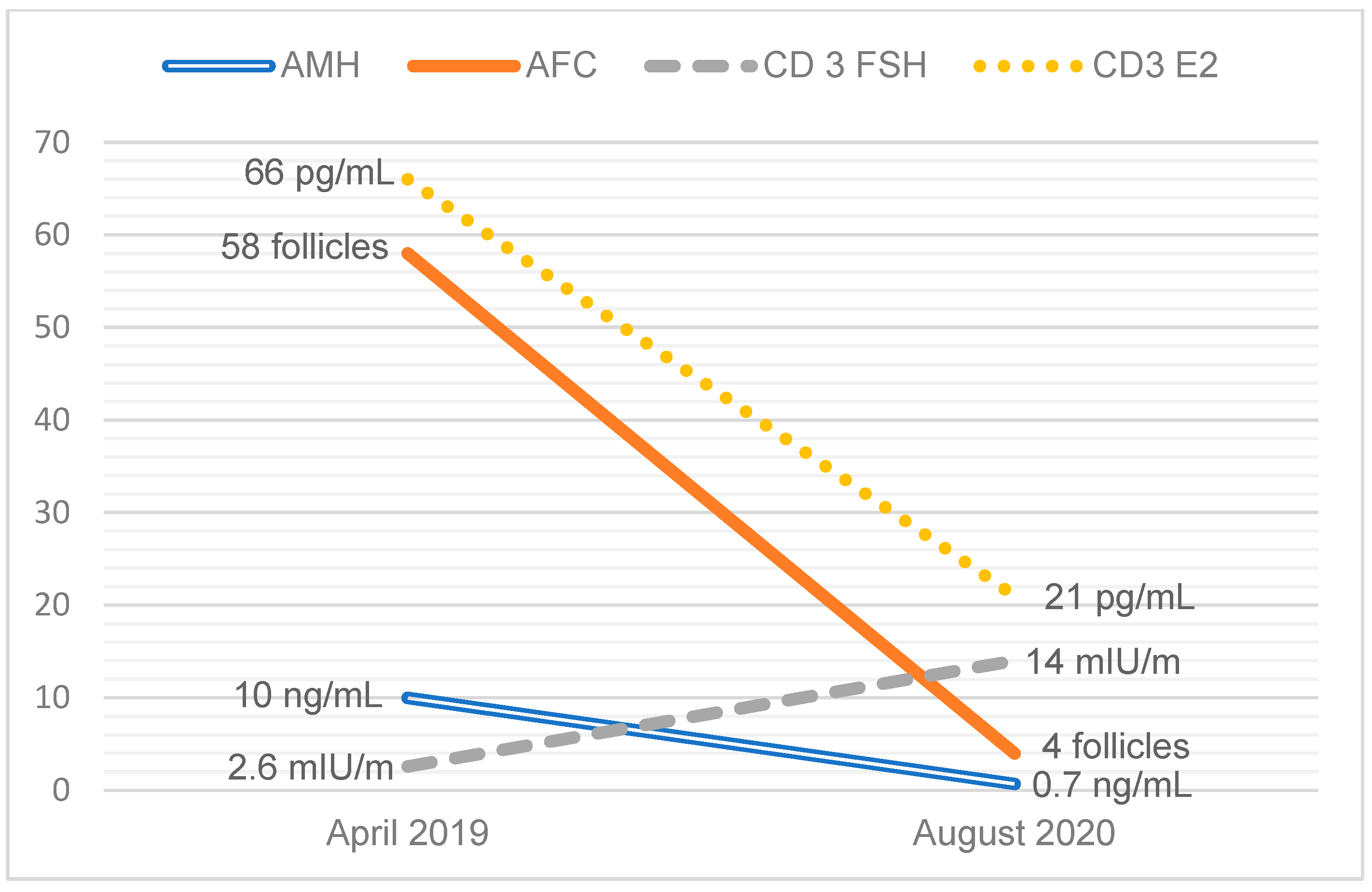
2. Case Report
3. Literature Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carson, S.A.; Kallen, A.N. Diagnosis and Management of Infertility: A Review. JAMA 2021, 326, 65–76. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine. Testing and Interpreting Measures of Ovarian Reserve: A Committee Opinion. Fertil. Steril. 2020, 114, 1151–1157. [Google Scholar] [CrossRef]
- Younis, J.S.; Ben-Ami, M.; Ben-Shlomo, I. The Bologna Criteria for Poor Ovarian Response: A Contemporary Critical Appraisal. J. Ovarian Res. 2015, 8, 76. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Primary Ovarian Insufficiency in Adolescents and Young Women: Committee Opinion No. 605. Obs. Gynecol 2014, 124, 193–197. [Google Scholar] [CrossRef]
- Moiseeva, A.V.; Kudryavtseva, V.A.; Nikolenko, V.N.; Gevorgyan, M.M.; Unanyan, A.L.; Bakhmet, A.A.; Sinelnikov, M.Y. Genetic Determination of the Ovarian Reserve: A Literature Review. J. Ovarian Res. 2021, 14, 102. [Google Scholar] [CrossRef] [PubMed]
- The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 Consensus on Diagnostic Criteria and Long-Term Health Risks Related to Polycystic Ovary Syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar] [CrossRef]
- Cheng, R.; Ma, Y.; Nie, Y.; Qiao, X.; Yang, Z.; Zeng, R.; Xu, L. Chromosomal Polymorphisms Are Associated with Female Infertility and Adverse Reproductive Outcomes after Infertility Treatment: A 7-Year Retrospective Study. Reprod. Biomed. Online 2017, 35, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Dana, M.; Stoian, V. Association of Pericentric Inversion of Chromosome 9 and Infertility in Romanian Population. Maedica 2012, 7, 25–29. [Google Scholar] [PubMed]
- Kumar, M.; Chapadgaonkar, S. Homozygosity and Heterozygosity of Pericentric Inversion of Chromosome 9 and Its Clinical Impact. J. Clin. Diagn. Res. 2012, 6, 816–820. [Google Scholar]
- Minocherhomji, S.; Athalye, A.S.; Madon, P.F.; Kulkarni, D.; Uttamchandani, S.A.; Parikh, F.R. A Case-Control Study Identifying Chromosomal Polymorphic Variations as Forms of Epigenetic Alterations Associated with the Infertility Phenotype. Fertil. Steril. 2009, 92, 88–95. [Google Scholar] [CrossRef]
- Sahin, F.I.; Yilmaz, Z.; Yuregir, O.O.; Bulakbasi, T.; Ozer, O.; Zeyneloglu, H.B. Chromosome Heteromorphisms: An Impact on Infertility. J. Assist. Reprod. Genet. 2008, 25, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Li, F.; Tan, W.; Tang, J. Analysis of the Clinical Features of Pericentric Inversion of Chromosome 9. J. Int. Med. Res. 2020, 48, 0300060520957820. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K. Population Studies of Inv(9) Chromosomes in 4300 Japanese: Incidence, Sex Difference and Clinical Significance. Jpn. J. Hum. Genet. 1992, 37, 293–301. [Google Scholar] [CrossRef]
- Azim, M.; Khan, A.H.; Khilji, Z.L.; Pal, J.A.; Khurshid, M. Chromosomal Abnormalities as a Cause of Recurrent Abortions: A Hospital Experience. J. Pak. Med. Assoc. 2003, 53, 117–119. [Google Scholar]
- Cozaru, G.C.; Butnariu, L.I.; Gorduza, E.V. Genetic Counselling in Reproductive Disorders. Procedia-Soc. Behav. Sci. 2012, 33, 213–217. [Google Scholar] [CrossRef]
- Dubey, S.; Chowdhury, M.R.; Prahlad, B.; Kumar, V.; Mathur, R.; Hamilton, S.; Kabra, M.; Menon, P.S.N.; Verma, I.C. Cytogenetic Causes for Recurrent Spontaneous Abortions—An Experience of 742 Couples (1484 Cases). Indian J. Hum. Genet. 2005, 11, 94–98. [Google Scholar] [CrossRef]
- Dutta, U.R.; Rajitha, P.; Pidugu, V.K.; Dalal, A.B. Cytogenetic Abnormalities in 1162 Couples with Recurrent Miscarriages in Southern Region of India: Report and Review. J. Assist. Reprod. Genet. 2011, 28, 145. [Google Scholar] [CrossRef] [PubMed]
- Elkarhat, Z.; Kindil, Z.; Zarouf, L.; Razoki, L.; Aboulfaraj, J.; Elbakay, C.; Nassereddine, S.; Nasser, B.; Barakat, A.; Rouba, H. Chromosomal Abnormalities in Couples with Recurrent Spontaneous Miscarriage: A 21-Year Retrospective Study, a Report of a Novel Insertion, and a Literature Review. J. Assist. Reprod. Genet. 2019, 36, 499–507. [Google Scholar] [CrossRef]
- Flynn, H.; Yan, J.; Saravelos, S.H.; Li, T.C. Comparison of Reproductive Outcome, Including the Pattern of Loss, between Couples with Chromosomal Abnormalities and Those with Unexplained Repeated Miscarriages. J. Obstet. Gynaecol. Res. 2014, 40, 109–116. [Google Scholar] [CrossRef]
- Ghazaey, S.; Keify, F.; Mirzaei, F.; Maleki, M.; Tootian, S.; Ahadian, M.; Abbaszadegan, M.R. Chromosomal Analysis of Couples with Repeated Abortions in Northeastern Iran. Int. J. Fertil. Steril. 2015, 9, 47. [Google Scholar] [CrossRef]
- Makino, T.; Tabuchi, T.; Nakada, K.; Iwasaki, K.; Tamura, S.; Iizuka, R. Chromosomal Analysis in Japanese Couples with Repeated Spontaneous Abortions. Int. J. Fertil. 1990, 35, 266–270. [Google Scholar] [PubMed]
- Mozdarani, H.; Mohseni Meybodi, A.; Karimi, H. Impact of Pericentric Inversion of Chromosome 9 [Inv (9) (P11q12)] on Infertility. Indian J. Hum. Genet. 2007, 13, 26–29. [Google Scholar] [CrossRef]
- Nonaka, T.; Takahashi, M.; Nonaka, C.; Enomoto, T.; Takakuwa, K. The Analysis of Chromosomal Abnormalities in Patients with Recurrent Pregnancy Loss, Focusing on the Prognosis of Patients with Inversion of Chromosome (9). Reprod. Med. Biol. 2019, 18, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Rawal, L.; Kumar, S.; Mishra, S.R.; Lal, V.; Bhattacharya, S.K. Clinical Manifestations of Chromosomal Anomalies and Polymorphic Variations in Patients Suffering from Reproductive Failure. J. Hum. Reprod. Sci. 2020, 13, 209–215. [Google Scholar] [CrossRef]
- Yuce, H. A Rare Seen Case with Homozygosity for Pericentric Inversion of Chromosome 9 and Primary Infertility. Am. J. Case Rep. 2008, 9, 385–388. [Google Scholar]
- Šípek, A.J.; Panczak, A.; Mihalová, R.; Hrčková, L.; Suttrová, E.; Sobotka, V.; Lonský, P.; Kaspříková, N.; Gregor, V. Pericentric Inversion of Human Chromosome 9 Epidemiology Study in Czech Males and Females. Folia Biol 2015, 61, 140–146. [Google Scholar]
- Demirhan, O.; Pazarbasi, A.; Suleymanova-Karahan, D.; Tanriverdi, N.; Kilinç, Y. Correlation of Clinical Phenotype with a Pericentric Inversion of Chromosome 9 and Genetic Counseling: A Report of 157 Carriers. Saudi Med. J. 2008, 29, 946–951. [Google Scholar]
- Yuksel, S.; Savaci, S.; Ekici, C.; Kurtoglu, E.L.; Korkmaz, S.; Yesilada, E. Prevalence of Pericentric Inversion of Chromosome 9 in Eastern Anatolia Region and Relationship to Reproductive Efficiency. EJMO 2018, 2, 40–42. [Google Scholar]
- Teo, S.H.; Tan, M.; Knight, L.; Yeo, S.H.; Ng, I. Pericentric Inversion 9—Incidence and Clinical Significance. Ann. Acad. Med. Singap. 1995, 24, 302–304. [Google Scholar]
- Kosyakova, N.; Grigorian, A.; Liehr, T.; Manvelyan, M.; Simonyan, I.; Mkrtchyan, H.; Aroutiounian, R.; Polityko, A.D.; Kulpanovich, A.I.; Egorova, T.; et al. Heteromorphic Variants of Chromosome 9. Mol. Cytogenet. 2013, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.; Jacobsen, J.C.; Ernst, C.; Hanscom, C.; Heilbut, A.; Blumenthal, I.; Mills, R.E.; Kirby, A.; Lindgren, A.M.; Rudiger, S.R.; et al. Complex Reorganization and Predominant Non-Homologous Repair Following Chromosomal Breakage in Karyotypically Balanced Germline Rearrangements and Transgenic Integration. Nat. Genet. 2012, 44, 390–397. [Google Scholar] [CrossRef]
- Stephens, P.J.; Greenman, C.D.; Fu, B.; Yang, F.; Bignell, G.R.; Mudie, L.J.; Pleasance, E.D.; Lau, K.W.; Beare, D.; Stebbings, L.A.; et al. Massive Genomic Rearrangement Acquired in a Single Catastrophic Event during Cancer Development. Cell 2011, 144, 27–40. [Google Scholar] [CrossRef]
- Kloosterman, W.P.; Hoogstraat, M.; Paling, O.; Tavakoli-Yaraki, M.; Renkens, I.; Vermaat, J.S.; van Roosmalen, M.J.; van Lieshout, S.; Nijman, I.J.; Roessingh, W.; et al. Chromothripsis Is a Common Mechanism Driving Genomic Rearrangements in Primary and Metastatic Colorectal Cancer. Genome Biol. 2011, 12, R103. [Google Scholar] [CrossRef] [PubMed]
- Shorokhova, M.; Nikolsky, N.; Grinchuk, T. Chromothripsis-Explosion in Genetic Science. Cells 2021, 10, 1102. [Google Scholar] [CrossRef] [PubMed]
- de Pagter, M.S.; van Roosmalen, M.J.; Baas, A.F.; Renkens, I.; Duran, K.J.; van Binsbergen, E.; Tavakoli-Yaraki, M.; Hochstenbach, R.; van der Veken, L.T.; Cuppen, E.; et al. Chromothripsis in Healthy Individuals Affects Multiple Protein-Coding Genes and Can Result in Severe Congenital Abnormalities in Offspring. Am. J. Hum. Genet. 2015, 96, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Starke, H.; Seidel, J.; Henn, W.; Reichardt, S.; Volleth, M.; Stumm, M.; Behrend, C.; Sandig, K.R.; Kelbova, C.; Senger, G.; et al. Homologous Sequences at Human Chromosome 9 Bands P12 and Q13-21.1 Are Involved in Different Patterns of Pericentric Rearrangements. Eur. J. Hum. Genet. 2002, 10, 790–800. [Google Scholar] [CrossRef]
- Dong, Z.; Yan, J.; Xu, F.; Yuan, J.; Jiang, H.; Wang, H.; Chen, H.; Zhang, L.; Ye, L.; Xu, J.; et al. Genome Sequencing Explores Complexity of Chromosomal Abnormalities in Recurrent Miscarriage. Am. J. Hum. Genet. 2019, 105, 1102–1111. [Google Scholar] [CrossRef]
- Merrion, K.; Maisenbacher, M. Pericentric Inversion (Inv) 9 Variant—Reproductive Risk Factor or Benign Finding? J. Assist. Reprod. Genet. 2019, 36, 2557–2561. [Google Scholar] [CrossRef]
- McAllister, J.M.; Legro, R.S.; Modi, B.P.; Strauss, J.F. Functional Genomics of PCOS: From GWAS to Molecular Mechanisms. Trends Endocrinol. Metab. 2015, 26, 118. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year | Country | Population | Control Group | Outcome | Results |
|---|---|---|---|---|---|
| Studies comparing the prevalence of Inv(9) in individuals with infertility or RPL to controls | |||||
| Cheng et al., 2017 [7] | China | Women ages 20–44 years with infertility. (N = 16,285 including N = 2175 with unexplained infertility) Women with chromosome aneuploidy were excluded. | Women in the same age group seeking preconception genetic testing for RPL or stillbirth, advanced maternal age, or history of a child with a prior genetic condition or birth defect. (N = 3665). | Prevalence of Inv(9) | Infertile cases: N = 195 (1.2%) Subset of women with unexplained infertility: N = 45 (2.1%) Fertile controls: N = 29 (0.79%) p < 0.05 for comparisons to controls |
| Dana et al., 2012 [8] | Romania | Men and women with infertility (N = 1800). | Amniocentesis from fetuses considered to be a sample of fertile population (spontaneous pregnancy) (N = 1116) | Prevalence of Inv(9) (p11q12), (p11q13) | Infertile cases: N = 41 (2.28%) Fertile controls: N = 44 (3.94%) N.S. |
| Kumar et al., 2012 [9] | India | Men and women with unexplained infertility (N = 1000). | Individuals of Indian origin in the general population (unpublished data) (N = 4500) | Prevalence of Inv(9) | Infertile cases: N = 26 (2.6%) General population: N = 33 (0.73) p < 0.001 compared to controls |
| Minocherhomji et al., 2009 [10] | India | Men and women with infertility (N = 760). | Age and geographically matched individuals without a history of infertility (N = 555) | Prevalence of Inv(9) | Infertile cases: N = 7 (0.9%) Fertile controls: N = 1 (0.2%) N.S. |
| Sahin et al., 2008 [11] | Turkey | Men and women with infertility (N = 276). | Amniocentesis from fetuses considered to be a sample of fertile population (spontaneous pregnancy) (N = 1130) | Prevalence of Inv(9) | Infertile cases: N = 4 (1.45%) Fertile controls: N = 8 (0.71%) N.S. |
| Xie et al., 2020 [12] | China | Men and women with infertility or RPL (N = 2816). | Adult patients without infertility were sent for karyotyping during the same time (N = 172) | Prevalence of Inv(9) | Infertile cases: N = 31 (2.1%) Fertile controls: N = 5 (2.91%) N.S. |
| Yamada et al., 1992 [13] | Japan | Men and women with more than two first-trimester pregnancy losses (N = 752). | Healthy volunteers (N = 1513) | Prevalence of Inv(9) | Infertile cases: N = 24 (3.2%) Fertile controls: N = 25 (1.7%) p = 0.02 |
| Studies reporting the prevalence of Inv(9) in individuals with infertility or RPL, no control group | |||||
| Azim, 2003 [14] | Pakistan | Men and women with RPL (N = 600). | None | Prevalence of Inv(9) | N = 4 (0.67%) |
| Cozaru et al., 2012 [15] | Romania | Men and women with RPL (N = 298) or primary infertility (N = 160). | None | Prevalence of Inv(9) | RPL: N = 2 (0.67%) Primary infertility; N = 4 (2.5%) |
| Dubey et al., 2005 [16] | India | Men and women with RPL (N = 1484). | None | Prevalence of Inv(9) | N = 3 (0.2%) |
| Dutta et al., 2011 [17] | India | Men and women with RPL (N = 2324). | None | Prevalence of Inv(9) | N = 14 (0.6%) |
| Elkarhart et al., 2019 [18] | Morroco | Men and women with RPL (N = 1254). | None | Prevalence of Inv(9) | N = 26 (2.1%) |
| Flynn et al., 2013 [19] | UK | Men and women with RPL (N = 1590). | None | Prevalence of Inv(9) | N = 1 (0.01%) |
| Ghazaey et al., 2015 [20] | India | Men and women with RPL (N = 1456). | None | Prevalence of Inv(9) | N = 20 (1.4%) |
| Makino et al., 1990 [21] | Japan | Men and women with RPL (N = 1278). | None | Prevalence of Inv(9) | N = 15 (1.2%) |
| Mozdarani et al., 2007 [22] | Iran | Men and women with at least 3 years of infertility (N = 601). | None | Prevalence of Inv(9) | N = 15 (2.5%) |
| Nonaka et al., 2019 [23] | Japan | Men and women with RPL (N = 4012). | None | Prevalence of Inv(9) | N = 52 (1.3%) |
| Rawal et al., 2020 [24] | India | Men and women with infertility, RPL, or IVF failure (N = 1276). | None | Prevalence of Inv(9) | N = 47 (3.7%) |
| Yuce et al., 2008 [25] | Turkey | Men and women with infertility (N = 2876). | None | Prevalence of Inv(9) | N = 41 (1.4%) |
| Studies comparing the prevalence of infertility or RPL in individuals with Inv(9) to controls | |||||
| Sipek et al., 2015 [26] | Czech Republic | Men and women with Inv(9) (N = 170) were identified from a large database of individuals referred for cytogenetic testing (N = 26,597). | Individuals with normal karyotypes were identified from the same overall cohort using the systemic sampling method (N = 661). | Prevalence of idiopathic reproductive failure | Inv(9): N = 63 (37.1%)Control: N = 214 (32.4%)p = 0.27 |
| Studies comparing the prevalence of infertility or RPL in individuals with Inv(9), no control group | |||||
| Demirhan et al., 2008 [27] | Turkey | Individuals with Inv(9) (N = 157) were identified from a large database of individuals referred for cytogenetic testing (N = 15,528). | None | Prevalence of RPL, primary amenorrhea, and infertility | Infertility: N = 2 (1.3%) RPL: N = 48 (29.9%) Primary amenorrhea: N= 4 (2.5%) |
| Yuksel et al., 2019 [28] | Turkey | Men and women with Inv(9) (N = 71) were identified from a large database of individuals referred for cytogenetic testing (N = 4168). | None | Prevalence of infertility and RPL | Infertility: N= 32 (45.1%) RPL: N = 4 (5.6%) |
| Teo et al., 1995 [29] | Singapore | Men and women with Inv(9) (N = 33) were identified from a large database of individuals referred for cytogenetic testing (N = 2448). | None | Prevalence of subfertility | Subfertility: N = 12 (36%) |
| Kosyakova et al., 2013 [30] | Multiple countries in Eastern + Western Europe | Individuals with Inv(9) were identified during routine diagnostic testing (N = 209). | None | Prevalence of infertility | Infertility: N = 79 (37.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bui, L.M.; Cooney, L.G.; Stanic, A.K. Rapid Ovarian Reserve Decline in a Woman with Pericentric Inv(9) Variant. Women 2023, 3, 421-431. https://doi.org/10.3390/women3030032
Bui LM, Cooney LG, Stanic AK. Rapid Ovarian Reserve Decline in a Woman with Pericentric Inv(9) Variant. Women. 2023; 3(3):421-431. https://doi.org/10.3390/women3030032
Chicago/Turabian StyleBui, Leeann M., Laura G. Cooney, and Aleksandar K. Stanic. 2023. "Rapid Ovarian Reserve Decline in a Woman with Pericentric Inv(9) Variant" Women 3, no. 3: 421-431. https://doi.org/10.3390/women3030032