1. Introduction
Body dissatisfaction is defined as a negative subjective evaluation of one’s own body. This negative evaluation is predominantly specific to an element of one’s body, such as weight, body shape, thinness, muscularity, or height, however, it can be generalized to the body as a whole [
1]. Research supports that body dissatisfaction is often associated with a greater risk of eating disorder pathology, psychological distress, and poor quality of life [
2,
3,
4]. Body ideals for both men and women are constantly evolving, and therefore our understanding of the nature of body dissatisfaction needs to progress with it. For instance, body fat and body weight were the traditional focus of body image research and treatment for women, with the belief of ‘not being thin enough’ considered the defining, and sometimes the sole attitude of body image-related psychopathology; emphasizing a greater drive for thinness in previous research [
1]. However, more recent studies have emphasized the importance of considering more muscular and toned physiques within female body image research, highlighting a focus on the drive for muscularity [
5,
6,
7]. Various studies have identified that a toned, lean, athletic muscularity constitutes the ideal female figure [
5,
6,
7]. Specifically, Bozsik and colleagues [
5] identified that US undergraduate women prefer a body shape that is both slim and muscular, whilst Cunningham and colleagues [
6] demonstrated the link between muscle dissatisfaction and eating disorder psychopathology in women. Additionally, previous research on body image highlights how vital it is to understand how factors such as the drive for thinness, the drive for muscularity, or body dissatisfaction influence body image perceptions [
5,
6,
7].
Alternatively, for men, body image research has predominantly focused on body fat and musculature, and how these factors influence body shape. Although, emerging research has implicated the importance of height and height dissatisfaction in the manifestation of body dissatisfaction in men. Notably, a negative association between height and height dissatisfaction (i.e., men of shorter stature tend to be more dissatisfied with their height compared to men of taller stature) has been demonstrated in undergraduate males [
8], sexual minority samples [
3], and in a sample of men recruited from an internet forum for short-statured individuals [
9]. These studies also showed that a greater height dissatisfaction is related to greater muscle dissatisfaction, desire to have greater muscular ideals, eating disorder symptoms, and an impaired quality of life [
3,
8,
9]. Despite the recent surge of research on height dissatisfaction as a key component of body image within male populations, the presence of height dissatisfaction and the potential significance of height has been largely overlooked within female populations.
1.1. Height and Body Image in Women
Even with body image research being predominantly specific to each gender, it still begs the question, why might height be an important facet of body image for women? For one, women of taller stature may feel that they challenge traditional norms of femininity and fall outside of height preferences for heterosexual romantic relationships. Prior studies have demonstrated that men and women both have consistent height preferences for heterosexual relationships (a dyad consisting of a taller man and shorter women) [
10,
11,
12]. For instance, Salska and colleagues [
11] found that both men and women preferred a heterosexual relationship to be composed of a taller man and a shorter woman, and only 4% of women (and 23% of men) would accept a dating relationship where the woman was taller. It has been suggested that these preferences are driven by historic notions of masculinity and femininity, with prior studies consistently demonstrating the link between tall stature and masculinity and interpersonal dominance [
13,
14,
15]. Therefore, women of taller stature may feel that they challenge traditional norms about women’s social status relative to men’s and might feel less feminine as a result. Additionally, recent research suggests that a taller women’s height may become the target of unwanted attention, resulting in a negative affect [
16,
17]. For instance, Fuller [
17] found that tall women frequently reported that they felt as though they were constantly the subject of unwanted height-related comments that draw attention to their tallness, resulting in self-consciousness related to their height. This concern over women’s tall stature has been and continues to be reinforced in some societies through growth-suppression treatments such as synthetic estrogen [
18,
19]. Although declining in use, a study from 2002 showed that approximately one-third of American pediatric endocrinologists offer growth suppression as a treatment for girls of taller stature. Notably, parents’ and patients’ concerns about the adverse social effects of unusually tall stature were cited as one of the central reasons for offering growth-suppression treatment [
20].
1.2. Height and Theoretical Models of Body Dissatisfaction
Theoretically, objectification theory could explain why societal perceptions of height may increase body/height dissatisfaction, especially in women. Objectification theory was developed to explain how everyday objectifying experiences lead women to view themselves from an outsider’s perspective within a feminist sociocultural framework [
21]. In this context, women are socialized to view and treat themselves as “objects” to be valued for their appearance or consumption [
21]. Thus, it could be assumed that negative comments or associations about their height or comparisons to others’ heights may lead to an increase in height dissatisfaction and poor quality of life. This appearance-focused shift can result in unrealistic socio-cultural ideals and greater dissatisfaction as height cannot be changed, perpetuating an unrelenting cycle [
22].
Similarly, social comparison theory also provides a solid foundation for understanding the relationship between height and height dissatisfaction. Social comparison theory posits that people make innate comparisons to others in order to inform the sufficiency or appropriateness of a characteristic of their own body [
23]. Social comparison theory outlines two types of social comparison: upward and downward comparisons. The upward comparison refers to the comparison of oneself to others they believe to be better than them on a given characteristic [
23,
24]. For example, an individual may compare themselves to a peer with a lower body fat percentage, a common desirable characteristic in Western society. Upwards comparisons such as this typically result in an increase in body dissatisfaction and drive for thinness. Alternately, downward comparison refers to the comparison to another who is perceived to be poorer or lesser on a given characteristic (e.g., an individual comparing themselves to another person who has a relatively greater body fat percentage). Typically, downward comparisons result in an increase in body satisfaction and mood [
23,
24]. It is plausible that these same mechanisms may occur when comparing one’s height to another, with comparisons to others with more desirable heights resulting in an increase in body dissatisfaction, or specifically height dissatisfaction.
1.3. Height and Drive for Thinness and Muscularity, and Quality of Life
Height differs from other aspects of body composition as it cannot easily be altered. For instance, if an individual wants to lose weight and gain muscular bulk, shape, or tone, they can alter their diet and increase their exercise frequency and intensity. However, no such behaviors can impact an individual’s height. Talbot and Mahlberg [
8] posit that consequently, the negative affect associated with height dissatisfaction might be directed toward other, more easily modifiable areas of body image, such as body fat percentage and muscular shape and tone. Thus, dissatisfaction with height may be associated with an increased drive for muscularity and/or thinness. Notably, drive for muscularity and thinness has been associated with increased body dissatisfaction generally [
25,
26,
27], suggesting that these behavioral intentions often reflect negative body image.
Another consideration of prior research is the relationship between height, height dissatisfaction, and quality of life. Quality of life is defined as the overall, self-perceived satisfaction with life areas of deemed importance, including relationships, occupation, leisure time, and opportunities for learning and creativity, and has been used as an indicator of the impact of mental health issues on day-to-day living [
28]. For women, poorer quality of life has been associated with greater body dissatisfaction [
29], and shorter stature in adult life is somewhat predictive of a poorer health-related quality of life [
30,
31]. Additionally, for men, poorer quality of life has been associated with shorter stature and greater height dissatisfaction [
3], meaning that stature and dissatisfaction with height appear to have a clear impact on the lives of men. However, no research has directly examined the association between height, height dissatisfaction, and quality of life in women.
1.4. Aims and Hypotheses
Given the established link between body dissatisfaction and height dissatisfaction in men [
3], and the potential negative ramifications of body dissatisfaction in general [
4], the paucity of research on this topic within a female population has led to the development of the present study. The present study aimed to examine the link between height, height dissatisfaction, and body dissatisfaction-related constructs in Australian women. These constructs include the drive for thinness and muscularity, how differently one is treated because of their height, and quality of life. Additionally, this study aimed to explore the height preferences of oneself and romantic partners in Australian women.
First, it was hypothesized (H1) that there would be a significant difference between the reported actual height of participants, and their ideal height (the height that they would like to be). Second, it was hypothesized (H2) that self-reported height would be positively correlated with height dissatisfaction, and women of taller stature would report that they believe they are treated worse due to their height, compared to shorter women. Third, based on established associations between height and height dissatisfaction in men [
3,
8,
9], it was hypothesized (H3) that there would be a positive correlation between height dissatisfaction, and drive for thinness and drive for muscularity, respectively, and a negative correlation between height dissatisfaction and quality of life. As height and height dissatisfaction is a relatively understudied aspect of body image in women, the present study also sought to explore women’s height preferences in romantic partners (i.e., whether Australian women prefer to date a partner who is taller, shorter, or the same height relative to them, and if women would date a partner who is shorter than them or not).
2. Materials and Methods
2.1. Participants
To fulfil the eligibility criteria for the present study, participants must have reported their sex as female, an age of 18 years or greater, and be an Australian resident. A total of 237 Australian women were recruited via snowballing on Facebook and Reddit and advertising via flyers displayed on noticeboards around the University of Notre Dame Australia, Sydney campus fulfilling the eligibility criteria and were therefore initially included in our study. Of this initial sample, 65 participants did not complete the survey and were therefore removed, meaning 172 participants were included in the final sample. Included participants were aged between 18 and 60 years (M = 27.38, SD = 9.09), with BMIs ranging from 16.65 to 62.50 (M = 24.24; SD = 6.05). Participants reported their ethnicity as White (49%), Australian (19%), Greek/Cypriot (16%), Asian (7%), and other (12%). All participants were residing in Australia at the time of undertaking the survey.
2.2. Procedure
The survey was hosted online by Qualtrics and distributed via a web link and a QR code. Participants completed the survey on their personal computers or smart devices. Participants were informed that the study aimed to ask questions about height and attitudes towards one’s own body. Upon entering the survey, and providing informed consent, participants were presented with the demographic questionnaire and then all other measures (detailed below); all components after the demographic questionnaire were randomized across respondents to control for bias due to order effects. After completion of the survey, participants were thanked and informed that their responses had been anonymously recorded. No monetary investment was made in this research project.
2.3. Measures
2.3.1. Demographic Questionnaire
Participants were asked to provide their sex, height (in centimeters), and weight (in kilograms). Body Mass Index (BMI) was calculated from participants’ weight and height using the formula BMI = kg/m2. Participants also reported their age and race/ethnicity.
2.3.2. Height Preferences
This measure involved two questions pertaining to how tall a respondent would like a romantic partner to be, relative to their own height. Respondents were asked: “Would you date a romantic partner that is shorter than you?” (yes or no), and “What is your height preference for a romantic partner?” (taller than me; shorter than me; the same height; or no preference).
2.3.3. Height Dissatisfaction
Participants were asked to report their actual and ideal height (in centimeters). Additionally, the Male Body Attitude Scale (MBAS)–Height Subscale [
32] was included. Although this scale was initially designed for men, the two questions that constitute the height scale are non-sex-specific and were used as an index of height dissatisfaction. Participants were also asked “Are you treated differently from other people due to your height?”, responding on a seven-point Likert scale (1 = “much worse than other people”; 7 = “much better than other people”). Alpha for the current sample was 0.91.
2.3.4. Female Muscularity Scale (FMS)
Drive for muscularity was measured by the FMS [
33]. The FMS is comprised of 10 items requiring participants to reflect on the extent to which they related to muscularity-driven attitudes and behaviors. Responses were provided on a 5-point Likert-type scale (1 = “never”; 5 = “always”) and averaged across all items. Higher scores indicated a higher drive for muscularity. The FMS has been shown to be a reliable and valid measure of drive for muscularity in women [
33]. Alpha for the current sample was 0.83.
2.3.5. Drive for Thinness (DTS)
Drive for thinness was measured using the DTS, a subscale of the Eating Disorder Inventory–3 [
34]. The measure includes 17 items (e.g., “I exaggerate or magnify the importance of my weight.”) with responses made on a 6-point rating scale ranging scale (1 = never; 6 = always) and averaged across all items. Higher scores on the DTS are indicative of a greater drive for thinness. The DTS has been shown to be a reliable and valid measure of drive for thinness in women [
34,
35]. Alpha for the current sample was 0.81.
2.3.6. Quality of Life (BBQS)
The 12-item BBQS [
36] was used to measure the quality of life. Items on the BBQS cover six life areas, namely, leisure, creativity, learning, friends and friendship, view on one’s life, and view on one’s self. Responses are given on a 5-point response scale (0 = “do not agree at all”; 4 = “agree completely”). The BBQS explicitly takes into account the importance that each participant ascribes to each life area when determining their overall quality of life score. The BBQS has been shown to be a reliable and valid measure of the quality of life in women [
36]. Alpha for the current sample was 0.81.
2.4. Statistical Analysis
G*Power version 3.1 was used to determine that our sample size of 172 was adequate for our selected analysis. Age and BMI were initially intended to be included as covariates in our analyses, however, they did not correlate with any of our variables of interest and therefore were not included in further analyses. For H1, a Shapiro-Wilks test identified that the assumptions of normality were violated for ideal height scores, so the present study employed a non-parametric test. Therefore, to examine H1, a Wilcoxon signed-rank test was used to examine whether there was a significant difference between participant’s actual and ideal height, and Matched Pair Rank Biserial Correlation r was applied to demonstrate the effect size. To examine H2 and H3, a series of Pearson’s correlations were conducted between self-reported height, Height Dissatisfaction scores, treated differently because of height scores, the FMS, the DTS, and the BBQS. To further examine H2, two non-parametric one-way ANOVAs (Kruskal-Wallis tests) were utilized. For the first one-way ANOVA, the height quartile was the independent variable, and height dissatisfaction was the dependent variable. For the second one-way ANOVA, the height quartile was the independent variable, and treatment due to height score was the dependent variable. Partial eta squared was applied to demonstrate effect sizes. Post hoc pairwise comparisons were utilized to examine specific differences between each height quartile. Additionally, descriptive statistics for height preferences were reported. Ethics approval for the study was granted by an appropriate institutionalized Human Ethics Research Board (Approval number = 2021-055S).
3. Results
All data were collected between 6 and 30 May 2021. In relation to H1, results of the Wilcoxon signed-rank test showed that on average, women reported a significantly greater ideal height (
M = 167.65 cm,
SD = 7.08) compared to their actual height (
M = 165.61 cm,
SD = 7.49),
Z(166) = −4.27,
p < 0.001,
r = −0.49. Notably, 45% of participants wanted to be taller than their current height, 16% wanted to be shorter than their current height, and 39% of participants reported that their height was in line with their ideal height.In relation to H2, results showed that height and height dissatisfaction were negatively correlated, meaning that women who were shorter in stature tended to be more dissatisfied with their height. Additionally, height was positively correlated with treatment due to height score, indicating that shorter women tended to report that they believed they were treated worse compared to taller women. There was also a significant negative correlation between height dissatisfaction and the treatment due to height score, meaning that women who were dissatisfied with their height also tended to believe that they were treated poorly due to their height (
Table 1).
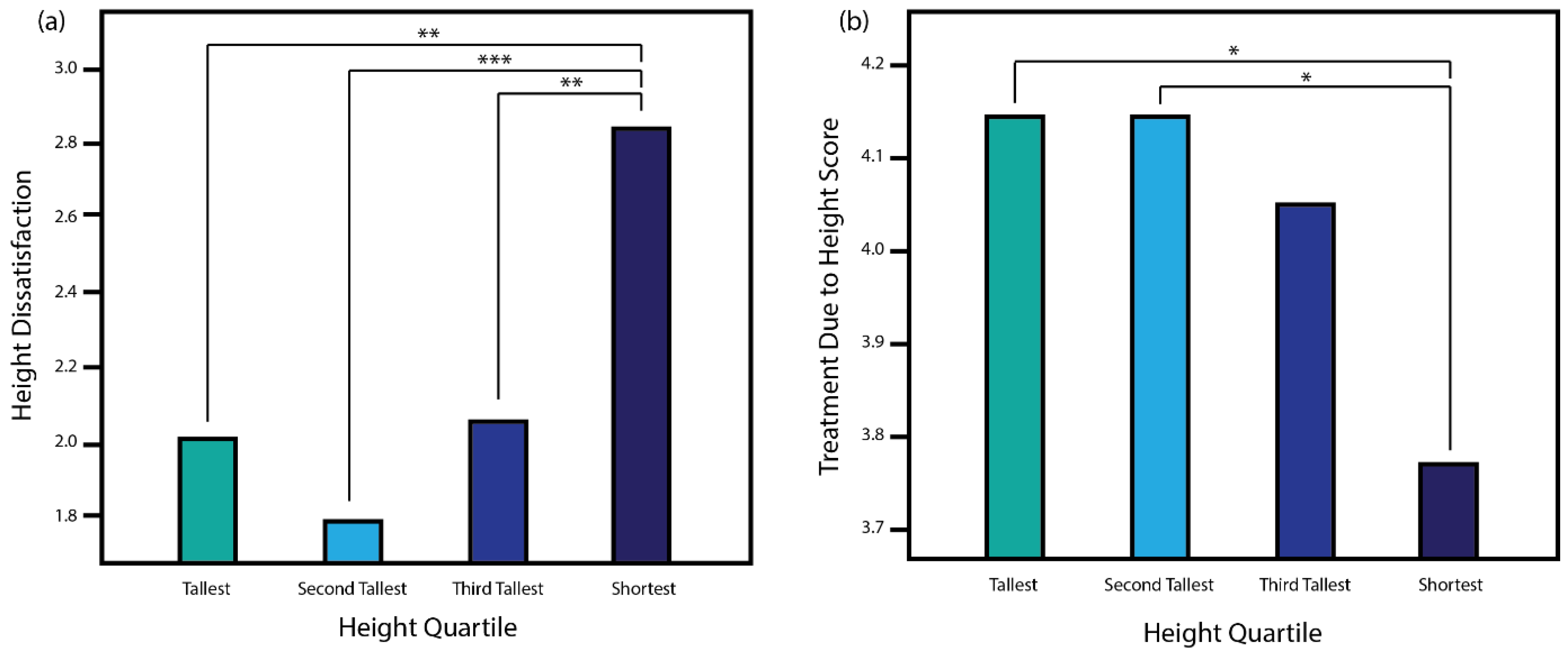
Further, two one-way ANOVAs were conducted to assess differences in height dissatisfaction and how differently one is treated because of their height across each height quartile. There were 43 participants in each quartile. Participants’ height in the tallest quartile ranged from 170 to 185 cm (
M = 174.68,
SD = 4.06). Participants’ height in the second tallest quartile ranged from 167 to 170 cm (
M = 168.19,
SD = 1.07). Participants’ height in the third tallest quartile ranged from 160 to 166 cm (
M = 163.35,
SD = 1.74). Participants’ height in the shortest quartile ranged from 149 to 160 cm (
M = 155.45,
SD = 2.94). Results showed that there was a statistically significant difference in height dissatisfaction across height quartiles,
F(3168) = 9.60,
p < 0.001, η
p2 = 0.15. Post hoc pairwise comparisons showed that women in the shortest quartile were significantly greater in height dissatisfaction compared to those in all other quartiles (
p < 0.01;
Figure 1a). The most significant difference was between the second tallest and shortest quartiles (
p < 0.001). There were no other significant differences in height dissatisfaction between other quartiles.
Similarly, results showed that there was a statistically significant difference in treatment due to height across height quartiles,
F(3168) = 4.49,
p = 0.005, η
p2 = 0.08, with additional post hoc pairwise comparisons determining that women in the shortest quartile reported significantly lower treatment due to height scores (indicating a greater belief that they were treated poorly) compared to those in the tallest (
p = 0.023) and second tallest (
p = 0.015) quartile (
Figure 1b). There were no other significant differences in treatment due to height between other quartiles.
In relation to H3, results showed that there was a significant negative correlation between height dissatisfaction and quality of life, meaning that women with greater height dissatisfaction tended to report poorer quality of life. However, there was no significant negative correlation between height dissatisfaction and drive for thinness or muscularity (
Table 1).
Exploratory Analyses
Results also showed that 57% of women would not date a romantic partner that was shorter than them. When considering trends for this preference across height quartiles, taller women were generally more accepting of dating a shorter partner compared to shorter women (
Table 2).
Additionally, 84% of women preferred a romantic partner that is taller than them, 11% had no preference, 4% preferred a partner of equal height, and 1% preferred a partner that was shorter than them. These preferences were generally consistent across height quartiles (
Table 3).
4. Discussion
The present study aimed to examine the link between height and height dissatisfaction in Australian women, and the extent to which height and height dissatisfaction relate to body dissatisfaction and quality of life. Additionally, the present study aimed to explore the height preferences of oneself and romantic partners in Australian women.
The first hypothesis is that there would be a significant difference between the reported actual height of participants, and their ideal height (the height that they would like to be), which was supported. On average, results showed that women in our sample wanted to be approximately 2 cm taller than their reported height. This result was comparable to that of Griffiths and colleagues [
3], who found that on average, the sexual minority men in their sample aspired to be 3 cm taller than their actual height. Notably, the majority of our sample (61%) idealized a height that was different from their current height, and 45% of participants reported wanting to be taller. These results inform our understanding of what constitutes the ideal height for Australian women (i.e., 167.65 cm), and demonstrate that, working through the lens of social comparison theory [
23], the majority of women likely engage in height-related upward comparisons, and that the majority of these upward comparisons are likely directed toward taller women.
The second hypothesis, that self-reported height would be positively correlated with height dissatisfaction, and women of taller stature would report that they believe they are treated worse due to their height, compared to shorter women, was not supported. Surprisingly, we found the opposite effect: that shorter women tended to be more dissatisfied with their height and were more likely to believe that they were treated poorly due to their height. Our one-way ANOVAs examining height dissatisfaction, and the extent to which women believed they were treated poorly due to their height across height quartiles evidenced that women in the shortest quartile were the drivers of both of these correlations. Thus, results suggest that analogous to men [
3,
8,
9], it is women with shorter stature who are most dissatisfied with their height and who are more likely to perceive that they are treated poorly due to their height. This result might be accounted for by the shifting nature of sex roles, femininity, and ideal female bodies. Our prediction that taller women would be more dissatisfied with their height was predicated on (potentially outdated) notions of femininity and the perception that taller women would feel that they were less likely to fit into height-based preferences within a romantic relationship [
10,
11,
12]. Our results suggest, however, that taller women are just as satisfied with their height as women of average height. This result appears to mirror that of Lever and colleagues [
37], who, utilizing a survey of 30,347 adult US women, showed that the majority of tall women were satisfied with their height and that women of shorter stature tended to be more dissatisfied with their height. One potential explanation for this result is that the perceived disadvantages of tall stature may be offset by advantages. Interestingly, taller women have been shown to have greater occupational income [
38], a greater authority status in the workplace [
39], and higher partner education and occupation status [
40]. Additionally, Lever and colleagues [
30] theorized that taller stature may be becoming a more desired factor in female body image, as an increasing number of tall female athletes and public figures are highly visible in the media [
41,
42]. These findings also help support our consideration of height within a social comparison theory framework. It is likely that women of shorter stature are making more upward comparisons to women with a taller, more ideal height, and thus are experiencing increasing levels of height dissatisfaction relative to average and taller stature women [
23,
24].
The third hypothesis, that there would be a positive correlation between height dissatisfaction and drive for thinness and drive for muscularity, respectively, and a negative correlation between height dissatisfaction and quality of life was partially supported. Results showed no significant relationship between height dissatisfaction and drive for thinness and muscularity. Thus, unlike men [
3,
8,
9], women’s height and height dissatisfaction appear to be unrelated to the drive for thinness and muscularity.
Notably, height dissatisfaction was negatively correlated with quality of life, meaning that women who were dissatisfied with their height were more likely to report a poorer quality of life. These results corresponded with Griffiths and colleagues’ [
3] findings in sexual minority men, and, although causality cannot be inferred, demonstrate that height and height dissatisfaction may play a role in significantly impacting the day-to-day lives of Australian women. Interestingly, height itself was not associated with quality of life, suggesting that women’s attitudes and the associated effect relating to their height is more important than height itself. Ultimately, these results underscore that height dissatisfaction is an important component of body image for women in that it is significantly associated with women’s perception of their position in life. These results also place a greater emphasis on objectification theory and that a more negative self-evaluation could result in poorer quality of life, especially as height is a largely unchangeable factor [
22].
Our exploratory analysis showed that over half (57%) of our sample would not date a romantic partner that was shorter than them, Notably, taller women seemed to report a more accepting attitude, with 56% of women in the tallest quartile of our sample reporting that they would date a shorter partner. This was largely in contrast to the shorter two qualities of our sample, for whom only a third would date a shorter partner. Additionally, the vast majority (84%) of women preferred dating a romantic partner that was taller than them. This preference was consistent across all height quartiles. These results largely correspond to past studies investigating women’s romantic partner preferences [
10,
11,
12]. Limitations of the present study are noted. First, our study utilized WEIRD participants [
43]. Thus, the generalizability of our results may be limited. Second, no data relating to sexual identity or sexuality was obtained, therefore romantic partner height preferences cannot be generalized to specific gendered partners. Third, the present study relied on self-reported measures of height, which may have compromised the accuracy of reporting. Fourth, participants were provided with information about the nature of the study and thus it is unknown if demanded characteristics influenced participants’ responses regarding their height attitudes and created a bias in the result, thus results should be considered with caution and replication is needed. However, this is unlikely to have significantly limited the validity of our study, as generally women only marginally under or overestimate their height [
44].
5. Conclusions
The present study aimed to examine the link between height, height dissatisfaction, and body dissatisfaction-related constructs in Australian women. Results showed that compared to men, women aspired to be taller than they were, and women of shorter stature tended to be more dissatisfied with their height and believed that they were treated poorly due to their height. Results, however, found no association between height dissatisfaction and other facets of body dissatisfaction but did implicate height and height dissatisfaction as important factors in relating to the quality of life. Future studies should consider height dissatisfaction as a potential contributing factor to poor quality of life and negative affect. It would also be important to investigate whether height dissatisfaction in both male and female populations was correlated with psychological distress, anxiety, depression, self-esteem, and other concepts that relate to one’s self-perception. Additionally, with limited research within the field of height dissatisfaction in females, replication and longitudinal studies are needed. Finally, greater body dissatisfaction can be associated with a higher risk for the development of eating disorders, and thus the importance of increasing research within this area as a preventative measure for eating disorder development. Body dissatisfaction, especially height dissatisfaction, should also be incorporated into eating disorder intervention development as negative self-evaluation may perpetuate disordered eating behaviors.





{kind=link}