
Styletubation versus Laryngoscopy: A New Paradigm for Routine Tracheal Intubation

Abstract
:1. History of Laryngoscopy
2. A Paradigm Shift of Videolaryngoscopy
3. Evolution of Optic/Video Intubating Tools
4. Styletubation
5. Cases Presentation
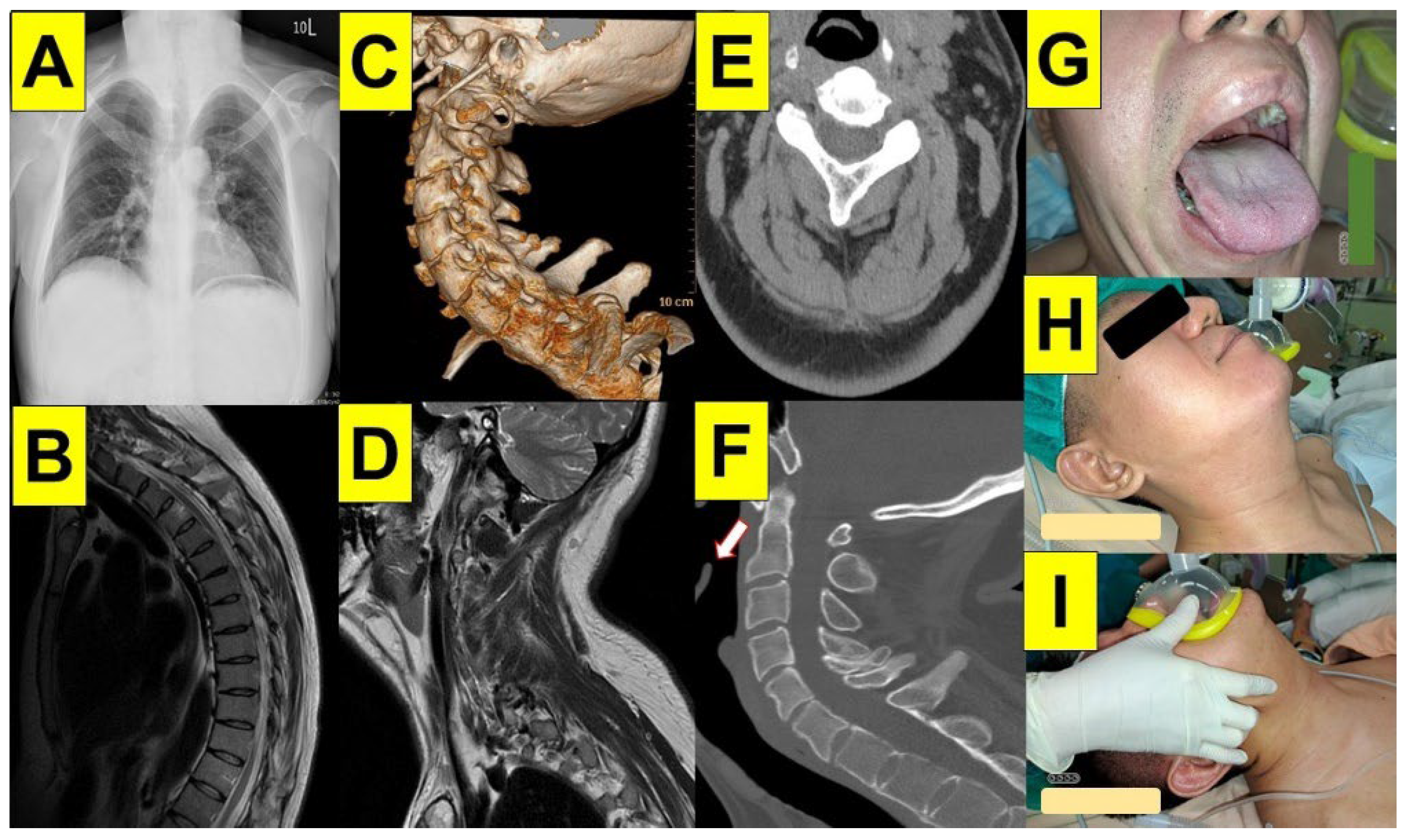
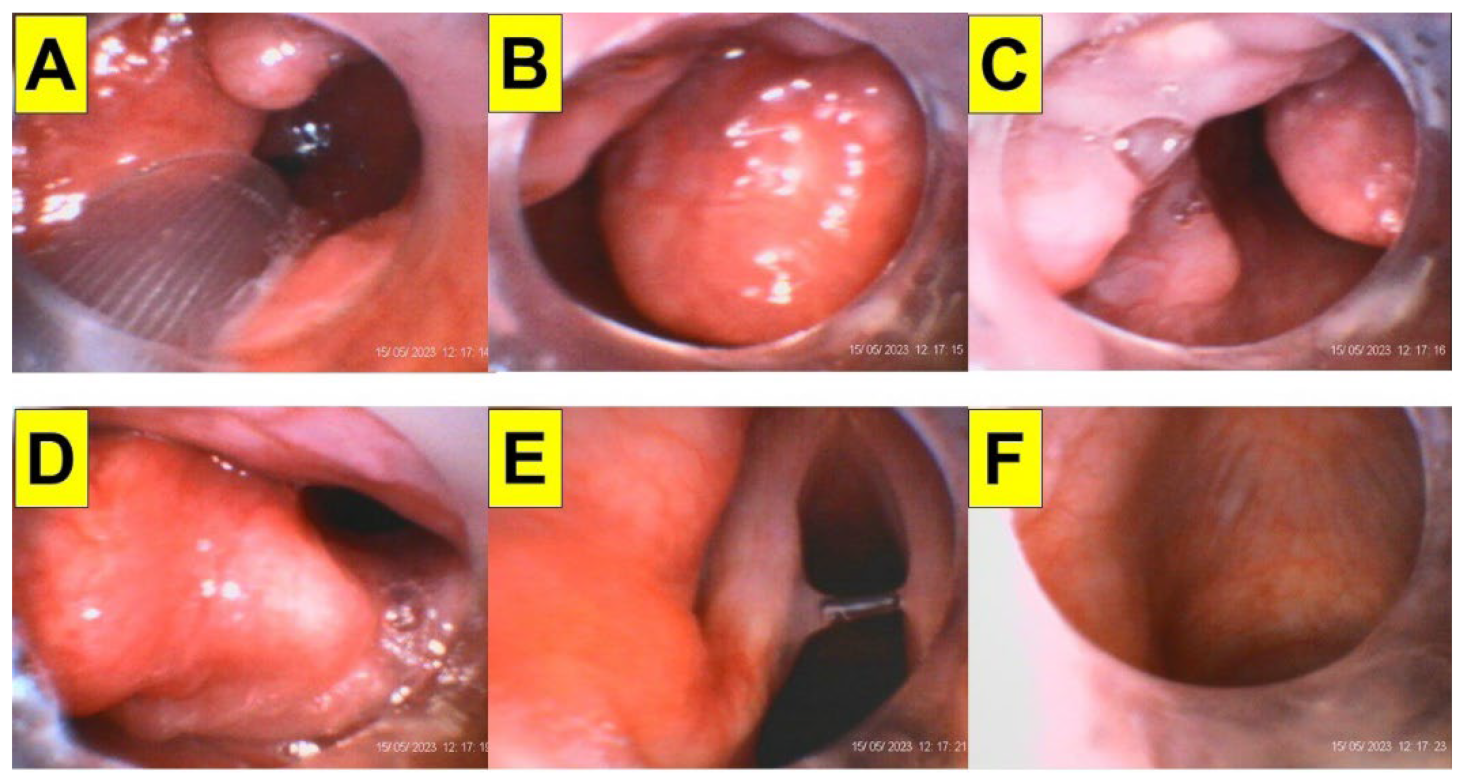
5.1. Awake FOB or Styletubation for Emergency Tracheostomy
5.2. Styletubation Grading System for Tracheal Intubation
5.3. Intubating Time and Ease of Maneuverability as Outcome Parameters
5.4. Ankylosing Spondylitis
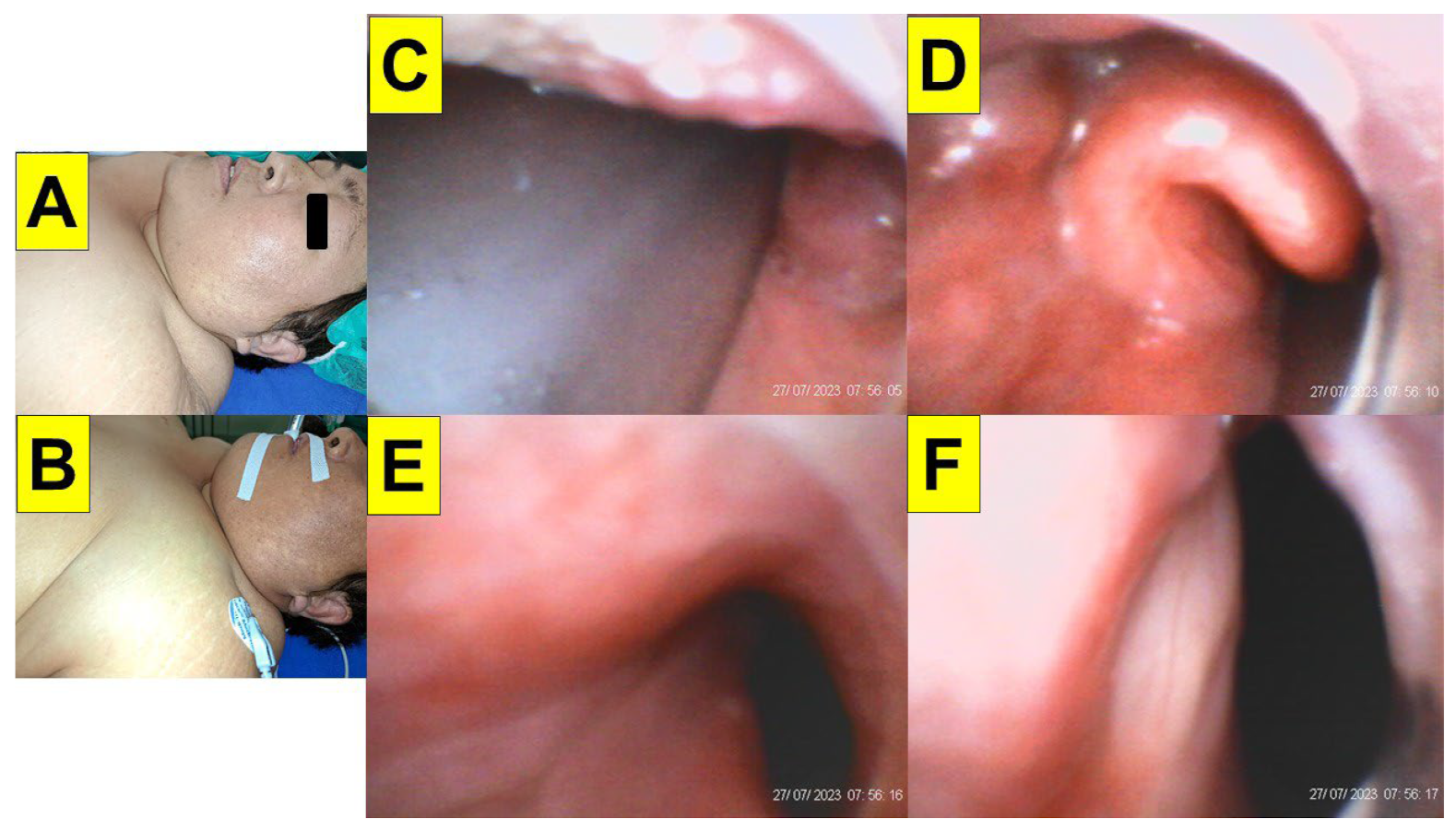
5.5. Obesity
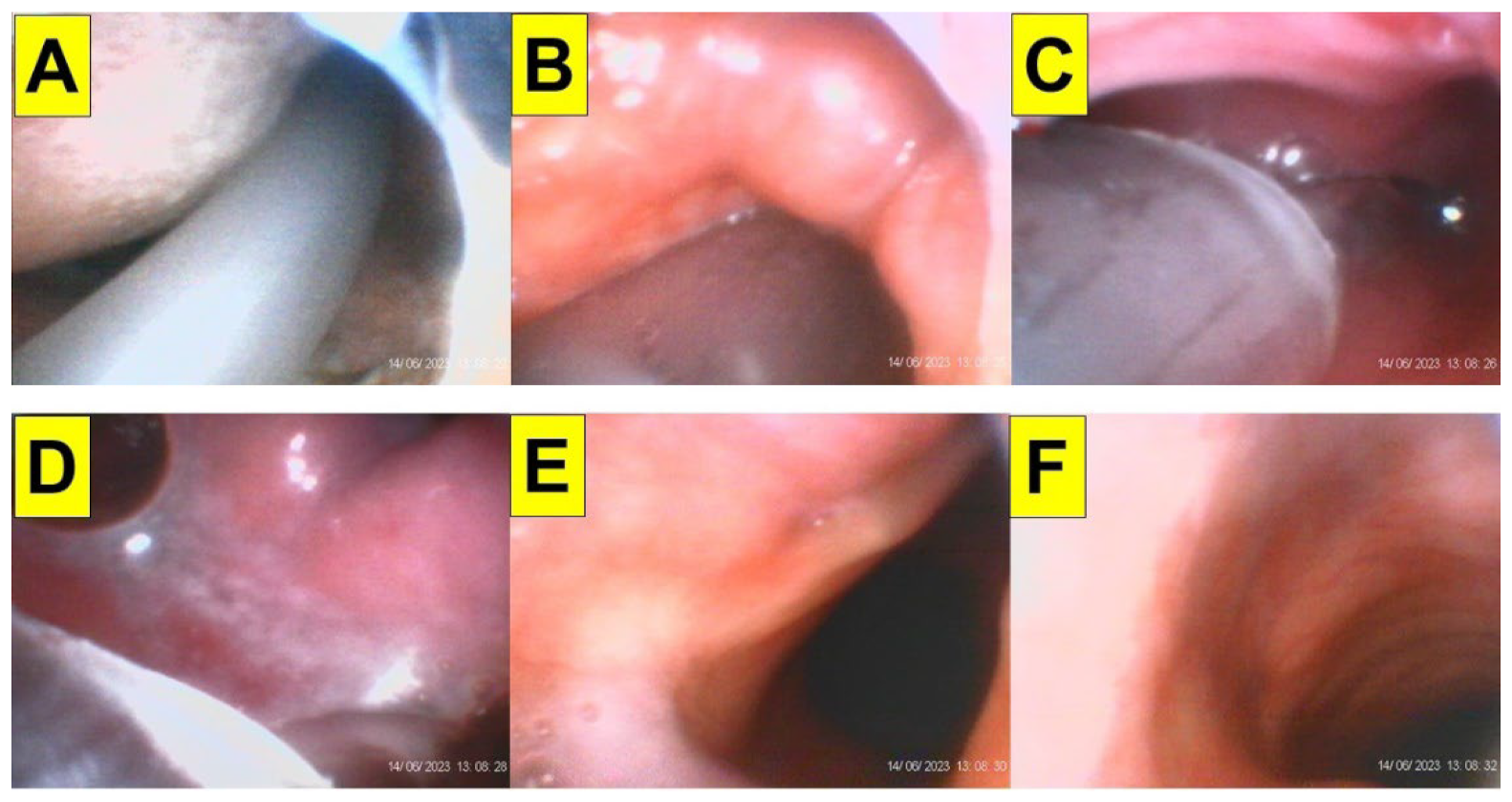
5.6. Rapid Sequence Induction/Intubation
5.7. COVID-19 Pandemic
5.8. Combined VL and VS
5.9. The Learning Curve
6. Time for Universal Practice of Styletubation?
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pieters, B.M.; Eindhoven, G.B.; Acott, C.; van Zundert, A.A. Pioneers of laryngoscopy: Indirect, direct and video laryngoscopy. Anaesth. Intensive Care 2015, 43, 4–11. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, J.W. Laryngoscope design and the difficult adult tracheal intubation. Can. J. Anaesth. 1989, 36, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Macintosh, R.R. A new laryngoscope. Lancet 1943, 241, 205. [Google Scholar] [CrossRef]
- Knill, R.L. Difficult laryngoscopy made easy with a “BURP”. Can. J. Anaesth. 1993, 40, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Benumof, J.L.; Cooper, S.D. Quantitative improvement in laryngoscopic view by optimal external laryngeal manipulation. J. Clin. Anesth. 1996, 8, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Takahata, O.; Kubota, M.; Mamiya, K.; Akama, Y.; Nozaka, T.; Matsumoto, H.; Ogawa, H. The efficacy of the “BURP” maneuver during a difficult laryngoscopy. Anesth. Analg. 1997, 84, 419–421. [Google Scholar] [CrossRef]
- Yu, T.; Wu, R.R.; Longhini, F.; Wang, B.; Wang, M.F.; Yang, F.F.; Hua, F.Z.; Yao, W.D.; Jin, X.J. The “BURP” maneuver improves the glottic view during laryngoscopy but remains a difficult procedure. J. Int. Med. Res. 2020, 48, 300060520925325. [Google Scholar] [CrossRef]
- Levitan, R.M.; Kinkle, W.C.; Levin, W.J.; Everett, W.W. Laryngeal view during laryngoscopy: A randomized trial comparing cricoid pressure, backward-upward-rightward pressure, and bimanual laryngoscopy. Ann. Emerg. Med. 2006, 47, 548–555. [Google Scholar] [CrossRef]
- Krantz, M.A.; Poulos, J.G.; Chaouki, K.; Adamek, P. The laryngeal lift: A method to facilitate endotracheal intubation. J. Clin. Anesth. 1993, 5, 297–301. [Google Scholar] [CrossRef]
- Bannister, F.B.; Macbeth, R.G. Direct laryngoscopy and tracheal intubation. Lancet 1944, 244, 651–654. [Google Scholar] [CrossRef]
- Takenaka, I.; Aoyama, K.; Iwagaki, T.; Ishimura, H.; Kadoya, T. The sniffing position provides greater occipito-atlanto-axial angulation than simple head extension: A radiological study. Can. J. Anaesth. 2007, 54, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Greenland, K.B.; Eley, V.; Edwards, M.J.; Allen, P.; Irwin, M.G. The origins of the sniffing position and the Three Axes Alignment Theory for direct laryngoscopy. Anaesth. Intensive Care 2008, 36, 23–27. [Google Scholar] [CrossRef] [PubMed]
- El-Orbany, M.; Woehlck, H.; Salem, M.R. Head and neck position for direct laryngoscopy. Anesth. Analg. 2011, 113, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Levitan, R.M.; Mechem, C.C.; Ochroch, E.A.; Shofer, F.S.; Hollander, J.E. Head-elevated laryngoscopy position: Improving laryngeal exposure during laryngoscopy by increasing head elevation. Ann. Emerg. Med. 2003, 41, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; Weightman, W.M. Laryngoscopy force in the sniffing position compared to the extension-extension position. Anaesthesia 2008, 63, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Adnet, F.; Borron, S.W.; Dumas, J.L.; Lapostolle, F.; Cupa, M.; Lapandry, C. Study of the “sniffing position” by magnetic resonance imaging. Anesthesiology 2001, 94, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Greenland, K.B. A proposed model for direct laryngoscopy and tracheal intubation. Anaesthesia 2008, 63, 156–161. [Google Scholar] [CrossRef]
- Chou, H.C.; Wu, T.L. Rethinking the three axes alignment theory for direct laryngoscopy. Acta Anaesthesiol. Scand. 2001, 45, 261–262. [Google Scholar] [CrossRef]
- Chou, H.C.; Wu, T.L. A reconsideration of three axes alignment theory and sniffing position. Anesthesiology 2002, 97, 753–754. [Google Scholar] [CrossRef]
- Joffe, A.M.; Aziz, M.F.; Posner, K.L.; Duggan, L.V.; Mincer, S.L.; Domino, K.B. Management of difficult tracheal intubation: A closed claims analysis. Anesthesiology 2019, 131, 818–829. [Google Scholar] [CrossRef]
- Cooper, R.M. Use of a new videolaryngoscope (GlideScope®) in the management of a difficult airway. Can. J. Anaesth. 2003, 50, 611–613. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.M.; Pacey, J.A.; Bishop, M.J.; McCluskey, S.A. Early clinical experience with a new videolaryngoscope (GlideScope®) in 728 patients. Can. J. Anaesth. 2005, 52, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Niforopoulou, P.; Pantazopoulos, I.; Demestiha, T.; Koudouna, E.; Xanthos, T. Video-laryngoscopes in the adult airway management: A topical review of the literature. Acta Anaesthesiol. Scand. 2010, 54, 1050–1061. [Google Scholar] [CrossRef]
- Hansel, J.; Rogers, A.M.; Lewis, S.R.; Cook, T.M.; Smith, A.F. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation: A Cochrane systematic review and meta-analysis update. Br. J. Anaesth. 2022, 129, 612–623. [Google Scholar] [CrossRef] [PubMed]
- Paolini, J.B.; Donati, F.; Drolet, P. Review article: Video-laryngoscopy: Another tool for difficult intubation or a new paradigm in airway management? Can. J. Anaesth. 2013, 60, 184–191. [Google Scholar] [CrossRef] [PubMed]
- De Jong, A.; Sfara, T.; Pouzeratte, Y.; Pensier, J.; Rolle, A.; Chanques, G.; Jaber, S. Videolaryngoscopy as a first-intention technique for tracheal intubation in unselected surgical patients: A before and after observational study. Br. J. Anaesth. 2022, 129, 624–634. [Google Scholar] [CrossRef] [PubMed]
- Prekker, M.E.; Driver, B.E.; Trent, S.A.; Resnick-Ault, D.; Seitz, K.P.; Russell, D.W.; Gaillard, J.P.; Latimer, A.J.; Ghamande, S.A.; Gibbs, K.W.; et al. Video versus direct laryngoscopy for tracheal intubation of critically ill adults. N. Engl. J. Med. 2023, 389, 418–429. [Google Scholar] [CrossRef]
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; et al. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology 2022, 136, 31–81. [Google Scholar] [CrossRef]
- Berci, G.; Katz, R. Optical stylet: An aid to intubation and teaching. Ann. Otol. Rhinol. Laryngol. 1979, 88, 828–831. [Google Scholar] [CrossRef]
- Matek, J.; Kolek, F.; Klementova, O.; Michalek, P.; Vymazal, T. Optical devices in tracheal intubation-State of the art in 2020. Diagnostics 2021, 11, 575. [Google Scholar] [CrossRef]
- Bonfils, P. Difficult intubation in Pierre-Robin children, a new method: The retromolar route. Anaesthesist 1983, 32, 363–367. [Google Scholar] [PubMed]
- Thong, S.Y.; Wong, T.G. Clinical uses of the Bonfils Retromolar Intubation Fiberscope: A review. Anesth. Analg. 2012, 115, 855–866. [Google Scholar] [CrossRef]
- Hung, O.R.; Pytka, S.; Morris, I.; Murphy, M.; Launcelott, G.; Stevens, S.; MacKay, W.; Stewart, R.D. Clinical trial of a new lightwand device (Trachlight) to intubate the trachea. Anesthesiology 1995, 83, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Agrò, F.; Hung, O.R.; Cataldo, R.; Carassiti, M.; Gherardi, S. Lightwand intubation using the TrachlightTM: A brief review of current knowledge. Can. J. Anaesth. 2001, 48, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Shikani, A.H. New “seeing” stylet-scope and method for the management of the difficult airway. Otolaryngol. Head Neck Surg. 1999, 120, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Greenland, K.B.; Liu, G.; Tan, H.; Edwards, M.; Irwin, M.G. Comparison of the Levitan FPS Scope and the single-use bougie for simulated difficult intubation in anaesthetised patients. Anaesthesia 2007, 62, 509–515, Erratum in Anaesthesia 2007, 62, 644. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.B.; Luk, H.N. Plastic sheet and video intubating stylet: A technical note. Asian J. Anesthesiol. 2021, 59, 117–121. [Google Scholar] [CrossRef]
- Tsay, P.J.; Yang, C.P.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-assisted intubating stylet technique for difficult intubation: A Case Series Report. Healthcare 2022, 10, 741. [Google Scholar] [CrossRef]
- Shih, T.L.; Koay, K.P.; Hu, C.Y.; Luk, H.N.; Qu, J.Z.; Shikani, A. The use of the Shikani video-assisted intubating stylet technique in patients with restricted neck mobility. Healthcare 2022, 10, 1688. [Google Scholar] [CrossRef]
- Yang, C.P.; Luk, H.N.; Qu, J.Z.; Shikani, A. The use of a video-assisted intubating stylet technique in a critically ill and contagious COVID-19 patient. Healthcare 2022, 10, 388. [Google Scholar] [CrossRef]
- Huang, C.H.; Su, I.M.; Jhuang, B.J.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-assisted stylet intubation with a plastic sheet barrier, a safe and simple technique for tracheal intubation of COVID-19 patients. Healthcare 2022, 10, 1105. [Google Scholar] [CrossRef] [PubMed]
- Jhuang, B.J.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-twin technique for airway management, combining video-intubating stylet with videolaryngoscope: A case series report and review of the literature. Healthcare 2022, 10, 2175. [Google Scholar] [CrossRef] [PubMed]
- Luk, H.N.; Luk, H.N.; Qu, J.Z.; Shikani, A. A paradigm shift of airway management: The role of video-assisted intubating stylet technique. In Advances in Tracheal Intubation; Lovich-Sapola, J., Ed.; IntechOpen [Internet]: London, UK, 2022. [Google Scholar] [CrossRef]
- Lan, C.H.; Luk, H.N.; Qu, J.Z.; Shikani, A. An approach to improve the effectiveness of the video-assisted intubating stylet technique for tracheal intubation: A case series report. Healthcare 2023, 11, 891. [Google Scholar] [CrossRef] [PubMed]
- Luk, H.N.; Qu, J.Z.; Shikani, A. Styletubation: The paradigmatic role of video-assisted intubating stylet technique for routine tracheal intubation. Asian J. Anesthesiol. 2023, preprint. [Google Scholar] [CrossRef]
- Luk, H.N.; Qu, J.Z.; Shikani, A. Styletubation for routine tracheal intubation for ear-nose-throat surgical procedures. Ann. Otol. Head Neck Surg. 2023, 2, 1–13. [Google Scholar]
- Wu, B.G.; Luk, H.N.; Qu, J.Z.; Shikani, A. Styletubation in bariatric surgery: A case report. Healthcare 2023, 11, 2256. [Google Scholar] [CrossRef]
- Pan, H.-S.; Corey, T.; Luk, H.-N.; Qu, J.Z.; Shikani, A. Combined styletubation with videolaryngoscopy for tracheal intubation in patients undergoing thyroidectomy with intraoperative neuromonitoring. Anesth. Res. 2023, 1, 8–23. [Google Scholar] [CrossRef]
- Hall, C.E.; Shutt, L.E. Nasotracheal intubation for head and neck surgery. Anaesthesia 2003, 58, 249–256. [Google Scholar] [CrossRef]
- Chowdhury, N.; Cagliani, J.A.; Loyola, A.; SchianodiCola, J. Massive ameloblastoma requiring awake nasal fiberoptic intubation. Cureus 2023, 15, e40760. [Google Scholar] [CrossRef]
- Tsukamoto, M.; Hitosugi, T.; Yokoyama, T. Awake fiberoptic nasotracheal intubation for patients with difficult airway. J. Dent. Anesth. Pain Med. 2018, 18, 301–304. [Google Scholar] [CrossRef]
- Hsu, H.T.; Lin, C.H.; Tseng, K.Y.; Shen, Y.C.; Chen, C.H.; Chuang, W.M.; Cheng, K.I. Trachway in assistance of nasotracheal intubation with a preformed nasotracheal tube in patients undergoing oral maxillofacial surgery. Br. J. Anaesth. 2014, 113, 720–721. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.C.; Tseng, K.Y.; Shen, Y.C.; Lin, C.H.; Hsu, C.W.; Hsu, H.J.; Lu, I.C.; Cheng, K.I. Nasotracheal intubation in patients with limited mouth opening: A comparison between fibreoptic intubation and the Trachway®. Anaesthesia 2016, 71, 31–38. [Google Scholar] [CrossRef]
- Cheng, T.; Wang, L.K.; Wu, H.Y.; Yang, X.D.; Zhang, X.; Jiao, L. Shikani Optical Stylet for awake nasal intubation in patients undergoing head and neck surgery. Laryngoscope 2021, 131, 319–325. [Google Scholar] [CrossRef]
- Hsieh, S.W.; Hung, K.C. Trachway® stylet: A perfect tool for nasotracheal intubation? Anaesthesia 2016, 71, 724. [Google Scholar] [CrossRef] [PubMed]
- Gemma, M.; Buratti, L.; Di Santo, D.; Calvi, M.R.; Ravizza, A.; Bondi, S.; Bussi, M.; Beretta, L. Pre-operative transnasal endoscopy as a predictor of difficult airway: A prospective cohort study. Eur. J. Anaesthesiol. 2020, 37, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Sasu, P.B.; Pansa, J.I.; Stadlhofer, R.; Wünsch, V.A.; Loock, K.; Buscher, E.K.; Dankert, A.; Ozga, A.K.; Zöllner, C.; Petzoldt, M. Nasendoscopy to predict difficult videolaryngoscopy: A multivariable model development study. J. Clin. Med. 2023, 12, 3433. [Google Scholar] [CrossRef]
- Barclay-Steuart, A.; Großhennig, H.L.; Sasu, P.; Wünsch, V.A.; Stadlhofer, R.; Berger, J.; Stark, M.; Sehner, S.; Zöllner, C.; Petzoldt, M. Transnasal videoendoscopy for preoperative airway risk stratification: Development and validation of a multivariable risk prediction model. Anesth. Analg. 2023, 136, 1164–1173. [Google Scholar] [CrossRef]
- Ahmad, I.; El-Boghdadly, K.; Bhagrath, R.; Hodzovic, I.; McNarry, A.F.; Mir, F.; O’Sullivan, E.P.; Patel, A.; Stacey, M.; Vaughan, D. Difficult Airway Society guidelines for awake tracheal intubation (ATI) in adults. Anaesthesia 2020, 75, 509–528. [Google Scholar] [CrossRef]
- Asai, T.; Shingu, K. Difficulty in advancing a tracheal tube over a fibreoptic bronchoscope: Incidence, causes and solutions. Br. J. Anaesth. 2004, 92, 870–881. [Google Scholar] [CrossRef]
- Touré, T.; Williams, S.R.; Kerouch, M.; Ruel, M. Patient factors associated with difficult flexible bronchoscopic intubation under general anesthesia: A prospective observational study. Can. J. Anaesth. 2020, 67, 706–714. [Google Scholar] [CrossRef]
- Detsky, M.E.; Jivraj, N.; Adhikari, N.K.; Friedrich, J.O.; Pinto, R.; Simel, D.L.; Wijeysundera, D.N.; Scales, D.C. Will this patient be difficult to intubate?: The rational clinical examination systematic review. JAMA 2019, 321, 493–503, Erratum in JAMA 2020, 323, 1194. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.; Pace, N.L.; Lee, A.; Hovhannisyan, K.; Warenits, A.M.; Arrich, J.; Herkner, H. Airway physical examination tests for detection of difficult airway management in apparently normal adult patients. Cochrane Database Syst. Rev. 2018, 5, CD008874. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.; Pace, N.L.; Lee, A.; Hovhannisyan, K.; Warenits, A.M.; Arrich, J.; Herkner, H. Bedside tests for predicting difficult airways: An abridged Cochrane diagnostic test accuracy systematic review. Anaesthesia 2019, 74, 915–928. [Google Scholar] [CrossRef] [PubMed]
- Mallampati, S.R. Clinical sign to predict difficult tracheal intubation (hypothesis). Can. Anaesth. Soc. J. 1983, 30, 316–317. [Google Scholar] [CrossRef] [PubMed]
- Mallampati, S.R.; Gatt, S.P.; Gugino, L.D.; Desai, S.P.; Waraksa, B.; Freiberger, D.; Liu, P.L. A clinical sign to predict difficult tracheal intubation: A prospective study. Can. Anaesth. Soc. J. 1985, 32, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Samsoon, G.L.; Young, J.R. Difficult tracheal intubation: A retrospective study. Anaesthesia 1987, 42, 487–490. [Google Scholar] [CrossRef]
- Mahmoodpoor, A.; Soleimanpour, H.; Golzari, S.E.; Nejabatian, A.; Pourlak, T.; Amani, M.; Hajmohammadi, S.; Hosseinzadeh, H.; Esfanjani, R.M. Determination of the diagnostic value of the modified Mallampati score, upper lip bite test and facial angle in predicting difficult intubation: A prospective descriptive study. J. Clin. Anesth. 2017, 37, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.C.; Ki, Y.; Kim, J.; Ahn, S.W. Ethnic considerations in the upper lip bite test: The reliability and validity of the upper lip bite test in predicting difficult laryngoscopy in Koreans. BMC Anesthesiol. 2019, 19, 9. [Google Scholar] [CrossRef]
- Wang, L.Y.; Zhang, K.D.; Zhang, Z.H.; Zhang, D.X.; Wang, H.L.; Qi, F. Evaluation of the reliability of the upper lip bite test and the modified Mallampati test in predicting difficult intubation under direct laryngoscopy in apparently normal patients: A prospective observational clinical study. BMC Anesthesiol. 2022, 22, 314. [Google Scholar] [CrossRef]
- Kar, S.; Senapati, L.K.; Samanta, P.; Satapathy, G.C. Predictive value of modified Mallampati test and upper lip bite test concerning Cormack and Lehane’s laryngoscopy grading in the anticipation of difficult intubation: A cross-sectional study at a tertiary care hospital, Bhubaneswar, India. Cureus 2022, 14, e28754. [Google Scholar] [CrossRef]
- Moslemi, F.; Khan, Z.H.; Alizadeh, E.; Khamnian, Z.; Eftekhar, N.; Hosseini, M.S.; Mahmoodpoor, A. Upper lip bite test compared to modified Mallampati test in predicting difficult airway in obstetrics: A prospective observational study. J. Perioper. Pract. 2023, 33, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Safavi, M.; Honarmand, A.; Zare, N. A comparison of the ratio of patient’s height to thyromental distance with the modified Mallampati and the upper lip bite test in predicting difficult laryngoscopy. Saudi J. Anaesth. 2011, 5, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Rao, K.V.N.; Dhatchinamoorthi, D.; Nandhakumar, A.; Selvarajan, N.; Akula, H.R.; Thiruvenkatarajan, V. Validity of thyromental height test as a predictor of difficult laryngoscopy: A prospective evaluation comparing modified Mallampati score, interincisor gap, thyromental distance, neck circumference, and neck extension. Indian J. Anaesth. 2018, 62, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Tian, T.; Li, X.; Jiang, T.; Xue, F. Use of the thyromental height test for prediction of difficult laryngoscopy: A systematic review and meta-analysis. J. Clin. Med. 2022, 11, 4906. [Google Scholar] [CrossRef] [PubMed]
- Amruthraju, C.M.; Shivaji, S.R.; Rooparani, K.; Vinay, R.; Vikas, K.N.; Deepak, T.S. The ratio of height to thyromental distance (RHTMD) and height to sternomental distance (RHSMD) as the predictive tests for difficult tracheal intubation. Cureus 2022, 14, e28734. [Google Scholar] [CrossRef]
- El-Ganzouri, A.R.; McCarthy, R.J.; Tuman, K.J.; Tanck, E.N.; Ivankovich, A.D. Preoperative airway assessment: Predictive value of a multivariate risk index. Anesth. Analg. 1996, 82, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Cook, T.M. A new practical classification of laryngeal view. Anaesthesia 2000, 55, 274–279. [Google Scholar] [CrossRef]
- Krage, R.; van Rijn, C.; van Groeningen, D.; Loer, S.A.; Schwarte, L.A.; Schober, P. Cormack-Lehane classification revisited. Br. J. Anaesth. 2010, 105, 220–227. [Google Scholar] [CrossRef]
- Levitan, R.M.; Ochroch, E.A.; Kush, S.; Shofer, F.S.; Hollander, J.E. Assessment of airway visualization: Validation of the percentage of glottic opening (POGO) scale. Acad. Emerg. Med. 1998, 5, 919–923. [Google Scholar] [CrossRef]
- Liu, D.X.; Ye, Y.; Zhu, Y.H.; Li, J.; He, H.Y.; Dong, L.; Zhu, Z.Q. Intubation of non-difficult airways using video laryngoscope versus direct laryngoscope: A randomized, parallel-group study. BMC Anesthesiol. 2019, 19, 75. [Google Scholar] [CrossRef]
- Serocki, G.; Bein, B.; Scholz, J.; Dörges, V. Management of the predicted difficult airway: A comparison of conventional blade laryngoscopy with video-assisted blade laryngoscopy and the GlideScope. Eur. J. Anaesthesiol. 2010, 27, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Misirlioglu, G.; Sen, O. Comparison of GlideScope video laryngoscopy and Macintosh laryngoscope in ear-nose and throat surgery. Ir. J. Med. Sci. 2016, 185, 729–733. [Google Scholar] [CrossRef] [PubMed]
- Van Zundert, A.; Maassen, R.; Lee, R.; Willems, R.; Timmerman, M.; Siemonsma, M.; Buise, M.; Wiepking, M. A Macintosh laryngoscope blade for videolaryngoscopy reduces stylet use in patients with normal airways. Anesth. Analg. 2009, 109, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Gayathri, B.; Mani, K.; Vishak, M.; John, J.; Srinivasan, R.G.; Mirunalini, G. Factors influencing the time of intubation using C-MAC D-Blade® video laryngoscope: An observational cross-sectional study. Cureus 2023, 15, e34050. [Google Scholar] [CrossRef] [PubMed]
- Singleton, B.N.; Morris, F.K.; Yet, B.; Buggy, D.J.; Perkins, Z.B. Effectiveness of intubation devices in patients with cervical spine immobilisation: A systematic review and network meta-analysis. Br. J. Anaesth. 2021, 126, 1055–1066. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Cho, Y.; Kim, W.; Choi, K.S.; Jang, B.H.; Shin, H.; Ahn, C.; Kim, J.G.; Na, M.K.; Lim, T.H.; et al. Comparisons of videolaryngoscopes for intubation undergoing general anesthesia: Systematic review and network meta-analysis of randomized controlled trials. J. Pers. Med. 2022, 12, 363. [Google Scholar] [CrossRef] [PubMed]
- Hansel, J.; Rogers, A.M.; Lewis, S.R.; Cook, T.M.; Smith, A.F. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation. Cochrane Database Syst. Rev. 2022, 4, CD011136. [Google Scholar] [CrossRef]
- Nedunchezhian, V.; Nedunchezhian, I.; Van Zundert, A. Clinically preferred videolaryngoscopes in airway management: An updated systematic review. Healthcare 2023, 11, 2383. [Google Scholar] [CrossRef]
- Amini, S.; Shakib, M. Hemodynamic changes following endotracheal intubation in patients undergoing cesarean section with general anesthesia: Application of glidescope® videolaryngoscope versus direct laryngoscope. Anesth. Pain Med. 2015, 5, e21836. [Google Scholar] [CrossRef]
- Pažur, I.; Maldini, B.; Hostić, V.; Ožegić, O.; Obraz, M. Comparison of Cormack Lehane grading system and intubation difficulty score in patients intubated by D-Blade Video and direct Macintosh laryngoscope: A randomized controlled study. Acta Clin. Croat. 2016, 55, 560–564. [Google Scholar] [CrossRef]
- Al-Ghamdi, A.A.; El Tahan, M.R.; Khidr, A.M. Comparison of the Macintosh, GlideScope®, Airtraq®, and King Vision™ laryngoscopes in routine airway management. Minerva Anestesiol. 2016, 82, 1278–1287. [Google Scholar] [PubMed]
- Akbar, S.H.; Ooi, J.S. Comparison between C-MAC video-laryngoscope and Macintosh direct laryngoscope during cervical spine immobilization. Middle East J. Anaesthesiol. 2015, 23, 43–50. [Google Scholar] [PubMed]
- Lim, Y.; Yeo, S.W. A comparison of the GlideScope® with the Macintosh laryngoscope for tracheal intubation in patients with simulated difficult airway. Anaesth. Intensive Care 2005, 33, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, D., Jr.; Filho, S.M.; Batista, S.; do Nascimento, P., Jr. Comparison of Macintosh and Airtraq™ laryngoscopes in obese patients placed in the ramped position. Anaesthesia 2012, 67, 980–985. [Google Scholar] [CrossRef] [PubMed]
- Foulds, L.T.; McGuire, B.E.; Shippey, B.J. A randomised cross-over trial comparing the McGrath® Series 5 videolaryngoscope with the Macintosh laryngoscope in patients with cervical spine immobilisation. Anaesthesia 2016, 71, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Yumul, R.; Elvir-Lazo, O.L.; White, P.F.; Sloninsky, A.; Kaplan, M.; Kariger, R.; Naruse, R.; Parker, N.; Pham, C.; Zhang, X.; et al. Comparison of three video laryngoscopy devices to direct laryngoscopy for intubating obese patients: A randomized controlled trial. J. Clin. Anesth. 2016, 31, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Kleine-Brueggeney, M.; Greif, R.; Schoettker, P.; Savoldelli, G.L.; Nabecker, S.; Theiler, L.G. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: A multicentre randomized controlled trial. Br. J. Anaesth. 2016, 116, 670–679. [Google Scholar] [CrossRef]
- Kleine-Brueggeney, M.; Buttenberg, M.; Greif, R.; Nabecker, S.; Theiler, L. Evaluation of three unchannelled videolaryngoscopes and the Macintosh laryngoscope in patients with a simulated difficult airway: A randomised, controlled trial. Anaesthesia 2017, 72, 370–378. [Google Scholar] [CrossRef]
- Zhu, H.; Liu, J.; Suo, L.; Zhou, C.; Sun, Y.; Jiang, H. A randomized controlled comparison of non-channeled king vision, McGrath MAC video laryngoscope and Macintosh direct laryngoscope for nasotracheal intubation in patients with predicted difficult intubations. BMC Anesthesiol. 2019, 19, 166. [Google Scholar] [CrossRef]
- Suzuki, K.; Kusunoki, S.; Tanigawa, K.; Shime, N. Comparison of three video laryngoscopes and direct laryngoscopy for emergency endotracheal intubation: A retrospective cohort study. BMJ Open 2019, 9, e024927. [Google Scholar] [CrossRef]
- Roh, G.U.; Kwak, H.J.; Lee, K.C.; Lee, S.Y.; Kim, J.Y. Randomized comparison of McGrath MAC videolaryngoscope, Pentax Airway Scope, and Macintosh direct laryngoscope for nasotracheal intubation in patients with manual in-line stabilization. Can. J. Anaesth. 2019, 66, 1213–1220. [Google Scholar] [CrossRef] [PubMed]
- Mallick, T.; Verma, A.; Jaiswal, S.; Haldar, M.; Sheikh, W.R.; Vishen, A.; Snehy, A.; Ahuja, R. Comparison of the time to successful endotracheal intubation using the Macintosh laryngoscope or KingVision video laryngoscope in the emergency department: A prospective observational study. Turk. J. Emerg. Med. 2020, 20, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Suppan, L.; Tramèr, M.R.; Niquille, M.; Grosgurin, O.; Marti, C. Alternative intubation techniques vs Macintosh laryngoscopy in patients with cervical spine immobilization: Systematic review and meta-analysis of randomized controlled trials. Br. J. Anaesth. 2016, 116, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Robitaille, A.; Williams, S.R.; Tremblay, M.H.; Guilbert, F.; Thériault, M.; Drolet, P. Cervical spine motion during tracheal intubation with manual in-line stabilization: Direct laryngoscopy versus GlideScope® videolaryngoscopy. Anesth. Analg. 2008, 106, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Houde, B.J.; Williams, S.R.; Cadrin-Chênevert, A.; Guilbert, F.; Drolet, P. A comparison of cervical spine motion during orotracheal intubation with the Trachlight® or the flexible fiberoptic bronchoscope. Anesth. Analg. 2009, 108, 1638–1643. [Google Scholar] [CrossRef] [PubMed]
- Paik, H.; Park, H.P. Randomized crossover trial comparing cervical spine motion during tracheal intubation with a Macintosh laryngoscope versus a C-MAC D-blade videolaryngoscope in a simulated immobilized cervical spine. BMC Anesthesiol. 2020, 20, 201. [Google Scholar] [CrossRef] [PubMed]
- Wetsch, W.A.; Spelten, O.; Hellmich, M.; Carlitscheck, M.; Padosch, S.A.; Lier, H.; Böttiger, B.W.; Hinkelbein, J. Comparison of different video laryngoscopes for emergency intubation in a standardized airway manikin with immobilized cervical spine by experienced anaesthetists. A randomized, controlled crossover trial. Resuscitation 2012, 83, 740–745. [Google Scholar] [CrossRef]
- Smereka, J.; Ladny, J.R.; Naylor, A.; Ruetzler, K.; Szarpak, L. C-MAC compared with direct laryngoscopy for intubation in patients with cervical spine immobilization: A manikin trial. Am. J. Emerg. Med. 2017, 35, 1142–1146. [Google Scholar] [CrossRef]
- Epaud, A.; Levesque, E.; Clariot, S. Dramatic cervical spine injury secondary to videolaryngoscopy in a patient suffering from ankylosing spondylitis. Anesthesiology 2021, 135, 495–496. [Google Scholar] [CrossRef]
- Gadomski, B.C.; Hindman, B.J.; Page, M.I.; Dexter, F.; Puttlitz, C.M. Intubation biomechanics: Clinical implications of computational modeling of intervertebral motion and spinal cord strain during tracheal intubation in an intact cervical spine. Anesthesiology 2021, 135, 1055–1065. [Google Scholar] [CrossRef]
- Gadomski, B.C.; Hindman, B.J.; Poland, M.J.; Page, M.I.; Dexter, F.; Puttlitz, C.M. Intubation biomechanics: Computational modeling to identify methods to minimize cervical spine motion and spinal cord strain during laryngoscopy and tracheal intubation in an intact cervical spine. J. Clin. Anesth. 2022, 81, 110909. [Google Scholar] [CrossRef] [PubMed]
- Hindman, B.J.; Santoni, B.G.; Puttlitz, C.M.; From, R.P.; Todd, M.M. Intubation biomechanics: Laryngoscope force and cervical spine motion during intubation with Macintosh and Airtraq laryngoscopes. Anesthesiology 2014, 121, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, C.V.; Thøgersen, B.; Afshari, A.; Christensen, A.L.; Eriksen, C.; Gätke, M.R. Awake fiberoptic or awake video laryngoscopic tracheal intubation in patients with anticipated difficult airway management: A randomized clinical trial. Anesthesiology 2012, 116, 1210–1216. [Google Scholar] [CrossRef] [PubMed]
- Yumul, R.; Elvir-Lazo, O.L.; White, P.F.; Durra, O.; Ternian, A.; Tamman, R.; Naruse, R.; Ebba, H.; Yusufali, T.; Wong, R.; et al. Comparison of the C-MAC video laryngoscope to a flexible fiberoptic scope for intubation with cervical spine immobilization. J. Clin. Anesth. 2016, 31, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, C.; Schneider, J.P.; Wallenborn, J.; Schaffranietz, L. Movement of the upper cervical spine during laryngoscopy: A comparison of the Bonfils intubation fibrescope and the Macintosh laryngoscope. Anaesthesia 2005, 60, 668–672. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.; Kim, B.G.; Lim, Y.J.; Jeon, Y.T.; Hwang, J.W.; Lee, S.Y.; Park, H.P. A comparison between the conventional and the laryngoscope-assisted lightwand intubation techniques in patients with cervical immobilization: A prospective randomized study. Anesth. Analg. 2017, 125, 854–859. [Google Scholar] [CrossRef]
- Nam, K.; Lee, Y.; Park, H.P.; Chung, J.; Yoon, H.K.; Kim, T.K. Cervical spine motion during tracheal intubation using an Optiscope versus the McGrath videolaryngoscope in patients with simulated cervical immobilization: A prospective randomized crossover study. Anesth. Analg. 2019, 129, 1666–1672. [Google Scholar] [CrossRef]
- Park, J.W.; An, S.; Park, S.; Nahm, F.S.; Han, S.H.; Kim, J.H. Comparison of a new Video Intubation Stylet and McGrath® MAC video laryngoscope for intubation in an airway manikin with normal airway and cervical spine immobilization scenarios by novice personnel: A randomized crossover study. Biomed Res. Int. 2021, 2021, 4288367. [Google Scholar] [CrossRef]
- Saricicek, V.; Mizrak, A.; Gul, R.; Goksu, S.; Cesur, M. GlideScope video laryngoscopy use tracheal intubation in patients with ankylosing spondylitis: A series of four cases and literature review. J. Clin. Monit. Comput. 2014, 28, 169–172. [Google Scholar] [CrossRef]
- Kumar, N.; Bindra, A.; Mahajan, C.; Yadav, N. Airway management in a patient of ankylosing spondylitis with traumatic cervical spine injury. Saudi J. Anaesth. 2015, 9, 327–329. [Google Scholar] [CrossRef]
- Hsieh, P.S.; Ma, H.P.; Wong, C.S.; Ong, J.R. Emergency tracheal intubation in an ankylosing spondylitis patient in a sitting position using an Airway Scope combined with face-to-face and digital intubation. J. Emerg. Med. 2018, 54, 674–677. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.C.; Lin, S.; He, H.F. Case report: Double visualization intubation strategy for patients with ankylosing spondylitis. Front. Med. 2022, 9, 659624. [Google Scholar] [CrossRef] [PubMed]
- Marrel, J.; Blanc, C.; Frascarolo, P.; Magnusson, L. Videolaryngoscopy improves intubation condition in morbidly obese patients. Eur. J. Anaesthesiol. 2007, 24, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Maassen, R.; Lee, R.; Hermans, B.; Marcus, M.; van Zundert, A. A comparison of three videolaryngoscopes: The Macintosh laryngoscope blade reduces, but does not replace, routine stylet use for intubation in morbidly obese patients. Anesth. Analg. 2009, 109, 1560–1565. [Google Scholar] [CrossRef]
- Moore, A.; El-Bahrawy, A.; El-Mouallem, E.; Lattermann, R.; Hatzakorzian, R.; LiPishan, W.; Schricker, T. Videolaryngoscopy or fibreoptic bronchoscopy for awake intubation of bariatric patients with predicted difficult airways—A randomised, controlled trial. Anaesthesia 2017, 72, 538–539. [Google Scholar] [CrossRef]
- Brozek, T.; Bruthans, J.; Porizka, M.; Blaha, J.; Ulrichova, J.; Michalek, P. A randomized comparison of non-channeled GlidescopeTM Titanium versus channeled KingVisionTM videolaryngoscope for orotracheal intubation in obese patients with BMI > 35 kg·m−2. Diagnostics 2020, 10, 1024. [Google Scholar] [CrossRef] [PubMed]
- Gaszynski, T.; Michalek, P.; Ratajczyk, P. A prospective comparative study of laryngeal glottic view using the Vie Scope® versus standard Macintosh laryngoscope in morbidly obese patients. Ther. Clin. Risk Manag. 2023, 19, 405–411. [Google Scholar] [CrossRef]
- Ruetzler, K.; Rivas, E.; Cohen, B.; Mosteller, L.; Martin, A.; Keebler, A.; Maheshwari, K.; Steckner, K.; Wang, M.; Praveen, C.; et al. McGrath video laryngoscope versus Macintosh direct laryngoscopy for intubation of morbidly obese patients: A randomized trial. Anesth. Analg. 2020, 131, 586–593. [Google Scholar] [CrossRef]
- Nassar, M.; Zanaty, O.M.; Ibrahim, M. Bonfils fiberscope vs GlideScope for awake intubation in morbidly obese patients with expected difficult airways. J. Clin. Anesth. 2016, 32, 101–105. [Google Scholar] [CrossRef]
- Bathory, I.; Granges, J.C.; Frascarolo, P.; Magnusson, L. Evaluation of the Video Intubation Unit in morbid obese patients. Acta Anaesthesiol. Scand. 2010, 54, 55–58. [Google Scholar] [CrossRef]
- Gaszynski, T.; Pietrzyk, M.; Szewczyk, T.; Gaszynska, E. A comparison of performance of endotracheal intubation using the Levitan FPS optical stylet or Lary-Flex videolaryngoscope in morbidly obese patients. Sci. World J. 2014, 2014, 207591. [Google Scholar] [CrossRef]
- Collins, J.S.; Lemmens, H.J.; Brodsky, J.B.; Brock-Utne, J.G.; Levitan, R.M. Laryngoscopy and morbid obesity: A comparison of the “sniff” and “ramped” positions. Obes. Surg. 2004, 14, 1171–1175. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Jang, E.A.; Hong, M.; Bae, H.B.; Kim, J. Ramped versus sniffing position in the videolaryngoscopy-guided tracheal intubation of morbidly obese patients: A prospective randomized study. Korean J. Anesthesiol. 2023, 76, 47–55. [Google Scholar] [CrossRef]
- Komasawa, N.; Kido, H.; Miyazaki, Y.; Tatsumi, S.; Minami, T. Cricoid pressure impedes tracheal intubation with the Pentax-AWS Airwayscope®: A prospective randomized trial. Br. J. Anaesth. 2016, 116, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Ma, D.; Li, B.; Yue, Y.; Xue, F. Video laryngoscopy does not improve the intubation outcomes in emergency and critical patients—A systematic review and meta-analysis of randomized controlled trials. Crit. Care 2017, 21, 288. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, S.; Maitra, S.; Baidya, D.K. A comparison between video laryngoscopy and direct laryngoscopy for endotracheal intubation in the emergency department: A meta-analysis of randomized controlled trials. J. Clin. Anesth. 2018, 47, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Sulser, S.; Ubmann, D.; Schlaepfer, M.; Brueesch, M.; Goliasch, G.; Seifert, B.; Spahn, D.R.; Ruetzler, K. C-MAC videolaryngoscope compared with direct laryngoscopy for rapid sequence intubation in an emergency department: A randomised clinical trial. Eur. J. Anaesthesiol. 2016, 33, 943–948. [Google Scholar] [CrossRef]
- Hossfeld, B.; Frey, K.; Doerges, V.; Lampl, L.; Helm, M. Improvement in glottic visualisation by using the C-MAC PM video laryngoscope as a first-line device for out-of-hospital emergency tracheal intubation: An observational study. Eur. J. Anaesthesiol. 2015, 32, 425–431. [Google Scholar] [CrossRef]
- Macke, C.; Gralla, F.; Winkelmann, M.; Clausen, J.-D.; Haertle, M.; Krettek, C.; Omar, M. Increased first pass success with C-MAC videolaryngoscopy in prehospital endotracheal intubation—A randomized controlled trial. J. Clin. Med. 2020, 9, 2719. [Google Scholar] [CrossRef]
- Hossfeld, B.; Thierbach, S.; Allgoewer, A.; Gaessler, H.; Helm, M. First pass success of tracheal intubation using the C-MAC PM videolaryngoscope as first-line device in prehospital cardiac arrest compared with other emergencies: An observational study. Eur. J. Anaesthesiol. 2021, 38, 806–812. [Google Scholar] [CrossRef]
- Szarpak, L.; Madziala, A.; Czekajlo, M.; Smereka, J.; Kaserer, A.; Dabrowski, M.; Madziala, M.; Yakubtsevich, R.; Ladny, J.R.; Ruetzler, K. Comparison of the UEScope videolaryngoscope with the Macintosh laryngoscope during simulated cardiopulmonary resuscitation: A randomized, cross-over, multi-center manikin study. Medicine 2018, 97, e12085. [Google Scholar] [CrossRef] [PubMed]
- Steffen, R.; Hischier, S.; Roten, F.M.; Huber, M.; Knapp, J. Airway management during ongoing chest compressions-direct vs. video laryngoscopy. A randomised manikin study. PLoS ONE 2023, 18, e0281186. [Google Scholar] [CrossRef] [PubMed]
- Birenbaum, A.; Hajage, D.; Roche, S.; Ntouba, A.; Eurin, M.; Cuvillon, P.; Rohn, A.; Compere, V.; Benhamou, D.; Biais, M.; et al. Effect of cricoid pressure compared with a sham procedure in the rapid sequence induction of anesthesia: The IRIS randomized clinical trial. JAMA Surg. 2019, 154, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Cook, T.M.; El-Boghdadly, K.; McGuire, B.; McNarry, A.F.; Patel, A.; Higgs, A. Consensus guidelines for managing the airway in patients with COVID-19: Guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia 2020, 75, 785–799. [Google Scholar] [CrossRef] [PubMed]
- Brewster, D.J.; Chrimes, N.; Do, T.B.; Fraser, K.; Groombridge, C.J.; Higgs, A.; Humar, M.J.; Leeuwenburg, T.J.; McGloughlin, S.; Newman, F.G.; et al. Consensus statement: Safe Airway Society principles of airway management and tracheal intubation specific to the COVID-19 adult patient group. Med. J. Aust. 2020, 212, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Foley, L.J.; Urdaneta, F.; Berkow, L.; Aziz, M.F.; Baker, P.A.; Jagannathan, N.; Rosenblatt, W.; Straker, T.M.; Wong, D.T.; Hagberg, C.A. Difficult airway management in adult Coronavirus Disease 2019 patients: Statement by the Society of Airway Management. Anesth. Analg. 2021, 133, 876–890. [Google Scholar] [CrossRef] [PubMed]
- Thiruvenkatarajan, V.; Wong, D.T.; Kothandan, H.; Sekhar, V.; Adhikary, S.D.; Currie, J.; Van Wijk, R.M. Airway management in the operating room and interventional suites in known or suspected COVID-19 adult patients: A practical review. Anesth. Analg. 2020, 131, 677–689. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.S.; Jeong, D.; Park, J.E.; Lee, G.T.; Shin, T.G.; Chang, H.; Kim, T.; Lee, S.U.; Yoon, H.; Cha, W.C.; et al. Endotracheal intubation using C-MAC video laryngoscope vs. direct laryngoscope while wearing personal protective equipment. J. Pers. Med. 2022, 12, 1720. [Google Scholar] [CrossRef]
- Gadek, L.; Szarpak, L.; Konge, L.; Dabrowski, M.; Telecka-Gadek, D.; Maslanka, M.; Drela, W.L.; Jachowicz, M.; Iskrzycki, L.; Bialka, S.; et al. Direct vs. video-laryngoscopy for intubation by paramedics of simulated COVID-19 patients under cardiopulmonary resuscitation: A randomized crossover trial. J. Clin. Med. 2021, 10, 5740. [Google Scholar] [CrossRef]
- Szarpak, L.; Peacock, F.W.; Rafique, Z.; Ladny, J.R.; Nadolny, K.; Malysz, M.; Dabrowski, M.; Chirico, F.; Smereka, J. Comparison of Vie Scope® and Macintosh laryngoscopes for intubation during resuscitation by paramedics wearing personal protective equipment. Am. J. Emerg. Med. 2022, 53, 122–126. [Google Scholar] [CrossRef]
- Wieczorek, P.; Szarpak, L.; Dabrowska, A.; Pruc, M.; Navolokina, A.; Raczynski, A.; Smereka, J. A comparison of the bébé VieScope™ and direct laryngoscope for use while wearing PPE-AGP: A randomized crossover simulation trial. Children 2022, 9, 1774. [Google Scholar] [CrossRef] [PubMed]
- Kluj, P.; Fedorczak, A.; Fedorczak, M.; Gaszyński, T.; Kułak, C.; Wasilewski, M.; Znyk, M.; Bartczak, M.; Ratajczyk, P. Comparison of three video laryngoscopes and direct laryngoscopy for emergency endotracheal intubation while wearing PPE-AGP: A randomized, crossover, simulation trial. Healthcare 2023, 11, 884. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.Y.; Yiang, G.T.; Ke, J.Y.; Chen, C.S.; Lin, P.C.; Chen, Y.L. Role of Trachway versus conventional modes of intubation in difficult airway management in COVID-19 setups. Emerg. Med. Int. 2021, 2021, 6614523. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.L.; Huang, C.H.; Luk, H.N.; Tsai, P.B. Adaptation to the plastic barrier sheet to facilitate intubation during the COVID-19 pandemic. Anesth. Analg. 2020, 131, e97–e99. [Google Scholar] [CrossRef] [PubMed]
- Luk, H.N.; Yang, Y.L.; Tsai, P.B. Application of plastic sheet barrier and video intubating stylet to protect tracheal intubators during Coronavirus Disease 2019 pandemic: A Taiwan experience. Cell Transplant. 2021, 30, 0963689720987527. [Google Scholar] [CrossRef] [PubMed]
- Stacey, M.R.; Rassam, S.; Sivasankar, R.; Hall, J.E.; Latto, I.P. A comparison of direct laryngoscopy and jaw thrust to aid fibreoptic intubation. Anaesthesia 2005, 60, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Matioc, A.A. Use of the Airtraq® with a fibreoptic bronchoscope in a difficult intubation outside the operating room. Can. J. Anaesth. 2008, 55, 561–562. [Google Scholar] [CrossRef]
- Sharma, D.; Kim, L.J.; Ghodke, B. Successful airway management with combined use of Glidescope® videolaryngoscope and fiberoptic bronchoscope in a patient with Cowden syndrome. Anesthesiology 2010, 113, 253–255. [Google Scholar] [CrossRef]
- Gómez-Ríos, M.A.; Nieto Serradilla, L. Combined use of an Airtraq® optical laryngoscope, Airtraq video camera, Airtraq wireless monitor, and a fibreoptic bronchoscope after failed tracheal intubation. Can. J. Anaesth. 2011, 58, 411–412. [Google Scholar] [CrossRef]
- Lenhardt, R.; Burkhart, M.T.; Brock, G.N.; Kanchi-Kandadai, S.; Sharma, R.; Akça, O. Is video laryngoscope-assisted flexible tracheoscope intubation feasible for patients with predicted difficult airway? A prospective, randomized clinical trial. Anesth. Analg. 2014, 118, 1259–1265. [Google Scholar] [CrossRef]
- Van Zundert, A.A.; Pieters, B.M. Combined technique using videolaryngoscopy and Bonfils for a difficult airway intubation. Br. J. Anaesth. 2012, 108, 327–328. [Google Scholar] [CrossRef]
- Pieters, B.M.; Theunissen, M.; van Zundert, A.A. Macintosh blade videolaryngoscopy combined with rigid Bonfils intubation endoscope offers a suitable alternative for patients with difficult airways. Anesth. Analg. 2018, 126, 988–994. [Google Scholar] [CrossRef] [PubMed]
- Levitan, R.M. Design rationale and intended use of a short optical stylet for routine fiberoptic augmentation of emergency laryngoscopy. Am. J. Emerg. Med. 2006, 24, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Xia, Y.M.; Fan, Q.W. Application of UE visual laryngoscope combined with Seeing Optical Stylet to tracheal intubation in obese patients. J. Shanghai Jiao Tong Univ. 2021, 41, 70–73. [Google Scholar] [CrossRef]
- Chiu, W.C.; Wu, Z.F.; Lai, M.F.; Lai, H.C. Combination use of laryngoscope, jaw thrust, and Trachway for improving difficult tracheal intubation in obese. J. Med. Sci. 2022, 42, 197–198. [Google Scholar]
- Nouruzi-Sedeh, P.; Schumann, M.; Groeben, H. Laryngoscopy via Macintosh blade versus GlideScope: Success rate and time for endotracheal intubation in untrained medical personnel. Anesthesiology 2009, 110, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Gu, M.; Lian, M.; Gong, C.; Chen, L.; Li, S. The teaching order of using direct laryngoscopy first may improve the learning outcome of endotracheal incubation: A preliminary, randomized controlled trial. Medicine 2019, 98, e15624. [Google Scholar] [CrossRef]
- Ruetzler, K.; Szarpak, L.; Smereka, J.; Dabrowski, M.; Bialka, S.; Mosteller, L.; Szarpak, A.; Ludwin, K.; Wojewodzka-Zelezniakowicz, M.; Ladny, J.R. Comparison of direct and video laryngoscopes during different airway scenarios performed by experienced paramedics: A randomized cross-over manikin study. Biomed Res. Int. 2020, 2020, 5382739. [Google Scholar] [CrossRef]
- Nalubola, S.; Jin, E.; Drugge, E.D.; Weber, G.; Abramowicz, A.E. Video versus direct laryngoscopy in novice intubators: A systematic review and meta-analysis. Cureus 2022, 14, e29578. [Google Scholar] [CrossRef]
- Ayoub, C.M.; Kanazi, G.E.; Al Alami, A.; Rameh, C.; El-Khatib, M.F. Tracheal intubation following training with the GlideScope® compared to direct laryngoscopy. Anaesthesia 2010, 65, 674–678. [Google Scholar] [CrossRef]
- Maharaj, C.H.; Costello, J.F.; Higgins, B.D.; Harte, B.H.; Laffey, J.G. Learning and performance of tracheal intubation by novice personnel: A comparison of the Airtraq® and Macintosh laryngoscope. Anaesthesia 2006, 61, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Moon, Y.J.; Kim, J.; Seo, D.W.; Kim, J.W.; Jung, H.W.; Suk, E.H.; Ha, S.I.; Kim, S.H.; Kim, J.U. Endotracheal intubation by inexperienced trainees using the Clarus Video System: Learning curve and orodental trauma perspectives. J. Dent. Anesth. Pain Med. 2015, 15, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Tseng, K.Y.; Chau, S.W.; Su, M.P.; Shih, C.K.; Lu, I.C.; Cheng, K.I. A comparison of Trachway intubating stylet and Airway Scope for tracheal intubation by novice operators: A manikin study. Kaohsiung J. Med. Sci. 2012, 28, 448–451. [Google Scholar] [CrossRef]
- Hung, K.C.; Tan, P.H.; Lin, V.C.; Wang, H.K.; Chen, H.S. A comparison of the Trachway intubating stylet and the Macintosh laryngoscope in tracheal intubation: A manikin study. J. Anesth. 2013, 27, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.; Lee, C.L.; Huang, S.J.; Shyr, M.H. Comparison between the Trachway video intubating stylet and Macintosh laryngoscope in four simulated difficult tracheal intubations: A manikin study. Tzu Chi Med. J. 2016, 28, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Pius, J.; Noppens, R.R. Learning curve and performance in simulated difficult airway for the novel C-MAC® video-stylet and C-MAC® Macintosh video laryngoscope: A prospective randomized manikin trial. PLoS ONE 2020, 15, e0242154. [Google Scholar] [CrossRef] [PubMed]
- Tsay, P.J.; Hsu, S.W.; Peng, H.C.; Wang, C.H.; Lee, S.W.; Lai, H.Y. Trachway intubating stylet for tracheal intubation in an ankylosing spondylitis patient undergoing total hip replacement under general anesthesia. Acta Anaesthesiol. Taiwan 2011, 49, 159–161. [Google Scholar] [CrossRef]
- Hung, K.C. A novel modified method of using Trachway intubating stylet for awake tracheal intubation in patients with anticipated difficult airway. Acta Anaesthesiol. Taiwan 2013, 51, 90–93. [Google Scholar] [CrossRef]
- Chang, P.Y.; Hu, P.Y.; Lin, Y.C.; Chen, H.Y.; Chiang, F.Y.; Wu, C.W.; Dionigi, G.; Lu, I.C. Trachway video intubating stylet allows for optimization of electromyographic endotracheal tube placement for monitored thyroidectomy. Gland Surg. 2017, 6, 464–468. [Google Scholar] [CrossRef]
- Wang, M.; Ding, R.; Li, Z.; He, M.; Liu, C. Comparison of intubation of Shikani optical stylet and Clarus Video Stylet in patients with cervical spine immobilization. J. Pract. Med. 2017, 24, 3933–3936. [Google Scholar]
- Xu, M.; Li, X.X.; Guo, X.Y.; Wang, J. Shikani Optical Stylet versus Macintosh laryngoscope for intubation in patients undergoing surgery for cervical spondylosis: A randomized controlled trial. Chin. Med. J. 2017, 130, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.W.; Chen, J.Y.; Lan, K.M.; Hung, K.C. The use of Trachway for electromyographic (EMG) tube placement. Gland Surg. 2018, 7, 244–245. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.K.; Lee, H.C.; Park, J.B.; Oh, H.; Park, H.P. McGrath MAC videolaryngoscope versus Optiscope video stylet for tracheal intubation in patients with manual inline cervical stabilization: A randomized trial. Anesth. Analg. 2020, 130, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.H.; Heo, S.K.; Cheon, S.U.; Ryu, S.A. The effects of backward, upward, rightward pressure maneuver for intubation using the OptiscopeTM: A retrospective study. Anesth. Pain Med. 2021, 16, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Cook, T.M.; Boniface, N.J.; Seller, C.; Hughes, J.; Damen, C.; MacDonald, L.; Kelly, F.E. Universal videolaryngoscopy: A structured approach to conversion to videolaryngoscopy for all intubations in an anaesthetic and intensive care department. Br. J. Anaesth. 2018, 120, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.Y. Education: The last mile to universal videolaryngoscopy. Br. J. Anaesth. 2018, 120, 1431–1432. [Google Scholar] [CrossRef] [PubMed]
- Cook, T.M.; Kelly, F.E.; Boniface, N.; Seller, C. Universal videolaryngoscopy: The importance of choosing the right device. Reply to ‘Cognitive re-engineering after a 15-year experience with routine videolaryngoscopy’ (Br J Anaesth 2019; 122: e57–8). Br. J. Anaesth. 2019, 122, e59–e60. [Google Scholar] [CrossRef]
- Cook, T.M.; Aziz, M.F. Has the time really come for universal videolaryngoscopy? Br. J. Anaesth. 2022, 129, 474–477. [Google Scholar] [CrossRef]
- Penketh, J.; Kelly, F.E.; Cook, T.M. Use of videolaryngoscopy as the first option for all tracheal intubations: Technical benefits and a simplified algorithm for airway management. Br. J. Anaesth. 2023, 130, e425–e426. [Google Scholar] [CrossRef]
- Mirrakhimov, A.E.; Torgeson, E. Use of videolaryngoscopy as the first option for all tracheal intubations: Not so fast. Comment on Br J Anaesth 2022; 129: 624–634. Br. J. Anaesth. 2023, 130, e12–e13. [Google Scholar] [CrossRef]
- Pieters, B.M.A.; Maas, E.H.A.; Knape, J.T.A.; van Zundert, A.A.J. Videolaryngoscopy vs. direct laryngoscopy use by experienced anaesthetists in patients with known difficult airways: A systematic review and meta-analysis. Anaesthesia 2017, 72, 1532–1541. [Google Scholar] [CrossRef]
- Chen, I.W.; Li, Y.Y.; Hung, K.C.; Chang, Y.J.; Chen, J.Y.; Lin, M.C.; Wang, K.F.; Lin, C.M.; Huang, P.W.; Sun, C.K. Comparison of video-stylet and conventional laryngoscope for endotracheal intubation in adults with cervical spine immobilization: A PRISMA-compliant meta-analysis. Medicine 2022, 101, e30032. [Google Scholar] [CrossRef]
- Hung, K.C.; Chang, Y.J.; Chen, I.W.; Lin, C.M.; Liao, S.W.; Chin, J.C.; Chen, J.Y.; Yew, M.; Sun, C.K. Comparison of video-stylet and video-laryngoscope for endotracheal intubation in adults with cervical neck immobilisation: A meta-analysis of randomised controlled trials. Anaesth. Crit. Care Pain Med. 2021, 40, 100965. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | |
|---|---|---|---|---|---|---|---|
| Total anesthesia number | 16,077 | 17,831 | 17,998 | 193,07 | 19,721 | 19,244 | 19,765 |
| GA number | 153,39 | 16,893 | 17,497 | 18,481 | 19,009 | 18,574 | 19,061 |
| LMA–GA number | 5544 | 5134 | 5816 | 5902 | 5863 | 5714 | 4932 |
| ET–-GA number | 5953 | 6504 | 6920 | 6966 | 7418 | 6982 | 7602 |
| VL | 0 | 0 | 20 | 100 | 635 | 336 | 305 |
| Styletubation | 5953 | 6504 | 6900 | 6866 | 6783 | 6646 | 7297 |
| VL | Styletubation | |
|---|---|---|
| Affordability | Expensive (USD 7000~10,000) | Moderate (USD 600~5000) |
| Availability | Globally | Regionally |
| Accessibility | Yes | Yes |
| Maintenance | Easy | Easy |
| Learning curve (experienced and novice) | Fast | Very fast |
| Team performance | Excellent | Excellent |
| Rescue for difficult/failed intubation | Practical | Practical |
| Combined use with other tools | With FOB | With DL/VL/FOB |
| Use in ER, ICU, prehospital rescue by EMS | Often | Gradually increasing |
| View quality on video monitor | Excellent | Excellent |
| Required use of a laryngoscope blade | Yes | No |
| Required mouth opening | Yes | Yes |
| Required lifting force | Yes | No |
| Required alignment of airway axes | Yes | No |
| Often need external laryngeal manipulation | Yes | No |
| Glottic visualization | Excellent | Excellent |
| Difficulty inserting ET tube | Possible | Rare |
| Required stylet | Possible | No |
| Impact of collapsed epiglottis | Heavily | Heavily |
| Impact of secretions, blood, vomitus on the lens | Heavily | Heavily |
| First-attempt success rate | High | Perfect |
| Time to intubate | Varied | Fast |
| See around the corner of the airway structures | Yes | Yes |
| Esophageal intubation incidence | Possible | Very rare |
| Autonomic stimulation | Very much | Mild |
| Airway-related complications | Quite often | Very rare |
| Suitable for awake intubation | Yes | Yes |
| Operator’s subjective satisfaction | High | Extremely high |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luk, H.-N.; Qu, J.Z. Styletubation versus Laryngoscopy: A New Paradigm for Routine Tracheal Intubation. Surgeries 2024, 5, 135-161. https://doi.org/10.3390/surgeries5020015
Luk H-N, Qu JZ. Styletubation versus Laryngoscopy: A New Paradigm for Routine Tracheal Intubation. Surgeries. 2024; 5(2):135-161. https://doi.org/10.3390/surgeries5020015
Chicago/Turabian StyleLuk, Hsiang-Ning, and Jason Zhensheng Qu. 2024. "Styletubation versus Laryngoscopy: A New Paradigm for Routine Tracheal Intubation" Surgeries 5, no. 2: 135-161. https://doi.org/10.3390/surgeries5020015