

Biliary Leak from Ducts of Luschka: Systematic Review of the Literature
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
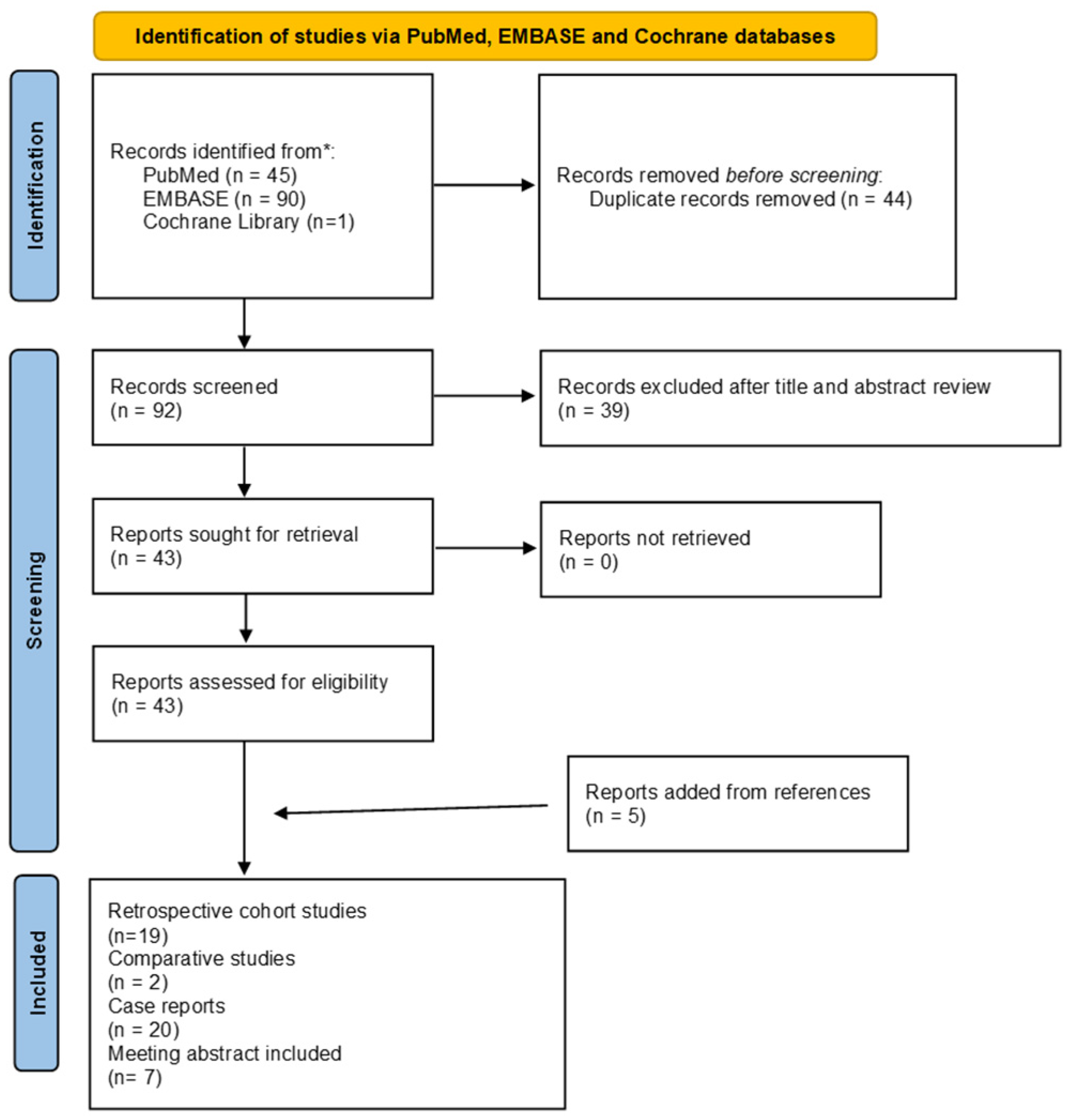
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
3. Results
3.1. Types of Studies
3.2. Rate of LD Leak
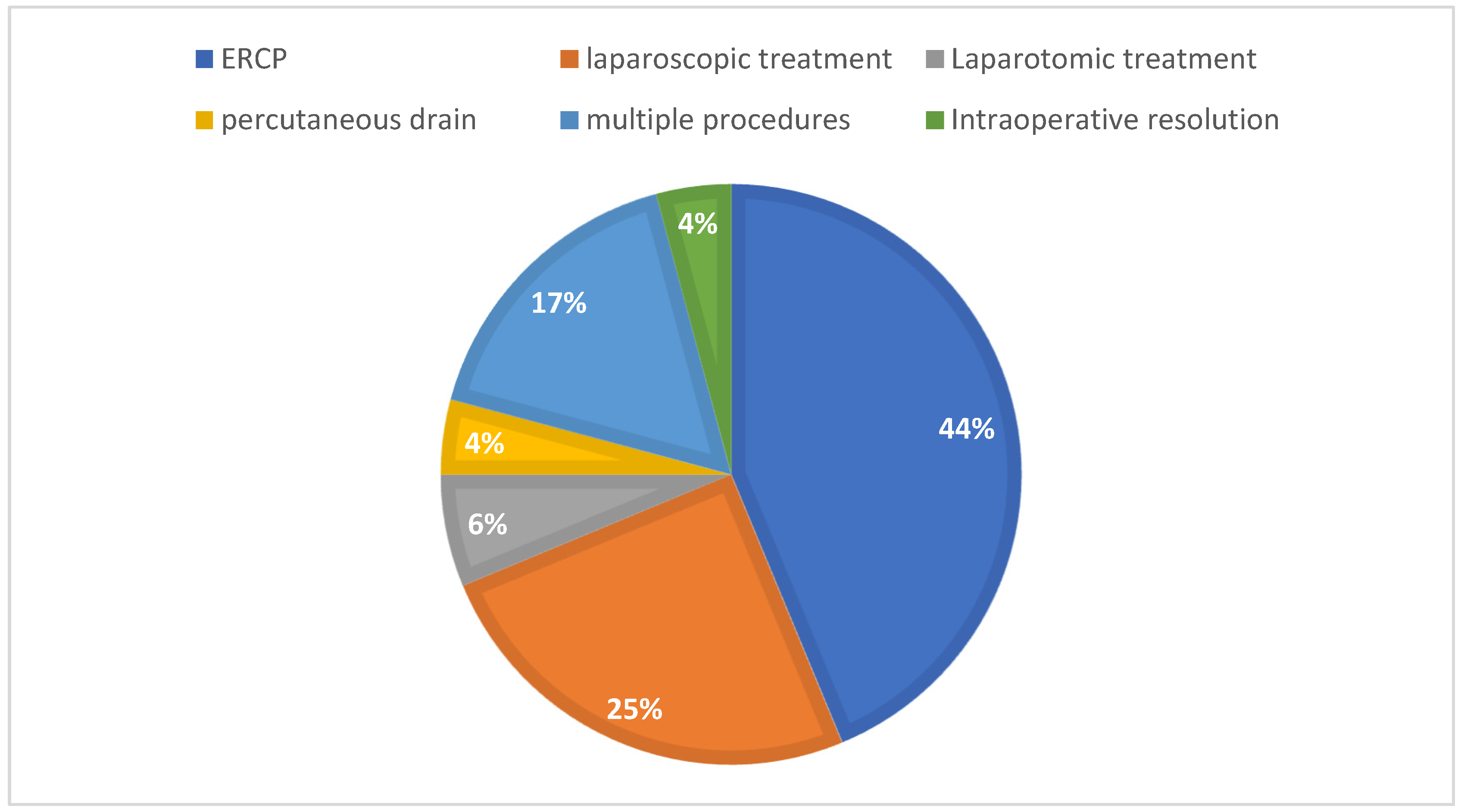
3.3. Type of Intervention and Treatment
4. Discussion
4.1. Deliberation
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pesce, A.; Portale, T.R.; Minutolo, V.; Scilletta, R.; Destri, G.L.; Puleo, S. Bile duct injury during laparoscopic cholecystectomy without intraoperative cholangiography: A retrospective study on 1,100 selected patients. Dig. Surg. 2012, 29, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Pesce, A.; Palmucci, S.; La Greca, G.; Puleo, S. Iatrogenic bile duct injury: Impact and management challenges. Clin. Exp. Gastroenterol. 2019, 12, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Chun, K. Recent classifications of the common bile duct injury. Korean J. Hepato-Biliary-Pancreat. Surg. 2014, 18, 69–72. [Google Scholar] [CrossRef]
- Christoforidis, E.; Vasiliadis, K.; Goulimaris, I.; Tsalis, K.; Kanellos, I.; Papachilea, T.; Tsorlini, E.; Betsis, D. A single center experience in minimally invasive treatment of postcholecystectomy bile leak, complicated with biloma formation. J. Surg. Res. 2007, 141, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Viste, A.; Horn, A.; Øvrebø, K.; Christensen, B.; Angelsen, J.-H.; Hoem, D. Bile duct injuries following laparoscopic cholecystectomy. Scand. J. Surg. 2015, 104, 233–237. [Google Scholar] [CrossRef]
- Garcia, S.; Concepción, A.M.; Wakoff, C. Bile Leak Due to Luschka Duct Injury after Laparoscopic Cholecystectomy: A Case Report. Cureus 2022, 14, e28427. [Google Scholar] [CrossRef]
- Doumenc, B.; Boutros, M.; Dégremont, R.; Bouras, A. Biliary leakage from gallbladder bed after cholecystectomy: Luschka duct or hepaticocholecystic duct? Morphologie 2016, 100, 36–40. [Google Scholar] [CrossRef]
- Schnelldorfer, T.; Sarr, M.G.; Adams, D.B. What is the Duct of Luschka?—A Systematic Review. J. Gastrointest. Surg. 2012, 16, 656–662. [Google Scholar] [CrossRef]
- Tabanera, A.V.; Vicente, A.P.; Buenadicha, A.L.; Peromingo, R.; Hervás, P.L.; Vazquez-Garza, J.N. Luschka Duct Leak: An Unexpected Cause of Choleperitoneum after Liver Transplant. Transplantation 2020, 18, 526–528. [Google Scholar] [CrossRef]
- Handra-Luca, A.; Ben Romdhane, H.M.; Hong, S.-M. Luschka Ducts of the Gallbladder in Adults: Case Series Report and Review of the Medical Literature. Int. J. Surg. Pathol. 2020, 28, 482–489. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Crowley, C.; Elojeimy, S.; Rieter, W.J. Utility of Dynamic Hepatobiliary Scintigraphy in Identifying a Duct of Luschka Bile Leak. Clin. Nucl. Med. 2021, E172–E173. [Google Scholar] [CrossRef]
- Sánchez, M.; Heiberger, F.; Rojas, R.; Sánchez, R.; Bordón, A. Conservative Management of Bile Leak Secondary to an Accessory Duct of Luschka. HPB 2021, 23 (Suppl. S1), S384. [Google Scholar] [CrossRef]
- Nagaratnam, P.; Ngo, J.S.L.; Ling, L.L.; Kharlina, K.; Gew, L.T.; Sidhu, J. A multicentre study on the endoscopic management of bile duct injury. J. Gastroenterol. Hepatol. 2021, 36 (Suppl. S2). [Google Scholar] [CrossRef]
- Hussain, A.; Lafaurie, G.; Hafeez, R.; El-Hasani, S. Is Specialisation Needed in Laparoscopic Cholecystectomy? A Retrospective Cohort Study of 5122 Patients. Chirurgia 2020, 115, 756–766. [Google Scholar] [CrossRef]
- Chandra, S.; Murali, A.R.; Masadeh, M.; Silverman, W.B.; Johlin, F.C. Comparison of Biliary Stent versus Biliary Sphincterotomy Alone in the Treatment of Bile Leak. Dig. Dis. 2020, 38, 32–37. [Google Scholar] [CrossRef]
- Paramythiotis, D.; Moysidis, M.; Rafailidis, V.; Bangeas, P.; Karakatsanis, A.; Kalogera, A.; Michalopoulos, A. Ducts of Luschka as a rare cause of postoperative biloma. MRCP findings. Radiol. Case Rep. 2019, 14, 1237–1240. [Google Scholar] [CrossRef] [PubMed]
- Masoni, L.; Landi, L.; Maglio, R. Intraoperative Treatment of Duct of Luschka during Laparoscopic Cholecystectomy: A Case Report and Revision of Literature. Case Rep. Surg. 2018, 2018, 9813489. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Chandra, A. Management of bile leak from subvesical duct (duct of Luschka) during laparoscopic cholecystectomy. Turk. J. Surg. 2018, 37, 80–81. [Google Scholar] [CrossRef]
- Lytvyn, O.I.; Usenko, O.Y.U.; Nichitaylo, M.Y.; Ogorodnik, P.V.; Lytvyn, O.I.; Deynichenko, A.G. Re-laparoscopy in diagnostic and management of postoperative bile leak after extrahepatic biliary operations. Surg. Endosc. 2019, 33 (Suppl. S2), S693. [Google Scholar]
- Antequera, A.; MacAno, C.; Lopez, M.; Robba, M.; Edmons, R.; Coleman, N. Duct of Lushcka. Source of complications. Surg. Endosc. 2019, 33 (Suppl. S2), S695. [Google Scholar]
- Abtar, H.K.; Mhana, T.M.; Zbibo, R.; Mneimneh, M.; Asmar, A.E. First case report of bile leak from the duct of Luschka in a patient with mini-gastric bypass: The challenge of management. Ann. Med. Surg. 2018, 35, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Bonatti, H.J.R.; Corey, M.R.; Taylor, J.T.; Geevarghese, S.K. Bile leak from the gallbladder fossa after liver transplantation. Eur. Surg. 2018, 50, 33–36. [Google Scholar] [CrossRef]
- Ko, S.Y.; Lee, J.R.; Wang, J.H. Endoscopic Nasobiliary Drainage for Bile Leak Caused by Injury to the Ducts of Luschka. Korean J. Gastroenterol. 2017, 69, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Mariolis-Sapsakos, T.; Zarokosta, M.; Zoulamoglou, M.; Piperos, T.; Papapanagiotou, I.; Sgantzos, M.; Birbas, K.; Kaklamanos, I. Aberrant subvesical bile ducts identified during laparoscopic cholecystectomy: A rare case report and review of the literature. Int. J. Surg. Case Rep. 2017, 31, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Aspinen, S.; Harju, J.; Kinnunen, M.; Juvonen, P.; Kokki, H.; Eskelinen, M. A randomized multicenter study of minilaparotomy cholecystectomy versus laparoscopic cholecystectomy with ultrasonic dissection in both groups. Scand. J. Gastroenterol. 2016, 51, 354–359. [Google Scholar] [CrossRef]
- Shahnawaz, Z.; Arif, M.O.; Roy, A. Post cholecystectomy bile leak from the duct of Luschka in a patient with Marfan’s syndrome. Am. J. Gastroenterol. 2015, 110 (Suppl. S1), S115–S116. [Google Scholar] [CrossRef]
- Salsano, G.; Paparo, F.; Valdata, A.; Patrone, L.; Filauro, M.; Rollandi, G.A.; De Caro, G. Management of Bile Leak from Luschka Ducts after Laparoscopic Cholecystectomy: An Original Procedure for Coil Embolization. Cardiovasc. Interv. Radiol. 2016, 39, 483–486. [Google Scholar] [CrossRef]
- Gutierrez, J.P.; Smith, I.B.; Wilcox, C.M.; Mönkemüller, K. Bile leak from the duct of Luschka treated with double-balloon enteroscopy ERCP in a patient with Roux-en-Y gastric bypass. Endoscopy 2013, 45, E404. [Google Scholar] [CrossRef]
- Tewani, S.K.; Turner, B.G.; Chuttani, R.; Pleskow, D.K.; Sawhney, M.S. Location of bile leak predicts the success of ERCP performed for postoperative bile leaks. Gastrointest. Endosc. 2013, 77, 601–608. [Google Scholar] [CrossRef]
- Thayalasekaran, S.; Gibson, M.; Kinchen, J.; Booth, J.; Booth, M.; Mee, A. Bile duct leaks from an aberrant duct of Luschka. Gut 2012, 61 (Suppl. S2), A381–A382. [Google Scholar] [CrossRef]
- Lo Nigro, C.; Geraci, G.; Sciuto, A.; Li Volsi, F.; Sciume, C.; Modica, G. Bile leaks after videolaparoscopic cholecystectomy: Duct of Luschka. Endoscopic treatment in a single centre and brief literature review on current management. Ann. Ital. Chir. 2012, 83, 303–312. [Google Scholar]
- Tran, T.; Kureshi, I. Bile leak from the duct of luschka: A multidisciplinary approach. Am. J. Gastroenterol. 2011, 106 (Suppl. S2), S216. [Google Scholar] [CrossRef]
- Hwang, J.C.; Kim, J.H.; Yoo, B.M.; Lim, S.-G.; Kim, W.H.; Kim, M.W. Temporary placement of a newly designed, fully covered, self-expandable metal stent for refractory bile leaks. Gut Liver 2011, 5, 96–99. [Google Scholar] [CrossRef]
- Fasoulas, K.; Zavos, C.; Chatzimavroudis, G.; Trakateli, C.; Vasiliadis, T.; Ioannidis, A.; Kountouras, J.; Katsinelos, P. Eleven-year experience on the endoscopic treatment of post-cholecystectomy bile leaks. Ann. Gastroenterol. 2011, 24, 200–205. [Google Scholar]
- Neumann, H.; Fry, L.C.; Malfertheiner, P.; Mönkemüller, K. Bile leak from the duct of Luschka. Z. Gastroenterol. 2010, 48, 256–257. [Google Scholar] [CrossRef]
- Pinkas, H.; Brady, P.G. Biliary leaks after laparoscopic cholecystectomy: Time to stent or time to drain. Hepatobiliary Pancreat Dis. Int. 2008, 7, 628–632. [Google Scholar]
- Bledsoe, S.E.; Maull, K.I. Image of the month. Subvesical bile duct (Luschka) leak. Arch. Surg. 2008, 143, 1127. [Google Scholar] [CrossRef] [PubMed]
- Tantia, O.; Jain, M.; Khanna, S.; Sen, B. Iatrogenic biliary injury: 13,305 cholecystectomies experienced by a single surgical team over more than 13 years. Surg. Endosc. 2008, 22, 1077–1086. [Google Scholar] [CrossRef] [PubMed]
- Rulli, F.; Grasso, E. Biliary peritonitis for duct of Luschka bile leak after laparoscopic cholecystectomy performed with a 10-mm harmonic scalpel. Langenbeck’s Arch. Surg. 2007, 392, 111–112. [Google Scholar] [CrossRef] [PubMed]
- Ramia, J.M.; Muffak, K.; Mansilla, A.; Villar, J.; Garrote, D.; Ferron, J.A. Postlaparoscopic cholecystectomy bile leak secondary to an accessory duct of Luschka. JSLS 2005, 9, 216–217. [Google Scholar]
- Misra, M.; Schiff, J.; Rendon, G.; Rothschild, J.; Schwaitzberg, S. Laparoscopic cholecystectomy after the learning curve: What should we expect? Surg. Endosc. 2005, 19, 1266–1271. [Google Scholar] [CrossRef]
- Kaffes, A.J.; Hourigan, L.; De Luca, N.; Byth, K.; Williams, S.J.; Bourke, M.J. Impact of endoscopic intervention in 100 patients with suspected postcholecystectomy bile leak. Gastrointest. Endosc. 2005, 61, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Sandha, G.S.; Bourke, M.J.; Haber, G.B.; Kortan, P.P. Endoscopic therapy for bile leak based on a new classification: Results in 207 patients. Gastrointest. Endosc. 2004, 60, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Rossi, P.; Servili, S.; Contine, A.; Graziosi, L.; Carbone, E.; Annesi, M.; Framarini, M.; Tristaino, B. Bile leak from the hepatic bed after laparoscopic cholecystectomy. Chir. Ital. 2002, 54, 507–509. [Google Scholar]
- De Palma, G.D.; Galloro, G.; Iuliano, G.; Puzziello, A.; Persico, F.; Masone, S.; Persico, G. Leaks from laparoscopic cholecystectomy. Hepatogastroenterology 2002, 49, 924–925. [Google Scholar]
- Albishri, S.; Issa, S.; Kneteman, N.; Shapiro, A. Bile leak from duct of Luschka after liver transplantation. Transplantation 2001, 72, 338–340. [Google Scholar] [CrossRef]
- Braghetto, I.; Bastias, J.; Csendes, A.; Debandi, A. Intraperitoneal bile collections after laparoscopic cholecystectomy. Causes, clinical presentation, diagnosis and treatment. Surg. Endosc. 2000, 14, 1037–1041. [Google Scholar] [CrossRef]
- Wills, V.L.; Jorgensen, J.O.; Hunt, D.R. Role of relaparoscopy in the management of minor bile leakage after laparoscopic cholecystectomy. Br. J. Surg. 2000, 87, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, M.; Obermeyer, R.J.; Garcia, G.; Hashmi, M. Post-laparoscopic cholecystectomy bile leak secondary to an accessory duct of Luschka. Int. Surg. 1999, 84, 86–88. [Google Scholar]
- Mergener, K.; Strobel, J.C.; Suhocki, P.; Jowell, P.S.; Enns, R.A.; Branch, M.; Baillie, J. The role of ERCP in diagnosis and management of accessory bile duct leaks after cholecystectomy. Gastrointest. Endosc. 1999, 50, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Aru, G.M.; Davis, C.R.; Elliott, N.L.; Morris, S.J. Endoscopic retrograde cholangiopancreatography in the treatment of bile leaks and bile duct strictures after laparoscopic cholecystectomy. South. Med. J. 1997, 90, 705–708. [Google Scholar] [CrossRef] [PubMed]
- Bour, E.S.; Conter, R.L. Acute right-lower-quadrant mass presenting after laparoscopic cholecystectomy. Surg. Laparosc. Endosc. 1997, 7, 51–52. [Google Scholar] [CrossRef] [PubMed]
- Albasini, J.L.; Aledo, V.S.; Dexter, S.P.; Marton, J.; Martin, I.G.; McMahon, M.J. Bile leakage following laparoscopic cholecystectomy. Surg. Endosc. 1995, 9, 1274–1278. [Google Scholar] [CrossRef] [PubMed]
- Sefr, R.; Ochmann, J.; Kozumplik, L.; Vrastyak, J.; Penka, I. The role of relaparoscopy in the management of bile leaks after laparoscopic cholecystectomy. Int. Surg. 1995, 80, 356–357. [Google Scholar] [PubMed]
- Frakes, J.T.; Bradley, S.J. Endoscopic stent placement for biliary leak from an accessory duct of Luschka after laparoscopic cholecystectomy. Gastrointest. Endosc. 1993, 39, 90–92. [Google Scholar] [CrossRef]
- Brooks, D.C.; Becker, J.M.; Connors, P.J.; Carr-Locke, D.L. Management of bile leaks following laparoscopic cholecystectomy. Surg. Endosc. 1993, 7, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Kapoor, V.K. Epidemiology of Bile Duct Injury. In Post-Cholecystectomy Bile Duct Injury; Kapoor, V., Ed.; Springer: Singapore, 2020. [Google Scholar] [CrossRef]
- Pekolj, J.; Alvarez, F.A.; Palavecino, M.; Clariá, R.S.; Mazza, O.; de Santibañes, E. Intraoperative management and repair of bile duct injuries sustained during 10,123 laparoscopic cholecystectomies in a high-volume referral center. J. Am. Coll. Surg. 2013, 216, 894–901. [Google Scholar] [CrossRef]
- Booij, K.A.C.; de Reuver, P.R.; van Dieren, S.; van Delden, O.M.; Rauws, E.A.; Busch, O.R.; van Gulik, T.M.; Gouma, D.J. Long-term Impact of Bile Duct Injury on Morbidity, Mortality, Quality of Life, and Work Related Limitations. Ann. Surg. 2018, 268, 143–150. [Google Scholar] [CrossRef]
- Booij, K.A.C.; de Reuver, P.R.; Yap, K.; van Dieren, S.; van Delden, O.M.; Rauws, E.A.; Gouma, D.J. Morbidity and mortality after minor bile duct injury following laparoscopic cholecystectomy. Endoscopy 2015, 47, 40–46. [Google Scholar] [CrossRef] [PubMed]
- de’angelis, N.; Catena, F.; Memeo, R.; Coccolini, F.; Martínez-Pérez, A.; Romeo, O.M.; De Simone, B.; Di Saverio, S.; Brustia, R.; Rhaiem, R.; et al. 2020 WSES guidelines for the detection and management of bile duct injury during cholecystectomy. World J. Emerg. Surg. 2021, 16, 30. [Google Scholar] [CrossRef] [PubMed]
- Spanos, C.P.; Syrakos, T. Bile leaks from the duct of Luschka (subvesical duct): A review. Langenbeck’s Arch. Surg. 2006, 391, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Selleslag, S.; Vandeputte, M.; Walgraeve, M.-S. Unveiling the Hidden Culprit: A Case of Bile Leakage Post-Cholecystectomy Caused by a Luschka Duct. J. Belg. Soc. Radiol. 2023, 107, 59. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Type of Study | Leak (n/%) | DL/Other Causes of Leak (%) | Intervention | Treatment |
|---|---|---|---|---|---|
| Garcia et al. (2022) [6] | Case report | 1 | Not reported | LC | Re-laparoscopy |
| Crowley et al. (2021) [12] | Case report | 1 | Not reported | LC | Endoscopic |
| Sanchez et al. (2021) [13] | Poster presentation | 1 | Not reported | LC | Percutaneous drain |
| Nagaratnam et al. (2021) [14] | Poster presentation | 2 | 7.4% | LC | Endoscopic |
| Hussain et al. (2020) [15] | Retrospective cohort study | 4 (0.19%) | Not reported | LC | Re-laparoscopy |
| Chandra et al. (2020) [16] | Retrospective cohort study | 23 | 41% | LC; Hepatic resection, liver trauma | Endoscopic |
| Paramythiotis et al. (2019) [17] | Case report | 1 | Not reported | LC | Endoscopic |
| Tabanera et al. (2019) [9] | Case report | 1 | Not reported | Liver Transplant | Re-laparotomy |
| Masoni et al. (2018) [18] | Case report | 1 | Not reported | LC | Endoscopic |
| Kumar et al. (2018) [19] | Case report | 1 | Not reported | LC | Laparoscopic (intraoperative) |
| Lytvyn et al. (2019) [20] | Congress presentation | 52 | 41.50% | LC | Percutaneous drain, endoscopic and re-laparoscopy |
| Antequera et al. (2019) [21] | Congress presentation | 1 | Not reported | LC | Re-laparoscopy |
| Abtar et al. (2018) [22] | Case report | 1 | Not reported | LC after bariatric surgery | Re-laparoscopy |
| Bonatti et al. (2017) [23] | Case report | 1 | Not reported | LC | Endoscopic |
| Ko et al. (2017) [24] | Case report | 1 | Not reported | LC | Endoscopic |
| Mariolis et al. (2017) [25] | Case report | 1 | Not reported | LC | Laparoscopic (intraoperative) |
| Aspinen et al. (2015) [26] | Comparative study | 1 (1.9%) | Not reported | LC | Re-laparoscopy |
| Shahnawaz et al. (2015) [27] | Congress presentation | 1 | not reported | LC | Laparoscopic (intraoperative) + endoscopic |
| Salsano et al. (2015) [28] | Case report | 1 | Not reported | LC | Percutaneous transhepatic cholangiography (PTC) |
| Gutierrez et al. (2013) [29] | Case report | 1 | Not reported | LC after bariatric surgery | Endoscopic |
| Tewani et al. (2013) [30] | Retrospective cohort study | 30 | 24% | LC | Endoscopic |
| Thayalasekaran et al. (2012) [31] | Congress presentation | 11 | 13% | LC | Percutaneous drain, endoscopic and re-laparoscopy |
| Lo Nigro et al. (2012) [32] | Retrospective cohort study | 2 | 5.5% | LC | Endoscopic |
| Tran et al. (2011) [33] | Congress presentation | 1 | Not reported | LC | Percutaneous + endoscopic |
| Hwang et al. (2011) [34] | Case report | 1 | Not reported | LC | Endoscopic |
| Fasoulas et al. (2011) [35] | Retrospective cohort study | 4 | 6.06% | LC | Endoscopic |
| Neumann et al. (2010) [36] | Case report | 1 | Not reported | OC | Endoscopic |
| Pinkas et al. (2008) [37] | Comparative study | 5 | 25% | LC | Endoscopic |
| Bledsoe et al. (2008) [38] | Case report | 1 | Not reported | LC | Endoscopic |
| Tantia et al. (2008) [39] | Retrospective cohort study | 11 | 21% | LC | Endoscopic/Surgical |
| Rulli et al. (2006) [40] | Case report | 1 | Not reported | LC | Re-laparoscopy |
| Ramia et al. (2005) [41] | Retrospective cohort study | 2 (0.15%) | Not reported | LC | Re-laparoscopy |
| Misra et al. (2005) [42] | Retrospective cohort study | 5 (0.5%) | 45% | LC | Endoscopic, fibrin glue, re-laparoscopy |
| Kaffes et al. (2005) [43] | Retrospective cohort study | 15 | 15% | LC | Endoscopic |
| Sandha et al. (2004) [44] | Retrospective cohort study | 26 | 13% | LC | Endoscopic |
| Rossi et al. (2002) [45] | Retrospective cohort study | 5 (2%) | Not reported | LC | Endoscopic |
| De Palma et al. (2002) [46] | Retrospective cohort study | 4 | 6,3% | LC | Endoscopic |
| Albishri et al. (2001) [47] | Case report | 1 | Not reported | Liver Transplant | Re-laparotomy |
| Braghetto et al. (2000) [48] | Retrospective cohort study | 3 (0.05%) | 23% | LC | Re-laparotomy |
| Wills et al. (2000) [49] | Retrospective cohort study | 10 (0.5%) | 67% | LC | Re-laparoscopy |
| Jamshidi et al. (1999) [50] | Case report | 1 | Not reported | LC | Re-laparoscopy |
| Mergener et al. (1999) [51] | Retrospective cohort study | 15 | 17% | LC; OC | Percutaneous drain, endoscopic, re-laparotomy and re-laparoscopy |
| Aru et al. [52] | Retrospective cohort study | 1 (10%) | 10% | LC | Endoscopic |
| Bour et al. (1997) [53] | Case report | 1 | Not reported | LC | Re-laparoscopy |
| Albasini et al. (1995) [54] | Retrospective cohort study | 1 (0.2%) | Not reported | LC | Re-laparoscopy |
| Sefr et al. [55] | Retrospective cohort study | 3 (0.2%) | 37.5% | LC | Re-laparoscopy |
| Frakes et al. (1993) [56] | Case report | 1 | Not reported | LC | Endoscopic |
| Brooks et al. (1993) [57] | Retrospective cohort study | 2 (0.3%) | 22% | LC | Percutaneous drain, endoscopic, re-laparotomy and re-laparoscopy |
| Frakes et al. (1993) [56] | Case report | 1 | Not reported | LC | Endoscopic |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitiello, A.; Spagnuolo, M.; Persico, M.; Peltrini, R.; Berardi, G.; Calabrese, P.; De Werra, C.; Rescigno, C.; Troisi, R.; Pilone, V. Biliary Leak from Ducts of Luschka: Systematic Review of the Literature. Surgeries 2024, 5, 63-72. https://doi.org/10.3390/surgeries5010008
Vitiello A, Spagnuolo M, Persico M, Peltrini R, Berardi G, Calabrese P, De Werra C, Rescigno C, Troisi R, Pilone V. Biliary Leak from Ducts of Luschka: Systematic Review of the Literature. Surgeries. 2024; 5(1):63-72. https://doi.org/10.3390/surgeries5010008
Chicago/Turabian StyleVitiello, Antonio, Maria Spagnuolo, Marcello Persico, Roberto Peltrini, Giovanna Berardi, Pietro Calabrese, Carlo De Werra, Carmela Rescigno, Roberto Troisi, and Vincenzo Pilone. 2024. "Biliary Leak from Ducts of Luschka: Systematic Review of the Literature" Surgeries 5, no. 1: 63-72. https://doi.org/10.3390/surgeries5010008