1. Introduction
The use of large animal models in preclinical studies has provided invaluable data for evaluating the safety and efficacy of new therapies and devices and has facilitated the development and clinical application of cardiovascular innovations. With an increasingly valuable role, the implementation of large animal models has expanded, serving to bridge the translation of physiologic and economic aspects of animal research to the successful treatment of human heart failure [
1].
To test the safety, performance, and efficacy of a mechanical circulatory support device, we must determine the effects of the device on physiology, particularly with respect to the hematologic and hemodynamic changes. Detecting these physiologic changes requires a comparison with baseline data to evaluate the deviation from what is normal. Large animals are the model of choice for testing mechanical circulatory support devices [
2]. Among them, bovines have become the standard model, because their cardiovascular system is anatomically similar to that of humans. Furthermore, calves are easily available, their significant vessels are easily accessible, and they can withstand the physical stress of chronic instrumentation [
3]. Previous experimental surgical studies [
3,
4], performed between 1961 and 1971, reported hemodynamic measurements in unanesthetized calves; however, in retrospect, these studies were limited by the technology available at that time. Presently, although the necessary equipment is available for performing experimental studies to acquire baseline hemodynamic values in bovines, the cost remains prohibitive. This is because grants often fund the development of animal models for the study of a therapeutic agent and not for the purpose of obtaining baseline measurements.
In this study, we evaluated baseline hemodynamic values, including aortic and pulmonary blood flow, in a bovine model during a 62-day survival period after performing a control procedure. These baseline values are useful for developing mechanical circulatory support devices in the preclinical setting.
2. Materials and Methods
2.1. Animals
An 8-month-old female Corriente crossbred calf weighing 178 lbs. (80.9 kg) was used for this study. The animal received humane and routine care, treatment, and feeding before and throughout the study period. The protocol used was approved by the Texas Heart Institute Institutional Animal Care and Use Committee.
2.2. Anesthesia and Surgical Procedure
The preoperative screening was performed before surgery, to record heart rate, respiration rate, body temperature, and baseline clinical pathology values (i.e., complete blood count, blood chemistry, coagulation profile, and plasma-free hemoglobin level) (Equine Laboratories, Houston, TX, USA). No clinical abnormalities were noted in the animal’s condition, and the baseline clinical pathology values were within the normal range (reference values provided by Equine Laboratories). Before the procedure, the animal was stanchioned, and an angiocath was placed in the right jugular vein for fluid hydration. Food was withheld for approximately 18 h before surgery, and water was offered ad libitum. The animal was premedicated with 1 mg glycopyrrolate subcutaneously, 10 mg diazepam intravenously (IV), and 1000 mg ketamine IV to induce sedation. The animal was then intubated under direct vision with a cuffed endotracheal tube. An orogastric tube was placed for abdominal decompression. Under isoflurane anesthesia, the animal underwent replacement of the angiocath in the right jugular vein with a triple lumen catheter and was then given analgesic medication. Vancomycin (0.5 g in 100 mL NaCl IV) was administered for prevention against infection. The final prepping was completed, and the animal was transported to the operating room.
The animal was placed on the table in a right lateral recumbency position, and a cut-down was performed on the left side of the neck to insert a carotid artery pressure line for continuous postoperative monitoring. A left lateral thoracotomy was performed, and the fifth rib was removed. Fluid-filled pressure lines (aortic pressure (AoP), right atrial pressure (RAP), left atrial pressure (LAP), and pulmonary artery pressure (PAP)) and left and right flow probe lines were tunneled to exit the animal’s left side. A fluid-filled AoP line was placed in the internal thoracic artery. Fluid-filled lines for RAP, LAP, and PAP were then inserted into the right atrium, left atrium, and pulmonary artery, respectively. Flow probes (Transonic Systems Inc., Ithaca, NY, USA, 24 mm) were then placed on the aorta (left) and pulmonary artery (right) for postoperative blood flow measurement. A chest tube was placed in the left pleural cavity for postoperative fluid drainage, and an On-Q Catheter System (Alpharetta, GA, USA) was placed along the muscle line of the left superficial pectoral muscle for additional postoperative pain management.
All of the incisions were fully closed in layers. Before transfer, all of the exteriorized lines were secured to the skin. The animal was then moved to a stanchion and transported to the intensive care unit in stable condition for postoperative monitoring and care.
2.3. Postoperative Care and Data Collection
Throughout the postoperative period, the animal received butorphanol (10 mg IV) and flunixin meglumine (100 mg IV) every 4 to 8 h for pain prevention until postoperative days (PODs) 11 and 23, respectively. The On-Q Catheter System was also refilled with bupivacaine (Sensorcaine) as needed for additional pain prevention, until its removal on POD 11. For antibiotic therapy, the calf received the following: 1) ceftazidime (0.5 g in 100 mL NaCl IV) every 6 h from PODs 0 to 7; 2) vancomycin (0.5 g in 100 mL NaCl IV) every 12 h from PODs 0 to 7; and 3) enrofloxacin (300 mg subcutaneously) once daily from PODs 16 to 20, 24 to 28, and 37 to 41. In addition, the following were administered throughout the postoperative course to maintain and balance gut microbial organisms and to prevent the formation of gastric ulcers: (1) probiotic gel (10 g by mouth) once daily; (2) GastroGard (450 mg by mouth) twice daily; (3) ranitidine (150 mg by mouth) twice daily; and (4) misoprostol (200 mcg by mouth) twice daily. Fluids were infused for hydration and intravenous-line maintenance, and all of the pressure lines were routinely flushed with heparinized saline to prevent clotting within the lines. Anticoagulation was achieved with warfarin (1–7.5 mg by mouth) by monitoring the animal’s coagulation profile (international normalized ratio).
The physiologic pressures (AoP, RAP, LAP, and PAP), animal vital signs (heart rate, respiration rate, and temperature), aortic and pulmonary blood flow, and pulmonary and systemic vascular resistance (PVR and SVR, respectively) were recorded on an hourly basis by using PowerLab data acquisition hardware with LabChart Pro software (ADInstruments, Colorado Springs, CO, USA). Blood gas, hematocrit, and activated clotting time (ACT) were evaluated routinely. In addition, the hematologic and biochemistry parameters and blood-culture specimens were analyzed on at least a weekly basis to assess the animal for signs of bleeding, end-organ dysfunction, and infection.
Eight treadmill exercise evaluations were conducted from postoperative day (POD) 30 to case termination. The calf was transferred to a motorized treadmill (Good Horsekeeping, Inc., Ash Grove, MO, USA) and allowed to become familiarized with it. Afterwards, she was exercised for three-minute increments at various speed settings for a total duration of 15 to 30 min. To determine the animal’s hemodynamic response to exercise, physiological pressures (AoP, RAP, LAP, and PAP) and flows (aortic and pulmonary) were monitored, and arterial and venous blood gas values were analyzed at baseline, at each treadmill speed, and at recovery (19–31 min after exercise).
After a final treadmill exercise evaluation on POD 62, the animal was sedated and fully heparinized, after which it was euthanized with Euthasol (390 mg pentobarbital sodium/50 mg phenytoin sodium) at a dose of 0.22 mL/kg IV. The animal was weighed, and a postmortem examination was performed to evaluate the end organs.
2.4. Statistics
All of the hemodynamic data are reported as the mean ± standard deviation with the 95% confidence interval, as well as the minimum and maximum values during the treadmill tests.
3. Results
The animal’s clinical course was mostly uneventful. After surgery, the animal experienced some slight discomfort that resolved within the first postoperative week. The animal thrived throughout the postoperative course, gaining a total of 68.5 lbs. The clinical pathology values were in an acceptable range and showed no sign of infection or end-organ dysfunction.
Findings on gross examination after euthanasia were mostly unremarkable, except for a dark red-brown clot measuring up to 1.1 cm at the tip of the RAP line. On histopathologic examination, the clot was found to be made up of clumping red blood cells with a small number of enmeshed leukocytes, which is indicative of a postmortem clot. In addition, there was no indication of organization or layering, suggesting no chronicity. The histopathologic examination of the remaining tissues was generally unremarkable and did not demonstrate any significant pathologic sequela associated with the surgical procedure.
The hemodynamic data, including the parameters obtained while the animal was at rest in our laboratory’s intensive care unit (e.g., heart rate, pressure, flows, and vascular resistances) are provided in
Table 1.
Table 2 shows the pressures and flow rates at baseline and during treadmill trials. The average treadmill trial duration was 22.5 min, with an average distance walked of 2213.16 ft (674.5 m).
4. Discussion
The hemodynamic values that we obtained in a bovine model show cardiovascular physiologic behavior that is fairly similar to that observed in humans.
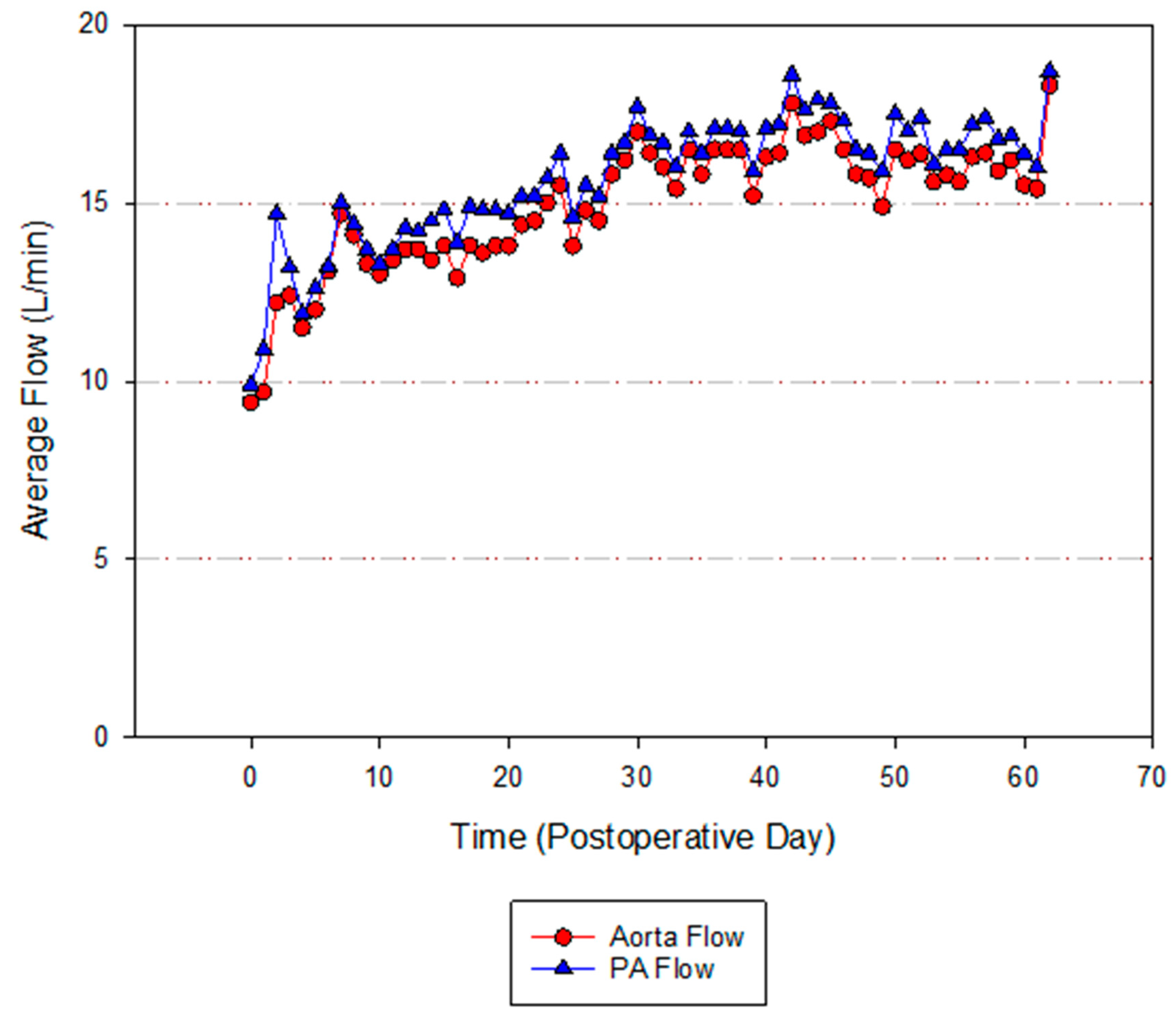
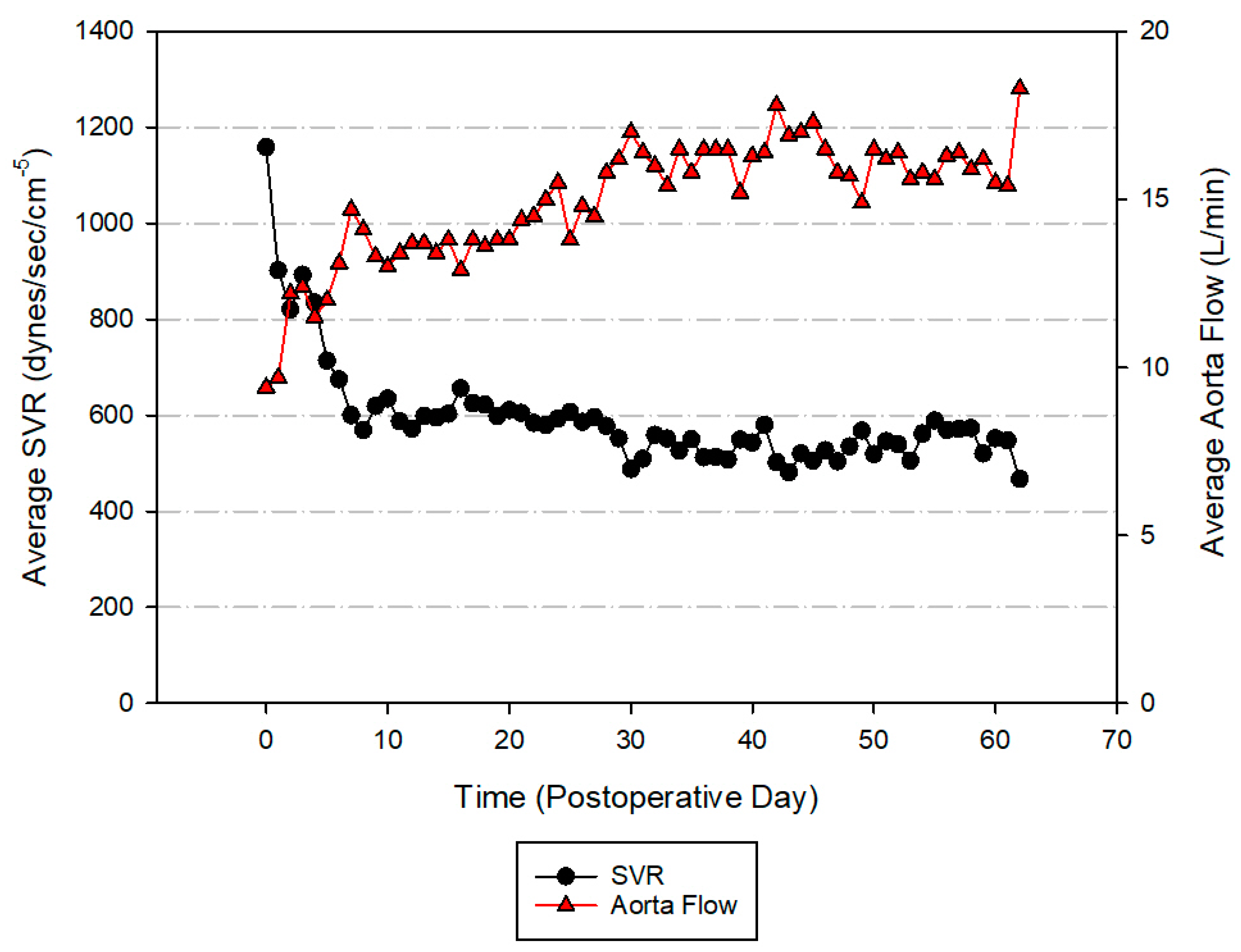
Figure 1, which shows the blood flow rates through the aorta and pulmonary artery during the duration of the study, reveals a steady increase in blood flow rates, which can be attributed to the weight gain and general growth of the animal. Another basic physiologic principle, as shown in
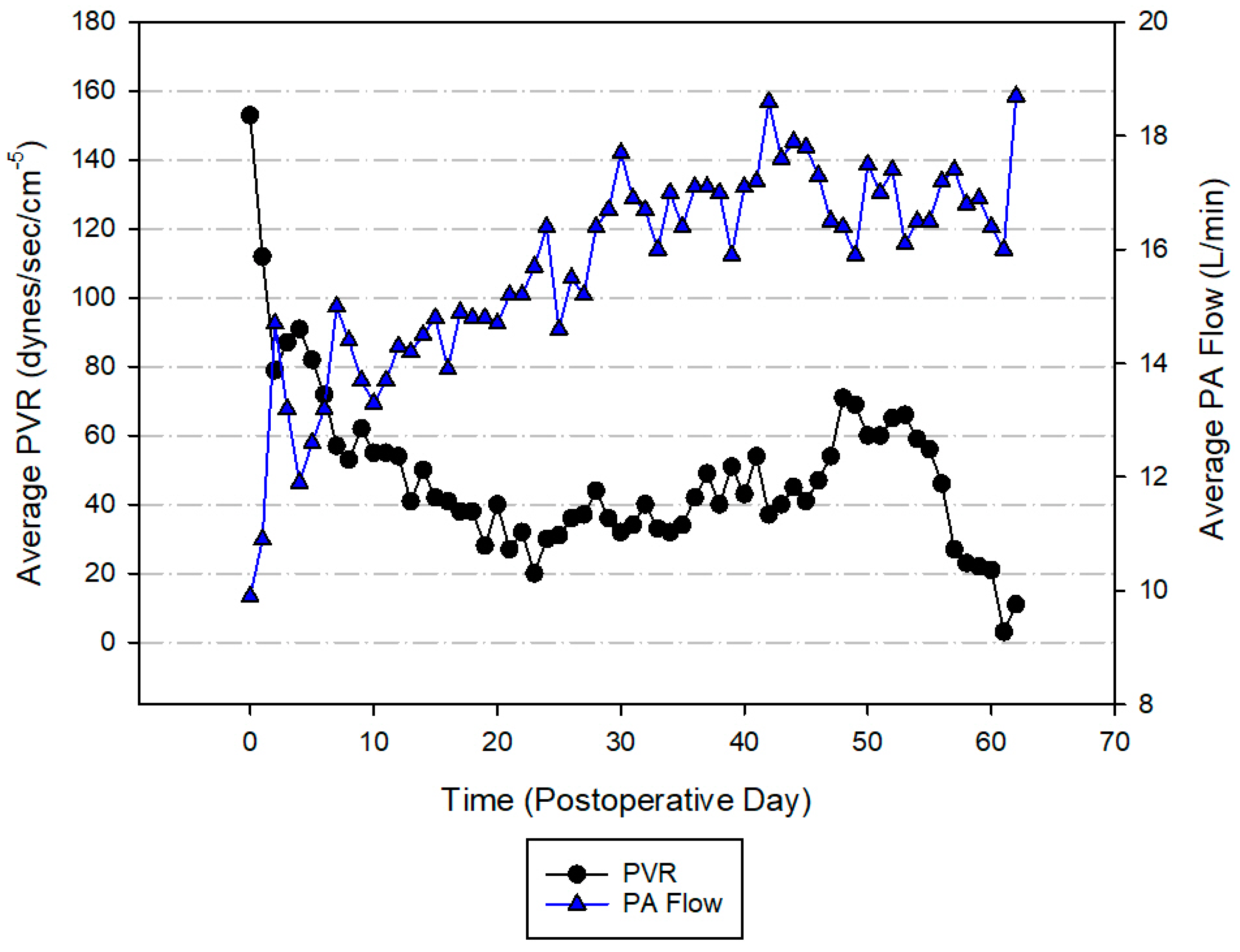
Figure 2 and
Figure 3, is that the blood flow through a vessel is equal to the change in pressure divided by the vascular resistance [
5]. This physiologic maxim is followed in these figures because of the negative correlation between systemic vascular resistance and aortic blood flow, as well as between PVR and pulmonary artery blood flow. When vascular resistance decreases, the blood flow increases.
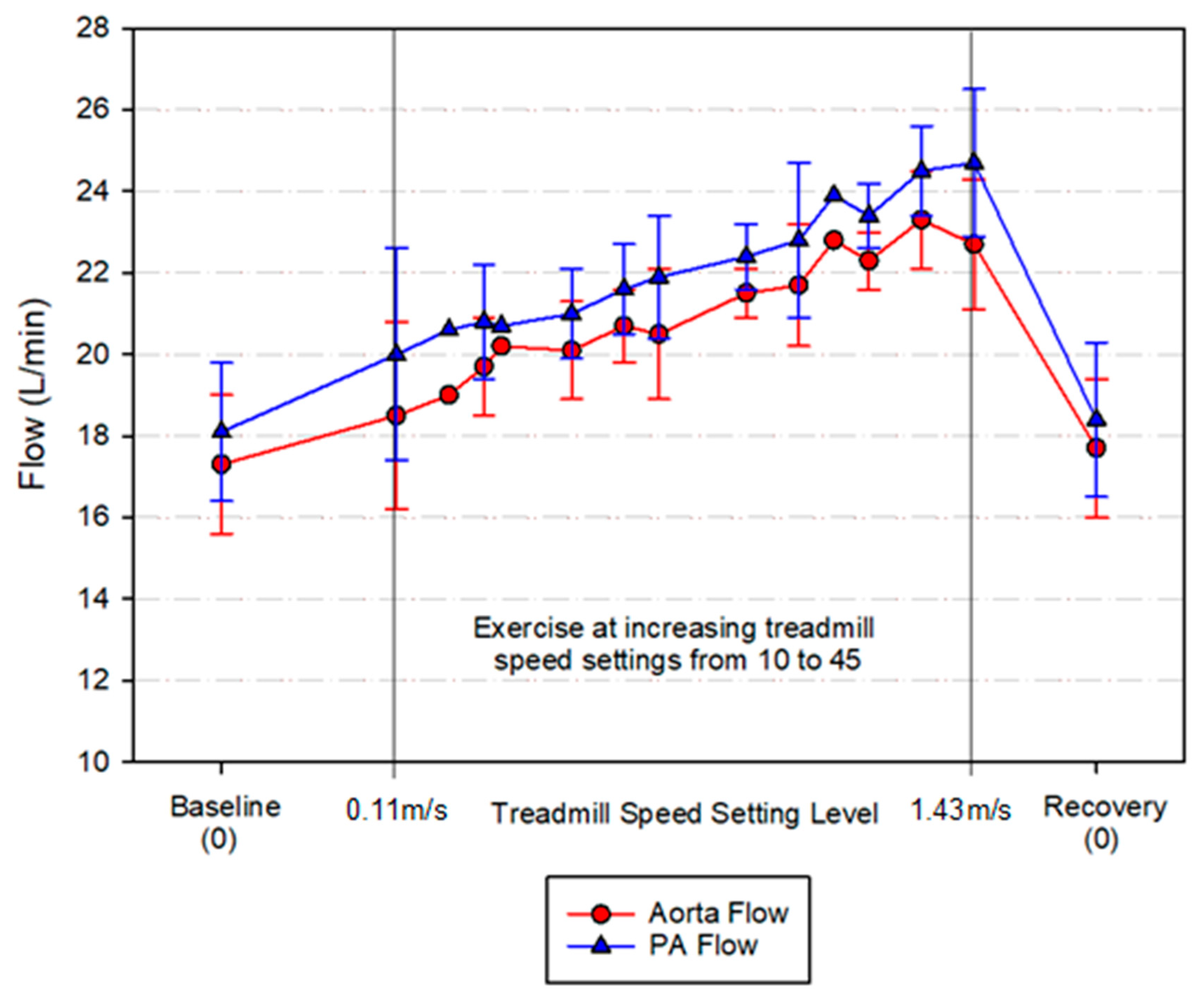
The evaluation of the blood flow rates during exercise, as shown in
Figure 4, reveals that exercise elicits several changes in the cardiovascular physiology. The activation of muscles requires hemodynamic and vasoregulatory adjustments to provide an optimal blood flow to the required sites. A consequence of these adjustments is a sympathetic discharge that results in increased sympathetic vascular tone, the release of catecholamines, and increased systolic blood pressure, which helps to improve the perfusion of actively contracting muscles [
6,
7]. However, despite increased systolic blood pressure, the rise in the mean arterial pressure is much lower, due to an overall decrease in the systemic vascular resistance. This decrease in the vascular resistance leads to the increase in blood flow observed in
Figure 4, once again presenting a predictable response to exercise. The average increase in the aortic blood flow during exercise was 16% (from an average aortic blood flow of 17.5 L/min before the treadmill trial to an average of 20 L/min during exercise). A similar increase was observed in the pulmonary artery blood flow, with an increase of 17% during exercise (from an average flow of 18 L/min before the treadmill trial to an average of 21 L/min during exercise). Although this adaptive change is also seen in humans, the bovine and human blood flow rates greatly differ. In humans, the average aortic and pulmonary artery blood flow rates during exercise are 7.1 L/min and 7 L/min [
8], respectively. These numbers represent a 10.94% and 11.11% increase compared with the baseline blood flow.
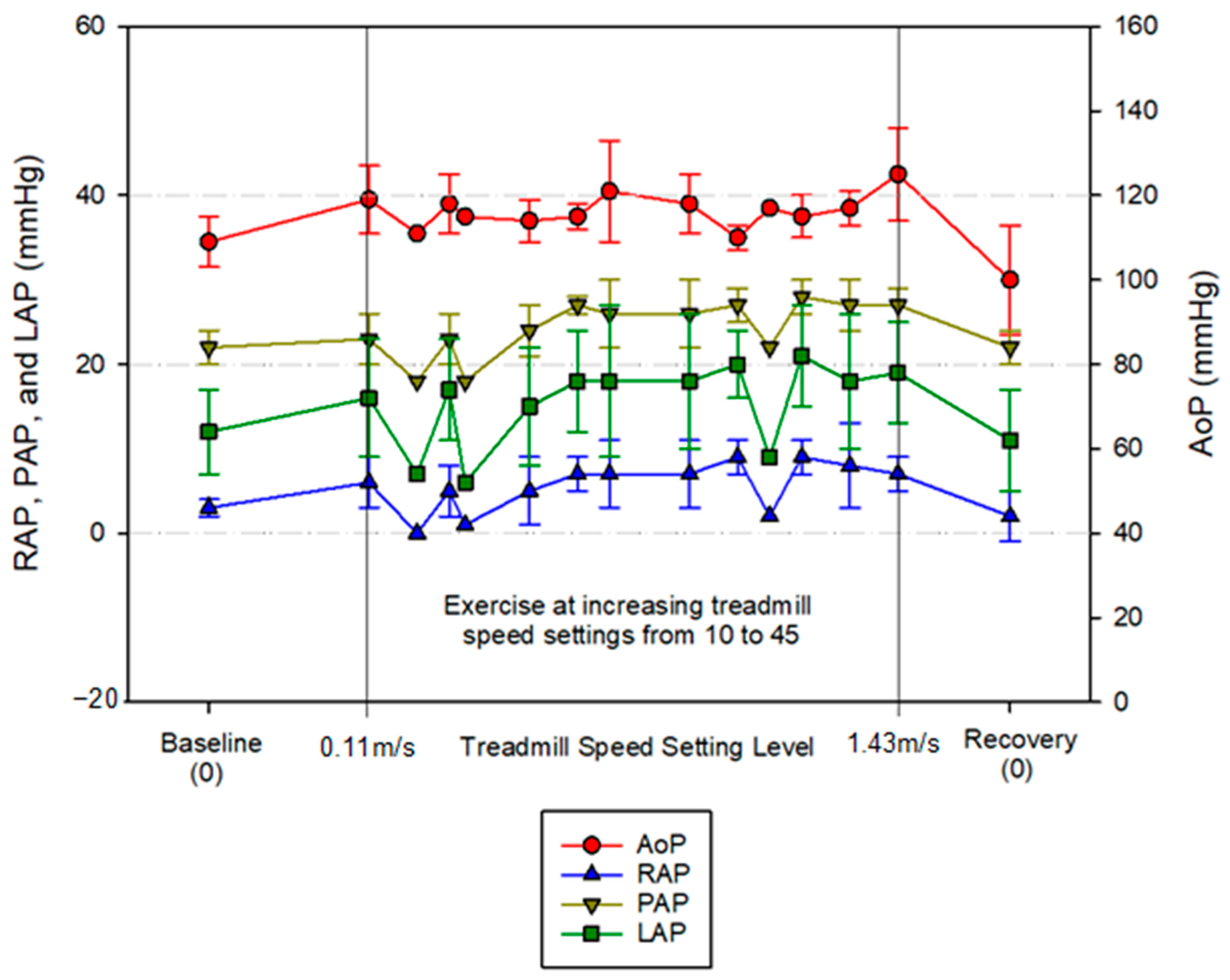
In
Figure 5, the relationship between the physiologic pressures (AoP, RAP, PAP, and LAP) and exercise is shown. As expected, during the treadmill exercise, an overall increase in the pressures was observed, as well as a decrease in the values during recovery. The increase in the pressures follows the same principles explained above—a sum of neurohormonal adaptive mechanisms. The decrease in the pressures is a direct consequence of the abrupt cessation of the activity, causing arterial vasodilation and decreased venous return [
9,
10].
The first animal studies in which these parameters were evaluated were also aimed at providing baseline hemodynamic indices. Some of them reported data for normal awake calves [
11], or anesthetized animals [
12]. Since the report by Stowe and Good in 1960 [
12], several other groups have studied the baseline hemodynamic parameters in calf models in response to different pharmacologic agents [
13,
14,
15], or procedures (e.g., myocardial infarction) [
16]. For most of these studies, the results were obtained through catheterization after using an interventional approach. In contrast, our results were obtained after performing a control procedure, in which we used a complete surgical approach as though we were going to implant a cardiac assist device. This allowed us to include flow rates and vascular resistance measurements—data that are not included in the aforementioned studies.
Notably, we observed lower LAP values during the POD 48 treadmill studies. On POD 47, blood could not be drawn back from the AoP and LAP lines. Cathflo Activase Alteplase (2 mg each) was injected into the AoP and LAP lines in an attempt to restore IV access and draw blood. On the following day (POD 48), blood could be drawn from the LAP line with effort, but not from the AoP line. We hypothesize that these problems with the line may have contributed to the observed lower LAP values.
A major limitation of this study was the small sample size (n = 1). To perform statistical analysis, a larger population is needed. However, conducting a study such as this is costly. Access to funding for this kind of experimental research (i.e., obtaining baseline values in an animal model) remains limited.
In conclusion, we sought to provide baseline hemodynamic values, including aortic and pulmonary blood flow, in a bovine model at rest and during exercise after a control procedure. By using these normal-range values, investigators will be able to detect any deviation from normality when developing a new device and assessing its effect on animal physiology during preclinical studies. These findings will help device engineers, researchers, and manufacturers to understand normal bovine cardiovascular physiology for technical consideration during device development for preclinical trials.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}