
Establishing a Resource to Assess Musculoskeletal Health in Older Adults in the Post-COVID-19 Era: Time to SaLSA?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
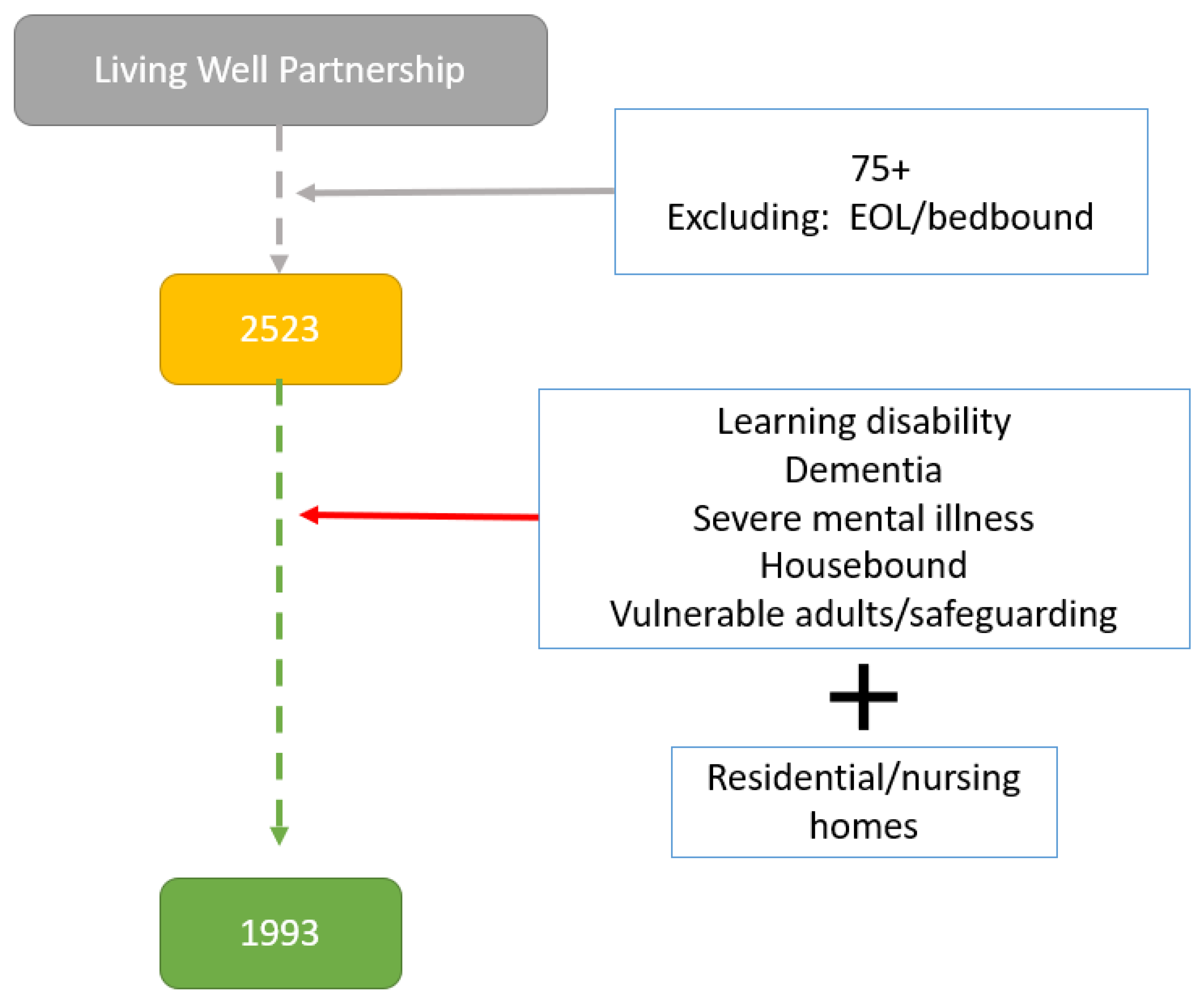
Study Design
- Patients with safeguarding issues;
- Patients with mental health and capacity issues;
- Patients with dementia or who were unable to provide consent;
- Patients with learning disabilities;
- Patients in end-of-life care;
- Patients who are permanently bedbound;
- Patients in residential or nursing homes.
3. Patient and Public Involvement (PPI)
4. Data Access
5. Results
Preliminary Sample
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Barnsley, J.; Buckland, G.; Chan, P.E.; Ong, A.; Ramos, A.S.; Baxter, M.; Laskou, F.; Dennison, E.M.; Cooper, C.; Patel, H.P. Pathophysiology and treatment of osteoporosis: Challenges for clinical practice in older people. Aging Clin. Exp. Res. 2021, 33, 759–773. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. Clin. Geriatr. Med. 2011, 27, 337–339. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, A.; Vaz, C. The role of sarcopenia in the risk of osteoporotic hip fracture. Clin. Rheumatol. 2015, 34, 1673–1680. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Shepard, D.S.; Katzmarzyk, P.T.; Roubenoff, R. The Healthcare Costs of Sarcopenia in the United States. J. Am. Geriatr. Soc. 2004, 52, 80–85. [Google Scholar] [CrossRef]
- Pinedo-Villanueva, R.; Westbury, L.D.; Syddall, H.E.; Sanchez-Santos, M.T.; Dennison, E.M.; Robinson, S.M.; Cooper, C. Health Care Costs Associated With Muscle Weakness: A UK Population-Based Estimate. Calcif. Tissue Int. 2019, 104, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Cawthon, P.M.; Manini, T.; Patel, S.M.; Newman, A.; Travison, T.; Kiel, D.P.; Santanasto, A.J.; Ensrud, K.E.; Xue, Q.L.; Shardell, M.; et al. Putative Cut-Points in Sarcopenia Components and Incident Adverse Health Outcomes: An SDOC Analysis. J. Am. Geriatr. Soc. 2020, 68, 1429–1437. [Google Scholar] [CrossRef]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Curtis, E.; Litwic, A.; Cooper, C.; Dennison, E. Determinants of Muscle and Bone Aging. J. Cell. Physiol. 2015, 230, 2618–2625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huo, Y.R.; Suriyaarachchi, P.; Gomez, F.; Curcio, C.L.; Boersma, D.; Muir, S.W.; Montero-Odasso, M.; Gunawardene, P.; Demontiero, O.; Duque, G. Phenotype of Osteosarcopenia in Older Individuals With a History of Falling. J. Am. Med. Dir. Assoc. 2015, 16, 290–295. [Google Scholar] [CrossRef]
- Hill, T.R.; Aspray, T.J. The role of vitamin D in maintaining bone health in older people. Ther. Adv. Musculoskelet. Dis. 2017, 9, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Stöcklin, E.; Sidelnikov, E.; Willett, W.C.; Edel, J.O.; Stähelin, H.B.; Wolfram, S.; Jetter, A.; Schwager, J.; et al. Oral supplementation with 25(OH)D3 versus vitamin D3: Effects on 25(OH)D levels, lower extremity function, blood pressure, and markers of innate immunity. J. Bone Miner. Res. 2012, 27, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Dennison, E. Assessment of How Older Adults Have Been Affected by COVID-19: A Look at the Hertfordshire Cohort Study-CLOSER. 2020. Available online: https://www.closer.ac.uk/news-opinion/blog/assessment-of-how-older-adults-have-been-affected/ (accessed on 26 October 2021).
- Han, M.F.Y.; Mahendran, R.; Yu, J. Associations Between Fear of COVID-19, Affective Symptoms and Risk Perception Among Community-Dwelling Older Adults During a COVID-19 Lockdown. Front. Psychol. 2021, 12, 961. [Google Scholar] [CrossRef]
- Washburn, R.A.; McAuley, E.; Katula, J.; Mihalko, S.L.; Boileau, R.A. The Physical Activity Scale for the Elderly (PASE): Evidence for Validity. J. Clin. Epidemiol. 1999, 52, 643–651. [Google Scholar] [CrossRef]
- Sinnett, S.; Bengle, R.; Brown, A.; Glass, A.P.; Johnson, M.A.; Lee, J.S. The validity of nutrition screening initiative DETERMINE Checklist responses in older Georgians. J. Nutr. Elder. 2010, 29, 393–409. [Google Scholar] [CrossRef]
- Mchorney, C.A.; Johne, W.; Anastasiae, R. The MOS 36-Item Short-Form Health Survey (SF-36). Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [Green Version]
- Bingham, S.A.; Gill, C.; Welch, A.; Day, K.; Cassidy, A.; Khaw, K.T.; Sneyd, M.J.; Key, T.J.A.; Roe, L.; Day, N.E. Comparison of dietary assessment methods in nutritional epidemiology: Weighed records v. 24 h recalls, food-frequency questionnaires and estimated-diet records. Br. J. Nutr. 1994, 72, 619–643. [Google Scholar] [CrossRef] [Green Version]
- Syddall, H.E.; Westbury, L.D.; Cooper, C.; Sayer, A.A. Self-Reported Walking Speed: A Useful Marker of Physical Performance Among Community-Dwelling Older People? J. Am. Med. Dir. Assoc. 2015, 16, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Malmstrom, T.K.; Morley, J.E. SARC-F: A simple questionnaire to rapidly diagnose sarcopenia. J. Am. Med. Dir. Assoc. 2013, 14, 531–532. [Google Scholar] [CrossRef] [PubMed]
- Syddall, H.E.; Simmonds, S.J.; Carter, S.A.; Robinson, S.M.; Dennison, E.M.; Cooper, C.; Bevilacqua, G.; Bloom, I.; Clynes, M.; Cox, K.; et al. The hertfordshire cohort study: An overview [version 1; referees: 3 approved]. F1000Research 2019, 8, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkisas, S.; Bastijns, S.; Baudry, S.; Bauer, J.; Beaudart, C.; Beckwée, D.; Cruz-Jentoft, A.; Gasowski, J.; Hobbelen, H.; Jager-Wittenaar, H.; et al. Application of ultrasound for muscle assessment in sarcopenia: 2020 SARCUS update. Eur. Geriatr. Med. 2021, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Westbury, L.D.; Dodds, R.M.; Syddall, H.E.; Baczynska, A.M.; Shaw, S.C.; Dennison, E.M.; Roberts, H.C.; Sayer, A.A.; Cooper, C.; Patel, H.P. Associations Between Objectively Measured Physical Activity, Body Composition and Sarcopenia: Findings from the Hertfordshire Sarcopenia Study (HSS). Calcif. Tissue Int. 2018, 103, 237. [Google Scholar] [CrossRef] [Green Version]
- Sample Size Calculator. Statistics Kingdom, 2017. Available online: https://www.statskingdom.com/sample_size_all.html (accessed on 26 October 2021).
- Patel, H.P.; Syddall, H.E.; Martin, H.J.; Stewart, C.E.; Cooper, C.; Sayer, A.A. Hertfordshire sarcopenia study: Design and methods. BMC Geriatr. 2010, 10, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cevei, M.; Onofrei, R.R.; Cioara, F.; Stoicanescu, D. Correlations between the Quality of Life Domains and Clinical Variables in Sarcopenic Osteoporotic Postmenopausal Women. J. Clin. Med. 2020, 9, 441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paintin, J.; Cooper, C.; Dennison, E. Osteosarcopenia. Proc. Br. J. Hosp. Med. 2018, 79, 253–258. [Google Scholar] [CrossRef]
- Patel, H.P.; Dawson, A.; Westbury, L.D.; Hasnaoui, G.; Syddall, H.E.; Shaw, S.; Sayer, A.A.; Cooper, C.; Dennison, E.M. Muscle Mass, Muscle Morphology and Bone Health Among Community-Dwelling Older Men: Findings from the Hertfordshire Sarcopenia Study (HSS). Calcif. Tissue Int. 2018, 103, 35. [Google Scholar] [CrossRef] [Green Version]
- Edwards, M.H.; Gregson, C.L.; Patel, H.P.; Jameson, K.A.; Harvey, N.C.; Sayer, A.A.; Dennison, E.M.; Cooper, C. Muscle size, strength, and physical performance and their associations with bone structure in the Hertfordshire Cohort Study. J. Bone Miner. Res. 2013, 28, 2295–2304. [Google Scholar] [CrossRef]
- Boutroy, S.; Bouxsein, M.L.; Munoz, F.; Delmas, P.D. In vivo assessment of trabecular bone microarchitecture by high-resolution peripheral quantitative computed tomography. J. Clin. Endocrinol. Metab. 2005, 90, 6508–6515. [Google Scholar] [CrossRef] [Green Version]
- Sornay-Rendu, E.; Boutroy, S.; Munoz, F.; Delmas, P.D. Alterations of cortical and trabecular architecture are associated with fractures in postmenopausal women, partially independent of decreased BMD measured by DXA: The OFELY study. J. Bone Miner. Res. 2007, 22, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.; Robinson, D.; Ward, K.; Javaid, M.; Walker-Bone, K.; Cooper, C.; Dennison, E. Cluster Analysis of Bone Microarchitecture from High Resolution Peripheral Quantitative Computed Tomography Demonstrates two Separate Phenotypes Associated with High Fracture Risk in Men and Women. Bone 2016, 88, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, E.M.; Liu, X.S.; Nickolas, T.L.; Cohen, A.; Thomas, V.; McMahon, D.J.; Zhang, C.; Yin, P.T.; Cosman, F.; Nieves, J.; et al. Abnormal Microarchitecture and Reduced Stiffness at the Radius and Tibia in Postmenopausal Women With Fractures. J. Bone Miner. Res. 2010, 25, 2572. [Google Scholar] [CrossRef] [PubMed]
- Litwic, A.E.; Westbury, L.D.; Robinson, D.E.; Ward, K.A.; Cooper, C.; Dennison, E.M. Bone Phenotype Assessed by HRpQCT and Associations with Fracture Risk in the GLOW Study. Calcif. Tissue Int. 2018, 102, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirk, B.; Zanker, J.; Duque, G. Osteosarcopenia: Epidemiology, diagnosis, and treatment—Facts and numbers. J. Cachexia. Sarcopenia Muscle 2020, 11, 609–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laskou, F.; Patel, H.P.; Cooper, C.; Dennison, E. A pas de deux of osteoporosis and sarcopenia: Osteosarcopenia. Climacteric 2022, 25, 88–95. [Google Scholar] [CrossRef]
- Hirschfeld, H.P.; Kinsella, R.; Duque, G. Osteosarcopenia: Where bone, muscle, and fat collide. Osteoporos. Int. 2017, 28, 2781–2790. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Female | Male | ||||||
|---|---|---|---|---|---|---|---|---|
| N | Median | IQR | % | N | Median | IQR | % | |
| Age | 53 | 80.53 | 77–84 | 119 | 80.4 | 77–83 | ||
| Number of medications | 53 | 5 | 3–7.75 | 117 | 4 | 3–7 | ||
| Polypharmacy (>=5) | 33 | 62.2 | 22 | 18.8 | ||||
| Number of comorbidities | 53 | 3 | 2–4 | 119 | 3 | 1–3 | ||
| Multimorbidity (>=2) | 22 | 82 | 86 | 71 | ||||
| N | N | % | N | N | % | |||
| Ethnic group | 53 | 118 | ||||||
| White | 50 | 94 | 118 | 100 | ||||
| Indian | 2 | 4 | 0 | 0 | ||||
| Black Caribbean | 1 | 2 | 0 | 0 | ||||
| Marital status | 53 | 119 | ||||||
| Alone | 36 | 68 | 38 | 32 | ||||
| Not alone (lives with friend/partner/family) | 17 | 32 | 81 | 68 | ||||
| Age leaving school | 52 | 119 | ||||||
| <=14 | 2 | 4 | 17 | 14 | ||||
| >14 | 50 | 96 | 102 | 86 | ||||
| Education after school | 52 | 119 | ||||||
| None | 24 | 46.1 | 33 | 27.7 | ||||
| Apprenticeship | 7 | 13.4 | 47 | 39.4 | ||||
| Part-time college | 8 | 15.3 | 45 | 37.8 | ||||
| Full-time college | 8 | 15.3 | 15 | 12.6 | ||||
| Other | 9 | 17.3 | 12 | 10 | ||||
| Higher qualifications | ||||||||
| None | 22 | 40 | 41 | 34 | ||||
| O levels | 23 | 42 | 48 | 40 | ||||
| A levels | 10 | 18 | 20 | 17 | ||||
| Vocational training certificate | 12 | 22 | 42 | 35 | ||||
| University degree | 1 | 2 | 20 | 17 | ||||
| Higher professional qualifications | 7 | 13 | 13 | 11 | ||||
| Smoking status | 53 | 118 | ||||||
| Ex-smoker | 20 | 71.6 | 78 | 66 | ||||
| Current smoker | 0 | 0 | 5 | 3.38 | ||||
| Alcohol | 54 | 121 | ||||||
| More than recommended units/week (14) | 1 | 1.85 | 25 | 20.6 | ||||
| COVID-19 infection | 50 | 117 | ||||||
| Yes | 0 | 0 | 4 | 3.41 | ||||
| No | 48 | 96 | 111 | 95 | ||||
| Suspected but not confirmed | 2 | 4 | 2 | 1.7 | ||||
| Self-reported walking speed | 54 | 121 | ||||||
| Fast | 2 | 4 | 1 | 1 | ||||
| Fairly brisk | 8 | 15 | 22 | 18 | ||||
| Normal speed | 13 | 24 | 40 | 33 | ||||
| Stroll at an easy pace | 15 | 28 | 34 | 28 | ||||
| Very slow | 15 | 28 | 23 | 19 | ||||
| Unable to walk | 1 | 2 | 1 | 1 | ||||
| N | N | % | N | N | % | |||
| Falls past year | 52 | 114 | ||||||
| >=1 fall | 17 | 32.6 | 28 | 24.5 | ||||
| Fracture since age 45 | 52 | 112 | ||||||
| Yes | 19 | 36.5 | 15 | 31.25 | ||||
| No | 33 | 67 | 97 | 87 | ||||
| Self-rated health (SF-36) | 53 | 120 | ||||||
| Excellent | 3 | 5.66 | 4 | 3.33 | ||||
| Very good | 13 | 24.5 | 27 | 22.5 | ||||
| Good | 19 | 35.8 | 51 | 42.5 | ||||
| Fair | 17 | 32 | 32 | 26.6 | ||||
| Poor | 1 | 1.88 | 6 | 5 | ||||
| Questionnaires |
|---|
| Living circumstances and lifestyle factors |
| COVID-19 questionnaire |
| Medical conditions and medication history |
| Physical activity scale for the elderly (PASE) |
| Self-reported walking speed |
| Bone health questionnaire |
| Fried frailty questionnaire |
| Sarcopenia questionnaire (SARC-F) |
| Quality of life questionnaire (SF-36) |
| DETERMINE checklist |
| Food frequency questionnaire (FFQ) |
| Variables | Instrument/Scale | Type of Assessment | 1st Phase | 2nd Phase |
|---|---|---|---|---|
| Age | Calculated based on the date of birth given | Questionnaire | √ | |
| Sex | Female or male stated | Questionnaire | √ | |
| Ethnicity | As self-reported | Questionnaire | √ | |
| Marital status | Self-reported marital status | Questionnaire | √ | |
| Education | Age of leaving school | Questionnaire | √ | |
| Self-reported education after school and/or higher qualifications | Questionnaire | |||
| Living arrangements | Self-reported: own property/rented accommodation/residential home/nursing home/other | Questionnaire | √ | |
| Smoking history | Self-reported as current or ex-smoker/packs/year | Questionnaire | √ | |
| Alcohol consumption | Self-reported as drinking or not alcohol and units/week | Questionnaire | √ | |
| Social status | Maastricht Social Participation Profile (MSSP), Hospital Anxiety and Depression Scale (HADS) | Questionnaire | √ | |
| Social isolation/loneliness | Six-item Lubben Social Network Scale (LSNS-6), De Jong Gierveld Short Loneliness Scale | Questionnaire | √ | |
| Occupation history | Self-reported current or previous employments | Questionnaire | √ | |
| Medical history/comorbidities | Self-recorded list of current regular medications including anti-osteoporosis medications | Questionnaire | √ | |
| Number of medications | List of medical conditions provided used previously in HCS study | Questionnaire | √ | |
| COVID-19 status | COVID-19 questionnaire developed during the pandemic and used previously in the HCS study. Assess COVID-19 infection status and symptomatology/long-term consequences; COVID-19 vaccination status | Questionnaire | √ | |
| Physical activity | Physical Activity Scale for the Elderly (PASE) | Questionnaire | √ | |
| Physical capability | Self-reported walking speed | Questionnaire | √ | |
| Frailty | Fried frailty criteria | Questionnaire and research visit | √ | √ |
| Clinical frailty scale | Research visit | √ | ||
| Frailty index (eFI) | Research visit | √ | ||
| Fractures/falls | Self-reported number of fractures since the age of 45 and in the past year X-rays and vertebral fracture assessment | Questionnaire | √ | |
| Self-reported number of falls since the age of 45 and in the past year | Questionnaire | √ | ||
| Muscle health | Strength, assistance with walking, rising from a chair, climbing stairs, and falls (SARC-F) Sarcopenia status (EWGSOP2) | Questionnaire | √ | |
| Bone, muscle, fat: density/microarchitecture/morphology | DXA scan of lumbar spine and femoral neck | Research visit | √ | |
| High-resolution peripheral quantitative computed tomography (HRpQCT) | Research visit | √ | ||
| Percutaneous muscle biopsy of vastus lateralis | Research visit | √ | ||
| Muscle ultrasound | Research visit | √ | ||
| Perceived health state | SF-36 SarQoL (sarcopenia and quality of life) | Questionnaire | √ | |
| Nutrition | DETERMINE checklist—identifying malnutrition | Questionnaire | √ | |
| Food frequency questionnaire—assessing habitual diet | Questionnaire | √ | ||
| Anthropometric measurements | Weight, height, BMI, waist, hip, mid–upper arm, and thigh circumferences | Research visit | √ | |
| Triceps, biceps, subscapular, and supra-iliac skinfold thicknesses | Research visit | √ | ||
| Blood pressure, pulse rate | Research visit | √ | ||
| Cardiovascular assessment | Standard 12-lead electrocardiograph | Research visit | √ | |
| Blood profile | Fasting blood samples to be taken from the anterior cubital fossa for subsequent glucose, insulin, HbA1c, bone profile, albumin, lipid profile, vitamin D, vitamin C, hormonal, inflammatory, and DNA analyses, for posterity and further assays; | Research visit | √ | |
| Physical performance | Grip strength (Jamar hand-grip dynamometer) Quadriceps strength Timed 6 m up-and-go test and 3 m walk Chair rises Timed one-legged stand | Research visit | √ | |
| Cognitive function | AMTS 1/MoCA 2 | Research visit | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laskou, F.; Linfield, A.; Aggarwal, P.; Dennison, E.M.; Patel, H.P. Establishing a Resource to Assess Musculoskeletal Health in Older Adults in the Post-COVID-19 Era: Time to SaLSA? Osteology 2022, 2, 41-51. https://doi.org/10.3390/osteology2010005
Laskou F, Linfield A, Aggarwal P, Dennison EM, Patel HP. Establishing a Resource to Assess Musculoskeletal Health in Older Adults in the Post-COVID-19 Era: Time to SaLSA? Osteology. 2022; 2(1):41-51. https://doi.org/10.3390/osteology2010005
Chicago/Turabian StyleLaskou, Faidra, Alexander Linfield, Pritti Aggarwal, Elaine M. Dennison, and Harnish P. Patel. 2022. "Establishing a Resource to Assess Musculoskeletal Health in Older Adults in the Post-COVID-19 Era: Time to SaLSA?" Osteology 2, no. 1: 41-51. https://doi.org/10.3390/osteology2010005