
Multi-Level Fibrotomy for Pediatric Patients with Cerebral Palsy: A Cohort Study


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Variables and Measurement
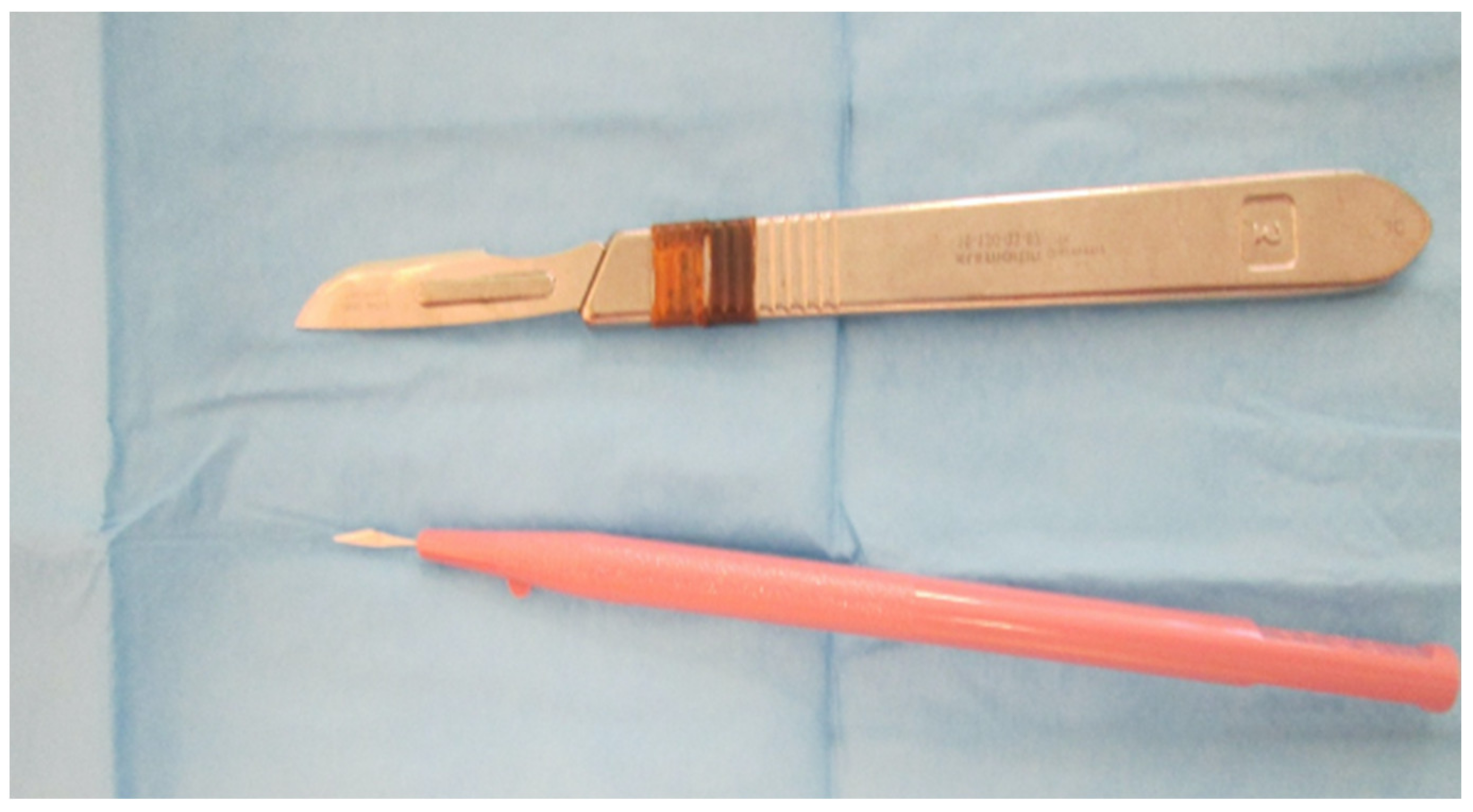
2.4. Surgical Devices
2.5. Surgical Technique
3. Results
3.1. Participants
3.2. Main Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vlachou, M.; Pierce, R.; Davis, R.M.; Sussman, M. Does Tendon Lengthening Surgery Affect Muscle Tone in Children with Cerebral Palsy? Acta Orthop. Belg. 2009, 75, 808–814. [Google Scholar]
- Thompson, N.; Stebbins, J.; Seniorou, M.; Wainwright, A.M.; Newham, D.J.; Theologis, T.N. The Use of Minimally Invasive Techniques in Multi-Level Surgery for Children with Cerebral Palsy: PRELIMINARY RESULTS. J. Bone Joint Surg. Br. 2010, 92-B, 1442–1448. [Google Scholar] [CrossRef]
- Genêt, F.; Denormandie, P.; Keenan, M.A. Orthopaedic Surgery for Patients with Central Nervous System Lesions: Concepts and Techniques. Ann. Phys. Rehabil. Med. 2019, 62, 225–233. [Google Scholar] [CrossRef]
- Longo, U.G.; Salvatore, G.; Risi Ambrogioni, L.; Cella, E.; Candela, V.; Carnevale, A.; Schena, E.; Ciccozzi, M.; Maffulli, N.; Denaro, V. Epidemiology of Achilles Tendon Surgery in Italy: A Nationwide Registry Study, from 2001 through 2015. BMC Musculoskelet. Disord. 2020, 21, 687. [Google Scholar] [CrossRef]
- Haberfehlner, H.; Jaspers, R.T.; Rutz, E.; Harlaar, J.; van der Sluijs, J.A.; Witbreuk, M.M.; van Hutten, K.; Romkes, J.; Freslier, M.; Brunner, R.; et al. Outcome of Medial Hamstring Lengthening in Children with Spastic Paresis: A Biomechanical and Morphological Observational Study. PLoS ONE 2018, 13, e0192573. [Google Scholar] [CrossRef]
- Jaddue, D.; Abbas, M.; Sayed-Noor, A. Open versus Percutaneous Tendo-Achilles Lengthening in Spastic Cerebral Palsy with Equines Deformity of the Foot in Children. J. Surg. Orthop. Adv. 2010, 19, 196–199. [Google Scholar]
- Khaje Mozafari, J.; Pisoudeh, K.; Gharanizade, K.; Abolghasemian, M. Percutaneous Versus Open Hamstring Lengthening in Spastic Diplegic Cerebral Palsy. Arch. Bone Jt. Surg. 2019, 7, 373–378. [Google Scholar]
- Kläusler, M.; Speth, B.M.; Brunner, R.; Tirosh, O.; Camathias, C.; Rutz, E. Long-Term Follow-up after Tibialis Anterior Tendon Shortening in Combination with Achilles Tendon Lengthening in Spastic Equinus in Cerebral Palsy. Gait Posture 2017, 58, 457–462. [Google Scholar] [CrossRef]
- Lin, C.-L.; Lin, C.-J.; Huang, M.-T.; Su, W.-R.; Wu, T.-T. Mesh Achilles Tendon Lengthening--a New Method to Treat Equinus Deformity in Patients with Spastic Cerebral Palsy: Surgical Technique and Early Results. J. Pediatr. Orthop. Part B 2013, 22, 14–19. [Google Scholar] [CrossRef]
- Nazareth, A.; Rethlefsen, S.; Sousa, T.C.; Mueske, N.M.; Wren, T.A.L.; Kay, R.M. Percutaneous Hamstring Lengthening Surgery Is as Effective as Open Lengthening in Children With Cerebral Palsy. J. Pediatr. Orthop. 2019, 39, 366–371. [Google Scholar] [CrossRef]
- Turhan, Y.; Arıcan, M. Clinical Comparison of Percutaneous and Open Hamstring Lengthening in Children with Spastic Cerebral Palsy. Medeni. Med. J. 2019, 34, 182–187. [Google Scholar] [CrossRef]
- Katz, K.; Arbel, N.; Apter, N.; Soudry, M. Early Mobilization after Sliding Achilles Tendon Lengthening in Children with Spastic Cerebral Palsy. Foot Ankle Int. 2000, 21, 1011–1014. [Google Scholar] [CrossRef]
- Comparison of Proximal and Distal Rotational Femoral Osteotomy in Children with Cerebral Palsy—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/12604941/ (accessed on 1 July 2021).
- Pirpiris, M.; Trivett, A.; Baker, R.; Rodda, J.; Nattrass, G.R.; Graham, H.K. Femoral Derotation Osteotomy in Spastic Diplegia. Proximal or Distal? J. Bone Joint Surg. Br. 2003, 85, 265–272. [Google Scholar] [CrossRef] [Green Version]
- Damiano, D.L.; Abel, M.F.; Pannunzio, M.; Romano, J.P. Interrelationships of Strength and Gait before and after Hamstrings Lengthening. J. Pediatr. Orthop. 1999, 19, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Brunner, R. [Muscle physiology and the effect of muscle-tendon surgery in cerebral palsy]. Orthopade 2004, 33, 1096–1102. [Google Scholar] [CrossRef]
- Gillani, S.F.U.H.S.; Rafique, A.; Taqi, M.; Chatta, M.A.U.H.; Masood, F.; Ahmad Blouch, T.; Awais, S.M. Effectiveness of Treatment in Children With Cerebral Palsy. Cureus 2021, 13, e13754. [Google Scholar] [CrossRef]
- Edwards, T.A.; Thompson, N.; Prescott, R.J.; Stebbins, J.; Wright, J.G.; Theologis, T. A Comparison of Conventional and Minimally Invasive Multilevel Surgery for Children with Diplegic Cerebral Palsy. Bone Jt. J. 2021, 103-B, 192–197. [Google Scholar] [CrossRef]
- El Hage, S.; Rachkidi, R.; Noun, Z.; Haidar, R.; Dagher, F.; Kharrat, K.; Ghanem, I. Is Percutaneous Adductor Tenotomy as Effective and Safe as the Open Procedure? J. Pediatr. Orthop. 2010, 30, 485–488. [Google Scholar] [CrossRef] [Green Version]
- De Pavía-Mota, E.; Neri-Gámez, S.; Reyes-Contreras, G.; Valencia-Posadas, M. Percutaneous tenotomy and aponeurotomy (PTA) for knee flexor contracture in children with spastic cerebral palsy. Acta Ortop. Mex. 2013, 27, 109–113. [Google Scholar]
- Bozinovski, Z.; Popovski, N. Operative Treatment of the Knee Contractures in Cerebral Palsy Patients. Med. Arch. Sarajevo Bosnia Herzeg. 2014, 68, 182–183. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, E.; Rosenbaum, P. The Gross Motor Function Classification System for Cerebral Palsy: A Study of Reliability and Stability over Time. Dev. Med. Child Neurol. 2007, 42, 292–296. [Google Scholar] [CrossRef]
- Faiz, K.W. [VAS--visual analog scale]. Tidsskr. Den Nor. Laegeforening Tidsskr. Prakt. Med. Ny Raekke 2014, 134, 323. [Google Scholar] [CrossRef]
- Shields, B.J.; Palermo, T.M.; Powers, J.D.; Grewe, S.D.; Smith, G.A. Predictors of a Child’s Ability to Use a Visual Analogue Scale. Child Care Health Dev. 2003, 29, 281–290. [Google Scholar] [CrossRef]
- Gómez-Andrés, D.; Pulido-Valdeolivas, I.; Martín-Gonzalo, J.A.; López-López, J.; Martínez-Caballero, I.; Gómez-Barrena, E.; Rausell, E. [External evaluation of gait and functional changes after a single-session multiple myofibrotenotomy in school-aged children with spastic diplegia]. Rev. Neurol. 2014, 58, 247–254. [Google Scholar]
- Dietz, F.R.; Albright, J.C.; Dolan, L. Medium Term Follow-up of Achilles Tendon Lengthening in the Treatment of Ankle Equinus in Cerebral Palsy. Iowa Orthop. J. 2006, 26, 27–32. [Google Scholar] [PubMed]
- Gordon, A.B.; Baird, G.O.; McMulkin, M.L.; Caskey, P.M.; Ferguson, R.L. Gait Analysis Outcomes of Percutaneous Medial Hamstring Tenotomies in Children with Cerebral Palsy. J. Pediatr. Orthop. 2008, 28, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Bernius, P. The Ulzibat Method – a New Surgical Technique. Neuropediatrics 2013, 44, PS11_1127. [Google Scholar] [CrossRef]
- Bar-On, L.; Molenaers, G.; Aertbeliën, E.; Van Campenhout, A.; Feys, H.; Nuttin, B.; Desloovere, K. Spasticity and Its Contribution to Hypertonia in Cerebral Palsy. BioMed Res. Int. 2015, 2015. [Google Scholar] [CrossRef]
- Anand, N.; Baron, E.M.; Thaiyananthan, G.; Khalsa, K.; Goldstein, T.B. Minimally Invasive Multilevel Percutaneous Correction and Fusion for Adult Lumbar Degenerative Scoliosis: A Technique and Feasibility Study. J. Spinal Disord. Tech. 2008, 21, 459–467. [Google Scholar] [CrossRef]
- Kalkman, B.M.; Bar-On, L.; Cenni, F.; Maganaris, C.N.; Bass, A.; Holmes, G.; Desloovere, K.; Barton, G.J.; O’Brien, T.D. Muscle and Tendon Lengthening Behaviour of the Medial Gastrocnemius during Ankle Joint Rotation in Children with Cerebral Palsy. Exp. Physiol. 2018, 103, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Krupiński, M.; Borowski, A.; Synder, M. Long Term Follow-up of Subcutaneous Achilles Tendon Lengthening in the Treatment of Spastic Equinus Foot in Patients with Cerebral Palsy. Ortop. Traumatol. Rehabil. 2015, 17, 155–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansour, T.; Derienne, J.; Daher, M.; Sarraf, D.; Zoghbi, Y.; Ghanem, I. Is Percutaneous Medial Hamstring Myofascial Lengthening as Anatomically Effective and Safe as the Open Procedure? J. Child. Orthop. 2017, 11, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, S.; Mutsuzaki, H.; Mataki, Y.; Takeuchi, R.; Kamada, H. A New Tendon-Lengthening Technique Using a Tendon Stripper for Knee Flexion Contracture in a Cerebral Palsy Patient. J. Orthop. 2020, 18, 110–112. [Google Scholar] [CrossRef]
- Sahu, R.L. Percutaneous Adductor Release in Nonambulant Children with Cerebral Palsy. JNMA J. Nepal Med. Assoc. 2014, 52, 702–706. [Google Scholar] [CrossRef]
- Uyttendaele, D.; Burssens, P.; Pollefliet, A.; Claessens, H. Simultaneous Achilles and Tibialis Posterior Tendon Lengthening in Cerebral Palsy. Acta Orthop. Belg. 1989, 55, 62–66. [Google Scholar] [PubMed]
- Norlin, R.; Tkaczuk, H. One-Session Surgery for Correction of Lower Extremity Deformities in Children with Cerebral Palsy. J. Pediatr. Orthop. 1985, 5, 208–211. [Google Scholar] [CrossRef] [PubMed]
- McGinley, J.L.; Dobson, F.; Ganeshalingam, R.; Shore, B.J.; Rutz, E.; Graham, H.K. Single-Event Multilevel Surgery for Children with Cerebral Palsy: A Systematic Review. Dev. Med. Child Neurol. 2012, 54, 117–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomason, P.; Selber, P.; Graham, H.K. Single Event Multilevel Surgery in Children with Bilateral Spastic Cerebral Palsy: A 5 Year Prospective Cohort Study. Gait Posture 2013, 37, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Schranz, C.; Kruse, A.; Kraus, T.; Steinwender, G.; Svehlik, M. Does Unilateral Single-Event Multilevel Surgery Improve Gait in Children with Spastic Hemiplegia? A Retrospective Analysis of a Long-Term Follow-Up. Gait Posture 2017, 52, 135–139. [Google Scholar] [CrossRef]
- Carbonell, P.G. Compartmental Pressure after Percutaneous Tenotomy of the Achilles Tendon in Children with Infantile Cerebral Palsy. Childs Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2015, 31, 297–300. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients Demographics |
|---|
| Sex (M/F) 110/79 |
| GMFCS level (II/III) 92/97 |
| Age at operation (y) 12.81 ± 6.47 (2–18) |
| Mean Follow-up duration (months) 20.6 (6–64) |
| Surgical procedures |
| Adductors of the hip 149 (R: 2; L: 3; B: 72) |
| Hamstrings 158 (R: 8; L: 4; B: 73) |
| Posterior Tibialis 14 (R: 3; L: 3; B: 4) |
| Achilleus tendons 164 (R: 29; L: 21; B: 57) |
| Mean preoperative ROM |
| Hip abduction 11.3 ± 6.4° |
| Knee extension −81 ± 14.6° |
| Ankle dorsiflexion 26 ± 4.9° |
| Total 485 (2.5 ± 1.4 per patient) |
| Data are presented as mean SD. |
| GMFCS indicates Gross Motor Function Classification System. |
| R: right; L: left; B: bilateral |
| Results of Outcomes after Surgery |
|---|
| Operation time: 15.6 ± 12,3 min per site |
| Blood loss: not evaluable (less than 20 cc) |
| Postoperative pain (VAS assessed in 84 eligible patients): 3.8 ± 1.2 |
| Drug consumption after surgery: paracetamol and 7 ketorolac (no opioids) |
| Casting time: 24 h |
| Days of hospitalization: 2.2 (range: 1–4) |
| ROM mean change |
| Hip abduction: + 27.9 ± 1.0°; p < 0.05 |
| Knee extension: + 21.5 ± 0.5°; p < 0.05 |
| Ankle extension: + 17.0 ± 1.7°; p < 0.05 |
| Data presented as mean and SD. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costici, P.F.; De Salvatore, S.; Russo, R.; Oggiano, L.; Burrofato, A.; Donati, F.; Ruzzini, L. Multi-Level Fibrotomy for Pediatric Patients with Cerebral Palsy: A Cohort Study. Osteology 2021, 1, 141-148. https://doi.org/10.3390/osteology1030015
Costici PF, De Salvatore S, Russo R, Oggiano L, Burrofato A, Donati F, Ruzzini L. Multi-Level Fibrotomy for Pediatric Patients with Cerebral Palsy: A Cohort Study. Osteology. 2021; 1(3):141-148. https://doi.org/10.3390/osteology1030015
Chicago/Turabian StyleCostici, Pier Francesco, Sergio De Salvatore, Rosa Russo, Leonardo Oggiano, Aaron Burrofato, Fabrizio Donati, and Laura Ruzzini. 2021. "Multi-Level Fibrotomy for Pediatric Patients with Cerebral Palsy: A Cohort Study" Osteology 1, no. 3: 141-148. https://doi.org/10.3390/osteology1030015