Comparative Evaluation of Primary Stability between Different Diameters Multi-Scale Roughness Dental Implant by Solid Rigid Polyurethane Simulation

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Polyurethane Foam Blocks
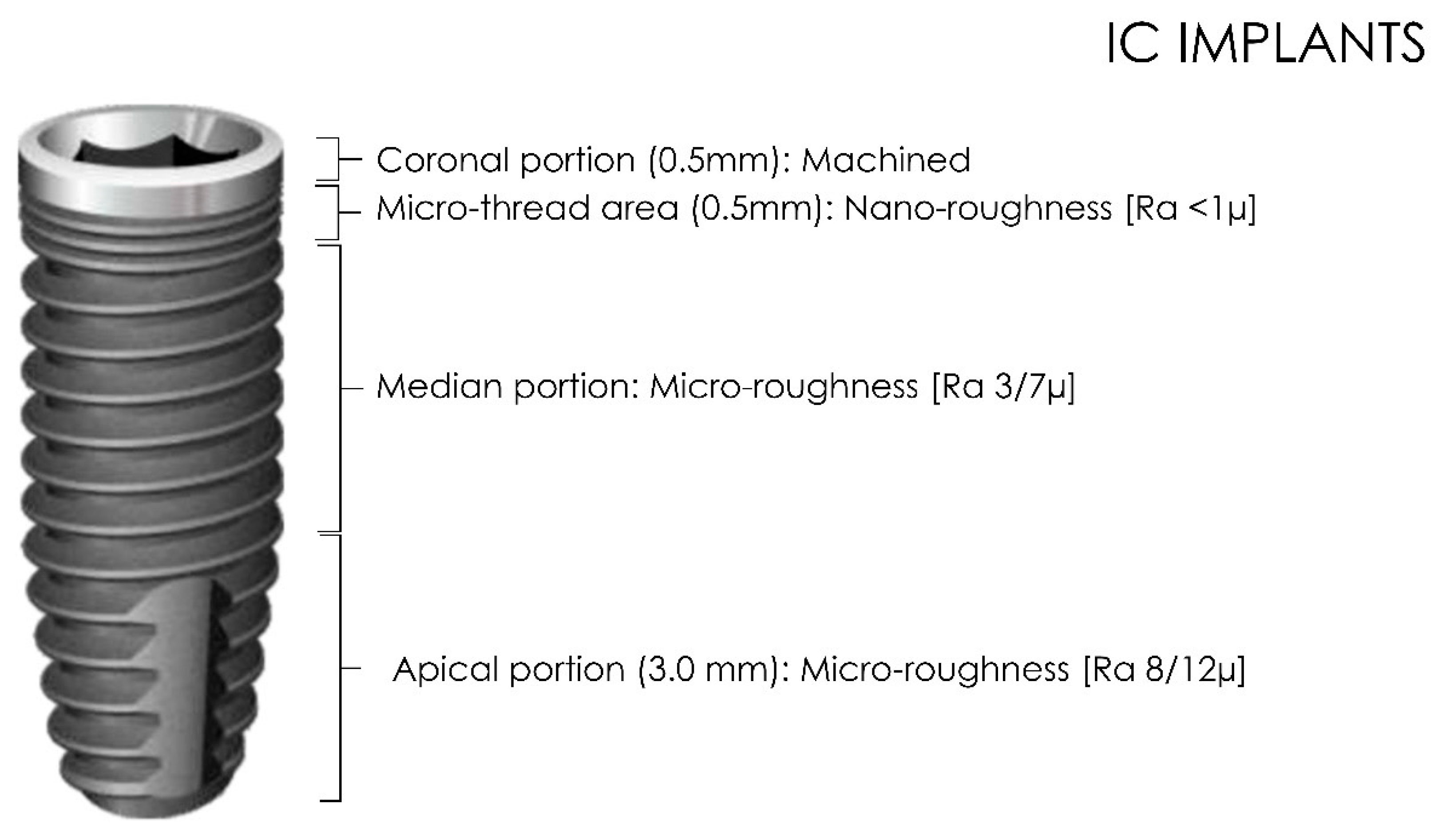
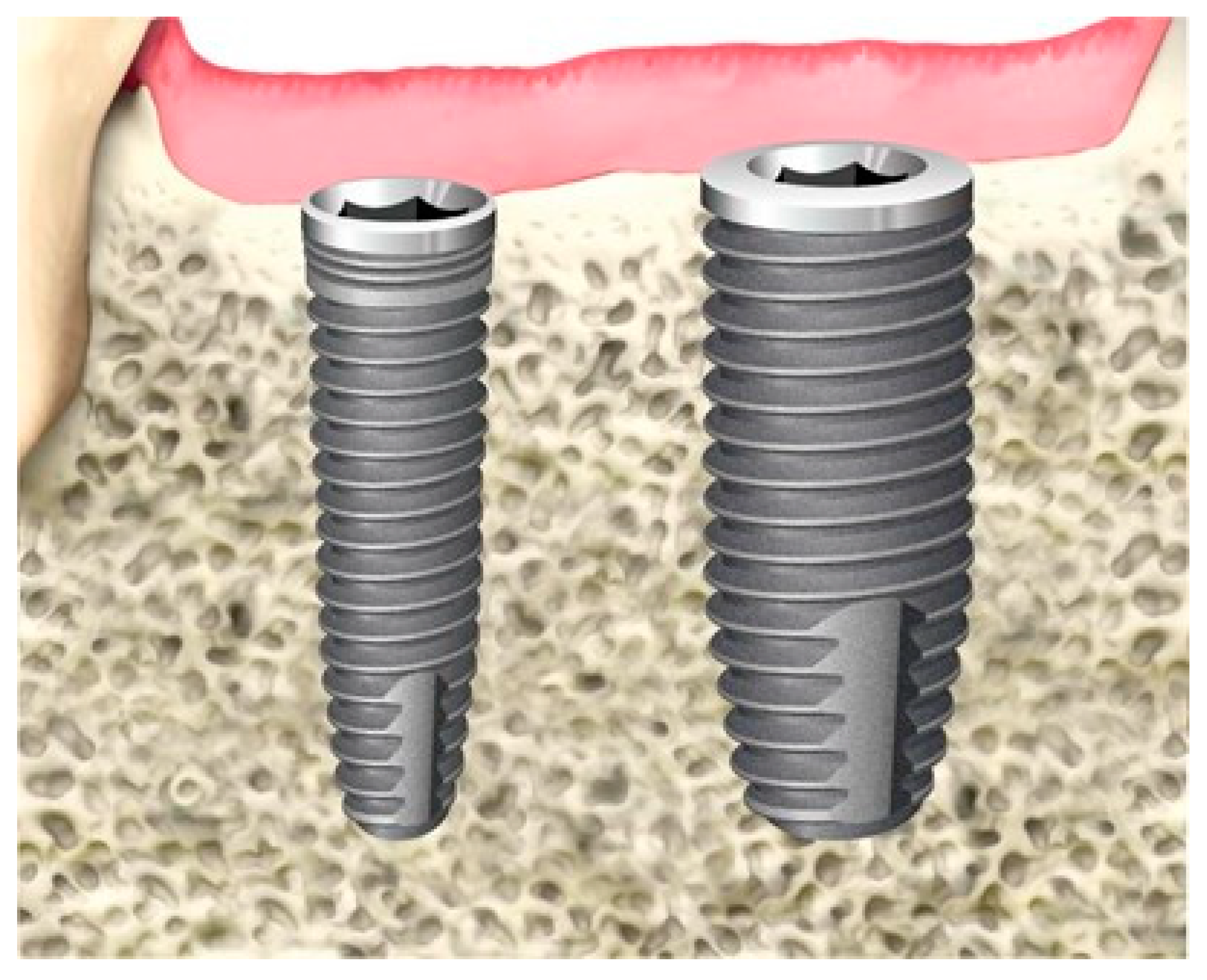
2.2. Implant Characteristics
2.3. Drilling Protocol and Insertion (IT) and Removal Torque (RT) Assessment
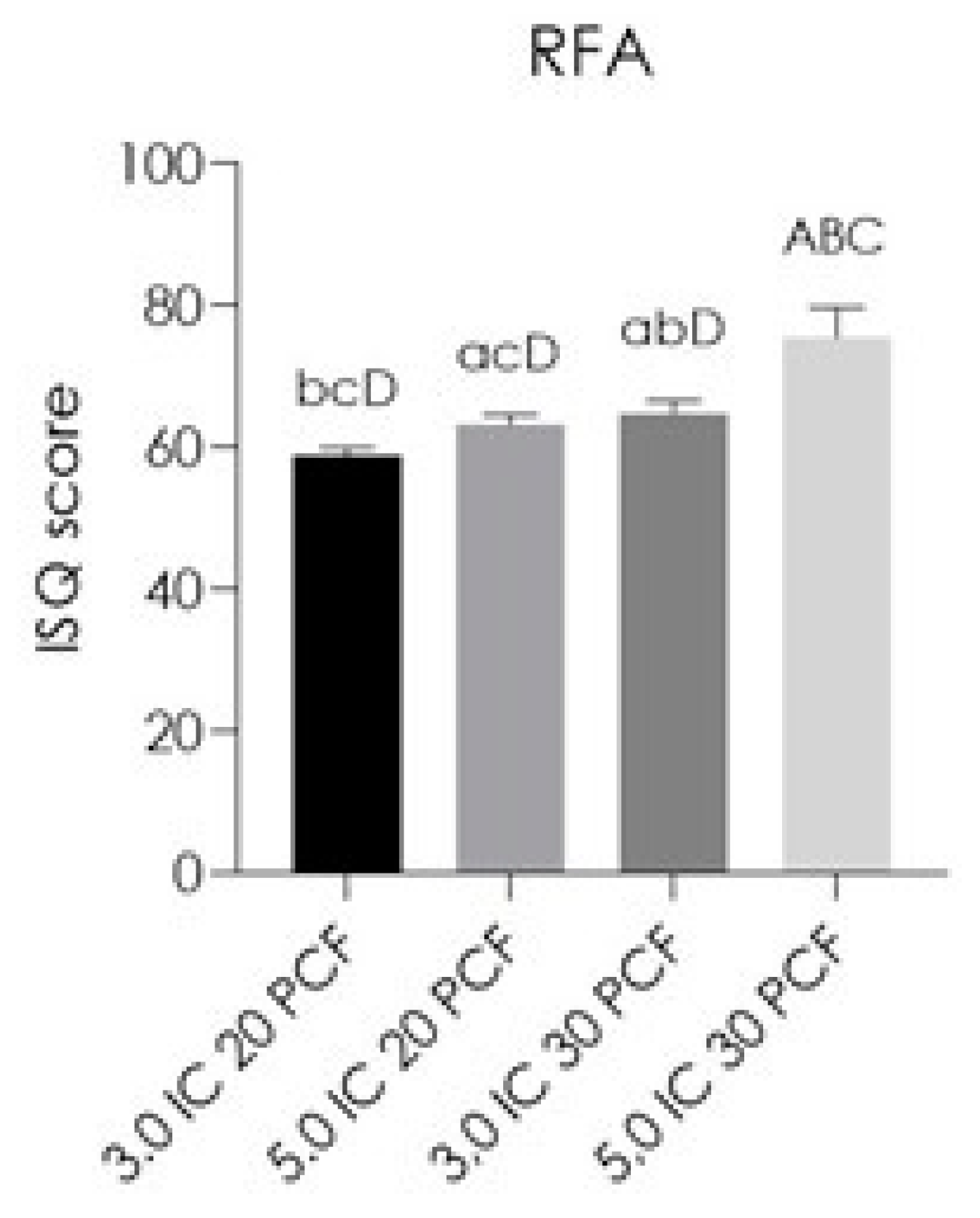
2.4. Resonance Frequency Analysis (RFA)
- -
- Good stability: >70 implant stability quotient (ISQ);
- -
- Medium stability: 60–69 implant stability quotient (ISQ);
- -
- Low stability: <60 implant stability quotient (ISQ).
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Monje, A.; Ravidà, A.; Wang, H.-L.; Helms, J.A.; Brunski, J.B. Relationship Between Primary/Mechanical and Secondary/Biological Implant Stability. Int. J. Oral Maxillofac. Implant. 2019, 34, s7–s23. [Google Scholar] [CrossRef]
- Di Stefano, D.A.; Arosio, P.; Gastaldi, G.; Gherlone, E. The Insertion Torque-Depth Curve Integral as a Measure of Implant Primary Stability: An In Vitro Study on Polyurethane Foam Blocks. J. Prosthet. Dent. 2018, 120, 706–714. [Google Scholar] [CrossRef]
- Davies, J.E. Understanding Peri-Implant Endosseous Healing. J. Dent. Educ. 2003, 67, 932–949. [Google Scholar] [CrossRef]
- de Oliveira Nicolau Mantovani, A.K.; de Mattias Sartori, I.A.; Azevedo-Alanis, L.R.; Tiossi, R.; Fontão, F.N.G.K. Influence of Cortical Bone Anchorage on the Primary Stability of Dental Implants. Oral Maxillofac. Surg. 2018, 22, 297–301. [Google Scholar] [CrossRef]
- Comuzzi, L.; Tumedei, M.; Pontes, A.E.; Piattelli, A.; Iezzi, G. Primary Stability of Dental Implants in Low-Density (10 and 20 Pcf) Polyurethane Foam Blocks: Conical vs Cylindrical Implants. Int. J. Environ. Res. Public Health 2020, 17, 2617. [Google Scholar] [CrossRef] [Green Version]
- Del Giudice, R.; Piattelli, A.; Grande, N.-M.; Cataneo, E.; Crispino, A.; Petrini, M. Implant Insertion Torque Value in Immediate Loading: A Retrospective Study. Med. Oralpatol. Oral Y Cir. Bucal 2019, 24, e398–e403. [Google Scholar] [CrossRef] [PubMed]
- Tumedei, M.; Piattelli, A.; Degidi, M.; Mangano, C.; Iezzi, G. A 30-Year (1988–2018) Retrospective Microscopical Evaluation of Dental Implants Retrieved for Different Causes: A Narrative Review. Int. J. Periodontics Restor. Dent. 2020, 40, e211–e227. [Google Scholar] [CrossRef] [PubMed]
- Goellner, M.; Schmitt, J.; Karl, M.; Wichmann, M.; Holst, S. The Effect of Axial and Oblique Loading on the Micromovement of Dental Implants. Int. J. Oral Maxillofac. Implant. 2011, 26, 257–264. [Google Scholar]
- Freitas, A.C.; Bonfante, E.A.; Giro, G.; Janal, M.N.; Coelho, P.G. The Effect of Implant Design on Insertion Torque and Immediate Micromotion. Clin. Oral Implant. Res. 2012, 23, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Tumedei, M.; Piattelli, A.; Degidi, M.; Mangano, C.; Iezzi, G. A Narrative Review of the Histological and Histomorphometrical Evaluation of the Peri-Implant Bone in Loaded and Unloaded Dental Implants. A 30-Year Experience (1988–2018). Int. J. Environ. Res. Public Health 2020, 17, 2088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comuzzi, L.; Tumedei, M.; Piattelli, A.; Iezzi, G. Short vs. Standard Length Cone Morse Connection Implants: An In Vitro Pilot Study in Low Density Polyurethane Foam. Symmetry 2019, 11, 1349. [Google Scholar] [CrossRef] [Green Version]
- Fujiwara, S.; Kato, S.; Bengazi, F.; Urbizo Velez, J.; Tumedei, M.; Kotsu, M.; Botticelli, D. Healing at Implants Installed in Osteotomies Prepared Either with a Piezoelectric Device or Drills: An Experimental Study in Dogs. Oral Maxillofac. Surg. 2020, 25, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Kotsu, M.; Urbizo Velez, J.; Bengazi, F.; Tumedei, M.; Fujiwara, S.; Kato, S.; Botticelli, D. Healing at Implants Installed from ~70- to <10-Ncm Insertion Torques: An Experimental Study in Dogs. Oral Maxillofac. Surg. 2020, 25, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Al-Sabbagh, M.; Eldomiaty, W.; Khabbaz, Y. Can Osseointegration Be Achieved Without Primary Stability? Dent. Clin. N. Am. 2019, 63, 461–473. [Google Scholar] [CrossRef]
- Greenstein, G.; Cavallaro, J. Implant Insertion Torque: Its Role in Achieving Primary Stability of Restorable Dental Implants. Compend. Contin. Educ. Dent. (Jamesburg NJ) 2017, 38, 88–95. [Google Scholar]
- Palaskar, J.N.; Joshi, N.; Shah, P.M.; Gullapalli, P.; Vinay, V. Influence of Different Implant Placement Techniques to Improve Primary Implant Stability in Low-Density Bone: A Systematic Review. J. Indian Prosthodont. Soc. 2020, 20, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Carinci, F.; Lorusso, F.; Festa, F.; Bevilacqua, L.; Santos de Oliveira, P.; Maglione, M. Ultrasonic vs Drill Implant Site Preparation: Post-Operative Pain Measurement Through VAS, Swelling and Crestal Bone Remodeling: A Randomized Clinical Study. Materials (Basel Switz.) 2018, 11, 2516. [Google Scholar] [CrossRef] [Green Version]
- Scarano, A.; Lorusso, F.; Noumbissi, S. Infrared Thermographic Evaluation of Temperature Modifications Induced during Implant Site Preparation with Steel vs. Zirconia Implant Drill. J. Clin. Med. 2020, 9, 148. [Google Scholar] [CrossRef] [Green Version]
- Scarano, A.; Crincoli, V.; Di Benedetto, A.; Cozzolino, V.; Lorusso, F.; Podaliri Vulpiani, M.; Grano, M.; Kalemaj, Z.; Mori, G.; Grassi, F.R. Bone Regeneration Induced by Bone Porcine Block with Bone Marrow Stromal Stem Cells in a Minipig Model of Mandibular “Critical Size” Defect. Stem Cells Int. 2017, 2017, 9082869. [Google Scholar] [CrossRef]
- Scarano, A.; Petrini, M.; Mastrangelo, F.; Noumbissi, S.; Lorusso, F. The Effects of Liquid Disinfection and Heat Sterilization Processes on Implant Drill Roughness: Energy Dispersion X-Ray Microanalysis and Infrared Thermography. J. Clin. Med. 2020, 9, 1019. [Google Scholar] [CrossRef] [Green Version]
- Pai, U.Y.; Rodrigues, S.J.; Talreja, K.S.; Mundathaje, M. Osseodensification—A Novel Approach in Implant Dentistry. J. Indian Prosthodont. Soc. 2018, 18, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Fanali, S.; Tumedei, M.; Pignatelli, P.; Inchingolo, F.; Pennacchietti, P.; Pace, G.; Piattelli, A. Implant Primary Stability with an Osteocondensation Drilling Protocol in Different Density Polyurethane Blocks. Comput. Methods Biomech. Biomed. Eng. 2020, 25, 1–7. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Mazón, P.; Del Fabbro, M.; Tumedei, M.; Aramburú Júnior, J.; Pérez-Díaz, L.; De Aza, P.N. Histological and Histomorphometric Analyses of Two Bovine Bone Blocks Implanted in Rabbit Calvaria. Symmetry 2019, 11, 641. [Google Scholar] [CrossRef] [Green Version]
- Vayron, R.; Mathieu, V.; Michel, A.; Haïat, G. Assessment of in Vitro Dental Implant Primary Stability Using an Ultrasonic Method. Ultrasound Med. Biol. 2014, 40, 2885–2894. [Google Scholar] [CrossRef]
- Zizzari, V.L.; Berardi, D.; Congedi, F.; Tumedei, M.; Cataldi, A.; Perfetti, G. Morphological Aspect and INOS and Bax Expression Modification in Bone Tissue Around Dental Implants Positioned Using Piezoelectric Bone Surgery Versus Conventional Drill Technique. J. Craniofacial Surg. 2015, 26, 741–744. [Google Scholar] [CrossRef] [PubMed]
- Al-Almaie, S. Osteotome-Assisted Lateral Bone Expansion and Condensation with Immediate Dental Implants Placements. 2017. Available online: https://academicreads.com/wp-content/uploads/2017/10/DI-17-04-1_C.pdf (accessed on 12 December 2020).
- Degidi, M.; Daprile, G.; Piattelli, A. Influence of Underpreparation on Primary Stability of Implants Inserted in Poor Quality Bone Sites: An in Vitro Study. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2015, 73, 1084–1088. [Google Scholar] [CrossRef]
- Anitua, E.; Murias-Freijo, A.; Alkhraisat, M.H. Implant Site Under-Preparation to Compensate the Remodeling of an Autologous Bone Block Graft. J. Craniofacial Surg. 2015, 26, e374–e377. [Google Scholar] [CrossRef]
- Falisi, G.; Severino, M.; Rastelli, C.; Bernardi, S.; Caruso, S.; Galli, M.; Lamazza, L.; Di Paolo, C. The Effects of Surgical Preparation Techniques and Implant Macro-Geometry on Primary Stability: An in Vitro Study. Med. Oralpatol. Oral Y Cir. Bucal 2017, 22, e201–e206. [Google Scholar] [CrossRef]
- Comuzzi, L.; Iezzi, G.; Piattelli, A.; Tumedei, M. An In Vitro Evaluation, on Polyurethane Foam Sheets, of the Insertion Torque (IT) Values, Pull-Out Torque Values, and Resonance Frequency Analysis (RFA) of NanoShort Dental Implants. Polymers 2019, 11, 1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staedt, H.; Palarie, V.; Staedt, A.; Wolf, J.M.; Lehmann, K.M.; Ottl, P.; Kämmerer, P.W. Primary Stability of Cylindrical and Conical Dental Implants in Relation to Insertion Torque-A Comparative Ex Vivo Evaluation. Implant Dent. 2017, 26, 250–255. [Google Scholar] [CrossRef]
- Kastala, V.H.; Ramoji Rao, M.V. Comparative Evaluation of Implant Stability in Two Different Implant Systems at Baseline and 3-4 Months Intervals Using RFA Device (OSSTELL ISQ). Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2019, 30, 678–686. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Tumedei, M.; Aramburú Júnior, J.; Treichel, T.L.E.; Kolerman, R.; Lepore, S.; Piattelli, A.; Iezzi, G. Histological and Histomorphometrical Evaluation of a New Implant Macrogeometry. A Sheep Study. Int. J. Environ. Res. Public Health 2020, 17, 3477. [Google Scholar] [CrossRef]
- Miyashiro, M.; Suedam, V.; Moretti Neto, R.T.; Ferreira, P.M.; Rubo, J.H. Validation of an Experimental Polyurethane Model for Biomechanical Studies on Implant Supported Prosthesis--Tension Tests. J. Appl. Oral Sci. Rev. Fob 2011, 19, 244–248. [Google Scholar] [CrossRef] [Green Version]
- Scarano, A.; Iezzi, G.; Perrotti, V.; Tetè, S.; Staiti, G.; Mortellaro, C.; Cappucci, C. Ultrasonic versus Drills Implant Site Preparation: A Histologic Analysis in Bovine Ribs. J. Craniofacial Surg. 2014, 25, 814–817. [Google Scholar] [CrossRef] [PubMed]
- Trisi, P.; Berardini, M.; Falco, A.; Podaliri Vulpiani, M. New Osseodensification Implant Site Preparation Method to Increase Bone Density in Low-Density Bone: In Vivo Evaluation in Sheep. Implant Dent. 2016, 25, 24–31. [Google Scholar] [CrossRef] [Green Version]
- Kalemaj, Z.; Scarano, A.; Valbonetti, L.; Rapone, B.; Grassi, F.R. Bone Response to Four Dental Implants with Different Surface Topographies: A Histologic and Histometric Study in Minipigs. Int. J. Periodontics Restor. Dent. 2016, 36, 745–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Möhlhenrich, S.C.; Heussen, N.; Winterhalder, P.; Prescher, A.; Hölzle, F.; Modabber, A.; Wolf, M.; Kniha, K. Predicting Primary Stability of Orthodontic Mini-Implants, According to Position, Screw-Size, and Bone Quality, in the Maxilla of Aged Patients: A Cadaveric Study. Eur. J. Oral Sci. 2019, 127, 462–471. [Google Scholar] [CrossRef] [PubMed]
- ASTM. ASTM F 67-95: Standard Specification for Unalloyed Titanium for Surgical Implant Applications. In Annual Book of ASTM Standards; American Society for Testing and Materials: Philadelphia, PA, USA, 1995. [Google Scholar]
- Dental Implants Market Report Size, Share, Growth & Report [2027]. Available online: https://www.fortunebusinessinsights.com/industry-reports/dental-implants-market-100443 (accessed on 20 February 2021).
- Hsu, J.-T.; Shen, Y.-W.; Kuo, C.-W.; Wang, R.-T.; Fuh, L.-J.; Huang, H.-L. Impacts of 3D Bone-to- Implant Contact and Implant Diameter on Primary Stability of Dental Implant. J. Formos. Med Assoc./Taiwan Yi Zhi 2017, 116, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Tarnow, D.P.; Cho, S.C.; Wallace, S.S. The Effect of Inter-Implant Distance on the Height of Inter-Implant Bone Crest. J. Periodontol. 2000, 71, 546–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarnow, D.; Elian, N.; Fletcher, P.; Froum, S.; Magner, A.; Cho, S.-C.; Salama, M.; Salama, H.; Garber, D.A. Vertical Distance from the Crest of Bone to the Height of the Interproximal Papilla between Adjacent Implants. J. Periodontol. 2003, 74, 1785–1788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misch, C.E.; Strong, I.T.; Bidez, M.W. Implant Design. In Contemporary Implant Dentistry; Mosby: St. Louis, MI, USA, 2007; p. 200. [Google Scholar]
- Pan, C.-Y.; Liu, P.-H.; Tseng, Y.-C.; Chou, S.-T.; Wu, C.-Y.; Chang, H.-P. Effects of Cortical Bone Thickness and Trabecular Bone Density on Primary Stability of Orthodontic Mini-Implants. J. Dent. Sci. 2019, 14, 383–388. [Google Scholar] [CrossRef]
- Divac, M.; Stawarczyk, B.; Sahrmann, P.; Attin, T.; Schmidlin, P.R. Influence of Residual Bone Thickness on Primary Stability of Hybrid Self-Tapping and Cylindric Non-Self-Tapping Implants in Vitro. Int. J. Oral Maxillofac. Implant. 2013, 28, 84–88. [Google Scholar] [CrossRef]
- Jemat, A.; Ghazali, M.J.; Razali, M.; Otsuka, Y. Surface Modifications and Their Effects on Titanium Dental Implants. BioMed Res. Int. 2015, 2015, 791725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarano, A.; Crocetta, E.; Quaranta, A.; Lorusso, F. Influence of the Thermal Treatment to Address a Better Osseointegration of Ti6Al4V Dental Implants: Histological and Histomorphometrical Study in a Rabbit Model. BioMed Res. Int. 2018, 2018, 2349698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez y Baena, R.; Arciola, C.R.; Selan, L.; Battaglia, R.; Imbriani, M.; Rizzo, S.; Visai, L. Evaluation of Bacterial Adhesion on Machined Titanium, Osseotite® and Nanotite® Discs. Int. J. Artif. Organs 2012, 35, 754–761. [Google Scholar] [CrossRef] [PubMed]
- D’Ercole, S.; Cellini, L.; Pilato, S.; Di Lodovico, S.; Iezzi, G.; Piattelli, A.; Petrini, M. Material Characterization and Streptococcus Oralis Adhesion on Polyetheretherketone (PEEK) and Titanium Surfaces Used in Implantology. J. Mater. Science. Mater. Med. 2020, 31, 84. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Piattelli, A.; Quaranta, A.; Lorusso, F. Bone Response to Two Dental Implants with Different Sandblasted/Acid-Etched Implant Surfaces: A Histological and Histomorphometrical Study in Rabbits. BioMed Res. Int. 2017, 2017, 8724951. [Google Scholar] [CrossRef] [Green Version]
- Velasco, E.; Monsalve-Guil, L.; Jimenez, A.; Ortiz, I.; Moreno-Muñoz, J.; Nuñez-Marquez, E.; Pegueroles, M.; Pérez, R.A.; Gil, F.J. Importance of the Roughness and Residual Stresses of Dental Implants on Fatigue and Osseointegration Behavior. In Vivo Study in Rabbits. J. Oral Implantol. 2016, 42, 469–476. [Google Scholar] [CrossRef]
- Scarano, A.; Lorusso, F.; Staiti, G.; Sinjari, B.; Tampieri, A.; Mortellaro, C. Sinus Augmentation with Biomimetic Nanostructured Matrix: Tomographic, Radiological, Histological and Histomorphometrical Results after 6 Months in Humans. Front. Physiol. 2017, 8, 565. [Google Scholar] [CrossRef] [Green Version]
- Scarano, A.; Lorusso, F.; Arcangelo, M.; D’Arcangelo, C.; Celletti, R.; de Oliveira, P.S. Lateral Sinus Floor Elevation Performed with Trapezoidal and Modified Triangular Flap Designs: A Randomized Pilot Study of Post-Operative Pain Using Thermal Infrared Imaging. Int. J. Environ. Res. Public Health 2018, 15, 1277. [Google Scholar] [CrossRef] [Green Version]
- Elias, C.N.; Oshida, Y.; Lima, J.H.C.; Muller, C.A. Relationship between Surface Properties (Roughness, Wettability and Morphology) of Titanium and Dental Implant Removal Torque. J. Mech. Behav. Biomed. Mater. 2008, 1, 234–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotchkiss, K.M.; Reddy, G.B.; Hyzy, S.L.; Schwartz, Z.; Boyan, B.D.; Olivares-Navarrete, R. Titanium Surface Characteristics, Including Topography and Wettability, Alter Macrophage Activation. Acta Biomater. 2016, 31, 425–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
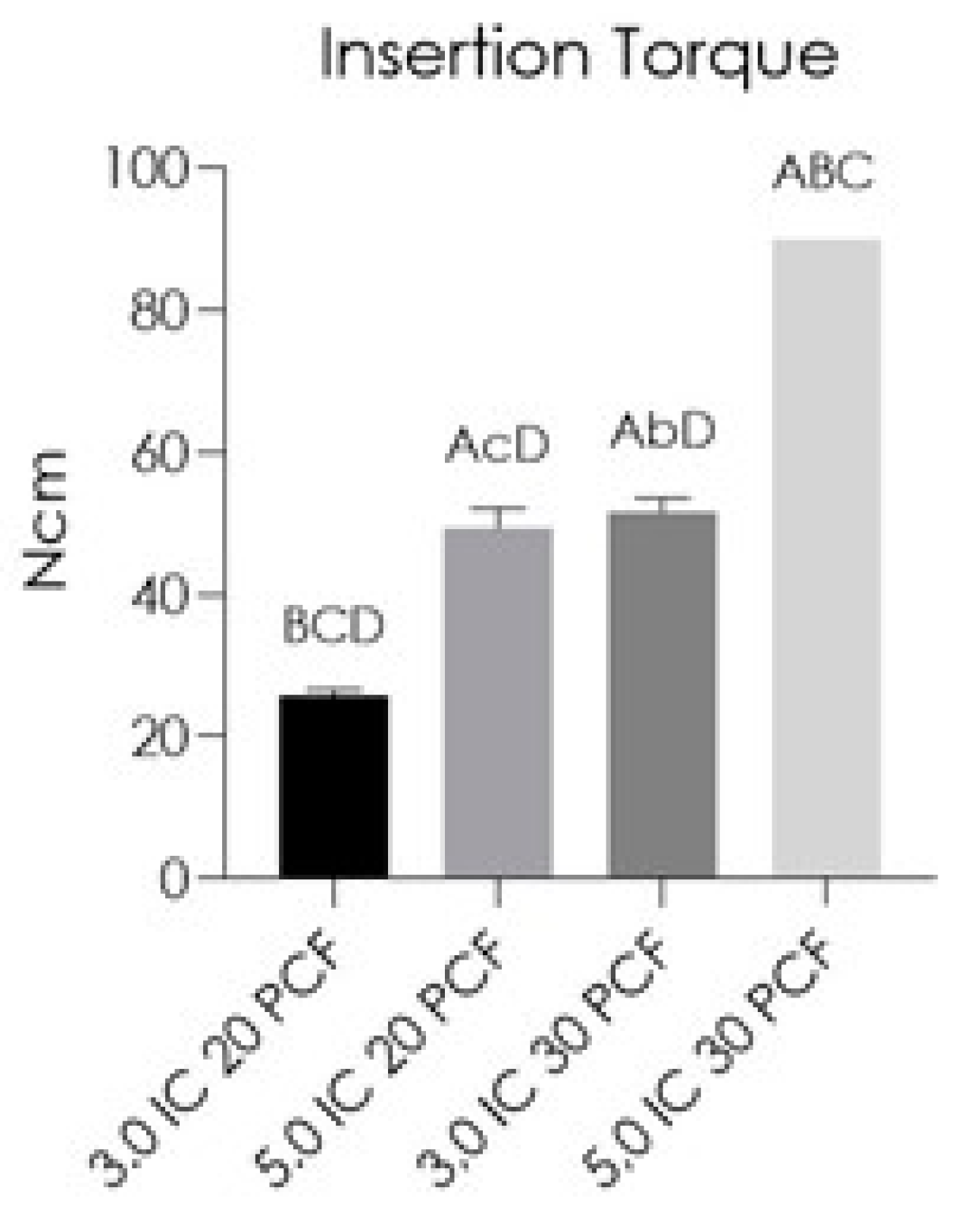
| INSERTION TORQUE | 3.0 IC 20 PCF | 5.0 IC 20 PCF | 3.0 IC 30 PCF | 5.0 IC 30 PCF |
|---|---|---|---|---|
| Minimum | 25.00 | 45.00 | 50.00 | 90.00 |
| 25% Percentile | 25.00 | 47.00 | 50.50 | 90.00 |
| Median | 26.00 | 50.00 | 51.00 | 90.00 |
| 75% Percentile | 26.50 | 51.50 | 53.00 | 90.00 |
| Maximum | 27.00 | 52.00 | 55.00 | 90.00 |
| Range | 2.000 | 7.000 | 5.000 | 0.000 |
| Mean | 25.80 | 49.40 | 51.60 | 90.00 |
| Std. Deviation | ±0.8367 | ±2.702 | ±1.949 | ±0.3012 |
| Std. Error of Mean | 0.3742 | 1.208 | 0.8718 | 0.000 |
| Lower 95% CI of mean | 24.76 | 46.05 | 49.18 | 90.00 |
| Upper 95% CI of mean | 26.84 | 52.75 | 54.02 | 90.00 |
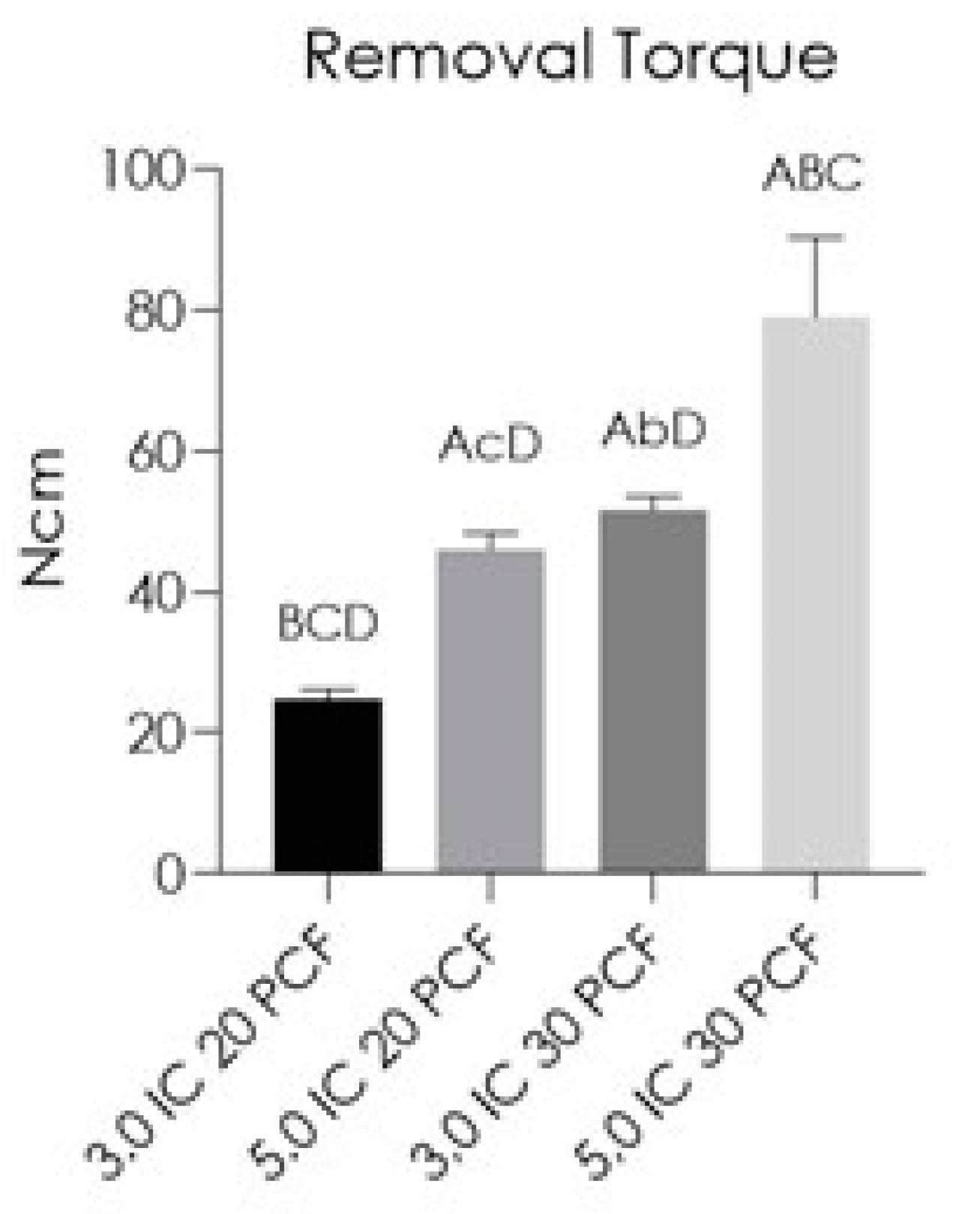
| REMOVAL TORQUE | 3.0 IC 20 PCF | 5.0 IC 20 PCF | 3.0 IC 30 PCF | 5.0 IC 30 PCF |
|---|---|---|---|---|
| Minimum | 23.00 | 43.00 | 50.00 | 60.00 |
| 25% Percentile | 23.50 | 43.50 | 50.50 | 70.00 |
| Median | 25.00 | 47.00 | 51.00 | 80.00 |
| 75% Percentile | 26.00 | 48.00 | 53.00 | 87.50 |
| Maximum | 26.00 | 48.00 | 55.00 | 90.00 |
| Range | 3.000 | 5.000 | 5.000 | 30.00 |
| Mean | 24.80 | 46.00 | 51.60 | 79.00 |
| Std. Deviation | ±1.304 | ±2.345 | ±1.949 | ±11.40 |
| Std. Error of Mean | 0.5831 | 1.049 | 0.8718 | 5.099 |
| Lower 95% CI of mean | 23.18 | 43.09 | 49.18 | 64.84 |
| Upper 95% CI of mean | 26.42 | 48.91 | 54.02 | 93.16 |
| RFA | 3.0 IC 20 PCF | 5.0 IC 20 PCF | 3.0 IC 30 PCF | 5.0 IC 30 PCF |
|---|---|---|---|---|
| Minimum | 58.00 | 61.00 | 62.50 | 68.00 |
| 25% Percentile | 58.00 | 62.25 | 63.00 | 72.25 |
| Median | 58.50 | 63.50 | 65.50 | 77.00 |
| 75% Percentile | 60.00 | 64.25 | 66.25 | 78.00 |
| Maximum | 60.50 | 64.50 | 67.00 | 78.50 |
| Range | 2.500 | 3.500 | 4.500 | 10.50 |
| Mean | 58.90 | 63.30 | 64.80 | 75.50 |
| Std. Deviation | ±1.084 | ±1.351 | ±1.789 | ±4.257 |
| Std. Error of Mean | 0.4848 | 0.6042 | 0.8000 | 1.904 |
| Lower 95% CI of mean | 57.55 | 61.62 | 62.58 | 70.21 |
| Upper 95% CI of mean | 60.25 | 64.98 | 67.02 | 80.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tumedei, M.; Petrini, M.; Cipollina, A.; Di Carmine, M.; Piattelli, A.; Cucurullo, A.; Iezzi, G. Comparative Evaluation of Primary Stability between Different Diameters Multi-Scale Roughness Dental Implant by Solid Rigid Polyurethane Simulation. Osteology 2021, 1, 62-72. https://doi.org/10.3390/osteology1010006
Tumedei M, Petrini M, Cipollina A, Di Carmine M, Piattelli A, Cucurullo A, Iezzi G. Comparative Evaluation of Primary Stability between Different Diameters Multi-Scale Roughness Dental Implant by Solid Rigid Polyurethane Simulation. Osteology. 2021; 1(1):62-72. https://doi.org/10.3390/osteology1010006
Chicago/Turabian StyleTumedei, Margherita, Morena Petrini, Alessandro Cipollina, Mariastella Di Carmine, Adriano Piattelli, Antonio Cucurullo, and Giovanna Iezzi. 2021. "Comparative Evaluation of Primary Stability between Different Diameters Multi-Scale Roughness Dental Implant by Solid Rigid Polyurethane Simulation" Osteology 1, no. 1: 62-72. https://doi.org/10.3390/osteology1010006