
Predictive Strategies to Reduce the Risk of Rehospitalization with a Focus on Frail Older Adults: A Narrative Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Reasons for Rehospitalization in Frail Older Adults
3. The Epidemiological Importance of Frailty for Hospitalization and Rehospitalization in Older Adults
4. Instruments Used to Identify Frailty
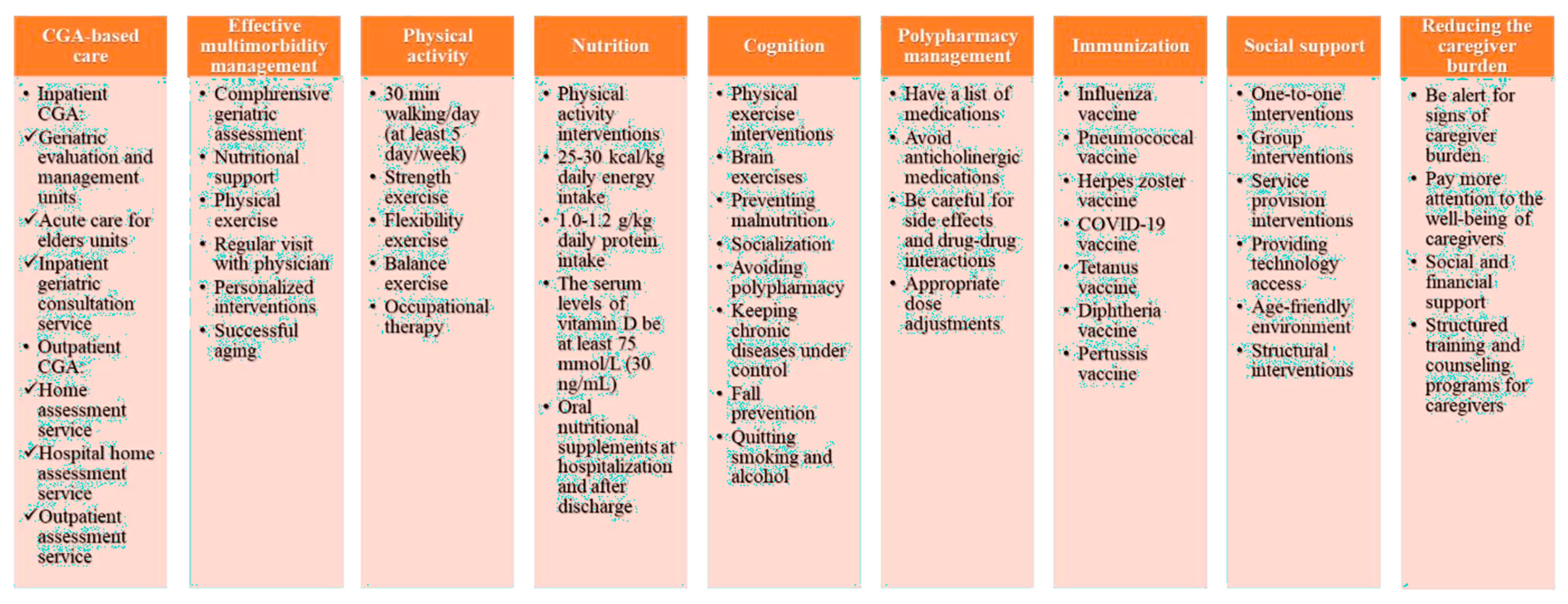
5. Predictive and Preventive Strategies
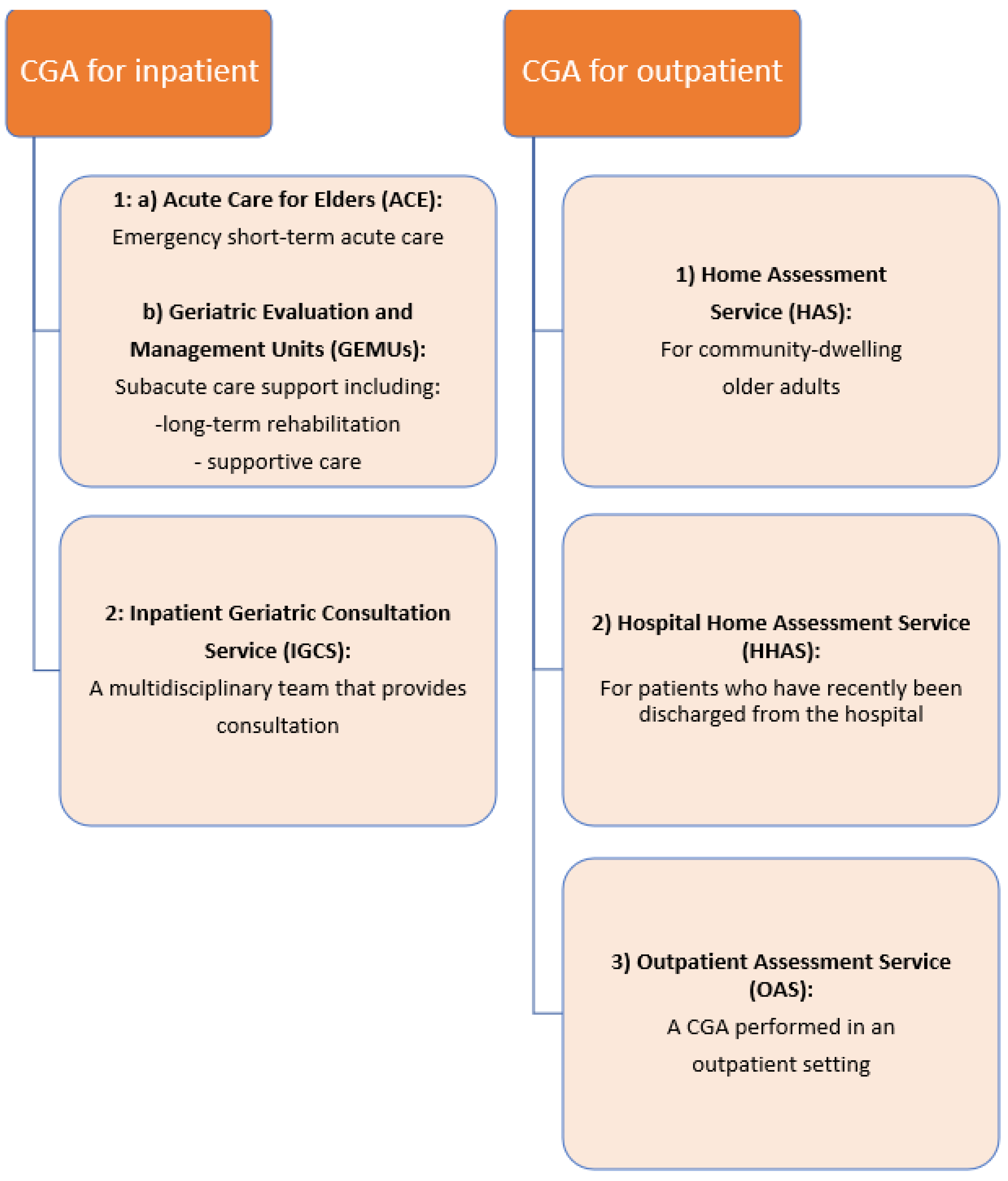
5.1. CGA-Based Care
5.2. Effective Multimorbidity Management
5.2.1. Heart Failure
5.2.2. Diabetes Mellitus
5.2.3. Chronic Obstructive Pulmonary Disease (COPD)
5.2.4. Dementia
5.2.5. Other Chronic Conditions
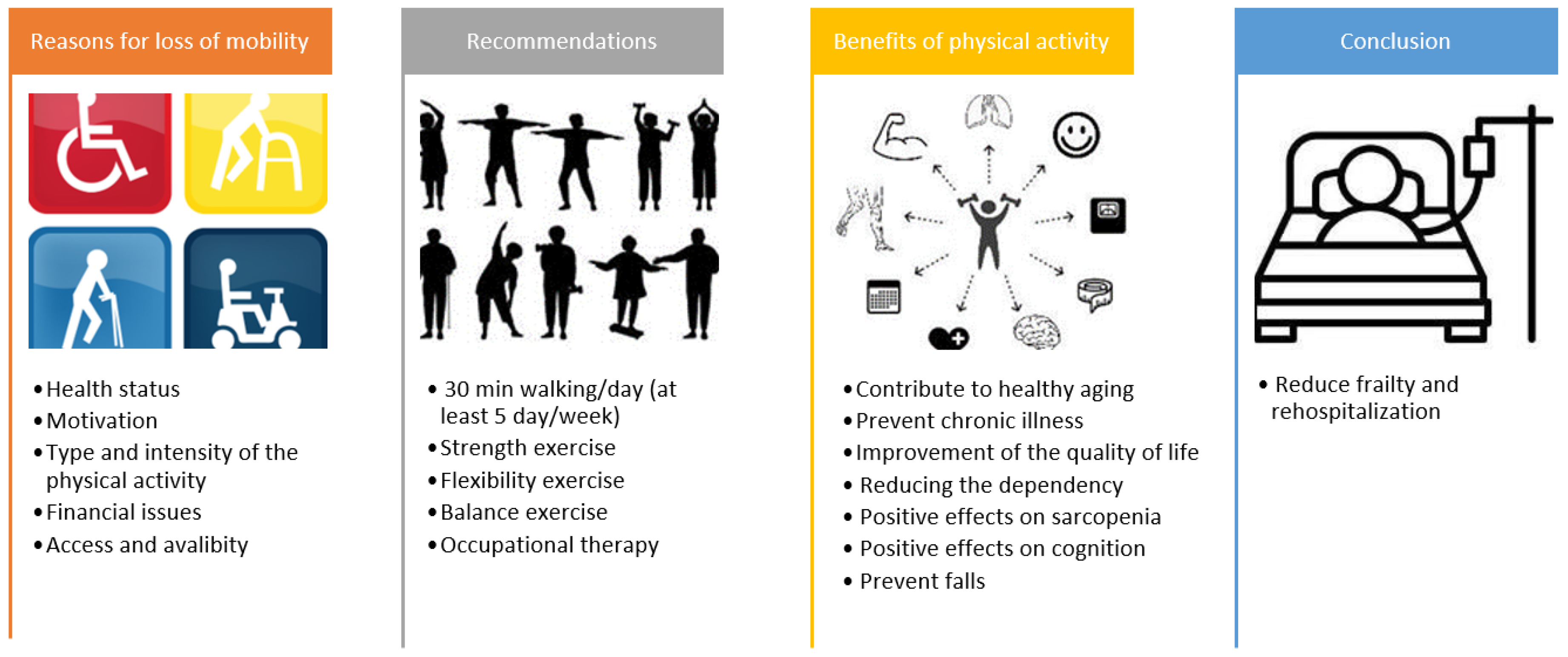
5.3. Physical Activity
5.4. Malnutrition and Sarcopenia
5.5. Cognition
5.6. Polypharmacy Management
5.7. Immunization
5.8. Social Isolation–Social Support
5.9. Reducing the Caregiver Burden
5.10. Palliative Care
6. Barriers for Strategies to Reduce Frailty Syndrome and Rehospitalization in Frail Older Adults
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Woodhouse, L.; Rodríguez-Mañas, L.; Fried, L.P.; Woo, J.; Aprahamian, I.; Sanford, A.; Lundy, J.; et al. Physical Frailty: ICFSR International Clinical Practice Guidelines for Identification and Management. J. Nutr. Health Aging 2019, 23, 771–787. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Theou, O.; Squires, E.; Mallery, K.; Lee, J.S.; Fay, S.; Goldstein, J.; Armstrong, J.J.; Rockwood, K. What do we know about frailty in the acute care setting? A scoping review. BMC Geriatr. 2018, 18, 139. [Google Scholar] [CrossRef]
- Fhon, J.R.S.; Rodrigues, R.A.P.; Santos, J.L.F.; Diniz, M.A.; Santos, E.B.D.; Almeida, V.C.; Giacomini, S.B.L. Factors associated with frailty in older adults: A longitudinal study. Rev. Saude Publica 2018, 52, 74. [Google Scholar] [CrossRef]
- Soysal, P.; Stubbs, B.; Lucato, P.; Luchini, C.; Solmi, M.; Peluso, R.; Sergi, G.; Isik, A.T.; Manzato, E.; Maggi, S.; et al. Inflammation and frailty in the elderly: A systematic review and meta-analysis. Ageing Res. Rev. 2016, 31, 1–8, Erratum in Ageing Res. Rev. 2017, 35, 364–365. [Google Scholar] [CrossRef]
- Soysal, P.; Isik, A.T.; Carvalho, A.F.; Fernandes, B.S.; Solmi, M.; Schofield, P.; Veronese, N.; Stubbs, B. Oxidative stress and frailty: A systematic review and synthesis of the best evidence. Maturitas 2017, 99, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Veronese, N.; Thompson, T.; Kahl, K.G.; Fernandes, B.S.; Prina, A.M.; Solmi, M.; Schofield, P.; Koyanagi, A.; Tseng, P.T.; et al. Relationship between depression and frailty in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2017, 36, 78–87. [Google Scholar] [CrossRef]
- Chen, X.; Mao, G.; Leng, S.X. Frailty syndrome: An overview. Clin. Interv. Aging 2014, 9, 433–441. [Google Scholar] [CrossRef]
- Carneiro, J.A.; Cardoso, R.R.; Durães, M.S.; Guedes, M.C.A.; Santos, F.L.; Costa, F.M.D.; Caldeira, A.P. Frailty in the elderly: Prevalence and associated factors. Rev. Bras. Enferm. 2017, 70, 747–752. [Google Scholar] [CrossRef]
- Handforth, C.; Clegg, A.; Young, C.; Simpkins, S.; Seymour, M.T.; Selby, P.J.; Young, J. The prevalence and outcomes of frailty in older cancer patients: A systematic review. Ann. Oncol. 2015, 26, 1091–1101. [Google Scholar] [CrossRef]
- Gale, C.R.; Cooper, C.; Aihie Sayer, A. Prevalence of frailty and disability: Findings from the English Longitudinal Study of Ageing. Age Ageing 2014, 44, 162–165. [Google Scholar] [CrossRef]
- Ates Bulut, E.; Soysal, P.; Isik, A.T. Frequency and coincidence of geriatric syndromes according to age groups: Single-center experience in Turkey between 2013 and 2017. Clin. Interv. Aging 2018, 13, 1899–1905. [Google Scholar] [CrossRef]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Joosten, E.; Demuynck, M.; Detroyer, E.; Milisen, K. Prevalence of frailty and its ability to predict in hospital delirium, falls, and 6-month mortality in hospitalized older patients. BMC Geriatr. 2014, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: A prospective analysis of 493 737 UK Biobank participants. Lancet Public Health 2018, 3, e323–e332. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Sermeus, W.; Van den Heede, K.; Sloane, D.M.; Busse, R.; McKee, M.; Bruyneel, L.; Rafferty, A.M.; Griffiths, P.; Moreno-Casbas, M.T.; et al. Patient safety, satisfaction, and quality of hospital care: Cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ 2012, 344, e1717. [Google Scholar] [CrossRef]
- Halfon, P.; Eggli, Y.; Prêtre-Rohrbach, I.; Meylan, D.; Marazzi, A.; Burnand, B. Validation of the potentially avoidable hospital readmission rate as a routine indicator of the quality of hospital care. Med. Care 2006, 44, 972–981. [Google Scholar] [CrossRef]
- Feigenbaum, P.; Neuwirth, E.; Trowbridge, L.; Teplitsky, S.; Barnes, C.A.; Fireman, E.; Dorman, J.; Bellows, J. Factors contributing to all-cause 30-day readmissions: A structured case series across 18 hospitals. Med. Care 2012, 50, 599–605. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, K.J.; Choi, J.W.; Kim, T.H.; Kim, C.O. Factors Related to Hospital Readmission of Frail Older Adults in Korea. Yonsei Med. J. 2022, 63, 984–990. [Google Scholar] [CrossRef]
- Willers, C.; Boström, A.M.; Carlsson, L.; Lager, A.; Lindqvist, R.; Rydwik, E. Readmission within three months after inpatient geriatric care-Incidence, diagnosis and associated factors in a Swedish cohort. PLoS ONE 2021, 16, e0248972. [Google Scholar] [CrossRef]
- Bahrmann, A.; Benner, L.; Christ, M.; Bertsch, T.; Sieber, C.C.; Katus, H.; Bahrmann, P. The Charlson Comorbidity and Barthel Index predict length of hospital stay, mortality, cardiovascular mortality and rehospitalization in unselected older patients admitted to the emergency department. Aging Clin. Exp. Res. 2019, 31, 1233–1242. [Google Scholar] [CrossRef]
- Lai, H.Y.; Huang, S.T.; Chen, L.K.; Hsiao, F.Y. Development of frailty index using ICD-10 codes to predict mortality and rehospitalization of older adults: An update of the multimorbidity frailty index. Arch. Gerontol. Geriatr. 2022, 100, 104646. [Google Scholar] [CrossRef]
- Cheng, R.K.; Cox, M.; Neely, M.L.; Heidenreich, P.A.; Bhatt, D.L.; Eapen, Z.J.; Hernandez, A.F.; Butler, J.; Yancy, C.W.; Fonarow, G.C. Outcomes in patients with heart failure with preserved, borderline, and reduced ejection fraction in the Medicare population. Am. Heart J. 2014, 168, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Dharmarajan, K.; Hsieh, A.F.; Lin, Z.; Bueno, H.; Ross, J.S.; Horwitz, L.I.; Barreto-Filho, J.A.; Kim, N.; Bernheim, S.M.; Suter, L.G.; et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA 2013, 309, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Golden, A.G.; Tewary, S.; Dang, S.; Roos, B.A. Care management’s challenges and opportunities to reduce the rapid rehospitalization of frail community-dwelling older adults. Gerontologist 2010, 50, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Sganga, F.; Landi, F.; Volpato, S.; Cherubini, A.; Ruggiero, C.; Corsonello, A.; Fabbietti, P.; Lattanzio, F.; Gravina, E.M.; Bernabei, R.; et al. Predictors of rehospitalization among older adults: Results of the CRIME Study. Geriatr. Gerontol. Int. 2017, 17, 1588–1592. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, M.K.; Meyer, G.; Uhrenfeldt, L. Risk factors for acute care hospital readmission in older persons in Western countries: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 454–485. [Google Scholar] [CrossRef]
- Gregersen, M.; Hansen, T.K.; Jørgensen, B.B.; Damsgaard, E.M. Frailty is associated with hospital readmission in geriatric patients: A prognostic study. Eur. Geriatr. Med. 2020, 11, 783–792. [Google Scholar] [CrossRef]
- Muscedere, J.; Waters, B.; Varambally, A.; Bagshaw, S.M.; Boyd, J.G.; Maslove, D.; Sibley, S.; Rockwood, K. The impact of frailty on intensive care unit outcomes: A systematic review and meta-analysis. Intensive Care Med. 2017, 43, 1105–1122. [Google Scholar] [CrossRef]
- Cunha, A.I.L.; Veronese, N.; de Melo Borges, S.; Ricci, N.A. Frailty as a predictor of adverse outcomes in hospitalized older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2019, 56, 100960. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.; Larbi, A.; Yap, K.B. Frailty in older persons: Multisystem risk factors and the Frailty Risk Index (FRI). J. Am. Med. Dir. Assoc. 2014, 15, 635–642. [Google Scholar] [CrossRef]
- Chong, E.; Ho, E.; Baldevarona-Llego, J.; Chan, M.; Wu, L.; Tay, L. Frailty and Risk of Adverse Outcomes in Hospitalized Older Adults: A Comparison of Different Frailty Measures. J. Am. Med. Dir. Assoc. 2017, 18, 638.e7–638.e11. [Google Scholar] [CrossRef] [PubMed]
- Covinsky, K.E.; Pierluissi, E.; Johnston, C.B. Hospitalization-associated disability: “She was probably able to ambulate, but I’m not sure”. JAMA 2011, 306, 1782–1793. [Google Scholar] [CrossRef]
- Stillman, G.R.; Stillman, A.N.; Beecher, M.S. Frailty Is Associated with Early Hospital Readmission in Older Medical Patients. J. Appl. Gerontol. 2021, 40, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman, R.B.; Sheingold, S.H.; Orav, E.J.; Ruhter, J.; Epstein, A.M. Readmissions, Observation, and the Hospital Readmissions Reduction Program. N. Engl. J. Med. 2016, 374, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Voora, R.S.; Qian, A.S.; Kotha, N.V.; Qiao, E.M.; Meineke, M.; Murphy, J.D.; Orosco, R.K. Frailty Index as a Predictor of Readmission in Patients with Head and Neck Cancer. Otolaryngol. Head Neck Surg. 2022, 167, 89–96. [Google Scholar] [CrossRef]
- Kundi, H.; Wadhera, R.K.; Strom, J.B.; Valsdottir, L.R.; Shen, C.; Kazi, D.S.; Yeh, R.W. Association of Frailty with 30-Day Outcomes for Acute Myocardial Infarction, Heart Failure, and Pneumonia Among Elderly Adults. JAMA Cardiol. 2019, 4, 1084–1091. [Google Scholar] [CrossRef]
- Upadhyay, S.; Stephenson, A.L.; Smith, D.G. Readmission Rates and Their Impact on Hospital Financial Performance: A Study of Washington Hospitals. Inquiry 2019, 56, 46958019860386. [Google Scholar] [CrossRef]
- Pilotto, A.; Cella, A.; Pilotto, A.; Daragjati, J.; Veronese, N.; Musacchio, C.; Mello, A.M.; Logroscino, G.; Padovani, A.; Prete, C.; et al. Three Decades of Comprehensive Geriatric Assessment: Evidence Coming from Different Healthcare Settings and Specific Clinical Conditions. J. Am. Med. Dir. Assoc. 2017, 18, 192.e1–192.e11. [Google Scholar] [CrossRef]
- Soysal, P.; Isik, A.T.; Buyukaydin, B.; Kazancioglu, R. A comparison of end-stage renal disease and Alzheimer’s disease in the elderly through a comprehensive geriatric assessment. Int. Urol. Nephrol. 2014, 46, 1627–1632. [Google Scholar] [CrossRef]
- Rockwood, K.; Mitnitski, A. Frailty in relation to the accumulation of deficits. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Isik, A.T.; Arik, F.; Kalan, U.; Eyvaz, A.; Veronese, N. Validity of the Mini-Nutritional Assessment Scale for Evaluating Frailty Status in Older Adults. J. Am. Med. Dir. Assoc. 2019, 20, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Veronese, N.; Arik, F.; Kalan, U.; Smith, L.; Isik, A.T. Mini Nutritional Assessment Scale-Short form can be useful for frailty screening in older adults. Clin. Interv. Aging 2019, 14, 693–699. [Google Scholar] [CrossRef]
- Clegg, A.; Bates, C.; Young, J.; Ryan, R.; Nichols, L.; Ann Teale, E.; Mohammed, M.A.; Parry, J.; Marshall, T. Development and validation of an electronic frailty index using routine primary care electronic health record data. Age Ageing 2016, 45, 353–360. [Google Scholar] [CrossRef]
- Morley, J.E.; Vellas, B.; van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Rolfson, D.B.; Majumdar, S.R.; Tsuyuki, R.T.; Tahir, A.; Rockwood, K. Validity and reliability of the Edmonton Frail Scale. Age Ageing 2006, 35, 526–529. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Ewing, S.K.; Taylor, B.C.; Fink, H.A.; Stone, K.L.; Cauley, J.A.; Tracy, J.K.; Hochberg, M.C.; Rodondi, N.; Cawthon, P.M.; et al. Frailty and risk of falls, fracture, and mortality in older women: The study of osteoporotic fractures. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 744–751. [Google Scholar] [CrossRef]
- Baitar, A.; Van Fraeyenhove, F.; Vandebroek, A.; De Droogh, E.; Galdermans, D.; Mebis, J.; Schrijvers, D. Evaluation of the Groningen Frailty Indicator and the G8 questionnaire as screening tools for frailty in older patients with cancer. J. Geriatr. Oncol. 2013, 4, 32–38. [Google Scholar] [CrossRef]
- Saliba, D.; Elliott, M.; Rubenstein, L.Z.; Solomon, D.H.; Young, R.T.; Kamberg, C.J.; Roth, C.; MacLean, C.H.; Shekelle, P.G.; Sloss, E.M.; et al. The Vulnerable Elders Survey: A tool for identifying vulnerable older people in the community. J. Am. Geriatr. Soc. 2001, 49, 1691–1699. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Pilotto, A.; Ferrucci, L.; Franceschi, M.; D’Ambrosio, L.P.; Scarcelli, C.; Cascavilla, L.; Paris, F.; Placentino, G.; Seripa, D.; Dallapiccola, B. Development and validation of a multidimensional prognostic index for one-year mortality from comprehensive geriatric assessment in hospitalized older patients. Rejuvenation Res. 2008, 11, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Pijpers, E.; Ferreira, I.; van de Laar, R.J.; Stehouwer, C.D.; Nieuwenhuijzen Kruseman, A.C. Predicting mortality of psychogeriatric patients: A simple prognostic frailty risk score. Postgrad. Med. J. 2009, 85, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, T.; Neuburger, J.; Kraindler, J.; Keeble, E.; Smith, P.; Ariti, C.; Arora, S.; Street, A.; Parker, S.; Roberts, H.C.; et al. Development and validation of a Hospital Frailty Risk Score focusing on older people in acute care settings using electronic hospital records: An observational study. Lancet 2018, 391, 1775–1782. [Google Scholar] [CrossRef] [PubMed]
- King, K.E.; Fillenbaum, G.G.; Cohen, H.J. A Cumulative Deficit Laboratory Test-based Frailty Index: Personal and Neighborhood Associations. J. Am. Geriatr. Soc. 2017, 65, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Picca, A.; Coelho-Junior, H.J.; Calvani, R.; Marzetti, E.; Vetrano, D.L. Biomarkers shared by frailty and sarcopenia in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2022, 73, 101530. [Google Scholar] [CrossRef]
- Okoye, C.; Arosio, B.; Carino, S.; Putrino, L.; Franchi, R.; Rogani, S.; Cesari, M.; Mari, D.; Vitale, G.; Malara, A.; et al. The Free Triiodothyronine/Free Thyroxine Ratio Is Associated with Frailty in Older Adults: A Longitudinal Multisetting Study. Thyroid 2023, 33, 169–176. [Google Scholar] [CrossRef]
- Marzetti, E.; Picca, A.; Marini, F.; Biancolillo, A.; Coelho-Junior, H.J.; Gervasoni, J.; Bossola, M.; Cesari, M.; Onder, G.; Landi, F.; et al. Inflammatory signatures in older persons with physical frailty and sarcopenia: The frailty “cytokinome” at its core. Exp. Gerontol. 2019, 122, 129–138. [Google Scholar] [CrossRef]
- Rodríguez-Mañas, L.; Féart, C.; Mann, G.; Viña, J.; Chatterji, S.; Chodzko-Zajko, W.; Gonzalez-Colaço, H.M.; Bergman, H.; Carcaillon, L.; Nicholson, C.; et al. Searching for an operational definition of frailty: A Delphi method based consensus statement: The frailty operative definition-consensus conference project. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 62–67. [Google Scholar] [CrossRef]
- Solomon, D.H. Geriatric assessment: Methods for clinical decision making. JAMA 1988, 259, 2450–2452. [Google Scholar] [CrossRef]
- Stuck, A.E.; Siu, A.L.; Wieland, G.D.; Adams, J.; Rubenstein, L.Z. Comprehensive geriatric assessment: A meta-analysis of controlled trials. Lancet 1993, 342, 1032–1036. [Google Scholar] [CrossRef] [PubMed]
- Ekdahl, A.W.; Wirehn, A.B.; Alwin, J.; Jaarsma, T.; Unosson, M.; Husberg, M.; Eckerblad, J.; Milberg, A.; Krevers, B.; Carlsson, P. Costs and Effects of an Ambulatory Geriatric Unit (the AGe-FIT Study): A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2015, 16, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Morin, T.; Lanièce, I.; Desbois, A.; Amiard, S.; Gavazzi, G.; Couturier, P. Évaluation du suivi des recommandations à 3 mois après prise en charge par une équipe mobile gériatrique hospitalière [Evaluation of adherence to recommendations within 3 months after comprehensive geriatric assessment by an inpatient geriatric consultation team]. Geriatr. Psychol. Neuropsychiatr. Vieil. 2012, 10, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Flood, K.L.; Maclennan, P.A.; McGrew, D.; Green, D.; Dodd, C.; Brown, C.J. Effects of an acute care for elders unit on costs and 30-day readmissions. JAMA Intern. Med. 2013, 173, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Ekerstad, N.; Karlson, B.W.; Dahlin Ivanoff, S.; Landahl, S.; Andersson, D.; Heintz, E.; Husberg, M.; Alwin, J. Is the acute care of frail elderly patients in a comprehensive geriatric assessment unit superior to conventional acute medical care? Clin. Interv. Aging 2016, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rezaei-Shahsavarloo, Z.; Atashzadeh-Shoorideh, F.; Gobbens, R.J.J.; Ebadi, A.; Ghaedamini Harouni, G. The impact of interventions on the management of frailty in hospitalized frail older adults: A systematic review and meta-analysis. BMC Geriatr. 2020, 20, 526. [Google Scholar] [CrossRef]
- Veronese, N.; Custodero, C.; Demurtas, J.; Smith, L.; Barbagallo, M.; Maggi, S.; Cella, A.; Vanacore, N.; Aprile, P.L.; Ferrucci, L.; et al. Special Interest Group in Systematic Reviews of the European Geriatric Medicine Society (EuGMS); Special Interest Group in Meta-analyses and Comprehensive Geriatric Assessment of the European Geriatric Medicine Society (EuGMS). Age Ageing 2022, 51, afac104. [Google Scholar] [CrossRef]
- Calsolaro, V.; Antognoli, R.; Pasqualetti, G.; Okoye, C.; Aquilini, F.; Cristofano, M.; Briani, S.; Monzani, F. 30-Day Potentially Preventable Hospital Readmissions in Older Patients: Clinical Phenotype and Health Care Related Risk Factors. Clin. Interv. Aging 2019, 14, 1851–1858. [Google Scholar] [CrossRef]
- Theou, O.; Rockwood, M.R.; Mitnitski, A.; Rockwood, K. Disability and co-morbidity in relation to frailty: How much do they overlap? Arch. Gerontol. Geriatr. 2012, 55, e1–e8. [Google Scholar] [CrossRef]
- Pefoyo, A.J.; Bronskill, S.E.; Gruneir, A.; Calzavara, A.; Thavorn, K.; Petrosyan, Y.; Maxwell, C.J.; Bai, Y.; Wodchis, W.P. The increasing burden and complexity of multimorbidity. BMC Public Health 2015, 15, 415. [Google Scholar] [CrossRef]
- Williams, J.S.; Egede, L.E. The Association Between Multimorbidity and Quality of Life, Health Status and Functional Disability. Am. J. Med. Sci. 2016, 352, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Nunes, B.P.; Flores, T.R.; Mielke, G.I.; Thumé, E.; Facchini, L.A. Multimorbidity and mortality in older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2016, 67, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Bähler, C.; Huber, C.A.; Brüngger, B.; Reich, O. Multimorbidity, health care utilization and costs in an elderly community-dwelling population: A claims data based observational study. BMC Health Serv. Res. 2015, 15, 23. [Google Scholar] [CrossRef] [PubMed]
- Aubert, C.E.; Schnipper, J.L.; Fankhauser, N.; Marques-Vidal, P.; Stirnemann, J.; Auerbach, A.D.; Zimlichman, E.; Kripalani, S.; Vasilevskis, E.E.; Robinson, E.; et al. Patterns of multimorbidity associated with 30-day readmission: A multinational study. BMC Public Health 2019, 19, 738. [Google Scholar] [CrossRef]
- Rodrigues, L.P.; de Oliveira Rezende, A.T.; Delpino, F.M.; Mendonça, C.R.; Noll, M.; Nunes, B.P.; de Oliviera, C.; Silveira, E.A. Association between multimorbidity and hospitalization in older adults: Systematic review and meta-analysis. Age Ageing 2022, 51, afac155. [Google Scholar] [CrossRef]
- Vitale, C.; Jankowska, E.; Hill, L.; Piepoli, M.; Doehner, W.; Anker, S.D.; Lainscak, M.; Jaarsma, T.; Ponikowski, P.; Rosano, G.M.C.; et al. Heart Failure Association/European Society of Cardiology position paper on frailty in patients with heart failure. Eur. J. Heart Fail. 2019, 21, 1299–1305. [Google Scholar] [CrossRef]
- Díaz-Toro, F.; Nazzal Nazal, C.; Verdejo, H.; Rossel, V.; Castro, P.; Larrea, R.; Concepción, R.; Sepúlveda, L. Factores asociados a fragilidad en pacientes hospitalizados con insuficiencia cardiaca descompensada [Frailty in patients admitted to hospital with acute decompensated heart failure]. Rev. Med. Chil. 2017, 145, 164–171. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Testa, G.; Curcio, F.; Liguori, I.; Basile, C.; Papillo, M.; Tocchetti, C.G.; Galizia, G.; Della-Morte, D.; Gargiulo, G.; Cacciatore, F.; et al. Physical vs. multidimensional frailty in older adults with and without heart failure. ESC Heart Fail. 2020, 7, 1371–1380. [Google Scholar] [CrossRef]
- Studzińska, K.; Wąż, P.; Frankiewicz, A.; Stopczyńska, I.; Studnicki, R.; Hansdorfer-Korzon, R. Employing the Multivariate Edmonton Scale in the Assessment of Frailty Syndrome in Heart Failure. J. Clin. Med. 2022, 11, 4022. [Google Scholar] [CrossRef]
- Al-Jarallah, M.; Rajan, R.; Al-Zakwani, I.; Dashti, R.; Bulbanat, B.; Ridha, M.; Sulaiman, K.; Alsheikh-Ali, A.A.; Panduranga, P.; AlHabib, K.F.; et al. Impact of diabetes on mortality and rehospitalization in acute heart failure patients stratified by ejection fraction. ESC Heart Fail. 2020, 7, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Hiriscau, E.I.; Bodolea, C. The Role of Depression and Anxiety in Frail Patients with Heart Failure. Diseases 2019, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Richter, D.; Guasti, L.; Walker, D.; Lambrinou, E.; Lionis, C.; Abreu, A.; Savelieva, I.; Fumagalli, S.; Bo, M.; Rocca, B.; et al. Frailty in cardiology: Definition, assessment and clinical implications for general cardiology. A consensus document of the Council for Cardiology Practice (CCP), Association for Acute Cardio Vascular Care (ACVC), Association of Cardiovascular Nursing and Allied Professions (ACNAP), European Association of Preventive Cardiology (EAPC), European Heart Rhythm Association (EHRA), Council on Valvular Heart Diseases (VHD), Council on Hypertension (CHT), Council of Cardio-Oncology (CCO), Working Group (WG) Aorta and Peripheral Vascular Diseases, WG e-Cardiology, WG Thrombosis, of the European Society of Cardiology, European Primary Care Cardiology Society (EPCCS). Eur. J. Prev. Cardiol. 2022, 29, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Reeves, G.R.; Whellan, D.J.; O’Connor, C.M.; Duncan, P.; Eggebeen, J.D.; Morgan, T.M.; Hewston, L.A.; Pastva, A.; Patel, M.J.; Kitzman, D.W. A Novel Rehabilitation Intervention for Older Patients with Acute Decompensated Heart Failure: The REHAB-HF Pilot Study. JACC Heart Fail. 2017, 5, 359–366. [Google Scholar] [CrossRef]
- Kalyani, R.R.; Tian, J.; Xue, Q.L.; Walston, J.; Cappola, A.R.; Fried, L.P.; Brancati, F.L.; Blaum, C.S. Hyperglycemia and incidence of frailty and lower extremity mobility limitations in older women. J. Am. Geriatr. Soc. 2012, 60, 1701–1707. [Google Scholar] [CrossRef]
- De Rekeneire, N.; Resnick, H.E.; Schwartz, A.V.; Shorr, R.I.; Kuller, L.H.; Simonsick, E.M.; Vellas, B.; Harris, T.B.; Health, Aging, and Body Composition study. Diabetes is associated with subclinical functional limitation in nondisabled older individuals: The Health, Aging, and Body Composition study. Diabetes Care 2003, 26, 3257–3263. [Google Scholar] [CrossRef]
- Chao, C.T.; Wang, J.; Chien, K.L.; COhort of GEriatric Nephrology in NTUH (COGENT) study group. Both pre-frailty and frailty increase healthcare utilization and adverse health outcomes in patients with type 2 diabetes mellitus. Cardiovasc. Diabetol. 2018, 17, 130. [Google Scholar] [CrossRef]
- Frankel, J.E.; Bean, J.F.; Frontera, W.R. Exercise in the elderly: Research and clinical practice. Clin. Geriatr. Med. 2006, 22, 239-vii. [Google Scholar] [CrossRef]
- Maltese, G.; Basile, G.; Meehan, H.; Fuller, M.; Cesari, M.; Fountoulakis, N.; Karalliedde, J. Frailty Is Associated with Impaired Diabetic Foot Ulcer Healing and All-Cause Re-Hospitalization. J. Nutr. Health Aging 2022, 26, 169–173. [Google Scholar] [CrossRef]
- Alqahtani, J.S.; Njoku, C.M.; Bereznicki, B.; Wimmer, B.C.; Peterson, G.M.; Kinsman, L.; Aldabayan, Y.S.; Alrajeh, A.M.; Aldhahir, A.M.; Mandal, S.; et al. Risk factors for all-cause hospital readmission following exacerbation of COPD: A systematic review and meta-analysis. Eur. Respir. Rev. 2020, 29, 190166. [Google Scholar] [CrossRef]
- Osadnik, C.; Kavanagh, A.; Macdonald, M.; Tran, A.; Haines, T.; Bardin, P. Characteristics of frail patients with acute exacerbations of COPD who experience readmissions. Eur. Respir. J. 2019, 54 (Suppl. S63), OA3813. [Google Scholar] [CrossRef]
- Hartl, S.; Lopez-Campos, J.L.; Pozo-Rodriguez, F.; Castro-Acosta, A.; Studnicka, M.; Kaiser, B.; Roberts, C.M. Risk of death and readmission of hospital-admitted COPD exacerbations: European COPD audit. Eur. Respir. J. 2016, 47, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Bernabeu-Mora, R.; García-Guillamón, G.; Valera-Novella, E.; Giménez-Giménez, L.M.; Escolar-Reina, P.; Medina-Mirapeix, F. Frailty is a predictive factor of readmission within 90 days of hospitalization for acute exacerbations of chronic obstructive pulmonary disease: A longitudinal study. Ther. Adv. Respir. Dis. 2017, 11, 383–392. [Google Scholar] [CrossRef]
- Alqahtani, J.S.; Aldabayan, Y.S.; Aldhahir, A.M.; Al Rajeh, A.M.; Mandal, S.; Hurst, J.R. Predictors of 30- and 90-Day COPD Exacerbation Readmission: A Prospective Cohort Study. Int. J. Chron. Obs. Pulmon Dis. 2021, 16, 2769–2781. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Bao, S.; Dull, P.; Wu, B.; Yu, F. Hospital readmission in persons with dementia: A systematic review. Int. J. Geriatr. Psychiatry 2019, 34, 1170–1184. [Google Scholar] [CrossRef]
- Kedia, S.K.; Chavan, P.P.; Boop, S.E.; Yu, X. Health care utilization among elderly medicare beneficiaries with coexisting dementia and cancer. Gerontol. Geriatr. Med. 2017, 3, 233372141668904. [Google Scholar] [CrossRef]
- Briggs, R.; Dyer, A.; Nabeel, S.; Collins, R.; Doherty, J.; Coughlan, T.; O’Neill, D.; Kennelly, S.P. Dementia in the acute hospital: The prevalence and clinical outcomes of acutely unwell patients with dementia. Qjm 2017, 110, 33–37. [Google Scholar] [CrossRef]
- Ma, C.; Shang, J.; Miner, S.; Lennox, L.; Squires, A. The prevalence, reasons, and risk factors for hospital readmissions among home health care patients: A systematic review. Home Health Care Manag. Pr. 2018, 30, 83–92. [Google Scholar] [CrossRef]
- Villars, H.; Dupuy, C.; Soler, P.; Gardette, V.; Soto, M.E.; Gillette, S.; Nourhashemi, F.; Vellas, B. A follow-up intervention in severely demented patients after discharge from a special Alzheimer acute care unit: Impact on early emergency room re-hospitalization rate. Int. J. Geriatr. Psychiatry 2013, 28, 1131–1140. [Google Scholar] [CrossRef]
- Chang, C.C.; Lin, P.H.; Chang, Y.T.; Chen, N.C.; Huang, C.W.; Lui, C.C.; Huang, S.H.; Chang, Y.H.; Lee, C.C.; Lai, W.A. The impact of admission diagnosis on recurrent or frequent hospitalizations in 3 dementia subtypes: A hospital-based cohort in Taiwan with 4 years longitudinal follow-ups. Medicine 2015, 94, e2091. [Google Scholar] [CrossRef]
- Boltz, M.; Chippendale, T.; Resnick, B.; Galvin, J.E. Testing family-centered, function-focused care in hospitalized persons with dementia. Neurodegener. Dis. Manag. 2015, 5, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Brian Cassel, J.; Kerr, K.M.; McClish, D.K.; Skoro, N.; Johnson, S.; Wanke, C.; Hoefer, D. Effect of a home-based palliative care program on healthcare use and costs. J. Am. Geriatr. Soc. 2016, 64, 2288–2295. [Google Scholar] [CrossRef] [PubMed]
- Boustani, M.A.; Sachs, G.A.; Alder, C.A.; Munger, S.; Schubert, C.C.; Guerriero Austrom, M.; Hake, A.M.; Unverzagt, F.W.; Farlow, M.; Matthews, B.R.; et al. Implementing innovative models of dementia care: The Healthy Aging Brain Center. Aging Ment. Health 2011, 15, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Gamarra Samaniego, M.D.P.; Blanquicett, C.J.; Araujo Castillo, R.V.; Chavez, J.C.; Beltrán Garate, B.E. Selected Domains within a Comprehensive Geriatric Assessment in Older Patients with Non-Hodgkin Lymphoma are Highly Associated with Frailty. Clin. Hematol. Int. 2022, 4, 35–43. [Google Scholar] [CrossRef]
- Taylor, D. Physical activity is medicine for older adults. Postgrad. Med. J. 2014, 90, 26–32. [Google Scholar] [CrossRef]
- Amireault, S.; Baier, J.M.; Spencer, J.R. Physical Activity Preferences Among Older Adults: A Systematic Review. J. Aging Phys. Act. 2018, 27, 128–139. [Google Scholar] [CrossRef]
- Geneva: World Health Organization. Global Recommendations on Physical Activity for Health. 2010. Available online: https://www.who.int/publications/i/item/9789241599979 (accessed on 14 November 2022).
- Beaudart, C.; Dawson, A.; Shaw, S.C.; Harvey, N.C.; Kanis, J.A.; Binkley, N.; Reginster, J.Y.; Chapurlat, R.; Chan, D.C.; Bruyère, O.; et al. Nutrition and physical activity in the prevention and treatment of sarcopenia: Systematic review. Osteoporos. Int. 2017, 28, 1817–1833. [Google Scholar] [CrossRef]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, Á.; Izquierdo, M. Role of physical exercise on cognitive function in healthy older adults: A systematic review of randomized clinical trials. Ageing Res. Rev. 2017, 37, 117–134. [Google Scholar] [CrossRef]
- Sherrington, C.; Fairhall, N.J.; Wallbank, G.K.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S.E. Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2019, 1, CD012424. [Google Scholar] [CrossRef]
- Pahor, M.; Guralnik, J.M.; Ambrosius, W.T.; Blair, S.; Bonds, D.E.; Church, T.S.; Espeland, M.A.; Fielding, R.A.; Gill, T.M.; Groessl, E.J.; et al. Effect of structured physical activity on prevention of major mobility disability in older adults: The LIFE study randomized clinical trial. JAMA 2014, 311, 2387–2396. [Google Scholar] [CrossRef]
- Martínez-Velilla, N.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Sáez de Asteasu, M.L.; Lucia, A.; Galbete, A.; García-Baztán, A.; Alonso-Renedo, J.; González-Glaría, B.; Gonzalo-Lázaro, M.; et al. Effect of Exercise Intervention on Functional Decline in Very Elderly Patients During Acute Hospitalization: A Randomized Clinical. JAMA Intern. Med. 2019, 179, 28–36, Erratum in JAMA Intern. Med. 2019, 179, 127. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, M.; Rodriguez-Mañas, L.; Sinclair, A.J. Editorial: What Is New in Exercise Regimes for Frail Older People—How Does the Erasmus Vivifrail Project Take Us Forward? J. Nutr. Health Aging 2016, 20, 736–737. [Google Scholar] [CrossRef] [PubMed]
- Casas-Herrero, Á.; Sáez de Asteasu, M.L.; Antón-Rodrigo, I.; Sánchez-Sánchez, J.L.; Montero-Odasso, M.; Marín-Epelde, I.; Ramón-Espinoza, F.; Zambom-Ferraresi, F.; Petidier-Torregrosa, R.; Elexpuru-Estomba, J.; et al. Effects of Vivifrail multicomponent intervention on functional capacity: A multicentre, randomized controlled trial. J. Cachexia Sarcopenia Muscle 2022, 13, 884–893. [Google Scholar] [CrossRef]
- De Coninck, L.; Bekkering, G.E.; Bouckaert, L.; Declercq, A.; Graff, M.J.L.; Aertgeerts, B. Home- and Community-Based Occupational Therapy Improves Functioning in Frail Older People: A Systematic Review. J. Am. Geriatr. Soc. 2017, 65, 1863–1869. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31, Erratum in Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [PubMed]
- Rothman, M.D.; Leo-Summers, L.; Gill, T.M. Prognostic significance of potential frailty criteria. J. Am. Geriatr. Soc. 2008, 56, 2211–2216. [Google Scholar] [CrossRef]
- Hu, X.; Zhang, L.; Wang, H.; Hao, Q.; Dong, B.; Yang, M. Malnutrition-sarcopenia syndrome predicts mortality in hospitalized older patients. Sci. Rep. 2017, 7, 3171. [Google Scholar] [CrossRef]
- Kaegi-Braun, N.; Boesiger, F.; Tribolet, P.; Gomes, F.; Kutz, A.; Hoess, C.; Pavlicek, V.; Bilz, S.; Sigrist, S.; Brändle, M.; et al. Validation of modified GLIM criteria to predict adverse clinical outcome and response to nutritional treatment: A secondary analysis of a randomized clinical trial. Clin. Nutr. 2022, 41, 795–804. [Google Scholar] [CrossRef]
- Leistra, E.; Willeboordse, F.; van Bokhorst-de van der Schueren, M.A.; Visser, M.; Weijs, P.J.; Haans-van den Oord, A.; Oostenbrink, J.; Evers, A.M.; Kruizenga, H.M. Predictors for achieving protein and energy requirements in undernourished hospital patients. Clin. Nutr. 2011, 30, 484–489. [Google Scholar] [CrossRef]
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Deiss, M.; Gomes, F.; Kutz, A.; Tribolet, P.; Bregenzer, T.; Braun, N.; et al. Individualised nutritional support in medical inpatients at nutritional risk: A randomised clinical trial. Lancet 2019, 393, 2312–2321. [Google Scholar] [CrossRef] [PubMed]
- Savino, E.; Sioulis, F.; Guerra, G.; Cavalieri, M.; Zuliani, G.; Guralnik, J.M.; Volpato, S. Potential Prognostic Value of Handgrip Strength in Older Hospitalized Patients. J. Frailty Aging 2012, 1, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Isaia, G.; Greppi, F.; Pastorino, A.; Bersano, E.M.; Rrodhe, S.; Aimonino Ricauda, N.; Bo, M.; Molinar Roet, K.; Zanocchi, M. Predictive effects of muscle strength after hospitalization in old patients. Aging Clin. Exp. Res. 2013, 25, 633–636. [Google Scholar] [CrossRef] [PubMed]
- Jyväkorpi, S.K.; Ramel, A.; Strandberg, T.E.; Piotrowicz, K.; Błaszczyk-Bębenek, E.; Urtamo, A.; Rempe, H.M.; Geirsdóttir, Ó.; Vágnerová, T.; Billot, M.; et al. The sarcopenia and physical frailty in older people: Multi-component treatment strategies (SPRINTT) project: Description and feasibility of a nutrition intervention in community-dwelling older Europeans. Eur. Geriatr. Med. 2021, 12, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.; Sobotka, L.; et al. ESPEN practical guideline: Clinical nutrition and hydration in geriatrics. Clin. Nutr. 2022, 41, 958–989. [Google Scholar] [CrossRef] [PubMed]
- Malmstrom, T.K.; Morley, J.E. Frailty and cognition: Linking two common syndromes in older persons. J. Nutr. Health Aging 2013, 17, 723–725. [Google Scholar] [CrossRef]
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; van Kan, G.A.; Ousset, P.J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J. Nutr. Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef]
- Ruan, Q.; Yu, Z.; Chen, M.; Bao, Z.; Li, J.; He, W. Cognitive frailty, a novel target for the prevention of elderly dependency. Ageing Res. Rev. 2015, 20, 1–10. [Google Scholar] [CrossRef]
- Chen, C.; Park, J.; Wu, C.; Xue, Q.; Agogo, G.; Han, L.; Hoogendijk, E.O.; Liu, Z.; Wu, Z. Cognitive frailty in relation to adverse health outcomes independent of multimorbidity: Results from the China health and retirement longitudinal study. Aging 2020, 12, 23129–23145. [Google Scholar] [CrossRef]
- Wang, J.; Kong, D.; Yu, F.; Conwell, Y.; Dong, X. Cognitive deficit, physical frailty, hospitalization and emergency department visits in later life. Aging Ment. Health 2021, 25, 521–527. [Google Scholar] [CrossRef]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Arai, H.; Satake, S.; Kozaki, K. Cognitive Frailty in Geriatrics. Clin. Geriatr. Med. 2018, 34, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Gómez, C.; Vega-Quiroga, S.; Bermejo-Pareja, F.; Medrano, M.J.; Louis, E.D.; Benito-León, J. Polypharmacy in the Elderly: A Marker of Increased Risk of Mortality in a Population-Based Prospective Study (NEDICES). Gerontology 2015, 61, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Stubbs, B.; Noale, M.; Solmi, M.; Pilotto, A.; Vaona, A.; Demurtas, J.; Mueller, C.; Huntley, J.; Crepaldi, G.; et al. Polypharmacy Is Associated With Higher Frailty Risk in Older People: An 8-Year Longitudinal Cohort Study. J. Am. Med. Dir. Assoc. 2017, 18, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Saum, K.U.; Schöttker, B.; Meid, A.D.; Holleczek, B.; Haefeli, W.E.; Hauer, K.; Brenner, H. Is Polypharmacy Associated with Frailty in Older People? Results from the ESTHER Cohort Study. J. Am. Geriatr. Soc. 2017, 65, e27–e32. [Google Scholar] [CrossRef]
- Morandi, A.; Bellelli, G.; Vasilevskis, E.E.; Turco, R.; Guerini, F.; Torpilliesi, T.; Speciale, S.; Emiliani, V.; Gentile, S.; Schnelle, J.; et al. Predictors of rehospitalization among elderly patients admitted to a rehabilitation hospital: The role of polypharmacy, functional status, and length of stay. J. Am. Med. Dir. Assoc. 2013, 14, 761–767. [Google Scholar] [CrossRef]
- Alshanberi, A.M. Recent Updates on Risk and Management Plans Associated with Polypharmacy in Older Population. Geriatrics 2022, 7, 97. [Google Scholar] [CrossRef]
- 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef]
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2015, 44, 213–218, Erratum in Age Ageing 2018, 47, 489. [Google Scholar] [CrossRef]
- Fusco, D.; Lattanzio, F.; Tosato, M.; Corsonello, A.; Cherubini, A.; Volpato, S.; Maraldi, C.; Ruggiero, C.; Onder, G. Development of CRIteria to assess appropriate Medication use among Elderly complex patients (CRIME) project: Rationale and methodology. Drugs Aging 2009, 26 (Suppl. S1), 3–13. [Google Scholar] [CrossRef]
- Unutmaz, G.D.; Soysal, P.; Tuven, B.; Isik, A.T. Costs of medication in older patients: Before and after comprehensive geriatric assessment. Clin. Interv. Aging 2018, 13, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Naharci, M.I.; Tasci, I. Frailty status and increased risk for falls: The role of anticholinergic burden. Arch. Gerontol. Geriatr. 2020, 90, 104136. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Chan, Y.F.; Shih, H.C.; Lee, C. Relationship between Potentially Inappropriate Anticholinergic Drugs (PIADs) and Adverse Outcomes among Elderly Patients in Taiwan. J. Food Drug Anal. 2012, 20, 930–937. [Google Scholar] [CrossRef]
- Gutiérrez-Valencia, M.; Martínez-Velilla, N.; Vetrano, D.L.; Corsonello, A.; Lattanzio, F.; Ladrón-Arana, S.; Onder, G. Anticholinergic burden and health outcomes among older adults discharged from hospital: Results from the CRIME study. Eur. J. Clin. Pharmacol. 2017, 73, 1467–1474. [Google Scholar] [CrossRef]
- Fuentes, E.; Fuentes, M.; Alarcon, M.; Palomo, I. Immune system dysfunction in the elderly. Acad. Bras. Cienc. 2017, 89, 285–299. [Google Scholar] [CrossRef]
- Crooke, S.N.; Ovsyannikova, I.G.; Poland, G.A.; Kennedy, R.B. Immunosenescence and human vaccine immune responses. Immun. Ageing 2019, 16, 25. [Google Scholar] [CrossRef]
- Franceschi, C.; Bonafè, M.; Valensin, S.; Olivieri, F.; De Luca, M.; Ottaviani, E.; De Benedictis, G. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann. N. Y Acad. Sci. 2000, 908, 244–254. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, S.; Leng, S.X. Chronic Low-grade Inflammatory Phenotype (CLIP) and Senescent Immune Dysregulation. Clin. Ther. 2019, 41, 400–409. [Google Scholar] [CrossRef]
- Soysal, P.; Arik, F.; Smith, L.; Jackson, S.E.; Isik, A.T. Inflammation, Frailty and Cardiovascular Disease. Adv. Exp. Med. Biol. 2020, 1216, 55–64. [Google Scholar] [CrossRef]
- Weinberger, B. Vaccination of older adults: Influenza, pneumococcal disease, herpes zoster, COVID-19 and beyond. Immun. Ageing 2021, 18, 38. [Google Scholar] [CrossRef]
- Mehrabi, F.; Béland, F. Effects of social isolation, loneliness and frailty on health outcomes and their possible mediators and moderators in community-dwelling older adults: A scoping review. Arch. Gerontol. Geriatr. 2020, 90, 104119. [Google Scholar] [CrossRef] [PubMed]
- Giuli, C.; Spazzafumo, L.; Sirolla, C.; Abbatecola, A.M.; Lattanzio, F.; Postacchini, D. Social isolation risk factors in older hospitalized individuals. Arch. Gerontol. Geriatr. 2012, 55, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, D.; Lee, D.C.A.; Robins, L.M.; Haines, T.P. Risk factors for social isolation in post-hospitalized older adults. Arch. Gerontol. Geriatr. 2020, 88, 104036. [Google Scholar] [CrossRef] [PubMed]
- Siette, J.; Cassidy, M.; Priebe, S. Effectiveness of befriending interventions: A systematic review and meta-analysis. BMJ Open 2017, 7, e014304. [Google Scholar] [CrossRef] [PubMed]
- Dickens, A.P.; Richards, S.H.; Greaves, C.J.; Campbell, J.L. Interventions targeting social isolation in older people: A systematic review. BMC Public Health 2011, 11, 647. [Google Scholar] [CrossRef]
- Czaja, S.J.; Sharit, J.; Boot, W.R.; Charness, N.H.; Rogers, W.A. The role of technology in supporting social engagement and social support among older adults. Innov. Aging 2017, 1 (Suppl. S1), 1026–1027. [Google Scholar] [CrossRef]
- The World Health Organization (WHO). Available online: https://www.who.int/teams/social-determinants-of-health/demographic-change-and-healthy-ageing/age-friendly-environments (accessed on 10 September 2023).
- Inouye, S.K.; Bogardus, S.T., Jr.; Baker, D.I.; Leo-Summers, L.; Cooney, L.M., Jr. The Hospital Elder Life Program: A model of care to prevent cognitive and functional decline in older hospitalized patients. Hosp. Elder. Life Program. J. Am. Geriatr. Soc. 2000, 48, 1697–1706. [Google Scholar] [CrossRef]
- Hshieh, T.T.; Yang, T.; Gartaganis, S.L.; Yue, J.; Inouye, S.K. Hospital Elder Life Program: Systematic Review and Meta-Analysis of Effectiveness. Am. J. Geriatr. Psychiatry 2018, 26, 1015–1033. [Google Scholar] [CrossRef]
- Ajay, S.; Kasthuri, A.; Kiran, P.; Malhotra, R. Association of impairments of older persons with caregiver burden among family caregivers: Findings from rural South India. Arch. Gerontol. Geriatr. 2017, 68, 143–148. [Google Scholar] [CrossRef]
- Riffin, C.; Van Ness, P.H.; Wolff, J.L.; Fried, T. Multifactorial Examination of Caregiver Burden in a National Sample of Family and Unpaid Caregivers. J. Am. Geriatr. Soc. 2019, 67, 277–283. [Google Scholar] [CrossRef]
- Ringer, T.J.; Hazzan, A.A.; Kennedy, C.C.; Karampatos, S.; Patterson, C.; Marr, S.; Misiaszek, B.; Woo, T.; Ioannidis, G.; Papaioannou, A. Care recipients’ physical frailty is independently associated with subjective burden in informal caregivers in the community setting: A cross-sectional study. BMC Geriatr. 2016, 16, 186. [Google Scholar] [CrossRef] [PubMed]
- Gok Metin, Z.; Karadas, C.; Balci, C.; Cankurtaran, M. The Perceived Caregiver Burden Among Turkish Family Caregivers Providing Care for Frail Older Adults. J. Transcult. Nurs. 2019, 30, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Isik, A.T.; Soysal, P.; Solmi, M.; Veronese, N. Bidirectional relationship between caregiver burden and neuropsychiatric symptoms in patients with Alzheimer’s disease: A narrative review. Int. J. Geriatr. Psychiatry 2019, 34, 1326–1334. [Google Scholar] [CrossRef] [PubMed]
- Casarett, D.; Pickard, A.; Bailey, F.A.; Ritchie, C.; Furman, C.; Rosenfeld, K.; Shreve, S.; Chen, Z.; Shea, J.A. Do palliative consultations improve patient outcomes? J. Am. Geriatr. Soc. 2008, 56, 593–599. [Google Scholar] [CrossRef]
- Morrison, R.S.; Penrod, J.D.; Cassel, J.B.; Caust-Ellenbogen, M.; Litke, A.; Spragens, L.; Meier, D.E.; Palliative Care Leadership Centers’ Outcomes Group. Cost savings associated with us hospital palliative care consultation programs. Arch. Intern. Med. 2008, 168, 1783–1790. [Google Scholar] [CrossRef]
- Sganga, F.; Barillaro, C.; Tamburrano, A.; Nicolotti, N.; Cambieri, A.; Bernabei, R.; Turriziani, A. The benefits of a hospital palliative care team. Int. J. Palliat. Nurs. 2019, 25, 345–352. [Google Scholar] [CrossRef]
- Shafiee Hanjani, L.; Fox, S.; Hubbard, R.E.; Gordon, E.; Reid, N.; Hilmer, S.N.; Saunders, R.; Gnjidic, D.; Young, A. Frailty knowledge, training and barriers to frailty management: A national cross-sectional survey of health professionals in Australia. Australas. J. Ageing 2023. ahead of print. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
|
|
| Frailty Instrument | Domains İncluded | Scoring | Time to Complete | Setting | |||||
|---|---|---|---|---|---|---|---|---|---|
| Physical Function | Physical Activity | Cognition | Comorbidity | Weight Loss | Other (Social, Demographic, etc.) | ||||
| Physical Frailty Phenotype [2] | yes | yes | no | no | yes | no | Frailty: ≥3 items Pre-frailty: 1–2 items Robust: 0 items | 5–10 min |
|
| Frailty Index [41] | yes | no | yes | yes | no | yes | Suggested cutoff score for frailty: >0.5 | Varies depending on number and type of measures included |
|
| Electronic Frailty Index [44] | yes | no | yes | yes | yes | yes | Severe frailty: score >0.36 Frailty: score >0.24–0.36 Mild frailty: score > 0.12–0.24 Fit: score ≤ 0.12 | Varies depending on number and type of measures included |
|
| FRAIL Scale [45] | yes | no | no | yes | yes | no | Score range 0 to 5 No frailty = 0 deficits Intermediate frailty = 1 or 2 deficits Frailty = 3 or more deficits | Less than 5 min |
|
| Clinical Frailty Scale [46] | yes | yes | no | yes | no | yes | Frailty: score ≥5 | Less than 5 min |
|
| Edmonton Frail Scale (EFS) [47] | yes | yes | yes | yes | yes | yes | Frailty: score ≥ 7 | 5–10 min |
|
| Study of Osteoporotic Fracture (SOF) Frailty Measure [48] | yes | yes | no | no | yes | no | Frailty: ≥2 items Pre-frailty: 1 item Robust: 0 items | Less than 5 min |
|
| Geriatric 8 Frailty Questionnaire for Oncology (G8 ) [49] | yes | no | yes | no | yes | yes | Frailty: score ≤ 14 | Less than 5 min |
|
| Vulnerable Elders Survey (VES-13) [50] | yes | yes | no | no | no | yes | Frailty: score ≥ 3 | Less than 5 min |
|
| Short Physical Performance Battery [51] | yes | yes | no | no | no | no | Frailty: score ≤ 9 | 5–10 min |
|
| Multidimensional Prognostic Index (MPI) [52] | yes | no | yes | yes | yes | yes | Frailty: Low risk: 0 Moderate risk: 0.5 Severe risk: 1 | varies depending on number and type of measures included. |
|
| Frailty Risk Score [53] | yes | yes | no | yes | no | yes | Very good: score < 45 Good: score 45–50 Moderate: score 51–55 Poor: score 56–61 Very poor: score > 61 | 5–10 min |
|
| Hospital Frailty Risk Score [54] | yes | no | yes | yes | no | no | Low risk: score < 5 Intermediate risk: score 5–15 High risk: score > 15 | 5–10 min |
|
| Pre-Physical Frailty | Physical Frailty | |
|---|---|---|
| Pre-MCI/SCD | Reversible cognitive frailty | |
| MCI | Potentially reversible cognitive frailty | Cognitive frailty |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bag Soytas, R.; Levinoff, E.J.; Smith, L.; Doventas, A.; Morais, J.A.; Veronese, N.; Soysal, P. Predictive Strategies to Reduce the Risk of Rehospitalization with a Focus on Frail Older Adults: A Narrative Review. Epidemiologia 2023, 4, 382-407. https://doi.org/10.3390/epidemiologia4040035
Bag Soytas R, Levinoff EJ, Smith L, Doventas A, Morais JA, Veronese N, Soysal P. Predictive Strategies to Reduce the Risk of Rehospitalization with a Focus on Frail Older Adults: A Narrative Review. Epidemiologia. 2023; 4(4):382-407. https://doi.org/10.3390/epidemiologia4040035
Chicago/Turabian StyleBag Soytas, Rabia, Elise J. Levinoff, Lee Smith, Alper Doventas, José A. Morais, Nicola Veronese, and Pinar Soysal. 2023. "Predictive Strategies to Reduce the Risk of Rehospitalization with a Focus on Frail Older Adults: A Narrative Review" Epidemiologia 4, no. 4: 382-407. https://doi.org/10.3390/epidemiologia4040035