
Racial/Ethnic Disparities of Cancer, Metabolic Syndrome, and Lifestyle Behaviors in People under 50: A Cross-Sectional Study of Data from the National Health and Nutrition Examination Survey

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Measures
2.3. Statistical Analysis
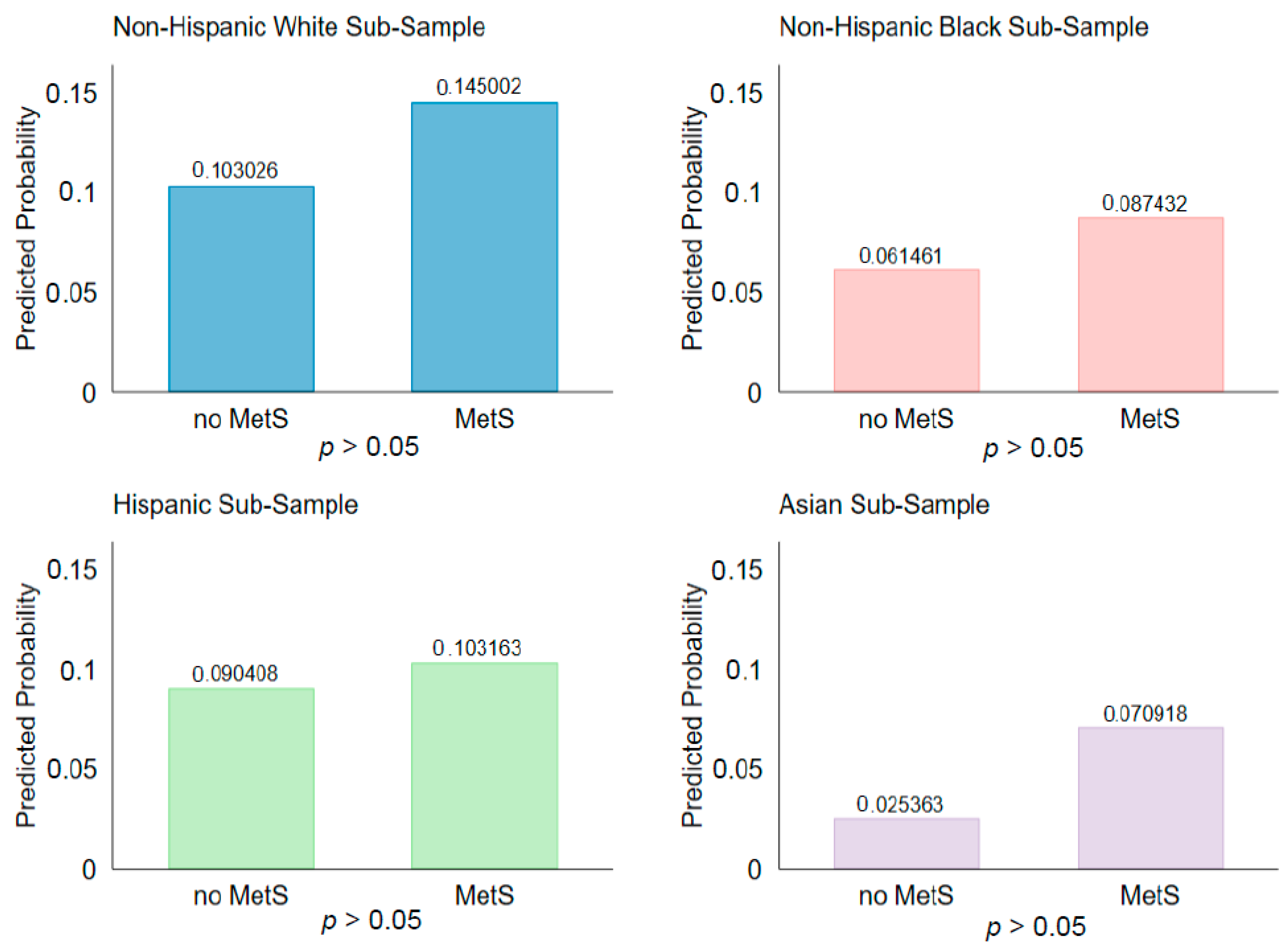
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kassi, E.; Pervanidou, P.; Kaltsas, G.; Chrousos, G. Metabolic Syndrome: Definitions and Controversies. BMC Med. 2011, 9, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, H.; Ryan, D.A.; Celzo, M.F.; Stapleton, D. Metabolic Syndrome: Definition and Therapeutic Implications. Postgrad. Med. 2012, 124, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C.; et al. Diagnosis and Management of the Metabolic Syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.M.; Zimmet, P.; Shaw, J. The Metabolic Syndrome—A New Worldwide Definition. The Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Welzel, T.M.; Graubard, B.I.; Zeuzem, S.; El-Serag, H.B.; Davila, J.A.; McGlynn, K.A. Metabolic Syndrome Increases the Risk of Primary Liver Cancer in the United States: A Study in the SEER-Medicare Database. Hepatology 2011, 54, 463–471. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Estevez, L.; Moreno-Bueno, G. Updating the Role of Obesity and Cholesterol in Breast Cancer. Breast Cancer Res. 2019, 21, 35. [Google Scholar] [CrossRef] [Green Version]
- Nicolucci, A. Epidemiological Aspects of Neoplasms in Diabetes. Acta Diabetol. 2010, 47, 87–95. [Google Scholar] [CrossRef]
- Giovannucci, E.; Harlan, D.M.; Archer, M.C.; Bergenstal, R.M.; Gapstur, S.M.; Habel, L.A.; Pollak, M.; Regensteiner, J.G.; Yee, D. Diabetes and Cancer: A Consensus Report. CA. Cancer J. Clin. 2010, 60, 207–221. [Google Scholar] [CrossRef] [Green Version]
- Maiti, B.; Kundranda, M.N.; Spiro, T.P.; Daw, H.A. The Association of Metabolic Syndrome with Triple-Negative Breast Cancer. Breast Cancer Res. Treat. 2010, 121, 479–483. [Google Scholar] [CrossRef]
- Alfa-Wali, M.; Boniface, S.; Sharma, A.; Tekkis, P.; Hackshaw, A.; Antoniou, A. Metabolic Syndrome (Mets) and Risk of Colorectal Cancer (CRC): A Systematic Review and Meta-Analysis. World J. Surg. Med. Radiat. Oncol. 2015, 4, 7. [Google Scholar]
- Trabert, B.; Wentzensen, N.; Felix, A.S.; Yang, H.P.; Sherman, M.E.; Brinton, L.A. Metabolic Syndrome and Risk of Endometrial Cancer in the United States: A Study in the SEER–Medicare Linked Database. Cancer Epidemiol. Prev. Biomark. 2015, 24, 261–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossman, E.; Messerli, F.H.; Boyko, V.; Goldbourt, U. Is There an Association between Hypertension and Cancer Mortality? Am. J. Med. 2002, 112, 479–486. [Google Scholar] [CrossRef]
- Tran, D.-M.T.; Zimmerman, L.M. Cardiovascular Risk Factors in Young Adults: A Literature Review. J. Cardiovasc. Nurs. 2015, 30, 298–310. [Google Scholar] [CrossRef]
- Lascar, N.; Brown, J.; Pattison, H.; Barnett, A.H.; Bailey, C.J.; Bellary, S. Type 2 Diabetes in Adolescents and Young Adults. Lancet Diabetes Endocrinol. 2018, 6, 69–80. [Google Scholar] [CrossRef] [Green Version]
- Szczurkowska, P.J.; Polonis, K.; Becari, C.; Hoffmann, M.; Narkiewicz, K.; Chrostowska, M. Epilepsy and Hypertension: The Possible Link for Sudden Unexpected Death in Epilepsy? Cardiol. J. 2021, 28, 330–335. [Google Scholar] [CrossRef] [Green Version]
- Venugopal, A.; Stoffel, E.M. Colorectal Cancer in Young Adults. Curr. Treat. Options Gastroenterol. 2019, 17, 89–98. [Google Scholar] [CrossRef]
- Sung, H.; Siegel, R.L.; Rosenberg, P.S.; Jemal, A. Emerging Cancer Trends among Young Adults in the USA: Analysis of a Population-Based Cancer Registry. Lancet Public Health 2019, 4, e137–e147. [Google Scholar] [CrossRef] [Green Version]
- Monestime, S.; Beech, B.; Kermah, D.; Norris, K. Prevalence and Predictors of Obesity-Related Cancers among Racial/Ethnic Groups with Metabolic Syndrome. PLoS ONE 2021, 16, e0249188. [Google Scholar] [CrossRef]
- Zavala, V.A.; Bracci, P.M.; Carethers, J.M.; Carvajal-Carmona, L.; Coggins, N.B.; Cruz-Correa, M.R.; Davis, M.; de Smith, A.J.; Dutil, J.; Figueiredo, J.C.; et al. Cancer Health Disparities in Racial/Ethnic Minorities in the United States. Br. J. Cancer 2021, 124, 315–332. [Google Scholar] [CrossRef]
- Haw, J.S.; Shah, M.; Turbow, S.; Egeolu, M.; Umpierrez, G. Diabetes Complications in Racial and Ethnic Minority Populations in the USA. Curr. Diab. Rep. 2021, 21, 2. [Google Scholar] [CrossRef] [PubMed]
- Falkner, B.; Cossrow, N.D.F.H. Prevalence of Metabolic Syndrome and Obesity-Associated Hypertension in the Racial Ethnic Minorities of the United States. Curr. Hypertens. Rep. 2014, 16, 449. [Google Scholar] [CrossRef] [Green Version]
- Lillie-Blanton, M.; Hoffman, C. The Role of Health Insurance Coverage In Reducing Racial/Ethnic Disparities In Health Care. Health Aff. 2005, 24, 398–408. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Jemal, A. Socioeconomic and Racial/Ethnic Disparities in Cancer Mortality, Incidence, and Survival in the United States, 1950–2014: Over Six Decades of Changing Patterns and Widening Inequalities. Available online: https://www.hindawi.com/journals/jeph/2017/2819372/abs/ (accessed on 1 April 2019).
- Polite, B.N.; Adams-Campbell, L.L.; Brawley, O.W.; Bickell, N.; Carethers, J.M.; Flowers, C.R.; Foti, M.; Gomez, S.L.; Griggs, J.J.; Lathan, C.S.; et al. Charting the Future of Cancer Health Disparities Research: A Position Statement from the American Association for Cancer Research, the American Cancer Society, the American Society of Clinical Oncology, and the National Cancer Institute. CA. Cancer J. Clin. 2017, 67, 353–361. [Google Scholar] [CrossRef] [Green Version]
- Zhu, S.; St-Onge, M.-P.; Heshka, S.; Heymsfield, S.B. Lifestyle Behaviors Associated with Lower Risk of Having the Metabolic Syndrome. Metabolism 2004, 53, 1503–1511. [Google Scholar] [CrossRef]
- Lin, K.-M.; Chiou, J.-Y.; Ko, S.-H.; Tan, J.-Y.; Huang, C.-N.; Liao, W.-C. Modifiable Lifestyle Behaviors Are Associated with Metabolic Syndrome in a Taiwanese Population. J. Nurs. Scholarsh. Off. Publ. Sigma Theta Tau Int. Honor Soc. Nurs. 2015, 47, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Moon, S. Unhealthy Lifestyle Behaviors in Korean People with Metabolic Syndrome. J. Community Health Nurs. 2017, 34, 69–79. [Google Scholar] [CrossRef]
- Chen, T.C.; Clark, J.; Riddles, M.K.; Mohadjer, L.K.; Fakhouri, T.H. National Health and Nutrition Examination Survey, 2015− 2018: Sample design and estimation procedures. Vital Health Stat. 2020, 184, 1–35. Available online: https://www.cdc.gov/nchs/data/series/sr_02/sr02-184-508.pdf (accessed on 2 October 2021).
- NHANES 2015-2016 Overview. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/overview.aspx?BeginYear=2015 (accessed on 12 February 2020).
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic Syndrome—A New World-Wide Definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- Taylor, A.L.; Denniston, M.M.; Klevens, R.M.; McKnight-Eily, L.R.; Jiles, R.B. Association of Hepatitis C Virus with Alcohol Use Among U.S. Adults: NHANES 2003–2010. Am. J. Prev. Med. 2016, 51, 206–215. [Google Scholar] [CrossRef] [Green Version]
- Smiley, A.; King, D.; Bidulescu, A. The Association between Sleep Duration and Metabolic Syndrome: The NHANES 2013/2014. Nutrients 2019, 11, 2582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stata 16 Base Reference Manual; StataCorp: College Station, TX, USA; Stata Press: College Station, TX, USA, 2017.
- Long, J.S.; Freese, J. Regression Models for Categorical Dependent Variables Using Stata, 3rd ed.; Stata Press: College Station, TX, USA, 2014; ISBN 978-1-59718-111-2. [Google Scholar]
- NHANES Subsample Notes and Data. Available online: https://wwwn.cdc.gov/nchs/nhanes/search/subsample_weights.aspx (accessed on 13 February 2020).
- Xue, F.; Michels, K.B. Diabetes, Metabolic Syndrome, and Breast Cancer: A Review of the Current Evidence. Am. J. Clin. Nutr. 2007, 86, 823S–835S. [Google Scholar] [CrossRef]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic Syndrome and Risk of Cancer: A Systematic Review and Meta-Analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef] [Green Version]
- Rose, D.P.; Haffner, S.M.; Baillargeon, J. Adiposity, the Metabolic Syndrome, and Breast Cancer in African-American and White American Women. Endocr. Rev. 2007, 28, 763–777. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.S.; Beech, B.M.; Griffith, D.M.; Thorpe, R.J., Jr. The Association between Hypertension and Race/Ethnicity among Breast Cancer Survivors. J. Racial Ethn. Health Disparities 2020, 7, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Cook, L.S.; Nelson, H.E.; Cockburn, M.; Olson, S.H.; Muller, C.Y.; Wiggins, C.L. Comorbidities and Endometrial Cancer Survival in Hispanics and Non-Hispanic Whites. Cancer Causes Control 2013, 24, 61–69. [Google Scholar] [CrossRef]
- Chen, Y.; Wu, F.; Saito, E.; Lin, Y.; Song, M.; Luu, H.N.; Gupta, P.C.; Sawada, N.; Tamakoshi, A.; Shu, X.-O.; et al. Association between Type 2 Diabetes and Risk of Cancer Mortality: A Pooled Analysis of over 771,000 Individuals in the Asia Cohort Consortium. Diabetologia 2017, 60, 1022–1032. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Tan, F.; Wei, L.; Li, X.; Lyu, Z.; Feng, X.; Wen, Y.; Guo, L.; He, J.; Dai, M.; et al. Sleep Duration and the Risk of Cancer: A Systematic Review and Meta-Analysis Including Dose–Response Relationship. BMC Cancer 2018, 18, 1149. [Google Scholar] [CrossRef] [Green Version]
- Knutson, K.L.; Spiegel, K.; Penev, P.; Van Cauter, E. The Metabolic Consequences of Sleep Deprivation. Sleep Med. Rev. 2007, 11, 163–178. [Google Scholar] [CrossRef] [Green Version]
- Narayan, K.M.V.; Aviles-Santa, L.; Oza-Frank, R.; Pandey, M.; Curb, J.D.; McNeely, M.; Araneta, M.R.G.; Palaniappan, L.; Rajpathak, S.; Barrett-Connor, E.; et al. Report of a National Heart, Lung, and Blood Institute Workshop: Heterogeneity in Cardiometabolic Risk in Asian Americans in the U.S.: Opportunities for Research. J. Am. Coll. Cardiol. 2010, 55, 966–973. [Google Scholar] [CrossRef] [Green Version]
- Das, A.; Ambale-Venkatesh, B.; Lima, J.A.C.; Freedman, J.E.; Spahillari, A.; Das, R.; Das, S.; Shah, R.V.; Murthy, V.L. Cardiometabolic Disease in South Asians: A Global Health Concern in an Expanding Population. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Yang, W.J.; Spence, C.B.; Bhimla, A.; Ma, G.X. Lean Yet Unhealthy: Asian American Adults Had Higher Risks for Metabolic Syndrome than Non-Hispanic White Adults with the Same Body Mass Index: Evidence from NHANES 2011–2016. Healthcare 2021, 9, 1518. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Chan, Z.; Chooi, Y.C.; Choo, J.; Sadananthan, S.A.; Chang, A.; Sasikala, S.; Michael, N.; Velan, S.S.; Magkos, F. Regulation of Glucose Metabolism in Nondiabetic, Metabolically Obese Normal-Weight Asians. Am. J. Physiol. Endocrinol. Metab. 2018, 314, E494–E502. [Google Scholar] [CrossRef]
- Lévy, P.; Bonsignore, M.R.; Eckel, J. Sleep, Sleep-Disordered Breathing and Metabolic Consequences. Eur. Respir. J. 2009, 34, 243–260. [Google Scholar] [CrossRef] [Green Version]
- Hairston, K.G.; Bryer-Ash, M.; Norris, J.M.; Haffner, S.; Bowden, D.W.; Wagenknecht, L.E. Sleep Duration and Five-Year Abdominal Fat Accumulation in a Minority Cohort: The IRAS Family Study. Sleep 2010, 33, 289–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toyama, Y.; Tanizawa, K.; Kubo, T.; Chihara, Y.; Harada, Y.; Murase, K.; Azuma, M.; Hamada, S.; Hitomi, T.; Handa, T.; et al. Impact of Obstructive Sleep Apnea on Liver Fat Accumulation According to Sex and Visceral Obesity. PLoS ONE 2015, 10, e0129513. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| % of Mean (95% Confidence Interval) | Non-Hispanic White (NHW) (N = 3604) | Non-Hispanic Black (NHB) (N = 2382) | Hispanic (N = 2646) | Asian (N = 1588) | p |
|---|---|---|---|---|---|
| Cancer (yes %) | 4.52% (3.91–5.60%) | 1.15% (0.70–1.51%) | 2.04% (1.31–2.29%) | 0.72% (0.22–1.11%) | <0.001 |
| MetS (yes %) | 25.65% (23.23–28.82%) | 19.32% (18.49–22.21%) | 31.44% (29.65–33.88%) | 22.81% (19.69–24.05%) | <0.001 |
| Age, mean | 33.89 (33.29–34.50) | 32.77 (32.00–33.54) | 32.72 (32.31–33.13) | 34.15 (33.36–34.94) | <0.001 † |
| Sex, female | 49.70% (48.19–51.17%) | 54.52% (53.39–56.84%) | 49.58% (48.07–51.16%) | 52.30% (50.73–54.70%) | 0.0013 |
| Education | <0.001 | ||||
| <HS | 9.15% (7.64–10.93%) | 14.61% (12.99–16.39%) | 33.69% (30.98–36.52%) | 8.14% (6.33–10.40%) | |
| HS or some college | 55.78% (52.64–58.86%) | 66.14% (63.80–68.41%) | 53.81% (51.53–56.08%) | 34.75% (30.31–39.47%) | |
| College or above | 35.06% (30.82–28.80%) | 19.25% (15.55–21.77%) | 12.49% (10.25–14.57%) | 57.11% (53.43–62.72%) | |
| Excessive drinking (yes %) | 55.53% (60.47–66.11%) | 49.38% (62.19–68.33%) | 62.61% (70.62–75.31%) | 32.65% (55.76–63.83%) | <0.001 |
| Tobacco use (yes %) | 43.21% (39.90–45.46%) | 30.16% (27.90–33.45%) | 30.65% (28.54–32.77%) | 19.18% (18.18–22.38%) | <0.001 |
| Sleep duration | <0.001 | ||||
| <6 h/day | 8.85% (8.17–11.26%) | 18.48% (17.15–21.21%) | 10.38% (9.11–12.46%) | 6.50% (5.05–8.43%) | |
| ≥6 h | 91.95% (89.69–92.94%) | 81.52% (79.82–83.10%) | 89.62% (88.00–91.05%) | 93.50% (91.86–94.83%) |
| Non-Hispanic White (NHW) | Non-Hispanic Black (NHB) | Hispanic | Asian | |
|---|---|---|---|---|
| Odds Ratio (95% Confident Interval) | ||||
| MetS | 1.57 * (1.01–2.45) | 1.57 (0.54–4.60) | 1.20 (0.56–2.60) | 3.67 (0.70–19.10) |
| Age, mean | 1.06 *** (1.04–1.09) | 1.10 ** (1.04–1.16) | 1.08 ** (1.03–1.14) | 1.08 (0.95–1.24) |
| Female sex (ref: male) | 2.40 *** (1.52–3.79) | 1.56 (0.52–4.73) | 4.67 *** (2.14–10.19) | 4.46 * (1.05–18.88) |
| College degree (ref: < HS) | ||||
| HS or some college | 0.96 (0.50–1.86) | 0.71 (0.22–2.22) | 1.20 (0.50–2.88) | 4.48 (0.06–3.72) |
| College or above | 1.41 (0.69–2.90) | 1.20 (0.32–4.43) | 0.66 (0.21–2.06) | 1.07 (0.22–5.33) |
| Excessive drinking (ref: no) | 0.99 (0.60–1.63) | 0.96 (0.41–2.24) | 0.78 (0.39–1.58) | 0.38 (0.05–2.63) |
| Tobacco use (ref: no) | 1.48 * (1.00–2.19) | 1.47 (0.52–4.20) | 2.39 * (1.09–5.24) | 2.09 (0.44–9.84) |
| Sleep duration ≥ 6 h (ref: < 6 h) | 0.83 (0.53–1.32) | 0.44 (0.16–1.26) | 0.91 (0.23–3.60) | 0.15 ** (0.04–0.54) |
| Constant | 0.002 | 0.0005 | 0.0003 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, L.; Rahman, A.; Yeh, M.-C.; Ma, G.X. Racial/Ethnic Disparities of Cancer, Metabolic Syndrome, and Lifestyle Behaviors in People under 50: A Cross-Sectional Study of Data from the National Health and Nutrition Examination Survey. Epidemiologia 2022, 3, 493-501. https://doi.org/10.3390/epidemiologia3040037
Zhu L, Rahman A, Yeh M-C, Ma GX. Racial/Ethnic Disparities of Cancer, Metabolic Syndrome, and Lifestyle Behaviors in People under 50: A Cross-Sectional Study of Data from the National Health and Nutrition Examination Survey. Epidemiologia. 2022; 3(4):493-501. https://doi.org/10.3390/epidemiologia3040037
Chicago/Turabian StyleZhu, Lin, Areebah Rahman, Ming-Chin Yeh, and Grace X. Ma. 2022. "Racial/Ethnic Disparities of Cancer, Metabolic Syndrome, and Lifestyle Behaviors in People under 50: A Cross-Sectional Study of Data from the National Health and Nutrition Examination Survey" Epidemiologia 3, no. 4: 493-501. https://doi.org/10.3390/epidemiologia3040037