
Orthopedic Complications and Management in Children with X-Linked Hypophosphatemia

Department of Orthopaedic Surgery, Osaka Women’s and Children’s Hospital, Izumi 594-1101, Osaka, Japan
Endocrines 2022, 3(3), 488-497; https://doi.org/10.3390/endocrines3030039
Submission received: 25 May 2022
/
Revised: 19 July 2022
/
Accepted: 28 July 2022
/
Published: 3 August 2022
(This article belongs to the Special Issue Update on X-linked Hypophosphatemia)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:X-linked hypophosphatemia is an inheritable disease of renal phosphate wasting that results in clinically manifestations associated with rickets or osteomalacia. The various symptoms in the skeletal system are well recognized, such as short stature; lower limb deformities; and bone, joint, or muscle pain, and it is often difficult to control these symptoms, despite the use of medication therapy in growing children. In addition, lower limb deformities can lead to degenerative osteoarthritis and dysfunction of lower limbs at the skeletal maturity. To prevent from future manifestation of those symptoms, orthopedic surgeries are applicable to growing patients with severe skeletal deformities or without response to conventional medication. Bone deformities are treated by acute or gradual corrective osteotomies and temporally hemiepiphysiodesis using guided growth method. The clinicians should choose the right procedure based on age, symptoms and state of deformities of the patient.
1. Introduction
X-linked hypophosphatemia (XLH, OMIM #307800) is a rare genetic disorder caused by renal phosphate wasting and is the most common form of hypophosphatemic rickets and osteomalacia. This disease causes fibroblast growth factor 23 (FGF23)-related hypophosphatemia. FGF23 is a circulating hormone for phosphate regulation throughout the whole body, and the elevation of this growth factor leads to renal wasting of phosphate and low serum phosphate. The responsible gene for XLH is identified on PHEX (phosphate-regulating protein with homology to endopeptidases on the X chromosome) [1,2]. A decrease or absence of PHEX activity induces an increase in FGF23. On the other hand, bone is mainly composed of hydroxyapatite and collagens, and hydroxyapatite contains phosphate in its own structure. Therefore, skeletal complications are caused as phosphate regulation is out of order in the PHEX/FGF23 axis. This condition causes rickets, which is characterized by the impairment of the maturation of growth plates in patients during childhood, as well as osteomalacia, which is characterized by the disturbance of mineralization in osteoids in adulthood. Lower limb deformities and various sequelae such as gait alterations or pain in the lower limbs, which are the main complaints of patients with rickets [3], have been reported in affected children and adults [4,5,6] and are associated with impairment of quality of life [7].
The diagnosis of patients with XLH is generally made in childhood, and the treatment with medication is continued throughout the lifetime. Oral phosphate and active vitamin D are generally administered, with active vitamin D being included in the conventional treatment. This treatment promotes the growth and improvement of skeletal deformities such as bowlegs and alleviates bone, joint, and muscle pain. The good control of phosphate caused by the medication reduces the need for orthopedic surgeries [8,9,10]. However, the responses to this medical treatment are varied, and operative procedures for bone deformities can be chosen in unsuccessful cases of medication [11,12,13]. Burosumab, an anti-fibroblast growth factor 23 antibody, is approved for this disease [14,15,16] and expected to be efficacious for various symptoms, including bone deformities. However, there are only two papers on the efficacy for bone deformities of this new medication at present.
This article reviews the orthopedic complications and recent orthopedic interventions in children with XLH.
2. Orthopedic Features and Treatments in Infancy and Early Childhood
XLH is a dominant disorder. If a parent or siblings of a newborn infant has been diagnosed with XLH, the baby can be expected to have XLH and a careful investigation of hypophosphatemia would be performed by a pediatrician. However, in the absence of the family history of XLH, this disorder should be suspected based on physical and radiographic findings as described below.
2.1. Bowlegs
The most characteristic orthopedic feature of XLH is a bowleg in childhood, especially after the start of standing and walking in early childhood. Weight-bearing leads lower limbs to more serious deformities than physiological varus or valgus knee deformities in XLH patients. Bowlegs in early childhood occur due to several causes, including vitamin D deficiency, Blount disease (epiphysitis in the proximally medial tibia), physiological factors, and so on. The clinicians should make a differential diagnosis between XLH and these conditions using various examinations.
Plain radiographic images of lower limbs should be examined for the differential diagnoses at the initial visit. The widening of epiphyseal plates and an unclear demarcation line between the epiphyseal plate and metaphysis are characteristically demonstrated in patients with rickets, and these factors should lead to a strong suspicion of rickets. However, these characteristic findings are detected in various forms of rickets. In particular, it is essential to differentiate between XLH and rickets caused by vitamin D insufficiency. In addition, these features are not always obvious upon first examination, and follow-up examinations are necessary for the diagnosis. In general, pediatricians commonly perform radiographic examinations of the wrist and knee joints in patients with rickets. From the point of view of orthopedists, radiographic images of the whole lower limbs should additionally be obtained not in a supine position but a standing position to evaluate the degree of a patient’s varus deformity and functional disability in a standing posture. For the evaluation of limb deformities and functional disability, a mechanical axis deviation (MAD) is the most valuable parameter (Figure 1) [17]. The mechanical axis is defined as the line between the center of the femoral head and the center of the ankle joint on plain radiographic images of whole lower limbs in a standing individual. It represents a main weight-bearing point on the knee joint. An MAD shows the displacement of the mechanical axis from the center of the knee joint, and a large deviation to the medial or lateral side indicates severe deformity of the limb alignment.
The ideal mechanical axis line passes through the center of the knee joint and the ideal MAD is 0 mm. This parameter is useful for the objective assessment of the improvement or aggravation of limb deformities during follow-up examinations [18].
If the clinicians find radiographic evidence of rickets, they can add a radiographic survey of the growth plate around the wrist or knee joints for an assessment of pathological conditions using the Ricket Severity Score (RSS), which is a quantitative method based on the degree of metaphyseal fraying, concavity, and the rate of affected physis [19]. Recently, the Radiographic Global Impression of Change (RGI-C) score, which was developed in the evaluation of changes in hypophosphatasia [20], has been used to assess the healing of rickets in pediatric XLH patients [21]. If the patient has less obvious findings in the radiographic images, the clinicians should follow the changes of the genu varum with age. The various deformities around knee joints do not get better in most rachitic cases, while almost all physiological bowlegs improve. The development of a varus deformity is useful for the differential diagnosis between rickets and other conditions.
Laboratory abnormalities, which include hypophosphatemia and elevated alkaline phosphatase activity, must be checked in cases of rickets, including XLH. Recently, the FGF23 level and a mutation analysis of the PHEX gene can be examined and are very useful for reaching a definite diagnosis of XLH. Most orthopedists ask the expert pediatricians for investigations of bone metabolisms or genetics if they suspect rickets.
For patients with rickets in early childhood, medication treatment with phosphate and active vitamin D is first chosen. Therefore, orthopedic surgeons mainly check whether limb deformities, especially bowlegs, develop or not via plain radiography. If the deformity, mostly a varus deformity, is not improved or gets worse despite medication, the orthopedists should intervene in the management of the limb deformities. The orthopedic interventions include orthotic management and surgical treatment in this period. The effectiveness of orthoses such as a knee–ankle–foot orthosis (long leg brace) is not evident and is controversial. An orthopedic book describes no efficacy of orthotic management for vitamin-D-resistant rickets [22]. In particular, there has been no report of efficacious evidence in rickets of XLH. On the other hand, a few Japanese papers reported that orthotic treatment was efficacious in a small number of rachitic patients, including individuals with XLH [23]. Therefore, the application of orthoses is at each doctor’s discretion in Japan for severe bowlegs caused by various pathologies, such as XLH or vitamin D deficiency. The author has no experience of the application of orthoses to rickets patients because of improvements in deformities caused by medication.
Osteotomies are performed in patients with XLH who have a severe deformity or less improvement of deformities via medication [24]. Most osteotomies are applied to the femur and tibia or fibula (Figure 2). Deformities of these long bones exist both around growth plates, i.e., the metaphysis, epiphysis, and diaphysis, and many deformity sites can exist in one lower limb. Therefore, it is difficult and unrealistic to correct a deformed bone to a normally morphological shape. The purpose of osteotomies is the acquisition of a better appearance and better function of the lower limbs. However, the clinicians should keep in mind that better function takes precedence over a better appearance. In early childhood, osteotomies around the inflection point of each bone are performed to improve the mechanical axis to as normal of a range as possible. However, the correction of deformities by osteotomies in early childhood is related with high recurrence rates and complications [12,25,26]. Petje et al. reported a recurrence rate of 90% after the first corrective osteotomy under adequate administration of phosphate [12]. Therefore, it is difficult to decide the time of the first surgical procedure, and two- or three-stage procedures should be planned during growth.
2.2. Short Stature
One of the clinical symptoms in XLH is well known to be a growth impairment, especially short stature. Many pediatric orthopedists have encountered XLH patients with bowlegs and short stature. Several studies previously assessed the height in small populations of children with XLH [27,28], and Mao et al. recently reported growth curves for a relatively large population of children with XLH. They suggested that the height velocity decreased during the growth period compared to the normal population and that there was a notable decline in age- and sex-matched height Z-scores after walking age [29]. Short stature in XLH is proportional, although bowlegs are prominent. An orthopedic intervention is unnecessary and the treatment with phosphate and calcitriol should be selected for slow growth. Growth hormone therapy is also applied for short stature in XLH. Some papers have reported on the efficacious administration of recombinant human growth hormone, while others have suggested no significant benefits.
Burosumab, a recombinant human monoclonal antibody for FGF23, may be promising for the improvement of short stature in XLH patients [30].
3. Orthopedic Features and Treatments in Late Childhood and Adolescence
The physical and radiographic findings in late childhood and adolescence are similar to those in early childhood. However, the skeletal deformities are more various in these periods than in early childhood and patients are more likely to complain of their symptoms by themselves.
3.1. Lower Limb Deformity
Deformities around the knee joints are prominent in late childhood and adolescence, as are bowlegs in early childhood. However, those deformities are complicated in those generations, while varus deformities are more typical in early childhood. For example, some patients have varus or valgus deformities in bilateral knee joints and the others have a varus deformity in one lower limb and a valgus deformity in the other. The latter deformity is known as a windswept lower leg deformity [31]. The windswept deformity often leads to a leg length discrepancy (LLD) and dysfunction of the lower legs. The various abnormalities of the lower limb alignment cause various symptoms such as joint pain, bone pain, or joint laxity in the lower limbs as patients gain body weight via their skeletal growth and are subject to more weight-bearing stress on the lower extremities. Many researchers have suggested that severe residual deformities lead to degenerative changes in the joints of the lower limbs and impaired quality of life in adulthood [7,32,33,34].
Symptomatic deformities in the lower limbs should be treated as soon as possible and some asymptomatic deformities should also be treated via orthopedic procedures to prevent the patients from developing degenerative osteoarthritis of the lower limbs, spondylosis with functional scoliosis caused by LLD, and musculoskeletal pain in adulthood [35].
Most relatively mild cases with varus or valgus knee deformities are not corrected by osteotomies of the femur or the tibia in those periods but recently by temporary hemiepiphysiodesis using the guided growth method [15,36,37]. In guided growth surgery, a small plate is fixed on one side of a growth plate with two screws. These implants work as a tether system to the growth in one side of the epiphyseal plate and allow the lower limb alignment to improve with skeletal growth [38]. This method is less invasive, and the patients can relatively quickly return to their school life. However, severe deformities, which are not completely corrected by the guided growth method, are acutely or gradually corrected by osteotomies with internal implants (plate and screws) or external fixators. Gradual correction, which is based on distraction osteogenesis (the bone lengthening concept), can induce relatively accurate results and is a useful method. This surgical method is well established and usually applied to angular deformities or shortening of the tubular bones in various disorders. On the other hand, gradual correction puts a huge burden on the patients due to the long treatment period or many mild complications, such as pin site infections. In addition, one treatment precaution was pointed out in XLH patients receiving gradual correction [39]. Cho et al. reported the negative correlation between the regeneration of lengthened bone and serum phosphate levels and concluded that a serum phosphate level of 2.5 mg/dL as a cut-off point should be considered in deciding whether deformity correction alone or with concomitant leg lengthening should be undertaken [39]. The transition of MAD changes is monitored for the degree of improvement of lower limb deformities in both temporary hemiepiphysiodesis and correction by osteotomies. In addition, the orthopedic surgeons should consider the joint orientation angle (JOA) as an additional parameter during treatment planning. The JOA represents the angle between the mechanical axis and joint surface line of the knee or ankle [40]. A large deviation of the JOA from the normal range can cause an increase in shear stress on the joint cartilage and leads to early degenerative osteoarthritis. Therefore, lower limb deformities should be treated in adolescence, with an acceptable MAD and JOA achieved at skeletal maturity.
The guided growth method is also used for the correction of LLD in various diseases [41,42] and can be applicable to patients with XLH. A set of one plate and two screws is fixed on one side of a growth plate for the correction of angular deformities, whereas two sets are on fixed both sides of the growth plate in the longer lower limbs for the correction of LLD. On the other hand, bone lengthening of the shorter bones or shortening osteotomy of the longer bones is sometimes applied to patients with both angular deformities and LLD.
Rotational deformities of the lower limbs are also noticed as toe-in gait in late childhood and adolescence. Those rotational deformities in XLH include internal rotation of the lower leg (tibia and fibula) and external rotation of the femur. An internal rotational deformity of the tibia is more critical to toe-in gait [36]. Slight toe-in gait seldom causes symptoms and dysfunctions of lower limbs in everyday life. However, severe toe-in gait often gives rise to various symptoms such as joint pain of the knee or ankle, muscle and bone pain in the lateral lesions of the lower legs, or easier stumbling and spraining of the ankle, because the plane of motion of the knee joint is out of alignment with that of the ankle joint.
The correction of rotational deformities is less frequent than that of angular deformities and LLD, because there is not much impairment in daily life. However, the spontaneous correction of rotational deformities is less likely to occur compared to other deformities in late childhood and adolescence despite the use of conventional medication. An external rotational osteotomy is sometimes performed for the improvement of toe-in gait or pain of the joint and muscle.
These surgical procedures contribute to a reduction in burden and improvement of function in patients with XLH. However, the XLH patients are more predisposed to relapse of the corrected deformities or the development of adverse deformities, even in those periods, and these problems can provoke a further burden of treatment. The author also has experience with unexpected improvements of LLD and adverse deformities from guided growth surgery (Figure 3). The clinicians should make a cautious plan for treatment throughout the growth period and reduce the frequency of exposure to surgical procedures.
Recently, Mindler et al. reported persistent lower limb deformities in children with XLH receiving Burosumab for one year [5]. They concluded no positive effects of Burosumab on lower limb deformities. However, they suggested the limitation of a small study group and a short follow-up period and the necessity for further prospective studies with a large cohort and a longer follow-up. On the other hand, Insogna et al. showed the promotion of fracture healing by Burosumab treatment in adult patients [43]. This result suggests that Burosumab treatment might have an influence on osteotomy healing in patients with XLH. When the short-term and long-term effects of Burosumab on bones are clarified, this could modulate orthopedic treatments in XLH patients.
3.2. Fractures
A nontraumatic fracture is uncommon in children. Several groups have reported that the mean age at the first fracture was in the third decade [3,44]. The bone properties and morphology are important determinants of mechanical loading on the lower limbs. As the deterioration of these factors can lead to pathological fractures, they must be dealt with before skeletal maturity using medications and orthopedic interventions.
3.3. Scoliosis
Scoliosis, which is a condition involving a laterally curved deformity of the spinal column, can be caused by XLH in adolescence. Growth disturbances and a decrease in the bone properties of the vertebral bodies can lead to vertebral deformities, and these deformities can have a bad influence on the spinal alignment. A pediatric orthopedic book contains only one sentence stating that kyphoscoliosis is caused by rickets [12]. However, there are no papers on structural scoliosis, which is made up of vertebral bone deformities caused by XLH rickets in late childhood and adolescence. On the other hand, several groups have reported kyphoscoliosis in young adults with osteomalacia, who had experienced back pain and undergone spinal surgery [45,46]. Even though there is no evidence of a high incidence of scoliosis in XLH children, clinicians should pay attention to the presence of spinal deformities during the growth period considering the bone properties and the possibility of the deterioration of the spinal alignment after skeletal maturity in children with XLH. In addition, lower limb deformities, such as windswept lower limb deformities or large LLD, in childhood and adolescence cause functional scoliosis, which adjusts the trunk balance, and functional scoliosis can result in structural and degenerative scoliosis in adulthood [47,48]. Therefore, the spinal alignment should be carefully evaluated in patients with severe lower limb deformities in adolescence.
3.4. Musculoskeletal Pain
Several papers have indicated that the muscle density and strength are lower in patients with XLH than normal controls, while the muscle size is normal [49,50]. In addition, they reported that muscle functions are much lower in patients with severe leg deformities than those without deformities [51]. Low bone and muscle properties can lead to bone, joint, and muscle pain, which can impair physical functions. Furthermore, impairments of physical functions can cause muscle and bone weakness. Skrinar et al. demonstrated that many children with XLH had musculoskeletal pain as much as adult patients in spite of medication use [3]. Ito et al. also reported that Japanese and Korean children with XLH have pain in their lower limbs as adult patients [44]. These papers indicate that conventional therapies do not have enough effectiveness in terms of pain control of the musculoskeletal system. Recently, the efficacy of Burosumab has been reported in several papers, showing improvement in symptoms of rickets in children with XLH [30,51]. However, the efficacy of Burosumab for musculoskeletal pain is unclear. Further studies are expected in the near future.
4. Summary
This paper presented the orthopedic problems and interventions in children with XLH. The major issues in the orthopedic field are complicated lower limb deformities and their tendency to relapse. To resolve these problems, several surgical procedures are chosen for treatment and multiple surgeries are often performed until skeletal maturity (Figure 4). Therefore, orthopedic surgeons should make a cautious surgical plan for treatment throughout the growth period and reduce the burden of treatment in cooperation with pediatricians.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No data availability.
Conflicts of Interest
The author declares no conflict of interest.
References
- Read, A.P.; Thakker, R.V.; Davies, K.E.; Mountford, R.C.; Brenton, D.P.; Davies, M.; Glorieux, F.; Harris, R.; Hendy, G.N.; King, A.; et al. Mapping of human X-linked hypophosphatemic rickets by multilocus linkage analysis. Hum. Genet. 1986, 73, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Machler, M.; Frey, D.; Gai, A.; Orth, U.; Wienker, T.F.; Fanconi, A.; Schmid, W. X-linked dominant hypophosphatemia is closely linked to DNA markers DXS41 and DXS43 at Xp22. Hum. Genet. 1986, 73, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Skrinar, A.; Dvorak-Ewell, M.; Evins, A.; Macica, C.; Linglart, A.; Imel, E.A.; Theodore-Oklota, C.; Martin, J.S. The lifelong impact of X-linked hypophosphatemia: Results from a burden of disease survey. J. Endocr. Soc. 2019, 3, 1321–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mindler, G.T.; Kranzl, A.; Stauffer, A.; Haeusler, G.; Ganger, R.; Raimann, A. Disease-specific gait deviations in pediatric patients with X-linked hypophosphatemia. Gait Posture 2020, 81, 78–84. [Google Scholar] [CrossRef]
- Mindler, G.T.; Kranzl, A.; Stauffer, A.; Kocijan, R.; Ganger, R.; Radler, C.; Haeusler, G.; Raimann, A. Lower limb deformity and gait deviations among adolescents and adults with X-linked hypophosphatemia. Front. Endocrinol. 2021, 12, 754084. [Google Scholar] [CrossRef] [PubMed]
- Steele, A.; Gonzalez, R.; Garbalosa, J.C.; Steigbigel, K.; Grgurich, T.; Parisi, E.J.; Feinn, R.S.; Tommasini, S.M.; Macica, C.M. Osteoarthritis, osteophytes and enthesophytes affect biomechanical function in adults with X-linked hypophosphatemia. J. Clin. Endocrinol. Metab. 2020, 105, e1798–e1814. [Google Scholar] [CrossRef] [PubMed]
- Seefried, L.; Smyth, M.; Keen, R.; Harvengt, P. Burden of disease associated with X-linked hypophosphataemia in adults: A systematic literature review. Osteoporos. Int. 2021, 32, 7–22. [Google Scholar] [CrossRef] [PubMed]
- Petersen, D.J.; Boniface, A.M.; Schranck, F.W.; Rupich, R.C.; Whyte, M.P. X-linked hypophosphatemic rickets: A study (with literature review) of linear growth response to calcitriol and phosphate therapy. J. Bone Miner. Res. 1992, 7, 583–597. [Google Scholar] [CrossRef]
- Carpenter, T.O. New perspectives on the biology and treatment of X-linked hypophosphatemic rickets. Pediatr. Clin. N. Am. 1997, 44, 443–466. [Google Scholar] [CrossRef]
- Carpenter, T.O.; Imel, E.A.; Holm, I.A.; Jan de Beur, S.M.; Insogna, K.L. A clinician’s guide to X-linked hypophosphatemia. J. Bone Miner. Res. 2011, 26, 1381–1388. [Google Scholar] [CrossRef] [Green Version]
- Fucentese, S.F.; Neuhaus, T.J.; Ramseier, L.E.; Ulrich Exner, G. Metabolic and orthopedic management of X-linked vitamin D-resistant hypophosphatemic rickets. J. Child. Orthop. 2008, 2, 285–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petje, G.; Meizer, R.; Radler, C.; Aigner, N.; Grill, F. Deformity correction in children with hereditary hypophosphatemic rickets. Clin. Orthop. Relat. Res. 2008, 466, 3078–3085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, G.A.; Arulanantham, K.; Gage, J.R. Primary hypophosphatemic rickets: Effect of oral phosphate and vitamin D on growth and surgical treatment. J. Bone Jt. Surg. Am. 1980, 62, 1130–1138. [Google Scholar] [CrossRef]
- European Medicines Agency. New Medicine for Rarebone Disease. EMA 2017. Available online: https://www.ema.europa.eu/en/news/new-medicine-rare-bone-disease_en.pdf (accessed on 1 August 2022).
- US Food & Drug Administration. FDA Approves First Therapy for Rare Inherited Form of Rickets, X-Linked Hypophosphatemia. 2018. Available online: https://www.fda.gov/newsevents/newsroom/pressannouncements/ucm604810.htm (accessed on 1 August 2022).
- Pharmaceutical Affairs and Food Sanitation Council. 2020. Available online: https://www.hospital.or.jp/pdg/14_20200825_02.pdf (accessed on 1 August 2022).
- Stevens, P.M.; Maguire, M.; Dales, M.; Robins, A.J. Physeal stapling for idiopathic genu valgum. J. Pediatr. Orthop. 1999, 19, 645–649. [Google Scholar] [CrossRef]
- Horn, A.; Wright, J.; Bockenhauer, D.; Van’t Hoff, W.; Eastwood, D.M. The orthopaedic management of lower limb deformity in hypophosphataemic rickets. J. Child. Orthop. 2017, 11, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Thacher, T.D.; Fischer, P.R.; Pettifor, J.M.; Lawson, J.O.; Manaster, B.J.; Reading, J.C. Radiographic scoring method for the assessment of the severity of nutritional rickets. J. Trop. Pediatr. 2000, 46, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Whyte, M.P.; Fujita, K.P.; Moseley, S.; Thompson, D.D.; McAlister, W.H. Validation of a nevel scoring system for changes in skeletal manifestations of hypophosphatasia in newborns, infants, and children: The Radiographic Global Impression of Change Scale. J. Bone Miner. Res. 2018, 33, 868–874. [Google Scholar] [CrossRef] [Green Version]
- Lim, R.; Shailam, R.; Hulett, R.; Skrinar, A.; Nixon, A.; Williams, A.; Nixon, M.; Thacher, T.D. Validation of the Radiographic Global Impression of Change (RGI-C) score to assess healing of rickets in pediatric X-linked hypophosphatemia (XLH). Bone 2021, 148, 115964. [Google Scholar] [CrossRef]
- Kim, H.K.W.; Seikaly, M.G. Metabolic and Endcrine Disorders of Bone. In Tachdjian’s Pediatric Orthopaedics, 6th ed.; Herring, J.A., Ed.; Elsevier: Philadelphia, PA, USA, 2020; Volume 2, pp. 1928–1938. [Google Scholar]
- Eguchi, Y.; Seki, A.; Uchikawa, S.; Tori, A.; Kimura, A.; Takayama, S. Kashisouguryouhou wo okonatta teirinnkesshousei-kurubyo (hypophosphatemic rickets) kannjinokeika. Nippon Shouniseikeigeka Gakkai Shi 2017, 26, 14–18. [Google Scholar]
- Sharkey, M.S.; Grunseich, K.; Carpenter, T.O. Contemporary medical and surgical management of X-linked hypophosphatemic rickets. J. Am. Acad. Orthop. Surg. 2015, 23, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Rohmiller, M.T.; Tylkowski, C.; Kriss, V.M.; Mier, R.J. The effect of osteotomy on bowing and height in children with X-linked hypophosphatemia. J. Pediatr. Orthop. 1999, 9, 114–118. [Google Scholar] [CrossRef]
- Nielsen, L.H.; Rahbek, E.T.; Beck-Nielsen, S.S.; Christesen, H.T. Treatment of hypophosphataemic rickets in children remains a challenge. Dan Med. J. 2014, 61, A4874. [Google Scholar] [PubMed]
- Cagnoli, M.; Richter, R.; Bohm, P.; Knye, K.; Empting, S.; Mohnike, K. Spontaneous growth and effect of early therapy with calcitriol and phosphate in X-linked hypophosphatemic rickets. Pediatr. Endocrinol. Rev. 2017, 15 (Suppl. S1), 119–122. [Google Scholar] [PubMed]
- Makitie, O.; Doria, A.; Kooh, S.W.; Cole, W.G.; Daneman, A.; Sochett, E. Early treatment improves growth and biochemical and radiographic outcome in X-linked hypophosphatemic rickets. J. Clin. Endocrinol. Metab. 2003, 88, 3591–3597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, M.; Carpenter, T.O.; Whyte, M.P.; Skrinar, A.; Chen, C.Y.; Martin, J.S.; Rogol, A.D. Growth curve for children with X-linked hypophosphatemia. J. Clin. Endocrinol. Metab. 2020, 105, 3243–3249. [Google Scholar] [CrossRef]
- Ward, L.M.; Glorieux, F.H.; Whyte, M.P.; Munns, C.F.; Portale, A.A.; Högler, W.; Simmons, J.H.; Gottesman, G.S.; Padidela, R.; Namba, N.; et al. Impact of Burosumab Compared with Conventional Therapy in Younger Versus Older Children with X-Linked Hypophosphatemia. J. Clin. Endocrinol. Metab. 2022, 107, e3241–e3253.dgac296. [Google Scholar] [CrossRef]
- Smyth, E.H. Windswept deformity. J. Bone Jt. Surg. Br. 1980, 62, 166–167. [Google Scholar] [CrossRef]
- Che, H.; Roux, C.; Etcheto, A.; Rothenbuhler, A.; Kamanicky, P.; Linglart, A.; Briot, K. Impaired quality of life in adults with X-linked hypophosphatemia and skeletal symptoms. Eur. J. Endocrinol. 2016, 174, 325–333. [Google Scholar] [CrossRef] [Green Version]
- Cheung, M.; Rylands, A.J.; Williams, A.; Bailey, K.; Bubbear, J. Patient-reported complications, symptoms, and experiences of living with X-linked hypophosphatemia across the life-course. J. Endocr. Soc. 2021, 5, bvab070. [Google Scholar] [CrossRef] [PubMed]
- Lecoq, A.-L.; Brandi, M.L.; Linglart, A.; Kamenicky, P. Management of X-linked hypophosphatemia in adults. Metabolism 2020, 103S, 154049. [Google Scholar] [CrossRef]
- Larson, A.N.; Trousdale, R.T.; Pagnano, M.W.; Hanssen, A.D.; Lewallen, D.G.; Sanchez-Sotelo, J. Hip and knee arthroplasty in hypophosphatemic rickets. J. Arthroplast. 2010, 25, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- Mindler, G.T.; Stauffer, A.; Kranzl, A.; Penzkofer, S.; Ganger, R.; Radler, C.; Haeusler, G.; Raimann, A. Persistent lower limb deformities despite amelioration of rickets in X-linked hypophosphatemia (XLH)—A prospective observation study. Front. Endocrinol. 2022, 13, 866170. [Google Scholar] [CrossRef] [PubMed]
- Novais, E.; Stevens, P.M. Hypophosphatemic rickets: The role of hemiepiphysiodesis. J. Pediatr. Orthop. 2006, 26, 238–244. [Google Scholar] [CrossRef]
- Stevens, P.M. Guided growth for angular correction: A preliminary series using a tension band plate. J. Pediatr. Orthop. 2007, 27, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.H.; Kim, J.K.; Chung, C.Y.; Cho, T.-J.; Lee, S.H.; Suh, S.W.; Whang, K.S.; Park, H.W.; Song, K.S. Deformity correction of knee and leg lengthening by Ilizarov method in hypophosphatemic rickets: Outcomes and significance of serum phosphate level. J. Pediatr. Orthop. 2002, 22, 626–631. [Google Scholar] [CrossRef]
- Paley, D.; Herzenberg, J.E.; Tetsworth, K.; McKie, J.; Bhave, A. Deformity planning for frontal and sagittal plane corrective osteotomies. Orthop. Clin. N. Am. 1994, 25, 425–465. [Google Scholar] [CrossRef]
- Lykissas, M.G.; Jain, V.V.; Manickam, V.; Nathan, S.; Eismann, E.A.; McCarthy, J.J. Guided growth for the treatment of limb length discrepancy: A comparative study of the three most commonly used surgical techniques. J. Pediat. Orthop. B 2013, 22, 311–317. [Google Scholar] [CrossRef]
- Byyham, I.A.; Karatas, A.F.; Rogers, K.J.; Bowen, J.R.; Thacker, M.M. Comparing percutaneous physeal epiphysiodesis and Eight-Plate epiphysiodesis for the treatment of limb length discrepancy. J. Pediatr. Orthop. 2015, 37, 323–327. [Google Scholar]
- Insogna, K.; Briot, K.; Imel, E.A.; Kamenicky, P.; Ruppe, M.D.; Portale, A.A.; Weber, T.; Pitukcheewanont, P.; Cheong, H.I.I.; Jan de Beur, S.; et al. A randomized, double-blind, placebo-controlled, phase 3 trial evaluating the efficacy of Burosumab, an anti-FGF23 antibody, in adults with X-linked hypophosphatemia: Week 24 primary analysis. J. Bone Miner. Res. 2018, 33, 1383–1393. [Google Scholar] [CrossRef] [Green Version]
- Ito, N.; Kang, H.G.; Nishida, Y.; Evins, A.; Skrinar, A.; Cheong, H.I. Burden of disease of X-linked hypophosphatemia in Japanese and Korean patients: A cross-sectional survey. Endocr. J. 2022, 69, 373–383. [Google Scholar] [CrossRef]
- Motosuneya, T.; Asazuma, T.; Yasuoka, H.; Tsuji, T.; Fujikawa, K. Severe kyphoscoliosis associated with osteomalacia. Spine J. 2006, 6, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Hensinger, R.N. Kyphosis secondary to skeletal dysplasias and metabolic disease. Clin. Orthop. Relat. Res. 1977, 128, 113–128. [Google Scholar] [CrossRef]
- Brunk, M. The importance of rickets in childhood as a cause of scoliosis in adult age. Acta Orthop. Scand. 1951, 9, 3–114. [Google Scholar] [CrossRef]
- Yang, X.; Zou, Q.; Song, Y.; Liu, L.; Zhou, C. A case report of severe degenerative lumbar scoliosis associated with windswept lower limb deformity. BMC Surg. 2020, 20, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Veilleux, L.-N.; Cheung, M.; Ben Amor, M.; Rauch, F. Abnormalities in muscle density and muscle function in hypophosphatemic rickets. J. Clin. Endocrinol. Metab. 2012, 97, E1492–E1498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veilleux, L.N.; Cheung, M.S.; Glorieux, F.H.; Rauch, F. The muscle-bone relationship in X-linked hypophosphatemic rickets. J. Clin. Endocrinol. Metab. 2013, 98, E990–E995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namba, N.; Kubota, T.; Muroya, K.; Tanaka, H.; Kanematsu, M.; Kojima, M.; Orihara, S.; Kanda, H.; Seino, Y.; Ozono, K. Safety and Efficacy of Burosumab in Pediatric Patients With X-Linked Hypophosphatemia: A Phase 3/4 Open-Label Trial. J. Endocr. Soc. 2022, 6, bvac021. [Google Scholar] [CrossRef]
Figure 1.
Mechanical axis deviation (MAD) and varus or valgus deformity of a lower limb. The mechanical axis is defined as the line between the center of the femoral head and the center of the ankle joint (white line). Mechanical axis deviation is defined as the displacement of the mechanical axis from the center of the knee joint. (a) Valgus deformity of the lower limb exists because of the lateral displacement of the MAD. (b) Varus deformity of the lower limb exists because of the medial displacement of the MAD.
Figure 1.
Mechanical axis deviation (MAD) and varus or valgus deformity of a lower limb. The mechanical axis is defined as the line between the center of the femoral head and the center of the ankle joint (white line). Mechanical axis deviation is defined as the displacement of the mechanical axis from the center of the knee joint. (a) Valgus deformity of the lower limb exists because of the lateral displacement of the MAD. (b) Varus deformity of the lower limb exists because of the medial displacement of the MAD.

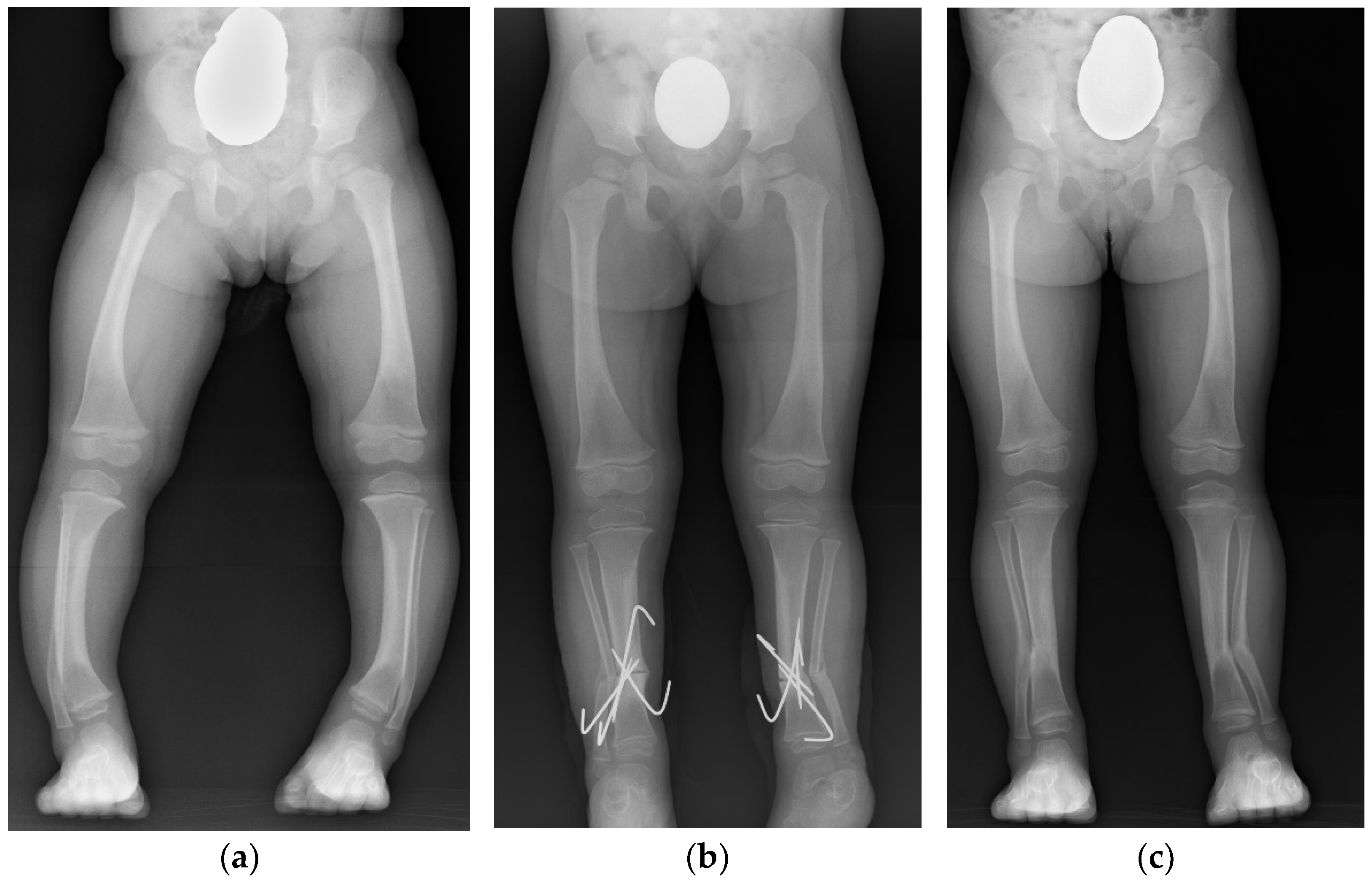
Figure 2.
A case of correction osteotomy: (a) varus deformities of bilateral lower legs before correction osteotomy; (b) corrected lower legs after bilateral osteotomy with wire fixation; (c) correction of MAD after bone healing at osteotomy site.
Figure 2.
A case of correction osteotomy: (a) varus deformities of bilateral lower legs before correction osteotomy; (b) corrected lower legs after bilateral osteotomy with wire fixation; (c) correction of MAD after bone healing at osteotomy site.

Figure 3.
A case with varied deformities. White lines are the mechanical axis. (a) Preoperative; valgus deformity of the right lower limb and leg length discrepancy (LLD) (b) 1 year after guided growth surgery; valgus deformity and LLD was improving. (c) After deformity correction; only one side of guided growth surgery led to correction of both valgus knee deformity and leg length discrepancy (d) 1 year after implant removal; varus deformity of the corrected right lower limb emerged.
Figure 3.
A case with varied deformities. White lines are the mechanical axis. (a) Preoperative; valgus deformity of the right lower limb and leg length discrepancy (LLD) (b) 1 year after guided growth surgery; valgus deformity and LLD was improving. (c) After deformity correction; only one side of guided growth surgery led to correction of both valgus knee deformity and leg length discrepancy (d) 1 year after implant removal; varus deformity of the corrected right lower limb emerged.

Figure 4.
Brief algorithm of the surgical indication and method for varus or valgus deformities and leg length discrepancies, which are corrected by the guided growth method in early childhood and by osteotomy in adolescence. Rotational deformities are corrected by osteotomy in all patients.
Figure 4.
Brief algorithm of the surgical indication and method for varus or valgus deformities and leg length discrepancies, which are corrected by the guided growth method in early childhood and by osteotomy in adolescence. Rotational deformities are corrected by osteotomy in all patients.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Higuchi, C. Orthopedic Complications and Management in Children with X-Linked Hypophosphatemia. Endocrines 2022, 3, 488-497. https://doi.org/10.3390/endocrines3030039
AMA Style
Higuchi C. Orthopedic Complications and Management in Children with X-Linked Hypophosphatemia. Endocrines. 2022; 3(3):488-497. https://doi.org/10.3390/endocrines3030039
Chicago/Turabian StyleHiguchi, Chikahisa. 2022. "Orthopedic Complications and Management in Children with X-Linked Hypophosphatemia" Endocrines 3, no. 3: 488-497. https://doi.org/10.3390/endocrines3030039