
Temporal Responses of a Low-Energy Meal Replacement Plan or Exercise Training on Cardiovascular Function and Fibro-Inflammatory Markers in People with Type 2 Diabetes—A Secondary Analysis of the “Diabetes Interventional Assessment of Slimming or Training to Lessen Inconspicuous Cardiovascular Dysfunction” Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
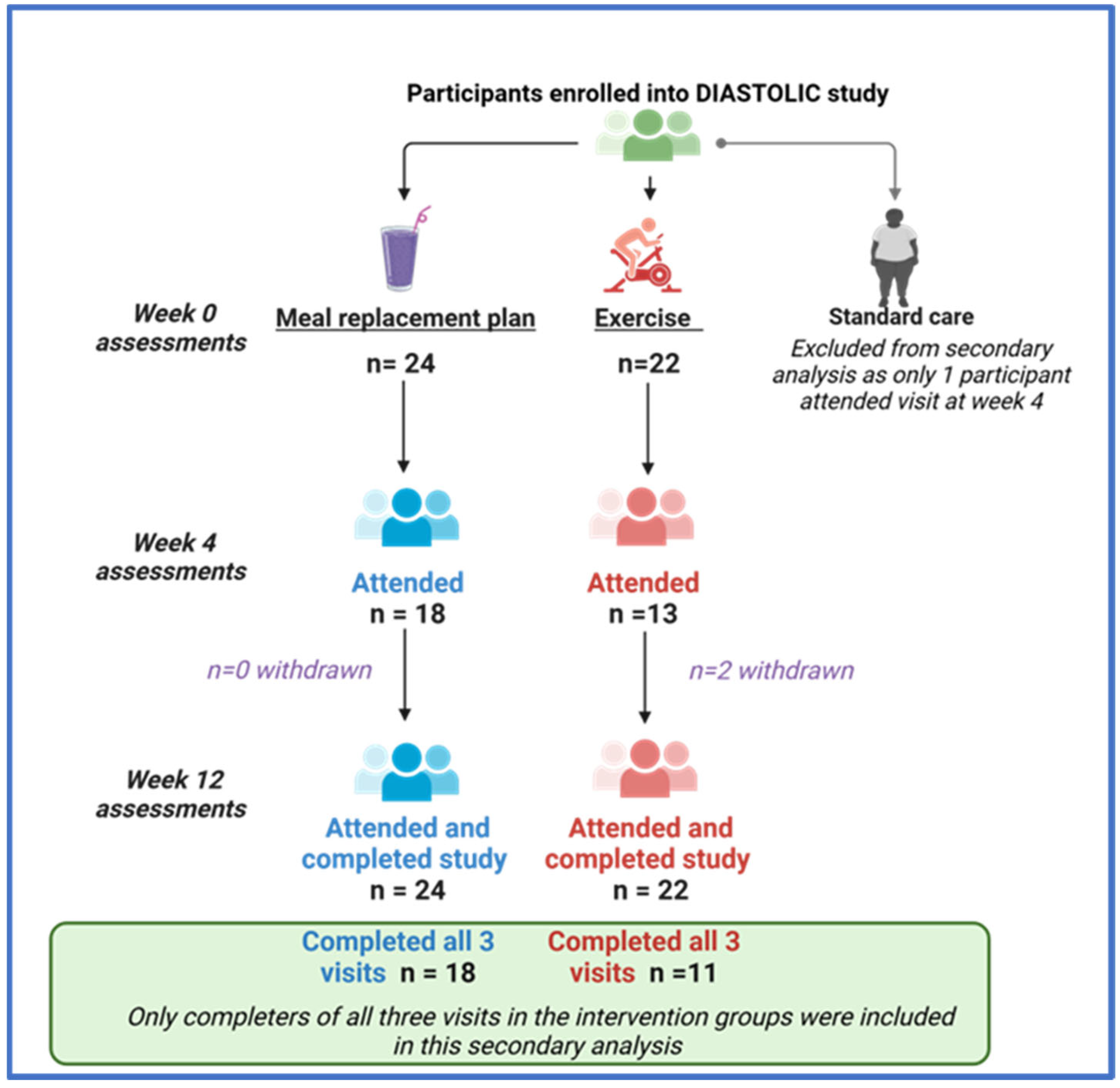
2.1. Study Population
2.2. Anthropometry
2.3. Biochemistry
2.4. CMR Image Acquisition and Analysis
2.5. Trial Interventions
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. The Temporal Changes in the Effects of MRP and Exercise between 0 to 4 and 4 to 12 Weeks
3.2.1. Body Weight
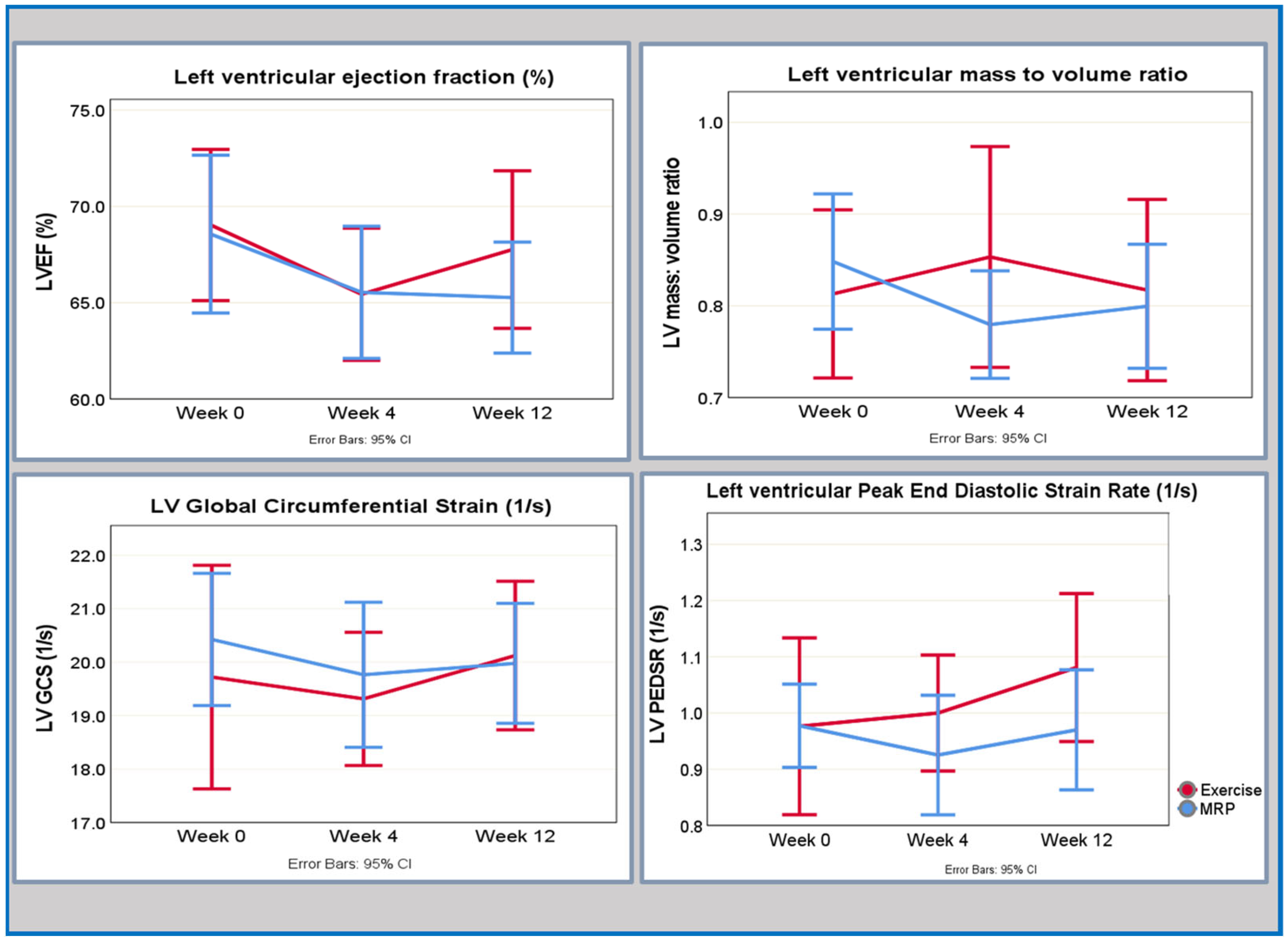
3.2.2. Cardiovascular Structure and Function
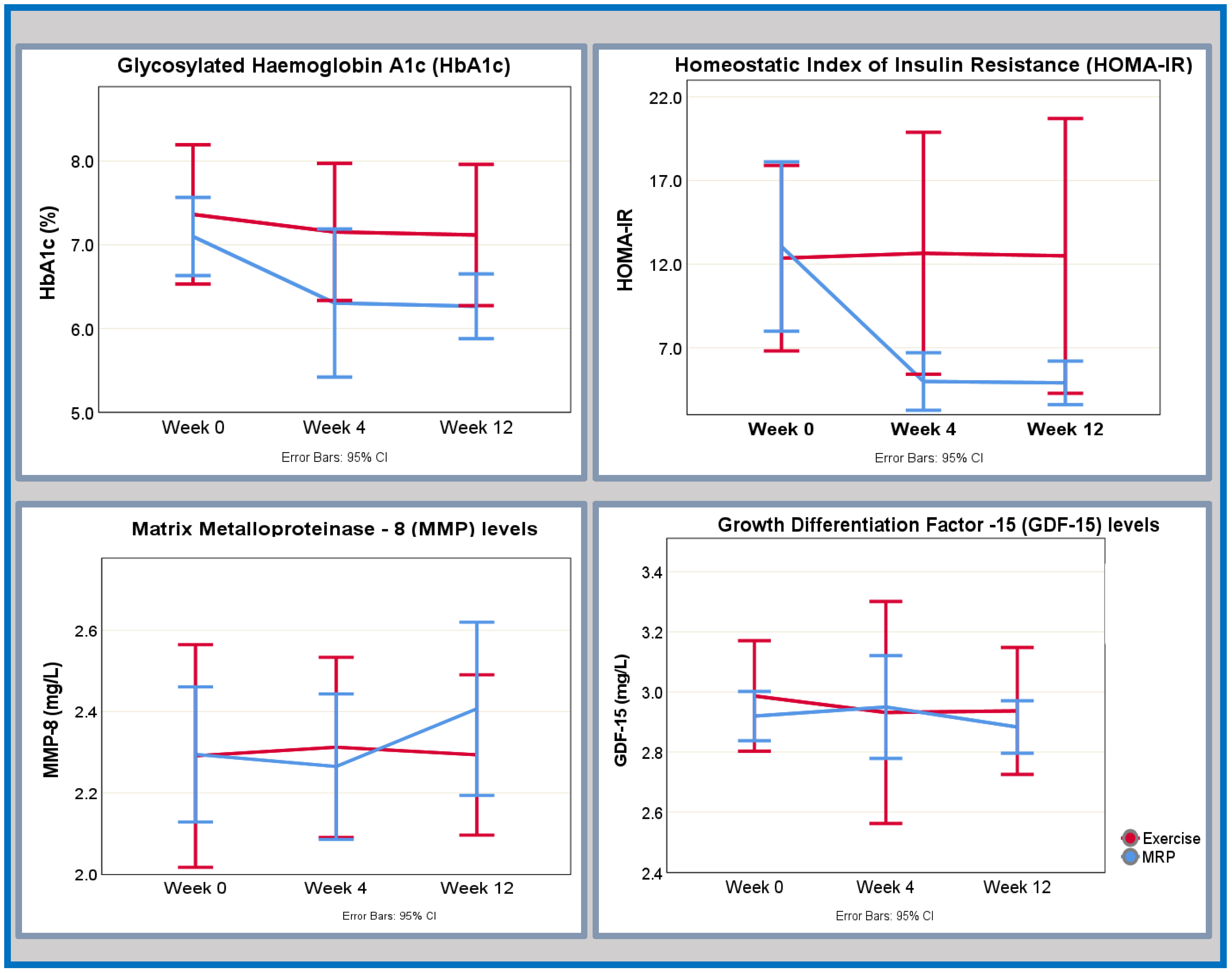
3.2.3. Glycometabolic Profile
3.2.4. Fibroinflammatory Biomarkers
4. Discussion
4.1. Changes in Left Ventricular Systolic and Diastolic Function
4.2. Changes in Cardiac Remodelling and the Role of Inflammation and Cardiac Autophagy
4.3. Changes in the Glycometabolic Profile and the Fibroinflammatory Markers
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
| MRP | Exercise | |||
|---|---|---|---|---|
| Excluded n = 6 | Included n = 18 | Excluded n = 11 | Included n = 11 | |
| Age, years | 48.2 ± 8.35 | 52.1 ± 4.39 | 51.2 ± 3.87 | 49.1 ± 9.73 |
| Male sex, n (%) | 3.00 (50.0) | 12.0 (66.7) | 7.00 (68.6) | 6.00 (54.5) |
| White ethnic background, n (%) | 6.00 (100) | 13.0 (72.2) | 11.00 (100) | 9.00 (81) |
| Hypertension, n (%) | 3.00 (50) | 12.0 (66.7) | 5.00 (45.4) | 4.00 (36.4) |
| Hypercholesterolemia, n (%) | 4.00 (66.7) | 12.0 (66.7) | 9.00 (81.8) | 5.00 (45.4) |
| Systolic BP, mmHg | 146 ± 16 | 151 ± 13.3 | 136 ± 18.7 | 136 ± 18.7 |
| Height, cm | 169 ± 9.80 | 169 ± 9.50 | 169 ± 9.81 | 169 ± 7.50 |
| Weight, kg | 104 ± 23.2 | 105 ± 13.5 | 98.7 ± 7.77 | 99.6 ± 22.3 |
| BMI, kg/m2 | 39.3 ± 8.33 | 36.7 ± 4.91 | 34.7 ± 5.12 | 34.8 ± 6.70 |
| HbA1c, % | 7.36 ± 1.54 | 7.10 ± 0.94 | 7.50 ± 1.02 | 7.34 ± 1.23 |
| Medication received, n (%) | ||||
| Insulin | 0 | 0 | 0 | 0 |
| Metformin | 6 (100) | 16 (88.8) | 11 (100) | 11 (100) |
| GLP-1 antagonist | 0 | 1 (5.56) | 3 (27.3) | 1 (9.09) |
| SGLT-2 inhibitor | 0 | 2 (11.1) | 2 (18.2) | 1 (9.09) |
| ACE inhibitor | 2 (33.3) | 7 (38.8) | 3 (27.3) | 3 (27.3) |
| Alpha blocker | 0 | 1 (5.56) | 1 (9.09) | 0 |
| ARB | 1 (16.6) | 2 (11.1) | 0 | 1 (9.09) |
| B-blockers | 0 | 2 (11.1) | 0 | 2 (18.2) |
| CCB | 3 (50) | 4 (22.2) | 3 (27.3) | 2 (18.2) |
| Statin | 4 (66.7) | 11 (611) | 9 (81.8) | 5 (45.4) |
| Fibrate | 1 (16.6) | 0 | 0 | 0 |
References
- Borlaug, B.A. The pathophysiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2014, 11, 507–515. [Google Scholar] [CrossRef]
- Shah, S.J.; Kitzman, D.W.; Borlaug, B.A.; van Heerebeek, L.; Zile, M.R.; Kass, D.A.; Paulus, W.J. Phenotype-Specific Treatment of Heart Failure with Preserved Ejection Fraction: A Multiorgan Roadmap. Circulation 2016, 134, 73–90. [Google Scholar] [CrossRef]
- Gregor, M.F.; Hotamisligil, G.S. Inflammatory Mechanisms in Obesity. Annu. Rev. Immunol. 2011, 29, 415–445. [Google Scholar] [CrossRef]
- Neeland, I.J.; Gupta, S.; Ayers, C.R.; Turer, A.T.; Rame, J.E.; Das, S.R.; Berry, J.D.; Khera, A.; McGuire, D.K.; Vega, G.L.; et al. Relation of regional fat distribution to left ventricular structure and function. Circ. Cardiovasc. Imaging. 2013, 6, 800–807. [Google Scholar] [CrossRef]
- Neeland, I.J.; Ross, R.; Després, J.P.; Matsuzawa, Y.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: A position statement. Lancet Diabetes Endocrinol. 2019, 7, 715–725. [Google Scholar] [CrossRef]
- Franssen, C.; Chen, S.; Unger, A.; Korkmaz, H.I.; De Keulenaer, G.W.; Tschope, C.; Leite-Moreira, A.F.; Musters, R.; Niessen, H.W.; Linke, W.A.; et al. Myocardial Microvascular Inflammatory Endothelial Activation in Heart Failure with Preserved Ejection Fraction. JACC Heart Fail. 2016, 4, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Paulus, W.J.; Tschope, C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J. Am. Coll. Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Paolillo, S.; Marsico, F.; Prastaro, M.; Renga, F.; Esposito, L.; De Martino, F.; Di Napoli, P.; Esposito, I.; Ambrosio, A.; Ianniruberto, M.; et al. Diabetic Cardiomyopathy: Definition, Diagnosis, and Therapeutic Implications. Heart Fail. Clin. 2019, 15, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Viljanen, A.P.; Karmi, A.; Borra, R.; Pärkkä, J.P.; Lepomäki, V.; Parkkola, R.; Lautamäki, R.; Järvisalo, M.; Taittonen, M.; Rönnemaa, T.; et al. Effect of caloric restriction on myocardial fatty acid uptake, left ventricular mass, and cardiac work in obese adults. Am. J. Cardiol. 2009, 103, 1721–1726. [Google Scholar] [CrossRef]
- Jonker, J.T.; Snel, M.; Hammer, S.; Jazet, I.M.; van der Meer, R.W.; Pijl, H.; Meinders, A.E.; de Roos, A.; Smit, J.W.; Romijn, J.A.; et al. Sustained cardiac remodeling after a short-term very low calorie diet in type 2 diabetes mellitus patients. Int. J. Cardiovasc. Imaging 2014, 30, 121–127. [Google Scholar] [CrossRef]
- Jonker, J.T.; Djaberi, R.; van Schinkel, L.D.; Hammer, S.; Bus, M.T.J.; Kerpershoek, G.; Kharagjitsingh, A.V.; Romijn, J.A.; Bax, J.J.; Jukema, J.W.; et al. Very-Low-Calorie Diet Increases Myocardial Triglyceride Content and Decreases Diastolic Left Ventricular Function in Type 2 Diabetes with Cardiac Complications. Diabetes Care. 2013, 37, e1–e2. [Google Scholar] [CrossRef]
- van der Meer, R.W.; Hammer, S.; Smit, J.W.A.; Frölich, M.; Bax, J.J.; Diamant, M.; Rijzewijk, L.J.; de Roos, A.; Romijn, J.A.; Lamb, H.J. Short-Term Caloric Restriction Induces Accumulation of Myocardial Triglycerides and Decreases Left Ventricular Diastolic Function in Healthy Subjects. Diabetes 2007, 56, 2849–2853. [Google Scholar] [CrossRef]
- Rayner, J.J.; Abdesselam, I.; Peterzan, M.A.; Akoumianakis, I.; Akawi, N.; Antoniades, C.; Tomlinson, J.W.; Neubauer, S.; Rider, O.J. Very low calorie diets are associated with transient ventricular impairment before reversal of diastolic dysfunction in obesity. Int. J. Obes. 2019, 43, 2536–2544. [Google Scholar] [CrossRef]
- Hammer, S.; Snel, M.; Lamb, H.J.; Jazet, I.M.; van der Meer, R.W.; Pijl, H.; Meinders, E.A.; Romijn, J.A.; de Roos, A.; Smit, J.W. Prolonged caloric restriction in obese patients with type 2 diabetes mellitus decreases myocardial triglyceride content and improves myocardial function. J. Am. Coll. Cardiol. 2008, 52, 1006–1012. [Google Scholar] [CrossRef]
- Rehackova, L.; Rodrigues, A.M.; Thom, G.; Brosnahan, N.; Barnes, A.C.; McCombie, L.; Leslie, W.S.; Zhyzhneuskaya, S.; Peters, C.; Adamson, A.J.; et al. Participant experiences in the Diabetes REmission Clinical Trial (DiRECT). Diabet. Med. 2022, 39, e14689. [Google Scholar] [CrossRef]
- Leslie, W.S.; Ali, E.; Harris, L.; Messow, C.M.; Brosnahan, N.T.; Thom, G.; McCombie, E.L.; Barnes, A.C.; Sattar, N.; Taylor, R.; et al. Antihypertensive medication needs and blood pressure control with weight loss in the Diabetes Remission Clinical Trial (DiRECT). Diabetologia 2021, 64, 1927–1938. [Google Scholar] [CrossRef]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Kosiborod, M.N.; Abildstrøm, S.Z.; Borlaug, B.A.; Butler, J.; Rasmussen, S.; Davies, M.; Hovingh, G.K.; Kitzman, D.W.; Lindegaard, M.L.; Møller, D.V.; et al. Semaglutide in Patients with Heart Failure with Preserved Ejection Fraction and Obesity. N. Engl. J. Med. 2023, 389, 1069–1084. [Google Scholar] [CrossRef] [PubMed]
- Gulsin, G.S.; Brady, E.M.; Swarbrick, D.J.; Athithan, L.; Henson, J.; Baldry, E.; McAdam, J.; Marsh, A.M.; Parke, K.S.; Wormleighton, J.V.; et al. Rationale, design and study protocol of the randomised controlled trial: Diabetes Interventional Assessment of Slimming or Training tO Lessen Inconspicuous Cardiovascular Dysfunction (the DIASTOLIC study). BMJ Open 2019, 9, e023207. [Google Scholar] [CrossRef] [PubMed]
- Gulsin, G.S.; Swarbrick, D.J.; Athithan, L.; Brady, E.M.; Henson, J.; Baldry, E.; Argyridou, S.; Jaicim, N.B.; Squire, G.; Walters, Y.; et al. Effects of Low-Energy Diet or Exercise on Cardiovascular Function in Working-Age Adults with Type 2 Diabetes: A Prospective, Randomized, Open-Label, Blinded End Point Trial. Diabetes Care 2020, 43, 1300–1310. [Google Scholar] [CrossRef] [PubMed]
- Brady, E.M.; Gulsin, G.S.; Mirkes, E.M.; Parke, K.; Kanagala, P.; Ng, L.L.; Graham-Brown, M.P.M.; Athithan, L.; Henson, J.; Redman, E.; et al. Fibro-inflammatory recovery and type 2 diabetes remission following a low calorie diet but not exercise training: A secondary analysis of the DIASTOLIC randomised controlled trial. Diabet. Med. 2022, 39, e14884. [Google Scholar] [CrossRef]
- Placzkowska, S.; Pawlik-Sobecka, L.; Kokot, I.; Piwowar, A. Indirect insulin resistance detection: Current clinical trends and laboratory limitations. Biomed. Pap. Med. 2019, 163, 187–199. [Google Scholar] [CrossRef]
- Gulsin, G.S.; Swarbrick, D.J.; Hunt, W.H.; Levelt, E.; Graham-Brown, M.P.M.; Parke, K.S.; Wormleighton, J.V.; Lai, F.Y.; Yates, T.; Wilmot, E.G.; et al. Relation of Aortic Stiffness to Left Ventricular Remodeling in Younger Adults with Type 2 Diabetes. Diabetes 2018, 67, 1395–1400. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Med. 2021, 31, 010502. [Google Scholar] [CrossRef] [PubMed]
- DeVore, A.D.; McNulty, S.; Alenezi, F.; Ersboll, M.; Vader, J.M.; Oh, J.K.; Lin, G.; Redfield, M.M.; Lewis, G.; Semigran, M.J.; et al. Impaired left ventricular global longitudinal strain in patients with heart failure with preserved ejection fraction: Insights from the RELAX trial. Eur. J. Heart Fail. 2017, 19, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Rui, L. Energy metabolism in the liver. Compr. Physiol. 2014, 4, 177–197. [Google Scholar] [PubMed]
- Kerr, M.; Dodd, M.S.; Heather, L.C. The ‘Goldilocks zone’ of fatty acid metabolism; to ensure that the relationship with cardiac function is just right. Clin. Sci. 2017, 131, 2079–2094. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Parashar, A.; Kumbhani, D.; Agarwal, S.; Garg, J.; Kitzman, D.; Levine, B.; Drazner, M.; Berry, J. Exercise training in patients with heart failure and preserved ejection fraction: Meta-analysis of randomized control trials. Circ. Heart Fail. 2015, 8, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Gulsin, G.S.; Henson, J.; Brady, E.M.; Sargeant, J.A.; Wilmot, E.G.; Athithan, L.; Htike, Z.Z.; Marsh, A.M.; Biglands, J.D.; Kellman, P.; et al. Cardiovascular Determinants of Aerobic Exercise Capacity in Adults with Type 2 Diabetes. Diabetes Care 2020, 43, 2248–2256. [Google Scholar] [CrossRef]
- Kamareddine, L.; Ghantous, C.M.; Allouch, S.; Al-Ashmar, S.A.; Anlar, G.; Kannan, S.; Djouhri, L.; Korashy, H.M.; Agouni, A.; Zeidan, A. Between Inflammation and Autophagy: The Role of Leptin-Adiponectin Axis in Cardiac Remodeling. J. Inflamm. Res. 2021, 14, 5349–5365. [Google Scholar] [CrossRef]
- Nishida, K.; Kyoi, S.; Yamaguchi, O.; Sadoshima, J.; Otsu, K. The role of autophagy in the heart. Cell Death Differ. 2009, 16, 31–38. [Google Scholar] [CrossRef]
- Kanamori, H.; Takemura, G.; Goto, K.; Tsujimoto, A.; Mikami, A.; Ogino, A.; Watanabe, T.; Morishita, K.; Okada, H.; Kawasaki, M.; et al. Autophagic adaptations in diabetic cardiomyopathy differ between type 1 and type 2 diabetes. Autophagy 2015, 11, 1146–1160. [Google Scholar] [CrossRef]
- Takemura, G.; Kanamori, H.; Goto, K.; Maruyama, R.; Tsujimoto, A.; Fujiwara, H.; Seishima, M.; Minatoguchi, S. Autophagy maintains cardiac function in the starved adult. Autophagy 2009, 5, 1034–1036. [Google Scholar] [CrossRef]
- Ghantous, C.M.; Kobeissy, F.H.; Soudani, N.; Rahman, F.A.; Al-Hariri, M.; Itani, H.A.; Sabra, R.; Zeidan, A. Mechanical stretch-induced vascular hypertrophy occurs through modulation of leptin synthesis-mediated ROS formation and GATA-4 nuclear translocation. Front. Pharmacol. 2015, 6, 240. [Google Scholar] [CrossRef]
- Guo, R.; Zhang, Y.; Turdi, S.; Ren, J. Adiponectin knockout accentuates high fat diet-induced obesity and cardiac dysfunction: Role of autophagy. Biochim. Biophys. Acta 2013, 1832, 1136–1148. [Google Scholar] [CrossRef]
- Jahng, J.W.; Turdi, S.; Kovacevic, V.; Dadson, K.; Li, R.K.; Sweeney, G. Pressure Overload-Induced Cardiac Dysfunction in Aged Male Adiponectin Knockout Mice Is Associated with Autophagy Deficiency. Endocrinology 2015, 156, 2667–2677. [Google Scholar] [CrossRef] [PubMed]
- Gogiraju, R.; Hubert, A.; Fahrer, J.; Straub, B.K.; Brandt, M.; Wenzel, P.; Münzel, T.; Konstantinides, S.; Hasenfuss, G.; Schäfer, K. Endothelial Leptin Receptor Deletion Promotes Cardiac Autophagy and Angiogenesis Following Pressure Overload by Suppressing Akt/mTOR Signaling. Circ. Heart Fail. 2019, 12, e005622. [Google Scholar] [CrossRef] [PubMed]
- Sari, İ.; Habipoğlu, S.; Seydel, G.; Erşan, S.; Güntürk, İ. The effect of acute step-aerobic exercise on adiponectin and leptin levels in premenopausal women. J. Sports Med. Phys. Fitness 2021, 61, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Koepp, K.E.; Obokata, M.; Reddy, Y.N.V.; Olson, T.P.; Borlaug, B.A. Hemodynamic and Functional Impact of Epicardial Adipose Tissue in Heart Failure with Preserved Ejection Fraction. JACC Heart Fail. 2020, 8, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.B.; Shah, S.; Verma, S.; Oudit, G.Y. Epicardial adipose tissue as a metabolic transducer: Role in heart failure and coronary artery disease. Heart Fail. Rev. 2017, 22, 889–902. [Google Scholar] [CrossRef] [PubMed]
- Kitzman, D.W.; Brubaker, P.; Morgan, T.; Haykowsky, M.; Hundley, G.; Kraus, W.E.; Eggebeen, J.; Nicklas, B.J. Effect of Caloric Restriction or Aerobic Exercise Training on Peak Oxygen Consumption and Quality of Life in Obese Older Patients with Heart Failure with Preserved Ejection Fraction: A Randomized Clinical Trial. JAMA 2016, 315, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Day, E.A.; Townsend, L.K.; Djordjevic, D.; Jørgensen, S.B.; Steinberg, G.R. GDF15: Emerging biology and therapeutic applications for obesity and cardiometabolic disease. Nat. Rev. Endocrinol. 2021, 17, 592–607. [Google Scholar] [CrossRef]
- Tsioufis, C.; Bafakis, I.; Kasiakogias, A.; Stefanadis, C. The role of matrix metalloproteinases in diabetes mellitus. Curr. Top. Med. Chem. 2012, 12, 1159–1165. [Google Scholar] [CrossRef] [PubMed]
- Dahlström, E.H.; Saksi, J.; Forsblom, C.; Uglebjerg, N.; Mars, N.; Thorn, L.M.; Harjutsalo, V.; Rossing, P.; Ahluwalia, T.S.; Lindsberg, P.J.; et al. The Low-Expression Variant of FABP4 Is Associated with Cardiovascular Disease in Type 1 Diabetes. Diabetes 2021, 70, 2391–2401. [Google Scholar] [CrossRef] [PubMed]
- Gonzalo-Encabo, P.; Maldonado, G.; Valadés, D.; Ferragut, C.; Pérez-López, A. The Role of Exercise Training on Low-Grade Systemic Inflammation in Adults with Overweight and Obesity: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 13258. [Google Scholar] [CrossRef]
- Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1–11. [Google Scholar] [CrossRef]
- Sonaglioni, A.; Nicolosi, G.L.; Trevisan, R.; Lombardo, M.; Grasso, E.; Gensini, G.F.; Ambrosio, G. The influence of pectus excavatum on cardiac kinetics and function in otherwise healthy individuals: A systematic review. Int. J. Cardiol. 2023, 381, 135–144. [Google Scholar] [CrossRef]
- Scatteia, A.; Baritussio, A.; Bucciarelli-Ducci, C. Strain imaging using cardiac magnetic resonance. Heart Fail. Rev. 2017, 22, 465–476. [Google Scholar] [CrossRef]


| MRP n = 18 | Exercise n = 11 | |
|---|---|---|
| Age, years | 52.1 ± 4.39 | 49.1 ± 9.73 |
| Male sex, n (%) | 12.0 (66.7) | 6.00 (54.5) |
| White ethnic background, n (%) | 13.0 (72.2) | 9.00 (81) |
| Hypertension, n (%) | 12.0 (66.7) | 4.00 (36.4) |
| Hypercholesterolemia, n (%) | 12.0 (66.7) | 5.00 (45.4) |
| Systolic blood pressure, mmHg | 151 ± 13.3 | 136 ± 18.7 |
| Height, cm | 169 ± 9.50 | 169 ± 7.50 |
| Weight, kg | 105 ± 13.5 | 99.6 ± 22.3 |
| Body mass index, kg/m2 | 36.7 ± 4.91 | 34.8 ± 6.70 |
| HbA1c, % | 7.10 ± 0.94 | 7.34 ± 1.23 |
| Medication received, n (%) | ||
| Insulin | 0 | 0 |
| Metformin | 16 (88.8) | 11 (100) |
| GLP-1 antagonist | 1 (5.56) | 1 (9.09) |
| SGLT-2 inhibitor | 2 (11.1) | 1 (9.09) |
| ACE inhibitor | 7 (38.8) | 3 (27.3) |
| Alpha blocker | 1 (5.56) | 0 |
| ARB | 2 (11.1) | 1 (9.09) |
| B-blockers | 2 (11.1) | 2 (18.2) |
| CCB | 4 (22.2) | 2(18.2) |
| Statin | 11 (611) | 5 (45.4) |
| Fibrate | 0 | 0 |
| Baseline–Week 4 | Week 4–Week 12 | ||||||
|---|---|---|---|---|---|---|---|
| Baseline | Week 4 | Week 12 | Mean Difference (95% CI) | Effect Size (95% CI) Cohen’s d | Mean Difference (95% CI) | Effect Size (95% CI) Cohen’s d | |
| MRP group | |||||||
| LV ejection fraction, % | 69.0 ± 7.6 | 65.6 ± 6.2 | 65.2 ± 5.4 | −3.4 (0.29; 6.45) | 0.56 (0.04; 1.07) | −0.3 (−2.543.09) | 0.05 (−0.44; 0.54) |
| LV mass indexed to height, g/cm | 0.78 ± 0.14 | 0.74 ± 0.15 | 0.69 ± 0.22 | −0.04 (0.00; 0.10) | 0.17 (−0.31; 0.64) | 0.00 (−0.05; 0.13) | 0.22 (−0.25; 0.70) |
| Longitudinal PEDSR, −1/s | 0.69 ± 0.08 | 0.71 ± 0.13 | 0.69 ± 0.14 | −0.02 (−0.09; 0.10) | −0.15 (−0.77; 0.48) | −0.02 (−0.09; 0.13) | 0.07 (−0.58; 0.72) |
| Circumferential PEDSR, −1/s | 0.97 ± 0.13 | 0.94 ± 0.19 | 0.97 ± 0.19 | −0.04 (−0.18; 0.08) | 0.20 (−0.29; 0.69) | −0.04 (−0.17; 0.08) | −0.18 (−0.69; 0.32) |
| Global longitudinal strain, % | 15.8 ± 2.6 | 16.5 ± 2.4 | 16.0 ± 1.8 | −0.70 (−2.0; 0.68) | −0.28 (−0.78; 0.24) | −0.57 (−2.0; 0.84) | 0.27 (−0.27; 0.80) |
| Global circumferential strain, % | 20.5 ± 1.09 | 19.9 ± 2.3 | 19.9 ± 1.9 | 0.59 (−0.26; 1.43) | 0.38 (−0.14; 0.90) | −0.21 (−1.01; 0.58) | −0.15 (0.68; 0.37) |
| LV mass-to-volume ratio | 0.86 ± 0.14 | 0.78 ± 0.11 | 0.80 ± 0.12 | −0.08 (0.028; 0.12) | 0.80 (0.24; 1.34) | −0.02 (−0.06; 0.02) | 0.24 (0.74; 0.25) |
| Exercise group | |||||||
| LV ejection fraction, % | 69.03 ± 5.8 | 65.4 ± 5.1 | 67.8 ± 6.1 | −3.39 (−2.23; 9.41) | 0.41 (−0.21; 1.02) | −2.31 (−6.28; 1.64) | 0.39 (−0.99; 0.23) |
| LV mass indexed to height, g/m | 0.70 ± 0.12 | 0.72 ± 0.12 | 0.71 ± 0.1 | −0.02 (−0.05; 0.14) | −0.38 (−0.98; 0.24) | 0.01 (−0.04; 0.14) | 0.07 (−0.51; 0.67) |
| Longitudinal PEDSR, −1/s | 0.76 ± 0.16 | 0.77 ± 0.12 | 0.79 ± 0.14 | −0.01 (0.04; 0.05) | –0.37 (−0.77; 0.71) | 0.02 (−0.14; 0.18) | −0.1 (−0.84; 0.64) |
| Circumferential PEDSR, −1/s | 0.97 ± 0.23 | 1.00 ± 0.15 | 1.08 ± 0.19 | −0.02 (−0.11; 0.06) | −0.17 ((−0.76; 0.43) | −0.08 (0.16; −0.002) | 0.05 (−1.15; 0.11) |
| Global longitudinal strain, % | 16.3 ± 2.9 | 16.1 ± 2.2 | 16.9 ± 2.1 | −0.29 (−2.3; 1.7) | 0.06 (−0.01; 1.29) | −0.92 (−1.69; −1.15) | 0.01 (−0.43; 0.73) |
| Global circumferential strain, % | 19.7 ± 3.1 | 19.3 ± 1.9 | 20.1 ± 2.1 | 0.41 (−1.48; 2.30) | 0.01 (−0.45; 0.73) | −0.81 (−1.83; 0.22) | −0.50 (−1.15; 0.11) |
| LV mass-to-volume ratio | 0.81 ± 0.142 | 0.85 ± 0.18 | 0.82 ± 0.15 | −0.04 (−0.10; 0.02) | −0.44 (−1.05; 0.18) | −0.03 (−0.01; 0.08) | 0.44 (−0.16; 1.04) |
| Baseline—Week 4 | Week 4–Week 12 | ||||||
|---|---|---|---|---|---|---|---|
| Baseline | Week 4 | Week 12 | Mean or Median Difference (95% CI or IQR) | Effect Size (95% CI) | Mean or Median Difference (95% CI or IQR) | Effect Size (95% CI) | |
| CRP, mg/L | 6.26 ± 0.18 | 6.12 ± 0.39 | 6.30 ± 0.19 | −0.14 (−0.07; 0.36) | 0.35 (−0.16; 0.85) | 0.18 (−0.39; 0.03) | 0.45 (−0.95; 0.07) |
| FABP-4, mg/L | 4.87 ± 0.19 | 5.15 ± 0.32 | 4.97 ± 0.30 | 0.27 (−0.42; −0.12) | 0.97 (−1.15; 0.36) | −0.18 (0.02; 0.33) | 0.61 (0.07; 1.14) |
| GDF-15, mg/L | 2.92 ± 0.15 | 2.95 ± 0.32 | 2.88 ± 0.16 | 0.03 (0.20; 0.14) | 0.10 (−0.58; 0.40) | −0.07(−0.08; 0.21) | 0.25 (−0.25; 0.74) |
| MMP-8, mg/L | 2.29 ± 0.31 | 2.26 ± 0.34 | 2.41 ± 0.40 | −0.03 (−0.10; 0.16) | 0.12 (−0.37; 0.62) | 0.14 (−0.28; 0.01) | 0.54 (−1.1; −0.06) |
| Adiponectin * 103, mg/L | 3.57 (2.56; 4.67) | 4.16 (3.23; 5.83) | 4.76 (3.16; 6.16) | 0.62 * (−1.9; 0.95) | 0.55 $ (0.045; 1.04) | 0.18 * (−1.13; 1.21) | 0.20 $ (−0.45; 0.48) |
| Leptin * 103, mg/L | 19.3 (11.9; 41.8) | 6.65 (3.84; 22.3) | 5.89 (3.75; 27.4) | −13.8 * (7.26; 20.34) | 1.05 $ (0.46; 1.62) | −2.53 * (−8.95; 3.89) | 0.20 $ (−0.66; 0.27) |
| Glycated HbA1c, % | 7.10 ± 0.94 | 6.31 ± 1.78 | 6.27 ± 0.78 | −0.79 (0.07; 1.52) | 0.55 (0.04; 1.03) | −0.04 (−0.73; 0.81) | 0.03 (−0.44; 0.48) |
| HOMA-IR | 10.8 (8.38; 14.3) | 4.32 (2.09; 7.62) | 3.98 (2.07; 7.60) | −5.40 * (2.52; 8.01) | 0.88 $ (0.28; 1.45) | −0.40 * (−1.67; 2.22) | 0.30 $ (−0.45; 0.52) |
| Triglycerides, mmol/L | 2.11 ± 1.04 | 1.04 ± 0.28 | 1.31 ± 0.46 | −1.07 (0.55; 1.59) | 1.06 (0.45; 1.64) | 0.27 (−0.51; 0.03) | 0.60 (−1.09; 0.06) |
| Cholesterol, total, mmol/L | 4.64 ± 1.08 | 3.50 ± 0.99 | 4.16 ± 1.24 | −1.14 (−0.81; −1.48) | 1.75 (0.97; 2.51) | 0.66 (1.09; 0.23) | 0.79 (0.23; 1.32) |
| HDL cholesterol, mmol/L | 1.17 ± 0.17 | 1.14 ± 0.19 | 1.21 ± 0.23 | −0.03 (−0.07; 0.12) | 0.14 (−0.56; 0.63) | 0.08 (−0.17; 0.02) | 0.42 (−0.91; 0.83) |
| LDL cholesterol, mmol/L | 2.55 ± 0.88 | 1.96 ± 0.96 | 2.35 (1.16) | −0.59 (0.24; 0.95) | 0.88 (0.29; 1.46) | 0.39 (0.83; 0.07) | 0.61 (0.08; 1.12) |
| Baseline—Week 4 | Week 4–Week 12 | ||||||
|---|---|---|---|---|---|---|---|
| Baseline | Week 4 | Week 12 | Mean or Median Difference (95% CI or IQR) | Effect Size (95% CI) | Mean or Median Difference (95% CI or IQR) | Effect Size (95% CI) | |
| CRP, mg/L | 6.28 ± 0.21 | 6.27 ± 0.26 | 6.26 ± 0.20 | −0.01 (−0.17; 0.19) | 0.35 (−0.58; 0.65) | −0.01 (−0.20; 0.22) | 0.37 (−0.58; 0.66) |
| FABP-4, mg/L | 4.84 ± 0.29 | 4.89 ± 0.35 | 4.80 ± 0.28 | 0.05 (−0.17; 0.05) | 0.36 (−0.99; 0.29) | −0.09 (−0.03; 0.21) | 0.53 (−0.14; 1.19) |
| GDF-15, mg/L | 2.99 ± 0.26 | 2.93 ± 0.52 | 2.94 ± 0.30 | −0.05 (−0.20; 0.31) | 0.15 (−0.48; 0.77) | 0.01 (−0.31; 0.30) | 0.01 (−0.63; 0.61) |
| MMP-8, mg/L | 2.29 ± 0.38 | 2.31 ± 0.31 | 2.29 ± 0.28 | 0.02 (−0.19; 0.15) | 0.09 (−0.70; 0.53) | −0.02 (−0.15; 0.19) | 0.08 (−0.54; 0.70) |
| Adiponectin * 103, mg/L | 3.12 (2.49; 7.29) | 2.73 (1.46; 6.95) | 3.07 (1.65; 7.62) | −0.39 * (−0.68; 1.44) | 0.61 $ (−0.50; 1.25) | 0.34 * (−1.84; 0.32) | 0.40 $ (0.23; 0.90) |
| Leptin * 103, mg/L | 14.4 (6.60; 35.1) | 13.5 (6.31; 35.9) | 11.5 (4.04; 38.9) | −1.05 * (−3.13; 2.57) | 0.07 $ (−0.65; 0.53) | −1.99 * (−4.30; 3.62) | 0.06 $ (−0.63; 0.51) |
| Glycated HbA1c, % | 7.36 ± 1.24 | 7.16 ± 1.22) | 7.12 ± 1.26 | −0.20 (0.10; 0.40) | 0.72 (0.036; 1.37) | −0.04 (−0.29; 0.37) | 0.07 (−0.52; 0.66) |
| HOMA-IR | 9.60 (6.27; 21.0) | 8.53 (6.53; 11.1) | 7.51 (5.70; 18.1) | −1.07 * (−4.21; 3.63) | 0.50 $ (−0.64; 0.74) | −1.01 * (−4.20; 3.60) | 0.30 $ (−0.65; 0.62) |
| Triglycerides, mmol/L | 2.09 ± 0.84 | 2.13 ± 0.86 | 2.16 ± 0.92 | −0.04 (−0.62; 0.54) | 0.05 (−0.64; 0.54) | 0.03 (−0.61; 0.55) | 0.03 (−0.62; 0.56) |
| Cholesterol, total, mmol/L | 4.78 ± 0.72 | 4.57 ± 0.88 | 4.68 ± 0.96 | −0.21 (−0.19; 0.61) | 0.35 (−0.27; 0.95) | 0.11 (−0.79; 0.57) | 0.11 (−0.69; 0.49) |
| HDL cholesterol, mmol/L | 1.22 ± 0.32 | 1.11 ± 0.26 | 1.09 ± 0.26 | −0.11 (0.04; 0.18) | 0.70 (0.29; 1.77) | −0.02 (−0.04; 0.08) | 0.20 (−0.39; 0.80) |
| LDL cholesterol, mmol/L | 2.55 ± 0.75 | 2.44 ± 0.73 | 2.57 ± 0.95 | −0.12 (−0.19; 0.41) | 0.26 (−0.38; 0.89) | 0.13 (−0.68; 0.42) | 0.17 (−0.79; 0.46) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bilak, J.M.; Gulsin, G.S.; Bountziouka, V.; Parke, K.S.; Redman, E.; Henson, J.; Zhao, L.; Costet, P.; Cvijic, M.E.; Maya, J.; et al. Temporal Responses of a Low-Energy Meal Replacement Plan or Exercise Training on Cardiovascular Function and Fibro-Inflammatory Markers in People with Type 2 Diabetes—A Secondary Analysis of the “Diabetes Interventional Assessment of Slimming or Training to Lessen Inconspicuous Cardiovascular Dysfunction” Study. Hearts 2024, 5, 165-181. https://doi.org/10.3390/hearts5010011
Bilak JM, Gulsin GS, Bountziouka V, Parke KS, Redman E, Henson J, Zhao L, Costet P, Cvijic ME, Maya J, et al. Temporal Responses of a Low-Energy Meal Replacement Plan or Exercise Training on Cardiovascular Function and Fibro-Inflammatory Markers in People with Type 2 Diabetes—A Secondary Analysis of the “Diabetes Interventional Assessment of Slimming or Training to Lessen Inconspicuous Cardiovascular Dysfunction” Study. Hearts. 2024; 5(1):165-181. https://doi.org/10.3390/hearts5010011
Chicago/Turabian StyleBilak, Joanna M., Gaurav S. Gulsin, Vasiliki Bountziouka, Kelly S. Parke, Emma Redman, Joseph Henson, Lei Zhao, Phillipe Costet, Mary Ellen Cvijic, Juan Maya, and et al. 2024. "Temporal Responses of a Low-Energy Meal Replacement Plan or Exercise Training on Cardiovascular Function and Fibro-Inflammatory Markers in People with Type 2 Diabetes—A Secondary Analysis of the “Diabetes Interventional Assessment of Slimming or Training to Lessen Inconspicuous Cardiovascular Dysfunction” Study" Hearts 5, no. 1: 165-181. https://doi.org/10.3390/hearts5010011