

In Vivo Biomechanical Response of the Human Cornea to Acoustic Waves

Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Corneal Acoustic Wave Generator
2.2. Instrument Calibration
2.3. Experimental Measurements
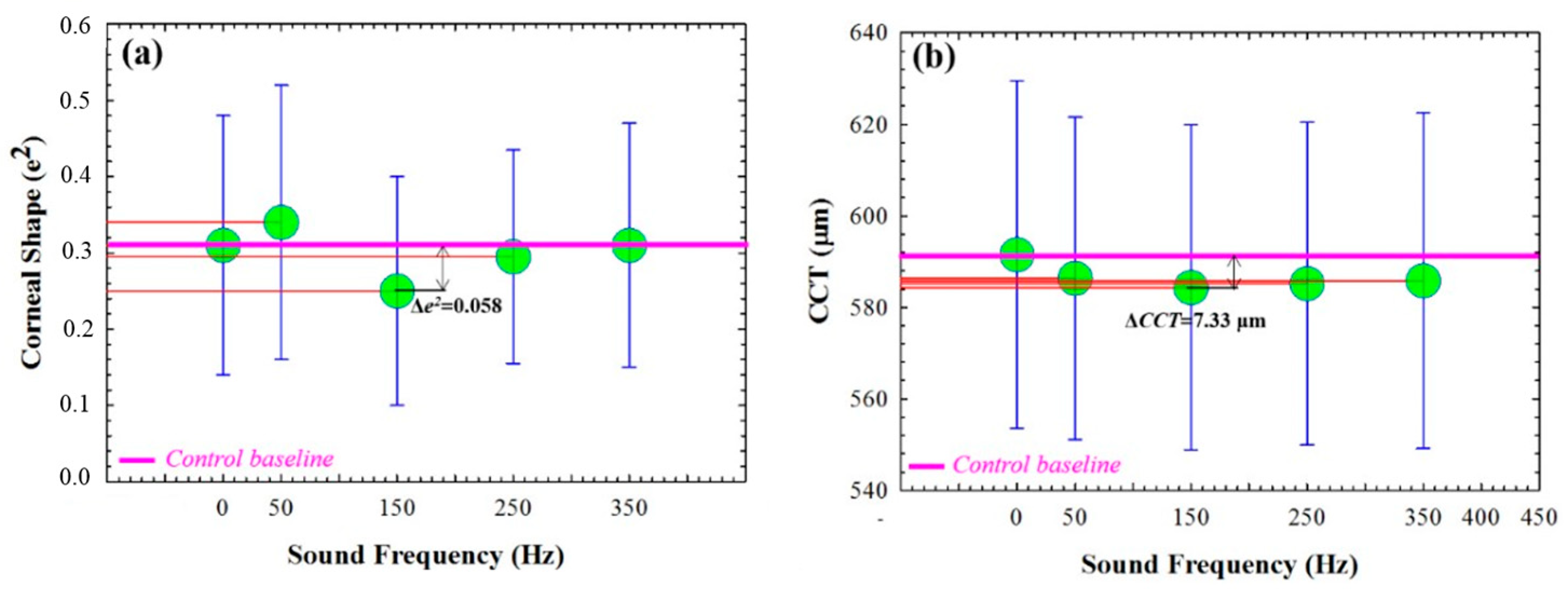
2.3.1. Galilei Dual Scheimpflug Analyzer: Shape Parameters
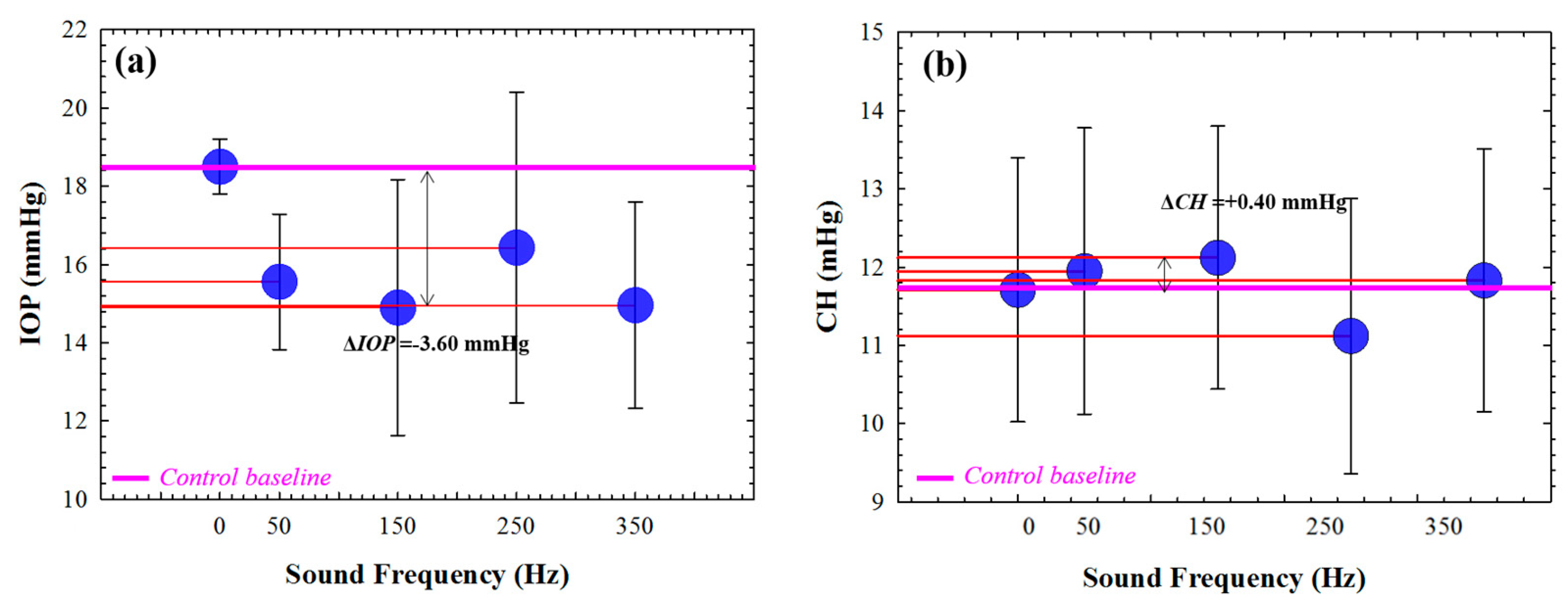
2.3.2. Ocular Response Analyzer: Biomechanical Assessment
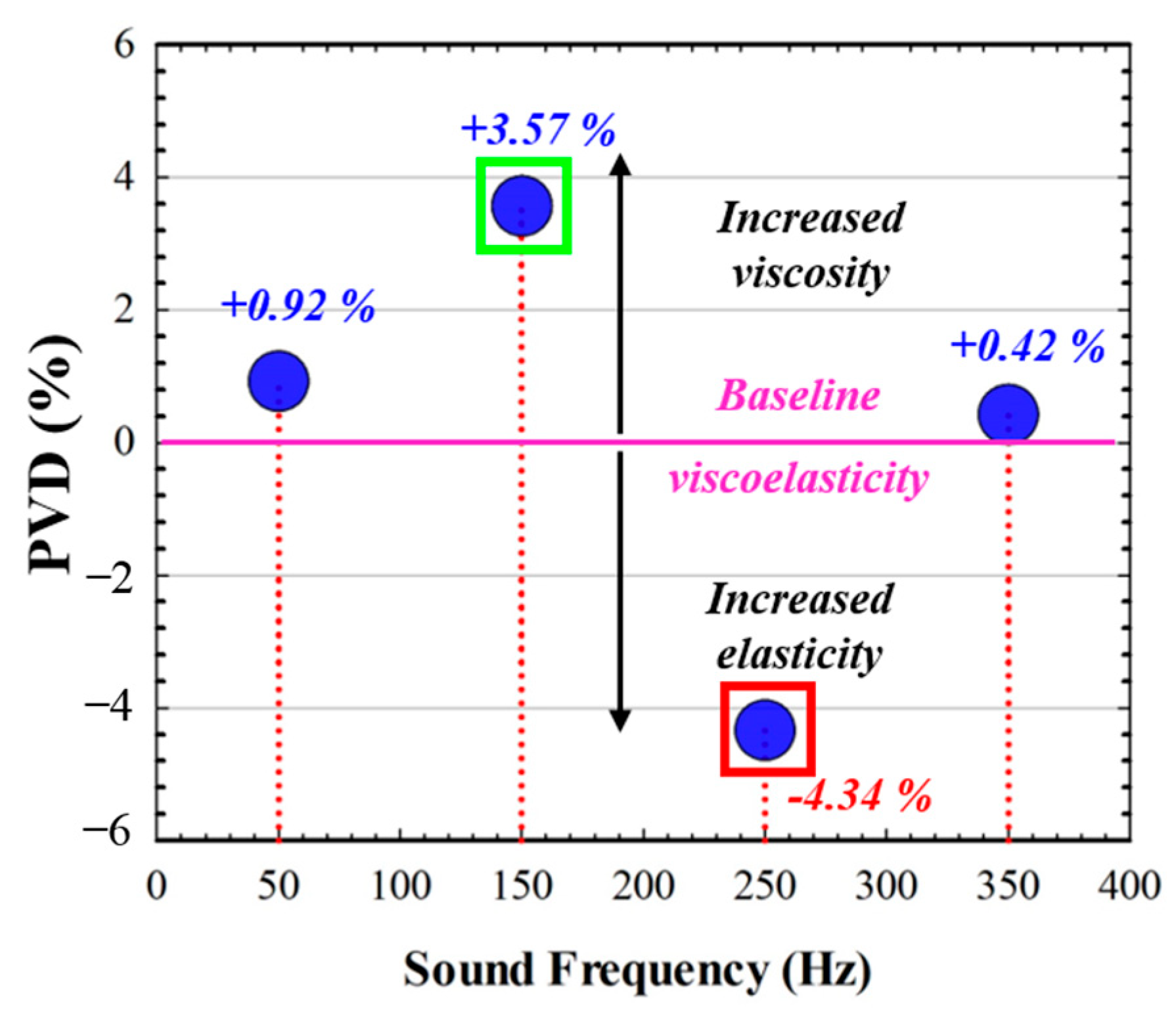
2.3.3. Pneumatic Viscoelastic Damping
3. Results
3.1. Corneal Shape Changes as a Function of the Sound Frequency
3.2. Biomechanical Variations and Sound Frequency
Pneumatic Viscoelastic Damping for Different Sound Wave Frequencies
3.3. Shape and Biomechanical Stability during Cornea and Acoustic Wave Interactions
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Piñero, D.P.; Alcón, N. Corneal biomechanics: A review. Clin. Exp. Optom. 2015, 98, 107–116. [Google Scholar] [CrossRef]
- Kling, S.; Hafezi, F. Corneal biomechanics—A review. Ophtalmic. Physiol. Opt. 2017, 37, 240–252. [Google Scholar] [CrossRef]
- Wilson, A.; Marshall, J. A review of corneal biomechanics: Mechanisms for measurement and the implications for refractive surgery. Indian J. Ophthalmol. 2020, 68, 2679–2690. [Google Scholar] [PubMed]
- Meek, K.M. Corneal collagen-its role in maintaining corneal shape and transparency. Biophys. Rev. 2009, 1, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.; Rodríguez-Vallejo, M.; Martínez, J.; Tauste, A.; Piñero, D.P. Corneal biomechanics after laser refractive surgery: Unmasking differences between techniques. J. Cataract. Refract. Surg. 2018, 44, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Cao, K.; Liu, L.; Yu, T.; Chen, F.; Bai, J.; Liu, T. Changes in corneal biomechanics during small-incision lenticule extraction (SMILE) and femtosecond-assisted laser in situ keratomileusis (FS-LASIK). Lasers Med. Sci. 2020, 35, 599–609. [Google Scholar] [CrossRef]
- Wallace, H.B.; McKelvie, J.; Green, C.R.; Misra, S.L. Corneal Curvature: The Influence of Corneal Accommodation and Biomechanics on Corneal Shape. Transl. Vis. Sci. Technol. 2019, 8, 5. [Google Scholar] [CrossRef]
- Wu, D.; Liu, C.; Li, B.; Wang, D.; Fang, X. Influence of Cap Thickness on Corneal Curvature and Corneal Biomechanics After SMILE: A Prospective, Contralateral Eye Study. J. Refract. Surg. 2020, 36, 82–88. [Google Scholar] [CrossRef]
- Kaushik, S.; Pandav, S.S. Ocular Response Analyzer. J. Curr. Glaucoma Pract. 2012, 6, 17–19. [Google Scholar] [CrossRef]
- Du, Y.; Zhang, Y.; Zhang, Y.; Li, T.; Wang, J.; Du, Z. Analysis of potential impact factors of corneal biomechanics in myopia. BMC Ophthalmol. 2023, 23, 143. [Google Scholar] [CrossRef]
- Choi, E.J.; Kim, K.N.; Song, M.Y.; Hwang, Y.H. Correlation between Interocular Asymmetry of Corneal Hysteresis and Visual Field Defect in Glaucoma. Korean J. Ophthalmol. 2023, 37, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Marcellán, M.C.; Remón, L.; Ávila, F.J. Corneal hysteresis and intraocular pressure are altered in silicone-hydrogel soft contact lenses wearers. Int. Ophthalmol. 2022, 42, 2801–2809. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat, M.R.; Momeni-Moghaddam, H.; Kangari, H.; Moradi, A.; Akbarzadeh, R.; Naroo, S.A. Changes in corneal biomechanical parameters in keratoconus eyes with various severities after corneal cross-linking (CXL): A comparative study. Eur. J. Ophthalmol. 2023, 3, 2114–2122. [Google Scholar] [CrossRef] [PubMed]
- Baptista, P.M.; Ambrosio, R.; Oliveira, L.; Meneres, P.; Beirao, J.M. Corneal Biomechanical Assessment with Ultra-High-Speed Scheimpflug Imaging During Non-Contact Tonometry: A Prospective Review. Clin. Ophthalmol. 2021, 15, 1409–1423. [Google Scholar] [CrossRef]
- Karmiris, E.; Tsiripidis, K.; Gartaganis, P.S.; Totou, S.; Vasilopoulou, M.G.; Patelis, A.; Giannakis, I.; Chalkiadaki, E. Comparison of intraocular pressure obtained by Goldmann applanation tonometer, Corvis ST and an airpuff tonometer in healthy adults. Eur. J. Ophthalmol. 2021, 32, 951–959. [Google Scholar] [CrossRef]
- Eltony, A.M.; Shaom, P.; Yun, S.H. Measuring mechanical anisotropy of the cornea with Brillouin microscopy. Nat. Commun. 2022, 13, 1354. [Google Scholar] [CrossRef]
- Sun, M.G.; Son, T.; Crutison, J.; Guaiquil, V.; Lin, S.; Nammari, L.; Klatt, D.; Yao, X.; Rosenblatt, M.I.; Royston, T.J. Optical coherence elastography for assessing the influence of intraocular pressure on elastic wave dispersion in the cornea. J. Mech. Behav. Biomed. Mater. 2022, 128, 105100. [Google Scholar] [CrossRef]
- Lan, G.; Twa, M.D.; Song, C.; Feng, J.; Huang, Y.; Xu, J.; Qin, J.; An, L.; Wei, X. In vivo corneal elastography: A topical review of challenges and opportunities. Comput. Struct. Biotechnol. J. 2023, 21, 2664–2687. [Google Scholar] [CrossRef]
- Qin, X.; Tian, L.; Zhang, H.; Zhang, D.; Jie, Y.; Zhang, H.X.; Li, L. Determine Corneal Biomechanical Parameters by Finite Element Simulation and Parametric Analysis Based on ORA Measurements. Front. Bioeng. Biotechnol. 2022, 10, 862947. [Google Scholar] [CrossRef]
- Hsu, F.L.; Shih, P.J.; Wang, I.J. Development and validation of an intuitive biomechanics-based method for intraocular pressure measurement: A modal analysis approach. BMC Ophthalmol. 2023, 23, 124. [Google Scholar] [CrossRef]
- Zhao, G.P.; Zhai, H.T.; Xiang, H.Z.; Wu, L.M.; Chen, Q.O.; Chen, C.; Zhou, M. Biomechanical study of cornea response under orthokeratology lens therapy: A finite element analysis. Int. J. Numer. Methods Biomed. Eng. 2023, 39, e3691. [Google Scholar] [CrossRef]
- Wardosanidze, Z.V. About the possible acoustic functions of the eye. Am. J. Biom. Sci. Res. 2021, 15, 79–81. [Google Scholar] [CrossRef]
- Coquart, L.; Depeursinge, C.; Gurnier, A.; Ohayon, R. A fluid-structure interaction problem in biomechanics: Prestressed vibrations of the eye by the finite element method. J. Biomech. 1992, 25, 1105–1118. [Google Scholar] [CrossRef] [PubMed]
- Shih, P.J.; Guo, Y.R. Resonance frequency of fluid-filled and prestressed spherical shell—A model of the human eyeball. J. Acoust. Soc. Am. 2016, 139, 1784. [Google Scholar] [CrossRef] [PubMed]
- Akca, B.I.; Chang, E.W.; Kling, S.; Ramier, A.; Scarcelli, G.; Marcos, S.; Yun, S.H. Observation of sound-induced corneal vibrational modes by optical coherence tomography. Biomed. Opt. Express 2015, 6, 3313–3319. [Google Scholar] [CrossRef]
- Ramier, A.; Tavakol, B.; Yun, S.H. Effect of intraocular pressure on the vibrational resonance of the cornea measured by optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2017, 58, 4326. [Google Scholar]
- Zimprich, L.; Diedrich, J.; Bleeker, A.; Schweitzer, J.A. Corneal Hysteresis as a Biomarker of Glaucoma: Current Insights. Clin. Ophthalmol. 2020, 14, 2255–2264. [Google Scholar] [CrossRef]
- Jammal, A.A.; Medeiros, F.A. Corneal hysteresis: Ready for prime time? Curr. Opin. Ophthalmol. 2022, 33, 243–249. [Google Scholar] [CrossRef]
- Walter, R.E.; Kitovitz, T.L. An experimental and theoretical study of the pneumatic tonometer. Exp. Eye Res. 1972, 13, 14–23. [Google Scholar]
- Kobayashi, A.S.; Staberg, L.G.; Schlegel, W.A. Viscoelastic properties of the human cornea. Exp. Mech. 1973, 13, 497–503. [Google Scholar] [CrossRef]
- Ávila, F.J.; Marcellán, M.C.; Remón, L. On the relationship between corneal biomechanics, macrostructure, and optical properties. J. Imaging 2021, 7, 280. [Google Scholar] [CrossRef] [PubMed]
- Martin, X.D. Normal intraocular pressure in man. Ophthalmologica 1992, 205, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Bakke, E.F.; Hisdal, J.; Semb, S.O. Intraocular Pressure Increases in Parallel with Systemic Blood Pressure during Isometric Exercise. Investig. Opthalmol. Vis. Sci. 2009, 50, 760–764. [Google Scholar] [CrossRef]
- Agarwal, D.; Ehrlich, J.; Shimmyo, M.; Radcliffe, N. The relationship between corneal hysteresis and the magnitude of intraocular pressure reduction with topical prostaglandin therapy. Br. J. Ophthalmol. 2011, 96, 254–257. [Google Scholar] [CrossRef]
- Herndon, L.W.; Choudhri, S.A.; Cox, T.; Damji, K.F.; Shields, M.B.; Allingham, R.R. Central corneal thickness in normal, glaucomatous, and ocular hypertensive eyes. Arch. Ophthalmol. 1997, 115, 1137–1141. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Fan, Z.; Wang, L.; Li, Z.; Jiao, W.; Li, Y. Correlation Analysis between Central Corneal Thickness and Intraocular Pressure in Juveniles in Northern China: The Jinan City Eye Study. PLoS ONE 2011, 9, e104842. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Shape Parameters | Biomechanical Parameters |
|---|---|
| CCT (µm) | IOP (mmg) |
| Eccentricity (e2) | CH (mmHg) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ávila, F.J.; Marcellán, M.C.; Remón, L. In Vivo Biomechanical Response of the Human Cornea to Acoustic Waves. Optics 2023, 4, 584-594. https://doi.org/10.3390/opt4040043
Ávila FJ, Marcellán MC, Remón L. In Vivo Biomechanical Response of the Human Cornea to Acoustic Waves. Optics. 2023; 4(4):584-594. https://doi.org/10.3390/opt4040043
Chicago/Turabian StyleÁvila, Francisco J., Maria Concepción Marcellán, and Laura Remón. 2023. "In Vivo Biomechanical Response of the Human Cornea to Acoustic Waves" Optics 4, no. 4: 584-594. https://doi.org/10.3390/opt4040043