
Development and Testing of the Aftercare Problem List, a Burn Aftercare Screening Instrument
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Phase 1: Content Refinement
3.2. Phase 2: Cognitive Evaluations
3.3. Phase 3: Testing the Instrument
3.4. Qualitative Results
3.5. Adjustments after the Testing Phase
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
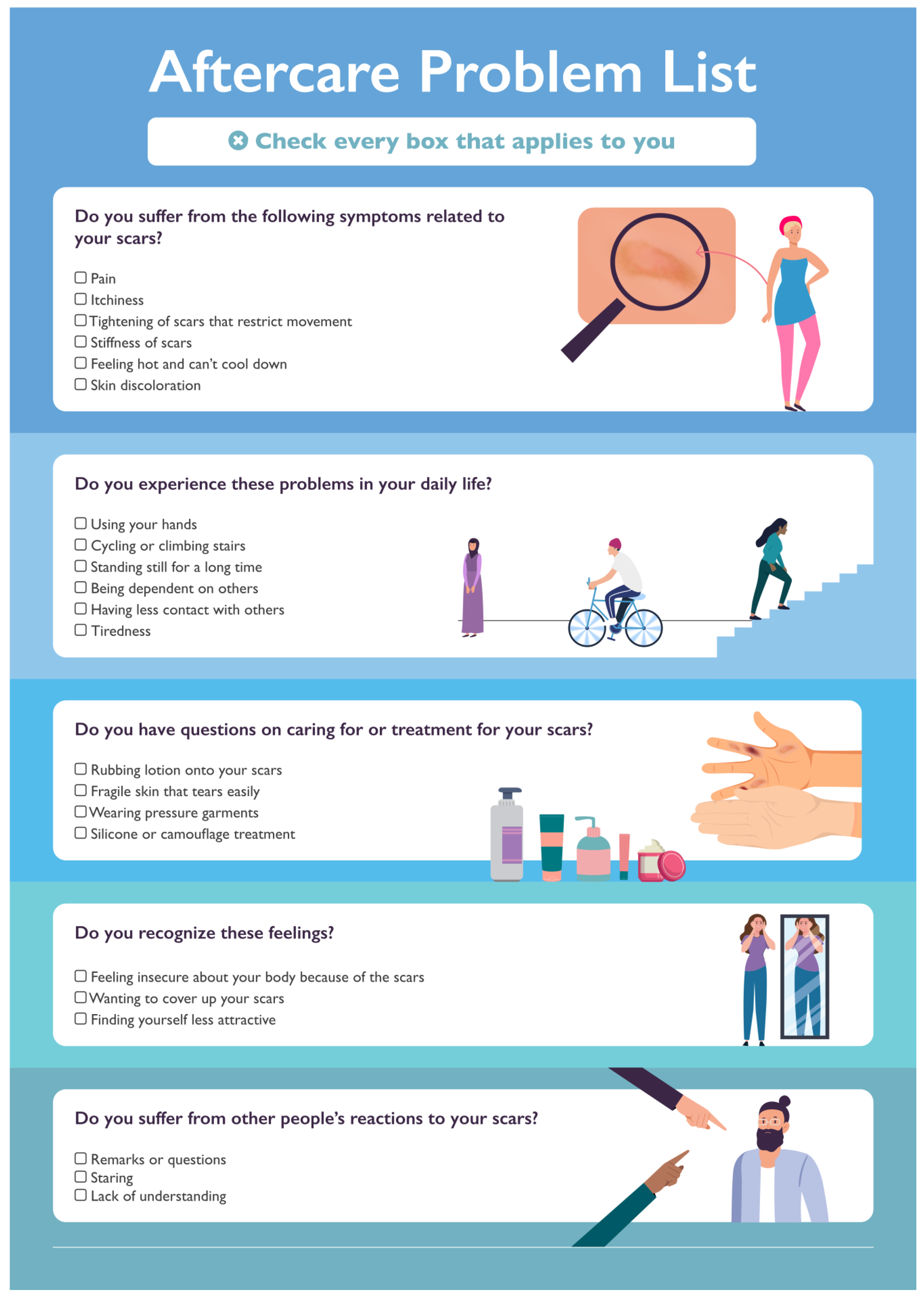
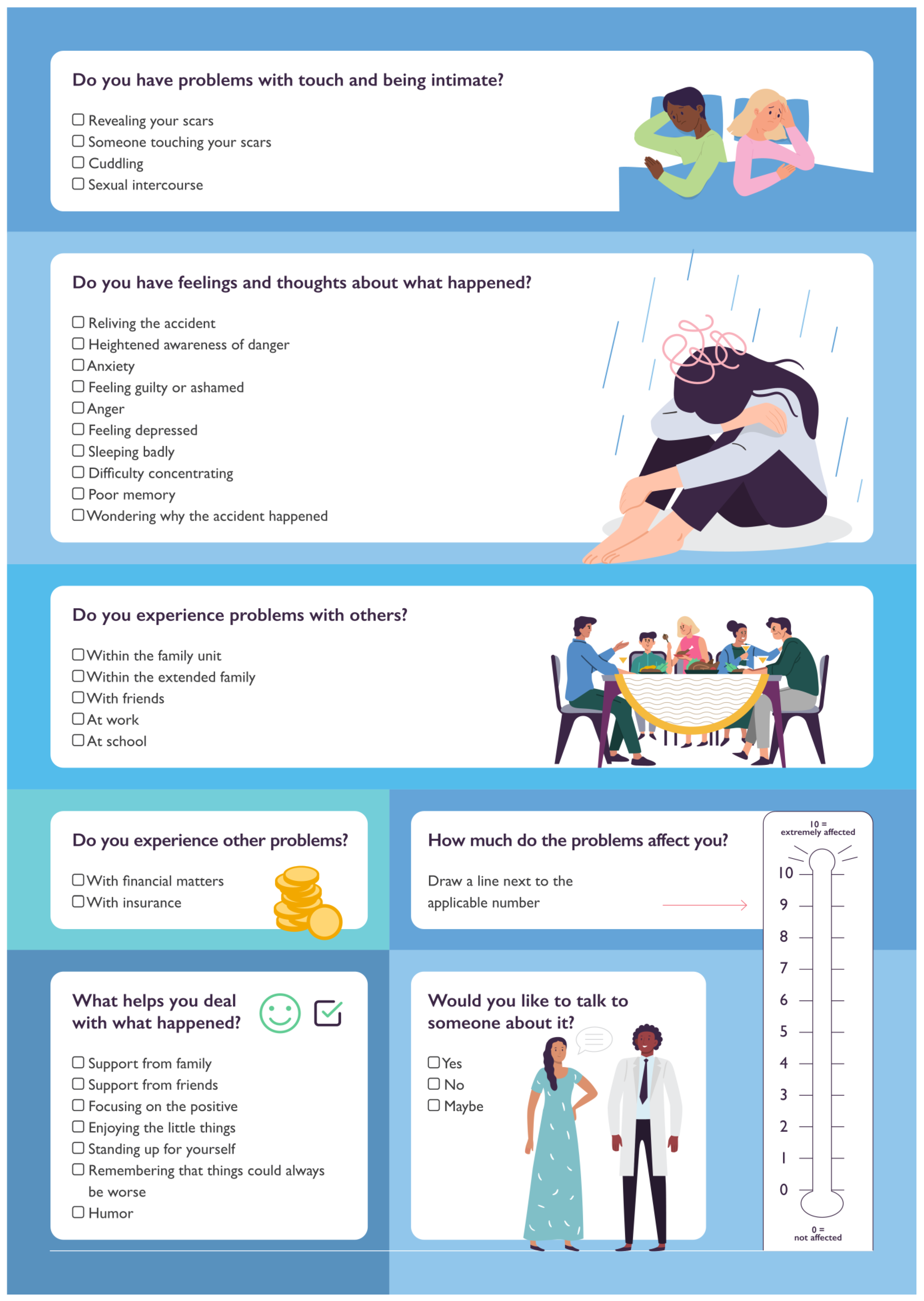
Appendix A. The Aftercare Problem List


References
- Bombaro, K.M.; Engrav, L.H.; Carrougher, G.J.; Wiechman, S.A.; Faucher, L.; Costa, B.A.; Heimbach, D.M.; Rivara, F.P.; Honari, S. What is the prevalence of hypertrophic scarring following burns? Burns 2003, 29, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Gerber, L.H.; Bush, H.; Holavanahalli, R.; Esselman, P.; Schneider, J.; Heinemann, A.; Garfinkel, S.; Cai, C. A scoping review of burn rehabilitation publications incorporating functional outcomes. Burns 2019, 45, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Carrougher, G.J.; Martinez, E.M.; McMullen, K.S.; Fauerbach, J.A.; Holavanahalli, R.K.; Herndon, D.N.; Wiechman, S.A.; Engrav, L.H.; Gibran, N.S. Pruritus in adult burn survivors: Postburn prevalence and risk factors associated with increased intensity. J. Burn. Care Res. 2013, 34, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Van Loey, N.E.E.; de Jong, A.E.E.; Hofland, H.W.C.; van Laarhoven, A.I.M. Role of burn severity and posttraumatic stress symptoms in the co-occurrence of itch and neuropathic pain after burns: A longitudinal study. Front. Med. 2022, 9, 997183. [Google Scholar] [CrossRef] [PubMed]
- Tracy, L.M.; Edgar, D.W.; Schrale, R.; Cleland, H.; Gabbe, B.J.; BRANZ Adult Long-Term Outcomes Pilot Project Participating Sites and Working Party. Predictors of itch and pain in the 12 months following burn injury: Results from the Burns Registry of Australia and New Zealand (BRANZ) Long-Term Outcomes Project. Burns Trauma 2020, 8, tkz004. [Google Scholar] [CrossRef] [PubMed]
- Van Loey, N.E.; Oggel, A.; Goemanne, A.S.; Braem, L.; Vanbrabant, L.; Geenen, R. Cognitive emotion regulation strategies and neuroticism in relation to depressive symptoms following burn injury: A longitudinal study with a 2-year follow-up. J. Behav. Med. 2014, 37, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Giannoni-Pastor, A.; Eiroa-Orosa, F.J.; Fidel Kinori, S.G.; Arguello, J.M.; Casas, M. Prevalence and Predictors of Posttraumatic Stress Symptomatology Among Burn Survivors: A Systematic Review and Meta-Analysis. J. Burn. Care Res. 2016, 37, e79–e89. [Google Scholar] [CrossRef]
- Fauerbach, J.A.; Heinberg, L.J.; Lawrence, J.W.; Bryant, A.G.; Richter, L.; Spence, R.J. Coping with body image changes following a disfiguring burn injury. Health Psychol. 2002, 21, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Thombs, B.D.; Notes, L.D.; Lawrence, J.W.; Magyar-Russell, G.; Bresnick, M.G.; Fauerbach, J.A. From survival to socialization: A longitudinal study of body image in survivors of severe burn injury. J. Psychosom. Res. 2008, 64, 205–212. [Google Scholar] [CrossRef]
- Ohrtman, E.A.; Shapiro, G.D.; Simko, L.C.; Dore, E.; Slavin, M.D.; Saret, C.; Amaya, F.; Lomelin-Gascon, J.; Ni, P.; Acton, A.; et al. Social Interactions and Social Activities After Burn Injury: A Life Impact Burn Recovery Evaluation (LIBRE) Study. J. Burn. Care Res. 2018, 39, 1022–1028. [Google Scholar] [CrossRef]
- Dyster-Aas, J.; Kildal, M.; Willebrand, M. Return to work and health-related quality of life after burn injury. J. Rehabil. Med. 2007, 39, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Willemse, H.; Geenen, R.; Egberts, M.R.; Engelhard, I.M.; Van Loey, N.E. Perceived stigmatization and fear of negative evaluation: Two distinct pathways to body image dissatisfaction and self-esteem in burn survivors. Psychol. Health 2021, 38, 445–458. [Google Scholar] [CrossRef] [PubMed]
- Hemmati Maslakpak, M.; Ajoudani, F.; Lotfi, M.; Alinejad, V. Burn self-stigma: A hybrid concept analysis. Burns 2022, 48, 1405–1416. [Google Scholar] [CrossRef] [PubMed]
- Boersma-van Dam, E.; Engelhard, I.M.; van de Schoot, R.; Van Loey, N.E.E. Bio-Psychological Predictors of Acute and Protracted Fatigue After Burns: A Longitudinal Study. Front. Psychol. 2021, 12, 794364. [Google Scholar] [CrossRef] [PubMed]
- Lerman, S.F.; Owens, M.A.; Liu, T.; Puthumana, J.; Hultman, C.S.; Caffrey, J.A.; Smith, M.T. Sleep after burn injuries: A systematic review and meta-analysis. Sleep. Med. Rev. 2022, 65, 101662. [Google Scholar] [CrossRef] [PubMed]
- Gabbe, B.J.; Cleland, H.; Watterson, D.; Schrale, R.; McRae, S.; Taggart, S.; Darton, A.; Wood, F.; Edgar, D.W.; BRANZ Adult Long Term Outcomes Pilot Project Participating Sites and Working Party. Predictors of moderate to severe fatigue 12 months following admission to hospital for burn: Results from the Burns Registry of Australia and New Zealand (BRANZ) Long Term Outcomes project. Burns 2016, 42, 1652–1661. [Google Scholar] [CrossRef] [PubMed]
- Hurley, A.; King, I.C.C.; Perry, F.M.; Dheansa, B.S. Addressing sexual function in adult burns victims: A multidisciplinary survey of current practice in UK burn units. Burns 2022, 48, 926–931. [Google Scholar] [CrossRef]
- Heath, J.; Shepherd, L.; Harcourt, D. Towards improved psychological outcomes for survivors of burn injuries. Scars Burn. Health 2018, 4, 2059513118765371. [Google Scholar] [CrossRef] [PubMed]
- Mason, S.A.; Nathens, A.B.; Byrne, J.P.; Ellis, J.; Fowler, R.A.; Gonzalez, A.; Karanicolas, P.J.; Moineddin, R.; Jeschke, M.G. Association Between Burn Injury and Mental Illness among Burn Survivors: A Population-Based, Self-Matched, Longitudinal Cohort Study. J. Am. Coll. Surg. 2017, 225, 516–524. [Google Scholar] [CrossRef]
- Mead, N.; Bower, P. Patient-centredness: A conceptual framework and review of the empirical literature. Soc. Sci. Med. 2000, 51, 1087–1110. [Google Scholar] [CrossRef]
- Lindsay, D.; Kirkwood, K.; Crawford, R. Psychosocial Screening in Adult Burns Inpatients within a Scottish Burns Unit. Eur. Burn. J. 2023, 4, 201–203. [Google Scholar] [CrossRef]
- Smith, M.B.; Wiechman, S.A.; Mandell, S.P.; Gibran, N.S.; Vavilala, M.S.; Rivara, F.P. Current Practices and Beliefs Regarding Screening Patients with Burns for Acute Stress Disorder and Posttraumatic Stress Disorder: A Survey of the American Burn Association Membership. Eur. Burn. J. 2021, 2, 215–225. [Google Scholar] [CrossRef]
- Loehr, V.G.; Goette, W.F.; Roaten, K. Screening and Assessment for Psychological Distress among Burn Survivors. Eur. Burn. J. 2022, 3, 57–88. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). In Distress Management; JNCCN: Plymouth Meeting, PA, USA, 2020; Volume 2. [Google Scholar] [CrossRef]
- Biddle, L.; Paramasivan, S.; Harris, S.; Campbell, R.; Brennan, J.; Hollingworth, W. Patients’ and clinicians’ experiences of holistic needs assessment using a cancer distress thermometer and problem list: A qualitative study. Eur. J. Oncol. Nurs. 2016, 23, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Hofland, H.W.C.; Van de Steenoven, A.; Van Loey, N.E.E. Aspects of Clinical Utility of the Distress Thermometer and Problem List after Burns. Eur. Burn. J. 2022, 3, 320–327. [Google Scholar] [CrossRef]
- Gibson, J.A.G.; Yarrow, J.; Brown, L.; Evans, J.; Rogers, S.N.; Spencer, S.; Shokrollahi, K. Identifying patient concerns during consultations in tertiary burns services: Development of the Adult Burns Patient Concerns Inventory. BMJ Open 2019, 9, e032785. [Google Scholar] [CrossRef] [PubMed]
- Kool, M.B.; Geenen, R.; Egberts, M.R.; Wanders, H.; Van Loey, N.E. Patients’ perspectives on quality of life after burn. Burns 2017, 43, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Spronk, I.; Legemate, C.M.; Dokter, J.; van Loey, N.E.E.; van Baar, M.E.; Polinder, S. Predictors of health-related quality of life after burn injuries: A systematic review. Crit. Care 2018, 22, 160. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.E.; Zelinski, E.L.; Toivonen, K.I.; Sundstrom, L.; Jobin, C.T.; Damaskos, P.; Zebrack, B. Prevalence of psychosocial distress in cancer patients across 55 North American cancer centers. J. Psychosoc. Oncol. 2019, 37, 5–21. [Google Scholar] [CrossRef]
- Graves, K.D.; Arnold, S.M.; Love, C.L.; Kirsh, K.L.; Moore, P.G.; Passik, S.D. Distress screening in a multidisciplinary lung cancer clinic: Prevalence and predictors of clinically significant distress. Lung Cancer 2007, 55, 215–224. [Google Scholar] [CrossRef]
- Bich, C.S.; Kostev, K.; Baus, A.; Jacob, L. Burn injury and incidence of psychiatric disorders: A retrospective cohort study of 18,198 patients from Germany. Burns 2021, 47, 1110–1117. [Google Scholar] [CrossRef]
- Hodder, K.; Chur-Hansen, A.; Parker, A. A Thematic Study of the Role of Social Support in the Body Image of Burn Survivors. Health Psychol. Res. 2014, 2, 1196. [Google Scholar] [CrossRef] [PubMed]
- Kornhaber, R.; Wilson, A.; Abu-Qamar, M.Z.; McLean, L. Adult burn survivors’ personal experiences of rehabilitation: An integrative review. Burns 2014, 40, 17–29. [Google Scholar] [CrossRef]
- Moi, A.L.; Gjengedal, E. The lived experience of relationships after major burn injury. J. Clin. Nurs. 2014, 23, 2323–2331. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, E.K.; Baig, S.A.; Persoskie, A. Developing and Validating Measures of Absolute and Relative E-Cigarette Product Risk Perceptions: Single Items Can Be Surprisingly Comprehensive. Nicotine Tob. Res. 2022, 24, 316–323. [Google Scholar] [CrossRef] [PubMed]
- McDermott, L.; Hotton, M.; Cartwright, A.V. Understanding the Barriers and Enablers for Seeking Psychological Support following a Burn Injury. Eur. Burn. J. 2023, 4, 303–317. [Google Scholar] [CrossRef]
- Shepherd, L.; Turner, A.; Reynolds, D.P.; Thompson, A.R. Acceptance and commitment therapy for appearance anxiety: Three case studies. Scars Burn. Health 2020, 6, 2059513120967584. [Google Scholar] [CrossRef]
- Fauerbach, J.A.; Gehrke, A.K.; Mason, S.T.; Gould, N.F.; Milner, S.M.; Caffrey, J. Cognitive Behavioral Treatment for Acute Posttrauma Distress: A Randomized, Controlled Proof-of-Concept Study among Hospitalized Adults with Burns. Arch. Phys. Med. Rehabil. 2020, 101, S16–S25. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Domain | N (%) | N (%) ≥ 1 Item Checked | Mdn DT Item Checked/ Mdn DT Item Unchecked |
|---|---|---|---|
| 1 Scars | 83 (81.4) | ||
| Pain | 34 (33.3%) | 6/2.5 | |
| Itch | 56 (54.9%) | 5/2.5 | |
| Tightening of scars that restrict movement | 48 (47.1%) | 6/2 | |
| Stiffness of scars | 36 (35.3%) | 6/3 | |
| Feeling hot and can’t cool down | 8 (7.8%) | 5/3 | |
| Skin discoloration | 41 (51.2%) | 5/4 | |
| 2 Daily life functioning | 60 (58.8) | ||
| Using your hands | 21 (20.6) | 5/3 | |
| Cycling or climbing stairs | 8 (7.8) | 5/4 | |
| Standing still for a long time | 16 (15.7) | 5/3 | |
| Being dependent on others | 19 (18.6) | 7/3 | |
| Having less contact with others | 19 (18.6) | 7/4 | |
| Tiredness | 31 (30.4) | 5/3 | |
| 3 Scar treatment | |||
| Rubbing lotion onto your scars | 51 (50) | 4/4 | |
| Fragile skin that tears easily | 14 (13.7) | 6/3 | |
| Wearing pressure garments | 30 (29.4) | 6/3 | |
| Silicone or camouflage treatment | 12 (15.8) | 6.5/3.5 | |
| 4 Body perceptions | 47 (46.1) | ||
| Feeling insecure about your body because of the scars | 26 (25.5) | 5.5/3 | |
| Wanting to cover up your scars | 30 (29.4) | 6/3 | |
| Finding yourself less attractive | 25 (24.5) | 7/3 | |
| 5 Stigmatization | 46 (45.1) | ||
| Remarks or questions | 30 (29.4) | 5.5/3 | |
| Staring | 21 (20.6) | 7/3 | |
| Lack of understanding | 10 (9.8) | 6/3.5 | |
| 6 Intimacy | 26 (25.5) | ||
| Revealing your scars | 19 (18.6) | 6/3 | |
| Someone touching your scars | 17 (16.7) | 7/3 | |
| Cuddling | 5 (4.9) | 6.5/4 | |
| Sexual intercourse | 7 (6.9) | 6.5/4 | |
| 7 Mental health | 71 (69.6) | ||
| Reliving the accident | 18 (17.6) | 5/3 | |
| Heightened awareness of danger | 31 (30.4) | 5/3 | |
| Feeling guilty, ashamed or angry | 25 (24.5) | 5/3 | |
| Feeling depressed | 29 (28.4) | 5/2.5 | |
| Sleeping badly | 21 (20.6) | 7.5/3 | |
| Difficulty concentrating and poor memory | 28 (27.5) | 7/3 | |
| Wondering why the accident happened | 23 (22.5) | 5/3 | |
| 8 Relationships | 25 (24.5) | ||
| Within the family unit | 12 (11.8) | 3/4 | |
| Within the extended family | 12 (11.8) | 2.5/4.5 | |
| With friends | 11 (10.8) | 4.5/4 | |
| At work or school | 10 (9.8) | 6/3 | |
| 9 Financial concerns | 9 (8.8) | ||
| With financial matters | 6 (5.9) | 6.5/3.5 | |
| With insurance | 5 (4.9) | 7/4 | |
| 10 Positive coping | 90 (88.2) | ||
| Support from family and friends | 62 (60.8) | 5/2 | |
| Focusing on the positive | 45 (44.1) | 4/4 | |
| Enjoying the little things | 37 (36.3) | 4/5 | |
| Standing up for yourself | 50 (49.0) | 5/3 | |
| Remembering that things could always be worse | 19 (18.6) | 3/5 | |
| Humor | 39 (38.2) | 3/5 |
| DT | D1 | D2 | D3 | D4 | D5 | D6 | D7 | D8 | D9 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| DT | - | ||||||||||
| D1 Scar | 0.47 ** | - | |||||||||
| D2 Functioning | 0.43 ** | 0.33 ** | - | ||||||||
| D3 Treatment | 0.19 | 0.26 ** | 0.13 | - | |||||||
| D4 Body | 0.60 ** | 0.39 ** | 0.38 ** | 0.20 * | - | ||||||
| D5 Stigma | 0.30 ** | 0.28 ** | 0.38 ** | 0.25 * | 0.48 ** | - | |||||
| D6 Intimacy | 0.44 ** | 0.26 ** | 0.40 ** | 0.10 | 0.62 ** | 0.37 ** | - | ||||
| D7 Mental | 0.62 ** | 0.37 ** | 0.51 ** | 0.08 | 0.68 ** | 0.38 ** | 0.56 ** | - | |||
| D8 Relations | 0.23 * | 0.16 | 0.31 ** | 0.20 * | 0.21 * | 0.16 | 0.20 * | 0.30 ** | - | ||
| D9 Financial | 0.28 ** | 0.09 | 0.34 ** | −0.01 | 0.21 * | 0.19 | 0.28 ** | 0.33 ** | 0.27 ** | - | |
| D10 Coping | 0.09 | 0.26 ** | 0.19 | 0.06 | 0.24 * | 0.14 | 0.15 | 0.35 ** | 0.07 | 0.08 | |
| Mean | 3.6 | 0.38 | 0.17 | 0.29 | 0.26 | 0.20 | 0.10 | 0.25 | 0.11 | 0.05 | 0.41 |
| SD | 2.7 | 0.26 | 0.20 | 0.24 | 0.35 | 0.26 | 0.24 | 0.25 | 0.22 | 0.18 | 0.29 |
| Variable | B | SE | Beta | t | p-Value |
|---|---|---|---|---|---|
| Constant | 1.86 | 0.39 | 4.74 | 0.000 | |
| Scars | 2.31 | 0.81 | 0.22 | 2.85 | 0.005 |
| Daily life functioning | 3.21 | 1.11 | 0.23 | 2.89 | 0.005 |
| Body perceptions | 2.02 | 0.74 | 0.26 | 2.74 | 0.007 |
| Mental health | 3.32 | 1.14 | 0.30 | 2.92 | 0.004 |
| Positive coping | −1.70 | 0.70 | −0.18 | −2.41 | 0.018 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Loey, N.E.E.; Boersma-van Dam, E.; Boekelaar, A.; van de Steenoven, A.; de Jong, A.E.E.; Hofland, H.W.C. Development and Testing of the Aftercare Problem List, a Burn Aftercare Screening Instrument. Eur. Burn J. 2024, 5, 90-103. https://doi.org/10.3390/ebj5020008
Van Loey NEE, Boersma-van Dam E, Boekelaar A, van de Steenoven A, de Jong AEE, Hofland HWC. Development and Testing of the Aftercare Problem List, a Burn Aftercare Screening Instrument. European Burn Journal. 2024; 5(2):90-103. https://doi.org/10.3390/ebj5020008
Chicago/Turabian StyleVan Loey, Nancy E. E., Elise Boersma-van Dam, Anita Boekelaar, Anneke van de Steenoven, Alette E. E. de Jong, and Helma W. C. Hofland. 2024. "Development and Testing of the Aftercare Problem List, a Burn Aftercare Screening Instrument" European Burn Journal 5, no. 2: 90-103. https://doi.org/10.3390/ebj5020008