
War at Sea: Burn Care Challenges—Past, Present and Future
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Naval Warfare, Medical Tactics and Burn Care at Sea: First and Second World Wars
2.1. World War I
2.2. World War II
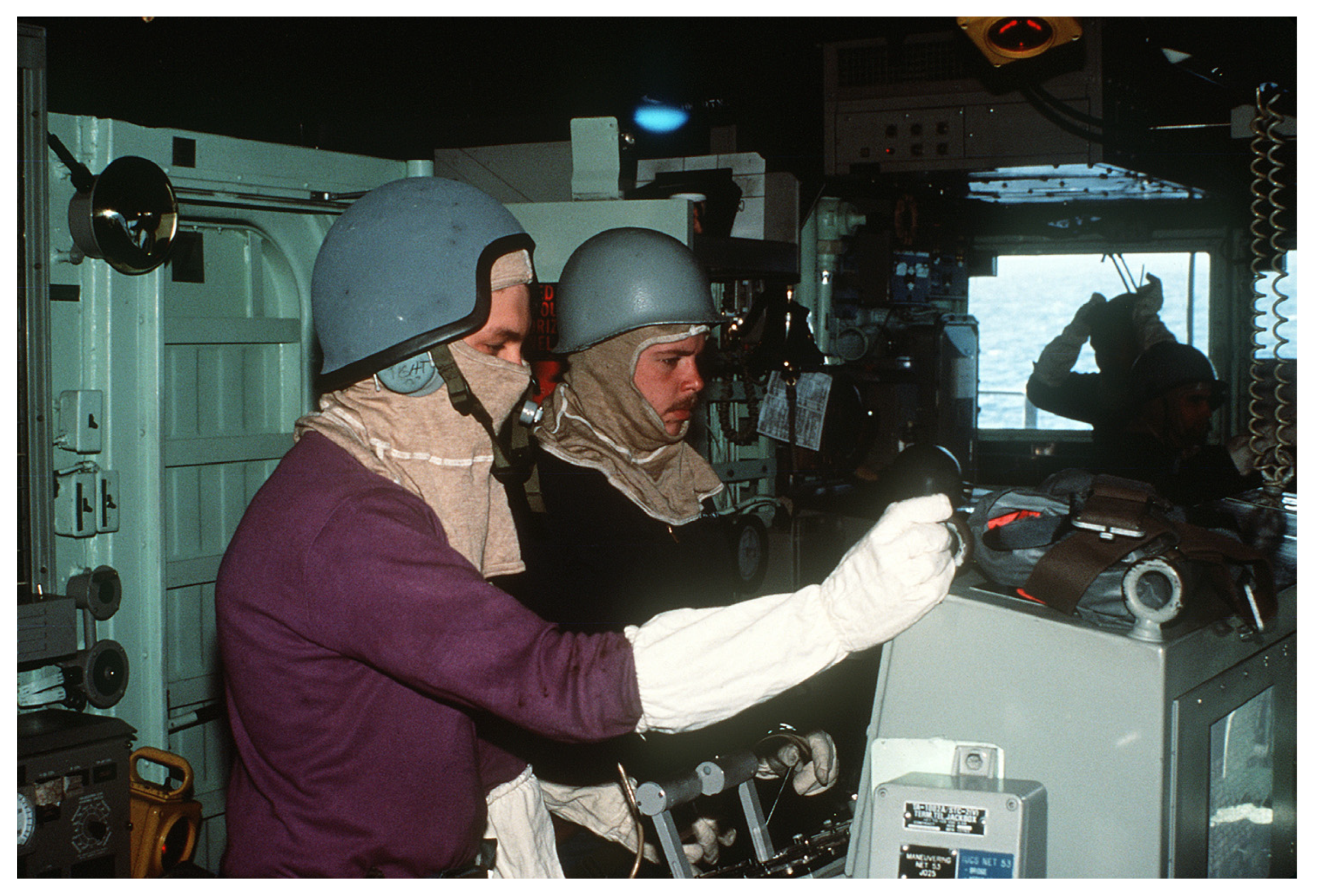
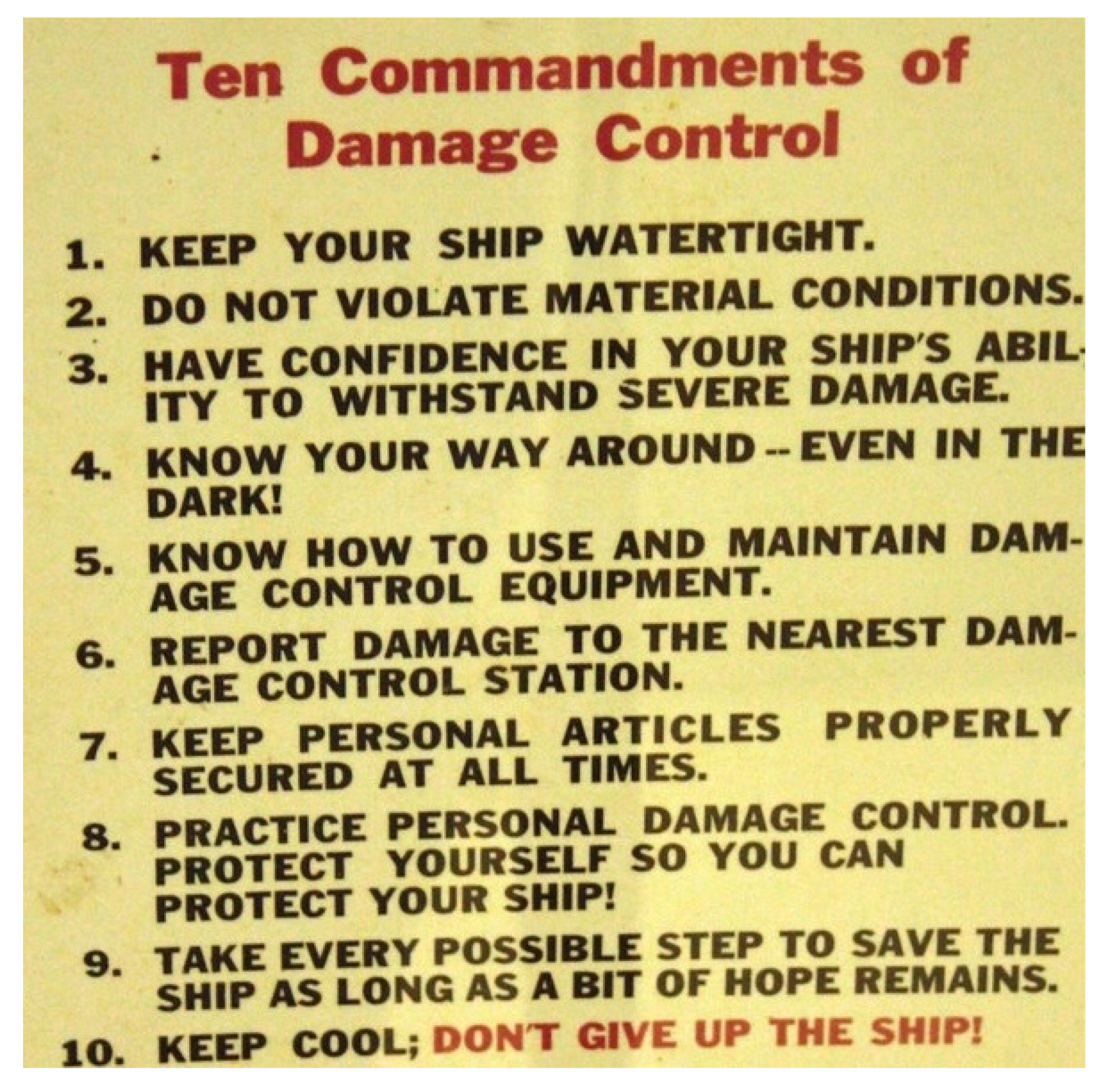
2.3. Current Shipboard Medical Tactics
- Make repairs to electrical and communication circuits and restore power throughout the ship.
- Give first aid (e.g., TCCC) and transport injured personnel to battle dressing stations without seriously reducing the party’s damage control capabilities.
- Detect, identify, and measure radiation dose and dose rate intensities.
- Decontaminate the affected areas of nuclear, biological, and chemical attacks.
- Identify, control, and extinguish all types of fires.
- Control and remove flooding water (using various pumps). Hull integrity is typically controlled with various types of shoring materials which can include mattresses, pil-lows, canvas materials, hydraulic jacks, wooden wedges, beams, plugs, and blocks.
- Evaluate and correctly report the extent of damage in the repair parties’ area of re-sponsibility.
- Make emergency repairs to various piping systems.
- Be familiar with all damage control fittings in the assigned area, such as watertight doors, hatches, scuttles, ventilation systems, and various valves.
- Control and clean up hazardous material spills.
3. Modern Shipboard Burn Injury during Routine Naval Operations
3.1. Major Burn Injury
3.2. Minor Burn Injury at Sea
4. Modern Naval Warfare and Burn Injury at Sea
4.1. USS Stark and USS Cole Attacks
4.2. Mine Warfare and the Power of Injury Prevention
4.3. The Falklands War
5. Distributed Maritime Operations and the Future Fight
5.1. Distributed Maritime Operations
5.2. The “Carrier Killer” Anti-Ship Ballistic Missile
5.3. Clinical Vignette: Severe Maritime Burn Injury and the Tyranny of Distance
6. Preparing for a Future War at Sea: The Good, the Bad, and the Ugly
6.1. The Good
6.1.1. Clinical Practice Guidelines
- Tactical Combat Casualty Care (TCCC) Guidelines available at: https://books.allogy.com/web/tenant/8/books/b729b76a-1a34-4bf7-b76b-66bb2072b2a7/ (accessed on 31 July 2023).
- Burn Care—CPG ID: 12 available at: https://jts.health.mil/assets/docs/cpgs/Burn_Care_11_May_2016_ID12.pdf (accessed on 31 July 2023).
- Inhalation Injury and Toxic Industrial Chemical Exposure—CPG ID: 25 available at: https://jts.health.mil/assets/docs/cpgs/Inhalation_Injury_Toxic_and_Industrial_Chemical_Exposure_26_Jul_2016_ID25_updated.pdf (accessed on 31 July 2023).
- Burn Wound Care in Prolonged Field Care (PFC)—CPG ID 57 available at: https://jts.health.mil/assets/docs/cpgs/Burn_Management_PFC_13_Jan_2017_ID57.pdf (accessed on 31 July 2023).
- Austere Resuscitative Surgical Care (ARSC)—CPG ID: 76 available at: https://jts.health.mil/assets/docs/cpgs/Austere_Resuscitative_Surgical_Care_30_Oct_2019_ID76.pdf (accessed on 31 July 2023).
- Prolonged Casualty Care Guidelines (PCC)—CPG ID 91 available at: https://jts.health.mil/assets/docs/cpgs/Prolonged_Casualty_Care_Guidelines_21_Dec_2021_ID91.pdf (accessed on 31 July 2023).
6.1.2. US Army Institute of Surgical Research Burn Center
USAISR Burn Center contact information:
- DSN 312-429-2876 (429-BURN)
- Commercial (210) 916-2876 or (210) 222-2876
- Email to burntrauma.consult.army@health.mil
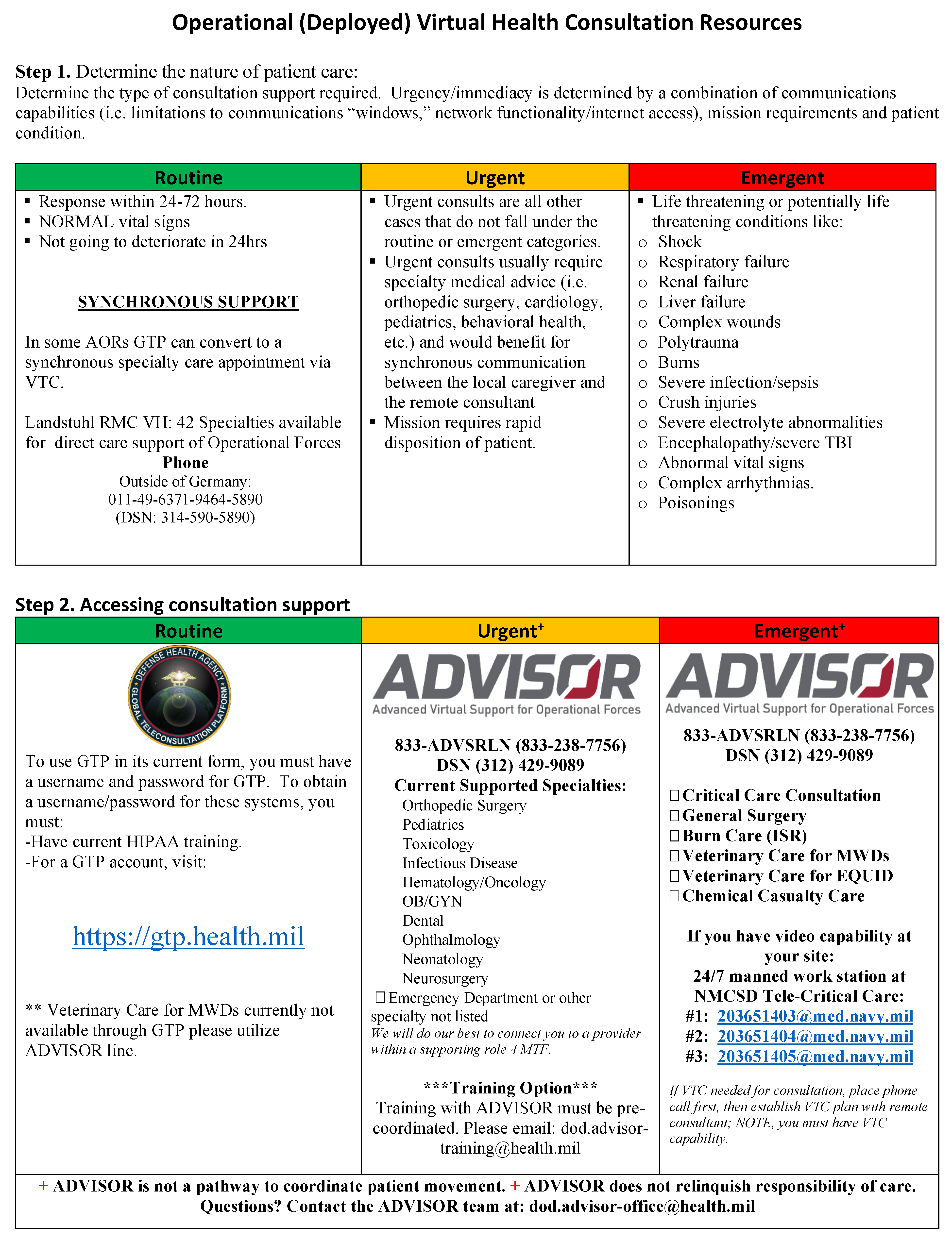
6.1.3. Operational Virtual Health Consultation Resources
6.1.4. Military Civilian Partnerships
6.2. The Bad
6.2.1. Availability of Routine Pre-Deployment Burn Care Training and Clinical Experience
6.2.2. Distribution and Re-Supply of Crystalloid and Dressing Supplies
6.3. The Ugly
6.3.1. Clinical Skills Sustainment Opportunities for Independent Duty Corpsmen
6.3.2. Acute Burn and Hemorrhagic Shock Resuscitation: Plasma and Whole Blood Availability
- It can be stored at room temperature for up to two years and pre-positioned in ship Battle Dressing Stations [98].
- It can be rapidly reconstituted in sterile water for administration [98].
- As many burn patients in the military setting have concomitant traumatic injuries, it also provides immediate resuscitation for hemorrhagic shock until other blood products are available [98].
6.3.3. Austere Role 2 and En Route Critical Care Capability
- Non-invasive and invasive airway management (e.g., intubation and cricothy-roidotomy).
- Non-invasive and ventilator management, airway maintenance, oxygen delivery, and monitoring. Consider and manage inhalation injury.
- Intravenous and central venous access.
- Shock management, vasopressors, monitoring, and oxygen delivery.
- Rule of Tens: 10 mL/h × % TBSA. Increase fluid rate by approximately 20–25%/h to maintain a urine output (UOP) of 30–50 mL/h. If UOP >50 mL/h, decrease fluid rate by 20% for two consecutive hours.
- Calculate burn size using Lund and Browder chart. Clean and debride wounds if possible. Wrap burns (scalp, trunk, neck, extremities) in sterile gauze soaked with a 5% solution of Sulfamylon. Alternatively, burns may be dressed with sil-ver-impregnated nylon, covered with sterile gauze, and moistened with sterile water (this can be left on for as long as 7 days).
- In patients who cannot be evacuated for burn excision, as a bridge to surgical care, consider using silver sulfadiazine cream alternated twice daily with mafenide acetate (Sulfamylon) cream to provide antimicrobial penetration of thick burn eschar.
- Early and continuous nutrition is vital to wound healing. Patients who are able to eat may need supplementation to meet calorie goals. Provide approximately 35 kcal/kg/day to burned adults. Nasoenteric feeding should be high protein, low fat.
- Venous thromboembolism, infection, pressure ulcers, lines/tubes.
- En route care preparation.
6.3.4. Burn Injury Prevention at Sea
6.3.5. Burn Mass Casualty, Triage and the Prevention of Moral Injury
7. Back to the Future: Conclusions and Recommendations
- Implement regular Advanced Burn Life Support training or equivalent to all Navy Medicine providers, including Independent Duty Corpsmen [2].
- Role 1 and Role 2 providers must be provided routine clinical skills sustainment experience relevant to Burn, Trauma, and Critical Care, including a focus on spe-cific skill sets such as airway and ventilator management, resuscitation, sedation, and critical care procedural skills [2].
- Develop and implement a comprehensive whole blood capability across all Role 1 capable surface and subsurface vessels [2].
- Improve clinical documentation for patient care as well as submitting the clinical data from shipboard injuries to the Department of Defense Trauma Registry [4].
- Research and development efforts should focus on clothing, helmets, and perhaps “maritime body armor” to prevent thermal and blast injury from high-energy weapons systems.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Potenza, B.M. Burn, Inhalation, and Electrical Injuries. In Expeditionary Surgery at Sea: A Practical Approach; Springer: Berlin/Heidelberg, Germany, 2023; pp. 529–567. [Google Scholar]
- Tadlock, M.D.; Gurney, J.; Tripp, M.S.; Cancio, L.C.; Sise, M.J.; Bandle, J.; Cubano, M.; Lee, J.; Vasquez, M.; Acosta, J.A. Between the devil and the deep blue sea: A review of 25 modern naval mass casualty incidents with implications for future Distributed Maritime Operations. J. Trauma Acute Care Surg. 2021, 91 (Suppl. S2), S46–S55. [Google Scholar] [CrossRef] [PubMed]
- Vasquez, M.C.; Vicente, D.A.; Tadlock, M.D. Mechanisms of Injury During Modern Naval Operations. In Expeditionary Surgery at Sea: A Practical Approach; Springer: Berlin/Heidelberg, Germany, 2023; p. 53. [Google Scholar]
- Benham, D.A.; Vasquez, M.C.; Kerns, J.; Checchi, K.D.; Mullinax, R.; Edson, T.D.; Tadlock, M.D. Injury Trends aboard U.S. Navy Vessels: A 50-year analysis of Mishaps at Sea. J. Trauma Acute Care Surg. 2023, 95, S41–S49. [Google Scholar] [CrossRef] [PubMed]
- Watt, J. The injuries of four centuries of naval warfare. Ann. R. Coll. Surg. Engl. 1975, 57, 3–24. [Google Scholar]
- Watt, J. The burns of seafarers under oars, sail and steam. Injury 1980, 12, 69–81. [Google Scholar] [CrossRef]
- Arkin, W.M.; Handler, J. Naval Accidents, 1945–1988; Greenpeace Greenpeace/Institute for Policy Studies: Washington, DC, USA, 1989. [Google Scholar]
- Tadlock, M.D.; Hernandez, A.A.; Miller, B.T. The Ship’s Surgeon and Surgery at Sea: A Brief History. In Expeditionary Surgery at Sea: A Practical Approach; Springer: Berlin/Heidelberg, Germany, 2023; pp. 33–52. [Google Scholar]
- Paine, L. The Sea and Civilization: A Maritime History of the World; Atlantic Books Ltd.: London, UK, 2014. [Google Scholar]
- Pryor, J.H.; Jeffreys, E.M. Age of the Dromōn: The Byzantine Navy Ca 500-1204 (medieval Mediterranean, 0928-5520; V. 62); Brill Academic Publishers: Leiden, The Netherlands, 2006. [Google Scholar]
- Hale, J.R. Lords of the Sea: The Epic Story of the Athenian Navy and the Birth of Democracy; Penguin: London, UK, 2009. [Google Scholar]
- Admiral James Stavridis, U. Sea Power: The History and Geopolitics of the World’s Oceans; Penguin: London, UK, 2017. [Google Scholar]
- Mann, W.L. The origin and early development of naval medicine. US Nav. Inst. Proc. 1929, 55, 772–782. [Google Scholar]
- Walker, A.J. The ‘Walker dip’. J. R. Nav. Med. Serv. 2018, 104, 173–176. [Google Scholar] [CrossRef]
- Mann, W.L. Medical Tactics in Naval Warfare; US Government Printing Office: Washington, DC, USA, 1927. [Google Scholar]
- Wallace, A.F. The influence of the Battle of Jutland on plastic surgery. Clin. Plast Surg. 1983, 10, 657–663. [Google Scholar]
- Watt, J. Some forgotten contributions of naval surgeons. J. R. Soc. Med. 1985, 78, 753–762. [Google Scholar] [CrossRef]
- Council, N.R. Technology and the Evolution of Naval Warfare: 1851–2001; Lautenschläger, K., Ed.; The National Academies Press: Washington, DC, USA, 1984; 60p. [Google Scholar]
- Gauker, E.D.; Blood, C.G. Severity of Battle Injuries Occurring Aboard US Naval Warships. 1992. Available online: https://apps.dtic.mil/sti/tr/pdf/ADA258369.pdf (accessed on 11 July 2023).
- Blood, C.G. Analyses of battle casualties by weapon type aboard U.S. Navy warships. Mil Med. 1992, 157, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Mc, L.C., Jr. The treatment of major burns in naval warfare. Nebr. State Med. J. 1945, 31, 11–19. [Google Scholar]
- Lane, D.A. Hospital ship doctrine in the United States Navy: The Halsey effect on scoop- and-sail tactics. Mil. Med. 1997, 162, 388–395. [Google Scholar] [CrossRef]
- Chapter 12, Damage Control. In Navy Basic Military Requirements, NAVEDTRA 14325. Available online: https://media.defense.gov/2014/Feb/21/2002655450/-1/-1/1/140221-N-ZZ182-5359.pdf (accessed on 17 November 2023).
- Joint Trauma System, Tactical Combat Casualty Care Guidelines. Available online: https://deployedmedicine.com/market/31/content/40 (accessed on 11 July 2023).
- OPNAVINST 1500.86. Tactical Combat Casualty Care Training. 12 April 2021. Available online: https://www.secnav.navy.mil/doni/Directives/01000%20Military%20Personnel%20Support/01-500%20Military%20Training%20and%20Education%20Services/1500.86.pdf (accessed on 19 November 2023).
- Butler, F.K.; Burkholder, T.; Chernenko, M.; Chimiak, J.; Chung, J.; Cubano, M.; Gurney, J.; Hall, A.B.; Holcomb, J.B.; Kotora, J.; et al. Tactical Combat Casualty Care Maritime Scenario: Shipboard Missile Strike. J. Spec. Oper. Med. 2022, 22, 9–28. [Google Scholar] [CrossRef]
- Butler, F.K., Jr.; Giebner, S. Tactical Combat Casualty Care Skill Sets by Responder Level. 22 April 2019. J. Spec. Oper. Med. 2019, 19, 143–145. [Google Scholar] [CrossRef] [PubMed]
- Major Fires Review. Available online: https://www.secnav.navy.mil/foia/readingroom/HotTopics/BHR%20and%20MFR%20Investigations/For%20Release%20Major%20Fires%20Review%20(19%20Oct%2021).pdf (accessed on 13 July 2023).
- 21 Hospitalized with Injuries from Fire, Explosion on USS Bonhomme Richard at Naval Base San Diego. Available online: https://www.cbs8.com/article/news/local/uss-bonhomme-richard-on-fire-at-naval-base-san-diego/509-6aec1280-f709-4e88-b9ee-2d393f942467 (accessed on 13 July 2023).
- Navy Report Blames Crew for Devastating Fire on the Bonhomme Richard. Available online: https://www.bbc.com/news/world-us-canada-58975431# (accessed on 13 July 2023).
- Perez, K.G.; Eskridge, S.L.; Clouser, M.C.; Cancio, J.M.; Cancio, L.C.; Galarneau, M.R. Burn injuries in US service members: 2001–2018. Burns 2023, 49, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Thomas, T.L.; Parker, A.L.; Horn, W.G.; Mole, D.; Spiro, T.R.; Hooper, T.I.; Garland, F.C. Accidents and injuries among U.S. Navy crewmembers during extended submarine patrols, 1997 to 1999. Mil. Med. 2001, 166, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Chapman, T.T.; Richard, R.L.; Hedman, T.L.; Renz, E.M.; Wolf, S.E.; Holcomb, J.B. Combat casualty hand burns: Evaluating impairment and disability during recovery. J. Hand. Ther. 2008, 21, 150–158; quiz 159. [Google Scholar] [CrossRef] [PubMed]
- Pinkstaff, C.A.; Sturtz, D.L.; Bellamy, R.F. USS Franklin and the USS Stark–recurrent problems in the prevention and treatment of naval battle casualties. Mil. Med. 1989, 154, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Davis, T.P.; Alexander, B.A.; Lambert, E.W.; Simpson, R.B.; Unger, D.V.; Lee, J.; Snyder, M.L.; Liston, W.A. Distribution and care of shipboard blast injuries (USS Cole DDG-67). J. Trauma 2003, 55, 1022–1027; discussion 1027–1028. [Google Scholar] [CrossRef]
- Langworthy, M.J.; Sabra, J.; Gould, M. Terrorism and blast phenomena: Lessons learned from the attack on the USS Cole (DDG67). Clin. Orthop. Relat. Res. 2004, 422, 82–87. [Google Scholar] [CrossRef]
- Lippold, K.S. Front Burner: Al Qaeda’s Attack on the USS Cole, 1st ed.; PublicAffairs: New York, NY, USA, 2012. [Google Scholar]
- Webster, T.; Mancini, J. Lessons Learned or Lessons Observed: The U.S. Navy’s Relationship with Mine Warfare. Available online: https://warontherocks.com/2023/08/lessons-learned-of-lessons-observed-the-u-s-navys-relationship-with-mine-warfare/ (accessed on 31 August 2023).
- Peniston, B. The Day Frigate Samuel B. Roberts Was Mined. Available online: https://news.usni.org/2015/05/22/the-day-frigate-samuel-b-roberts-was-mined (accessed on 30 September 2023).
- Stilwell, B. The Captain of a Navy Frigate Saved His Sinking Ship by Not Fighting a Fire. Available online: https://www.military.com/history/captain-of-navy-frigate-saved-his-sinking-ship-not-fighting-fire.html (accessed on 30 September 2023).
- British Ships Lost & Damaged. Available online: https://www.naval-history.net/F62-Falklands-British_ships_lost (accessed on 15 October 2020).
- Ryan, J. The Falklands war-triage. Ann. R. Coll. Surg. Engl. 1984, 66, 195. [Google Scholar]
- Marsh, A.R. A short but distant war—The Falklands campaign. J. R. Soc. Med. 1983, 76, 972–982. [Google Scholar] [CrossRef] [PubMed]
- Rylah, O.; Smith, J. The early management of the burned patient in the Naval service. BMJ Spec. J. 2015, 101, 55–62. [Google Scholar] [CrossRef]
- Loss of HMS SHEFFIELD-Board of Inquiry. 28 May 1982. Available online: http://www.admiraltytrilogy.com/read/BOI_Rpt_HMS_Sheffield_May82.pdf (accessed on 15 July 2023).
- Military and Security Developments Involving the People’s Republic of China—2023 Annual Report to Congress. Available online: https://media.defense.gov/2023/Oct/19/2003323409/-1/-1/1/2023-MILITARY-AND-SECURITY-DEVELOPMENTS-INVOLVING-THE-PEOPLES-REPUBLIC-OF-CHINA.PDF (accessed on 18 November 2023).
- Active in Commission—Naval Vessel Register. Available online: https://www.nvr.navy.mil/NVRSHIPS/ACTIVEINCOMMISSION.HTML (accessed on 18 November 2023).
- Advantage at Sea: Prevailing with Integrated All-Domain Naval Power, U.S. Department of Defense. Available online: https://media.defense.gov/2020/Dec/16/2002553074/-1/-1/0/ (accessed on 12 July 2023).
- Chief of Naval Operations Admiral Michael Gilday, “Statement of Admiral Michael M. Gilday, Chief of Naval Operations on the Posture of the United States Navy Before the House Armed Services Committee”, U.S. House Armed Services Committee, p. 7. Available online: https://docs.house.gov/meetings/AS/AS00/20210615/112796/HHRG-117-AS00-Wstate-GildayM-20210615.pdf (accessed on 13 July 2023).
- Prolonged Casualty Care Guidelines (PCC)—CPG ID 91. Available online: https://jts.health.mil/assets/docs/cpgs/Prolonged_Casualty_Care_Guidelines_21_Dec_2021_ID91.pdf (accessed on 11 July 2023).
- Remley, M.A.; Riesberg, J.C.; Drew, B.; Deaton, T.G.; Montgomery, H.R.; Jensen, S.D.; Gurney, J.M. Committee on Tactical Combat Casualty Care and Prolonged Casualty Care Working Group Consensus Statement. J. Spec. Oper. Med. 2023, 23, 124–125. [Google Scholar] [CrossRef] [PubMed]
- Joint Trauma System, Committee on Surgical Combat Casualty Care March 22–23, 2023 Meeting Minutes. Available online: https://jts.health.mil/index.cfm/committees/cosccc/mtg_minutes (accessed on 19 November 2023).
- Lesperance, R.N.; Adamson, S.; Gurney, J.M. Lessons Learned During Prolonged Care of Combat Casualties by a Minimally Manned Surgical Team. Mil. Med. 2023, 188, e1389–e1394. [Google Scholar] [CrossRef] [PubMed]
- Doyle, G.; Herzinger, B. Carrier Killer: China’s Anti-ship Ballistic Missiles and Theater of Operations in the Early 21st Century; Helion Limited: Warwick, UK, 2022. [Google Scholar]
- Edwards, C. Fire DOWN BELOW! Nav. Hist. 2011, 25, 58. [Google Scholar]
- Department of the Navy. Manual of the Judge Advocate General: Basic Final Investigative Report Concerning the Fire on Board the USS Forrestal (CVA 59); United States Navy: Washington, DC, USA, 1967. [Google Scholar]
- Cox, S.J. H-025-2: The USS Enterprise (CVAN-65) Conflagration, 14 January 1969. Naval History and Heritage Command. Available online: https://www.history.navy.mil/about-us/leadership/director/directors-corner/h-grams/h-gram-025/h-025-2.html (accessed on 30 April 2023).
- Gurney, J.; Tadlock, M.D.; Cancio, L.C. Burn Injuries from a military perspective. Curr. Trauma Rep. 2022, 8, 113–126. [Google Scholar] [CrossRef]
- Payne, R.; Glassman, E.; Turman, M.L.; Cancio, L.C. Pathophysiology and Treatment of Burns. J. Spec. Oper. Med. 2022, 22, 87–92. [Google Scholar] [CrossRef]
- King, B.; Cancio, L.C.; Jeng, J.C. Military Burn Care and Burn Disasters. Surg. Clin. N. Am. 2023, 103, 529–538. [Google Scholar] [CrossRef]
- Santaniello, J.M.; Luchette, F.A.; Esposito, T.J.; Gunawan, H.; Reed, R.L.; Davis, K.A.; Gamelli, R.L. Ten year experience of burn, trauma, and combined burn/trauma injuries comparing outcomes. J. Trauma Acute Care Surg. 2004, 57, 696–701. [Google Scholar] [CrossRef]
- Suresh, M.; Pruskowski, K.A.; Rizzo, J.A.; Gurney, J.M.; Cancio, L.C. Characteristics and outcomes of patients with inhalation injury treated at a military burn center during U.S. combat operations. Burns 2020, 46, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Falciola, V.; Waisel, D.B. Surgical and Anesthetic Challenges aboard Non-Hospital Ships in the Pacific during World War II. J. Anesth. Hist. 2018, 4, 214–221. [Google Scholar] [CrossRef]
- Beecher, H.K. Preparation of Battle Casualties for Surgery. Ann. Surg. 1945, 121, 769–792. [Google Scholar] [CrossRef]
- Gurney, J.M.; Kozar, R.A.; Cancio, L.C. Plasma for burn shock resuscitation: Is it time to go back to the future? Transfusion 2019, 59, 1578–1586. [Google Scholar] [CrossRef]
- Spinella, P.C.; Perkins, J.G.; Grathwohl, K.W.; Beekley, A.C.; Holcomb, J.B. Warm fresh whole blood is independently associated with improved survival for patients with combat-related traumatic injuries. J. Trauma 2009, 66 (Suppl. S4), S69. [Google Scholar] [CrossRef]
- Kauvar, D.S.; Holcomb, J.B.; Norris, G.C.; Hess, J.R. Fresh whole blood transfusion: A controversial military practice. J. Trauma Acute Care Surg. 2006, 61, 181–184. [Google Scholar] [CrossRef]
- Naumann, D.N.; Boulton, A.J.M.; Sandhu, A.M.; Campbell, K.M.; Charlton, W.B.; Gurney, J.M.; Martin, M.J.; Scorer, T.; Doughty, H. Fresh whole blood from walking blood banks for patients with traumatic hemorrhagic shock: A systematic review and meta-analysis. J. Trauma Acute Care Surg. 2020, 89, 792–800. [Google Scholar] [CrossRef]
- Gurney, J.M.; Staudt, A.M.; del Junco, D.J.; Shackelford, S.A.; Mann-Salinas, E.A.; Cap, A.P.; Spinella, P.C.; Martin, M.J. Whole blood at the tip of the spear: A retrospective cohort analysis of warm fresh whole blood resuscitation versus component therapy in severely injured combat casualties. Surgery 2022, 171, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Shackelford, S.A.; Gurney, J.M.; Taylor, A.L.; Keenan, S.; Corley, J.B.; Cunningham, C.W.; Drew, B.G.; Jensen, S.D.; Kotwal, R.S.; Montgomery, H.R.; et al. Joint trauma system, defense committee on trauma, and armed services blood program consensus statement on whole blood. Transfusion 2021, 61, S333–S335. [Google Scholar] [CrossRef] [PubMed]
- Talmy, T.; Malkin, M.; Esterson, A.; Yazer, M.H.; Sebbag, A.; Shina, A.; Shinar, E.; Glassberg, E.; Gendler, S.; Almog, O. Low-titer group O whole blood in military ground ambulances: Lessons from the Israel Defense Forces initial experience. Transfus. Med. 2023. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Levin, D.; Zur, M.; Shinar, E.; Moshe, T.; Tsur, A.M.; Nadler, R.; Yazer, M.H.; Epstein, D.; Avital, G.; Gelikas, S.; et al. Low-Titer Group O Whole-Blood Resuscitation in the Prehospital Setting in Israel: Review of the First 2.5 Years’ Experience. Transfus. Med. Hemother. 2021, 48, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.D.; Miles, E.A.; Broussard, M.A.; Corley, J.B.; Knight, R.; Remley, M.A.; Cap, A.P.; Gurney, J.M.; Shackelford, S.A. Low titer group O whole blood resuscitation: Military experience from the point of injury. J. Trauma Acute Care Surg. 2020, 89, 834–841. [Google Scholar] [CrossRef] [PubMed]
- Vanderspurt, C.K.; Spinella, P.C.; Cap, A.P.; Hill, R.; Matthews, S.A.; Corley, J.B.; Gurney, J.M. The use of whole blood in US military operations in Iraq, Syria, and Afghanistan since the introduction of low-titer Type O whole blood: Feasibility, acceptability, challenges. Transfusio 2019, 59, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Martinaud, C.; Fleuriot, E.; Pasquier, P. Implementation of Low Titer Whole Blood for French overseas operations: O positive or negative products in massive hemorrhage? Transfus Clin. Biol. 2022, 29, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Brill, J.B.; Tang, B.; Hatton, G.; Mueck, K.M.; McCoy, C.C.; Kao, L.S.; Cotton, B.A. Impact of Incorporating Whole Blood into Hemorrhagic Shock Resuscitation: Analysis of 1377 Consecutive Trauma Patients Receiving Emergency-Release Uncrossmatched Blood Products. J. Am. Coll. Surg. 2022, 234, 408–418. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.; Merutka, N.; Meyer, D.; Bai, Y.; Prater, S.; Cabrera, R.; Holcomb, J.B.; Wade, C.E.; Love, J.D.; Cotton, B.A. Safety profile and impact of low-titer group O whole blood for emergency use in trauma. J. Trauma Acute Care Surg. 2020, 88, 87–93. [Google Scholar] [CrossRef]
- Gallaher, J.R.; Dixon, A.; Cockcroft, A.; Grey, M.; Dewey, E.; Goodman, A.; Schreiber, M. Large volume transfusion with whole blood is safe compared with component therapy. J. Trauma Acute Care Surg. 2020, 89, 238–245. [Google Scholar] [CrossRef]
- Bohan, P.M.K.; McCarthy, P.M.; Wall, M.E.B.; Adams, A.M.; Chick, R.C.; Forcum, J.E.; Radowsky, J.S.; How, R.A.; Sams, V.G. Safety and efficacy of low-titer O whole blood resuscitation in a civilian level I trauma center. J. Trauma Acute Care Surg. 2021, 91 (Suppl. S2), S162–S168. [Google Scholar] [CrossRef]
- Ngatuvai, M.; Zagales, I.; Sauder, M.; Andrade, R.; Santos, R.; Bilski, T.; Kornblith, L.; Elkbuli, A. Outcomes of Transfusion With Whole Blood, Component Therapy, or Both in Adult Civilian Trauma Patients: A Systematic Review and Meta-Analysis. J. Surg. Res. 2023, 287, 193–201. [Google Scholar] [CrossRef]
- Brill, J.B.; Mueck, K.M.; Tang, B.; Sandoval, M.; Cotton, M.E.; Cameron McCoy, C.; Cotton, B.A. Is Low-Titer Group O Whole Blood Truly a Universal Blood Product? J. Am. Coll. Surg. 2023, 236, 506–513. [Google Scholar] [CrossRef]
- Shea, S.M.; Mihalko, E.P.; Lu, L.; Thomas, K.A.; Schuerer, D.; Brown, J.B.; Bochicchio, G.V.; Spinella, P.C. Doing more with less: Low-titer group O whole blood resulted in less total transfusions and an independent association with survival in adults with severe traumatic hemorrhage. J. Thromb. Haemost. 2023. online ahead of print. [Google Scholar] [CrossRef]
- Sperry, J.L.M.; A Cotton, B.; Luther, J.F.; Cannon, J.W.; A Schreiber, M.; Moore, E.E.; Namias, N.; Minei, J.P.; Wisniewski, S.R.; Guyette, F.X. Whole Blood Resuscitation and Association with Survival in Injured Patients with an Elevated Probability of Mortality. J. Am. Coll. Surg. 2023, 237, 206–219. [Google Scholar] [CrossRef]
- Guyette, F.X.; Zenati, M.; Triulzi, D.J.; Yazer, M.H.; Skroczky, H.B.; Early, B.J.B.; Adams, P.W.B.; Brown, J.B.M.; Alarcon, L.; Neal, M.D.; et al. Prehospital low titer group O whole blood is feasible and safe: Results of a prospective randomized pilot trial. J. Trauma Acute Care Surg. 2022, 92, 839–847. [Google Scholar] [CrossRef]
- Lee, J.S.; Khan, A.D.; Wright, F.L.; McIntyre, R.C.; Dorlac, W.C.; Cribari, C.; Brockman, V.; Vega, S.A.; Cofran, J.M.; Schroeppel, T.J. Whole Blood Versus Conventional Blood Component Massive Transfusion Protocol Therapy in Civilian Trauma Patients. Am. Surg. 2022, 88, 880–886. [Google Scholar] [CrossRef] [PubMed]
- Braverman, M.A.; Smith, A.; Pokorny, D.; Axtman, B.; Shahan, C.P.; Barry, L.; Corral, H.; Jonas, R.B.; Shiels, M.; Schaefer, R.; et al. Prehospital whole blood reduces early mortality in patients with hemorrhagic shock. Transfusion 2021, 61 (Suppl. S1), S15–S21. [Google Scholar] [CrossRef] [PubMed]
- Shea, S.M.; Staudt, A.M.; Thomas, K.A.; Schuerer, D.; Mielke, J.E.; Folkerts, D.; Lowder, E.; Martin, C.; Bochicchio, G.V.; Spinella, P.C. The use of low-titer group O whole blood is independently associated with improved survival compared to component therapy in adults with severe traumatic hemorrhage. Transfusion 2020, 60 (Suppl. S3), S2–S9. [Google Scholar] [CrossRef]
- Greenhalgh, D.G.; Cartotto, R.; Taylor, S.L.; Fine, J.R.; Lewis, G.M.; Smith, D.J., Jr.; Marano, M.A.; Gibson, A.; Wibbenmeyer, L.A.; Holmes, J.H.; et al. Burn Resuscitation Practices in North America: Results of the Acute Burn ResUscitation Multicenter Prospective Trial (ABRUPT). Ann. Surg. 2023, 277, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Cartotto, R.; Burmeister, D.M.; Kubasiak, J.C. Burn Shock and Resuscitation: Review and State of the Science. J. Burn Care Res. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Burn Care—CPG ID: 12. Available online: https://jts.health.mil/assets/docs/cpgs/Burn_Care_11_May_2016_ID12.pdf (accessed on 11 July 2023).
- Navickis, R.J.; Greenhalgh, D.G.; Wilkes, M.M. Albumin in Burn Shock Resuscitation: A Meta-Analysis of Controlled Clinical Studies. J. Burn Care Res. 2016, 37, e268–e278. [Google Scholar] [CrossRef]
- Eljaiek, R.; Heylbroeck, C.; Dubois, M.J. Albumin administration for fluid resuscitation in burn patients: A systematic review and meta-analysis. Burns 2017, 43, 17–24. [Google Scholar] [CrossRef]
- Human albumin administration in critically ill patients: Systematic review of randomised controlled trials. BMJ 1998, 317, 235–240. [CrossRef]
- Offringa, M. Excess mortality after human albumin administration in critically ill patients. Clinical and pathophysiological evidence suggests albumin is harmful. BMJ 1998, 317, 223–224. [Google Scholar] [CrossRef]
- Greenhalgh, D.G. Burn resuscitation: The results of the ISBI/ABA survey. Burns 2010, 36, 176–182. [Google Scholar] [CrossRef]
- Finfer, S.; Bellomo, R.; Boyce, N.; French, J.; Myburgh, J.; Norton, R. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N. Engl. J. Med. 2004, 350, 2247–2256. [Google Scholar] [PubMed]
- Cooper, D.J.; Myburgh, J.; Heritier, S.; Finfer, S.; Bellomo, R.; Billot, L.; Murray, L.; Vallance, S.; SAFE-TBI Investigators. Albumin resuscitation for traumatic brain injury: Is intracranial hypertension the cause of increased mortality? J. Neurotrauma 2013, 30, 512–518. [Google Scholar] [CrossRef]
- Polk, T.M.; Gurney, J.M.; Riggs, L.E.; Cannon, J.W.; Cap, A.P.; Friedrichs, G.P.A. Dried Plasma: An Urgent Priority for Trauma Readiness. J. Trauma Acute Care Surg. 2023, 95, S4–S6. [Google Scholar] [CrossRef]
- Inaba, K.; Branco, B.C.; Rhee, P.; Blackbourne, L.H.; Holcomb, J.B.; Teixeira, P.G.; Shulman, I.; Nelson, J.; Demetriades, D. Impact of plasma transfusion in trauma patients who do not require massive transfusion. J. Am. Coll. Surg. 2010, 210, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Zander, A.L.; Olson, E.J.; Van Gent, J.-M.; Bandle, J.; Calvo, R.Y.; Shackford, S.R.; Peck, K.A.; Sise, C.B.; Sise, M.J.; King, B.S. Does resuscitation with plasma increase the risk of venous thromboembolism? J. Trauma Acute Care Surg. 2015, 78, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Sarani, B.; Dunkman, W.J.; Dean, L.; Sonnad, S.; Rohrbach, J.I.; Gracias, V.H. Transfusion of fresh frozen plasma in critically ill surgical patients is associated with an increased risk of infection. Crit. Care Med. 2008, 36, 1114–1118. [Google Scholar] [CrossRef]
- Watson, G.A.; Sperry, J.L.; Rosengart, M.R.; Minei, J.P.; Harbrecht, B.G.; Moore, E.E.; Cuschieri, J.; Maier, R.V.; Billiar, T.R.; Peitzman, A.B. Fresh Frozen Plasma Is Independently Associated With a Higher Risk of Multiple Organ Failure and Acute Respiratory Distress Syndrome. J. Trauma Acute Care Surg. 2009, 67, 221–230. [Google Scholar] [CrossRef]
- O’Mara, M.S.; Slater, H.; Goldfarb, I.W.; Caushaj, P.F. A prospective, randomized evaluation of intra-abdominal pressures with crystalloid and colloid resuscitation in burn patients. J. Trauma 2005, 58, 1011–1018. [Google Scholar] [CrossRef]
- Lindsey, L.; Purvis, M.V.; Miles, D.; Lintner, A.; Scott, V.; McGinn, K.; Bright, A.; Kahn, S.A. An Adjusted Ideal Body Weight Index Formula With Fresh Frozen Plasma (FFP) Rescue Decreases Fluid Creep During Burn Resuscitation. Ann. Burn. Fire Disasters 2020, 33, 216–223. [Google Scholar]
- Vural, S.; Yasti, C.A.; Dolapçı, M. Comparison of Albumin and Fresh Frozen Plasma as Colloid Therapy in Patients With Major Burns. Cureus 2023, 15, e33485. [Google Scholar] [CrossRef]
- Jones, L.M.; Deluga, N.; Bhatti, P.; Scrape, S.R.; Bailey, J.K.; Coffey, R.A. TRALI following fresh frozen plasma resuscitation from burn shock. Burns 2017, 43, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.T.; Lin, A.H.; Clark, S.C.; Cap, A.P.; Dubose, J.J. Red tides: Mass casualty and whole blood at sea. J. Trauma Acute Care Surg. 2018, 85 (Suppl. S2), S134–S139. [Google Scholar] [CrossRef]
- Wallace, J.; Jensen, G.; Camelo, M.; Vicente, D.A. Damage Control Resuscitation and the Walking Blood Bank. In Expeditionary Surgery at Sea: A Practical Approach; Springer: Berlin/Heidelberg, Germany, 2023; pp. 463–477. [Google Scholar]
- Cartotto, R.; Callum, J. A Review on the Use of Plasma During Acute Burn Resuscitation. J. Burn Care Res. 2020, 41, 433–440. [Google Scholar] [CrossRef]
- Marshall, J.C.; Bosco, L.; Adhikari, N.K.; Connolly, B.; Diaz, J.V.; Dorman, T.; Fowler, R.A.; Meyfroidt, G.; Nakagawa, S.; Pelosi, P.; et al. What is an intensive care unit? A report of the task force of the World Federation of Societies of Intensive and Critical Care Medicine. J. Crit. Care 2017, 37, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, L.M.; Biester, T.W.; Jurkovich, G.J.; Buyske, J.; Malangoni, M.A.; Lewis, F.R., Jr.; Members of the Trauma, Burns and Critical Care Board of the American Board of Surgery. General surgery resident rotations in surgical critical care, trauma, and burns: What is optimal for residency training? Am. J. Surg. 2016, 212, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Dalton, M.K.; Remick, K.N.; Mathias, M.; Trinh, Q.-D.; Cooper, Z.; Elster, E.A.; Weissman, J.S. Analysis of surgical volume in military medical treatment facilities and clinical combat readiness of US military surgeons. JAMA Surg. 2022, 157, 43–50. [Google Scholar] [CrossRef]
- Tobin, J.M.; Via, D.K.; Carter, T. Tactical evacuation: Extending critical care on rotary wing platforms to forward surgical facilities. Mil Med. 2011, 176, 4–6. [Google Scholar] [CrossRef]
- Tobin, J.M.; Nelson, T.J.; Moore, J.D. It is time to reassess critical care evacuation. J. Trauma Acute Care Surg. 2014, 76, 250. [Google Scholar] [CrossRef]
- Tobin, J.M.; Reid, C.; Burns, B.J. Multidisciplinary prehospital critical care. J. Trauma Acute Care Surg. 2020, 89, e188–e189. [Google Scholar] [CrossRef] [PubMed]
- Ingalls, N.; Zonies, D.; Bailey, J.A.; Martin, K.D.; Iddins, B.O.; Carlton, P.K.; Hanseman, D.; Branson, R.; Dorlac, W.; Johannigman, J. A review of the first 10 years of critical care aeromedical transport during operation iraqi freedom and operation enduring freedom: The importance of evacuation timing. JAMA Surg. 2014, 149, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Savell, S.C.; Howard, J.T.; A VanFosson, C.; Medellín, K.L.; Staudt, A.M.; Rizzo, J.A.; Maddry, J.K.; Cancio, L.C. A Retrospective Cohort Study of Burn Casualties Transported by the US Army Burn Flight Team and US Air Force Critical Care Air Transport Teams. Mil. Med. 2022. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Cancian, M.F.; Cancian, M.; Heginbotham, E. First Battle of the Next War: Wargaming a Chinese Invasion of Taiwan; Center for Strategic and International Studies: Washington, DC, USA, 2023. [Google Scholar]
- Springer, J.A. Inferno: The Epic Life and Death Struggle of the USS Franklin in World War II; Zenith Press: Minneapolis, MI, USA, 2011. [Google Scholar]
- McDonald, V.S.; Ignacio, R.C.; Kuettel, M.A.; Schlitzkus, L.L.; Sullivan, M.E.; Edsoock, M.D. Practical bioethics for the humanitarian surgeon: The development, implementation and assessment of an ethics curriculum for residents participating in humanitarian missions. J. Surg. Educ. 2020, 77, 390–403. [Google Scholar] [CrossRef]
- McDonald, V.S.; Tadlock, M.D. Practical Bioethical Principles in the Deployed Maritime Environment. In Expeditionary Surgery at Sea: A Practical Approach; Springer: Berlin/Heidelberg, Germany, 2023; pp. 711–720. [Google Scholar]
- Kotwal, R.S.; Scott, L.L.; Janak, J.C.; Tarpey, B.W.; Howard, J.T.; Mazuchowski, E.L.; Butler, F.K.; Shackelford, S.A.; Gurney, J.M.; Stockinger, Z.T. The effect of prehospital transport time, injury severity, and blood transfusion on survival of US military casualties in Iraq. J. Trauma Acute Care Surg. 2018, 85, S112–S121. [Google Scholar] [CrossRef]
- Gurney, J.; Staudt, A.; Cap, A.; Shackelford, S.; Mann-Salinas, E.; Le, T.; Nessen, S.; Spinella, P. Improved survival in critically injured combat casualties treated with fresh whole blood by forward surgical teams in Afghanistan. Transfusion 2020, 60 (Suppl. S3), S180–S188. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Responder Level | Provider Type | TCCC Skill Examples | TCCC Burn Injury Intervention |
|---|---|---|---|
| Tier 1 | All service members | Basic life-threatening assessment to include hemorrhage, airway, and respirations. Basic hemorrhage control (e.g., direct pressure, packing, extremity tourniquet) Basic airway maneuvers (e.g., sit up/lean forward, jaw thrust) Care under fire/threat | Stop the burning process. Basic burn assessment: assess and treat as a trauma casualty with burns and not burn casualty with injuries. Facial burns, especially those that occur in closed spaces, may be associated with inhalation injury. Aggressively monitor airway status and oxygen saturation in such patients. Estimate total body surface area (TBSA) burned to the nearest 10% using the Rule of Nines. Apply dressing to burns: cover the burn area with dry, sterile dressings. All TCCC interventions can be performed on or through burned skin in a burn casualty. Burn patients are particularly susceptible to hypothermia. Extra emphasis should be placed on barrier heat loss prevention methods, particularly in those with extensive burns (>20%). |
| Tier 2 | Combat lifesaver | All Tier 1 skills Tactical evacuation care | Same as Tier 1 skills |
| Tier 3 | Combat Medic or Hospital Corpsman | All Tier 2 skills Triage Lifesaving interventions to include triage, junctional tourniquet application, use of airway adjuncts, cricothyroidotomy, oxygen administration, shock and burn resuscitation, and fracture management | Consider early surgical airway for respiratory distress or oxygen desaturation in patients with facial burns and/or at risk of inhalation injury. Burn fluid resuscitation using the Rule of Ten: initial IV/IO fluid rate is calculated as %TBSA × 10 mL/h for adults weighing 40–80 kg. For every 10 kg ABOVE 80 kg, increase initial rate by 100 mL/h. If burns are greater than 20% of TBSA, fluid resuscitation should be initiated as soon as IV/IO access is established. Resuscitation should be initiated with lactated Ringer’s, normal saline, or Hextend (if available). If Hextend is used, no more than 1000 mL should be given, followed by lactated Ringer’s or normal saline as needed. If hemorrhagic shock is also present, resuscitation for hemorrhagic shock takes precedence over resuscitation for burn shock. Administer IV/IO fluids per the TCCC guidelines Prehospital antibiotic therapy is not indicated solely for burns, but antibiotics should be given per the TCCC guidelines if indicated to prevent infection in penetrating wounds. |
| Tier 4 | Combat paramedic or provider (including physicians, physician assistants, and Independent Duty Corpsman) | All Tier 3 skills Advanced lifesaving interventions such as endotracheal intubation and tube or finger thoracostomy | Same as Tier 3 skills |
| Burn Injury Mechanism | Casualties (N) | Mortality (%) ** | Most Recent Occurrence |
|---|---|---|---|
| Fire/burn/smoke inhalation (103 events) | 923 | 13 | 2018 |
| Explosion (16 events) | 106 | 60.4 | 2003 |
| Chemical exposure/inhalation injury (27 events) | 104 | 27.9 | 2004 |
| Electrocution | 32 | 90.6 | 2018 |
| Ordinance-related mishap | 24 | 37.5 | 2004 |
| Collision (14 events) *** | 275 | 40.3 | 2017 |
| Year | Ship | War/Conflict | Mechanism | Estimated Crew | Casualties (%) | Mortality (%) ** |
|---|---|---|---|---|---|---|
| 1972 | USS Goldsborough (DDG-20) | Vietnam War | Coastal artillery fire | 354 | 5 (1.4) | 3 (60) |
| 1987 | USS Stark (FFG-31) | Iran–Iraq War | Exocet missile attack | 220 | 58 (15.6) | 37 (63.8) |
| 1988 | USS Samuel B. Roberts (FFG-58) | Iran–Iraq War | Naval mine | 205 | 10 (4.9) | 0 |
| 1991 | USS Princeton (CG-59) | Operation Desert Storm | Naval mine | 330 | 3 (0.9) | 0 |
| 1991 | USS Tripoli (LPH-10) | Operation Desert Storm | Naval mine | 2358 | 4 (0.17) | 0 |
| 2000 | USS Cole (DDG-67) | Terrorist attack | WBIED | 338 | 54 (16) | 17 (31.5) |
| Totals | 3805 | 134 (3.5%) | 57 (42.5) | |||
| Year | Ship | War/Location | Crew | Location/Cause | Casualties (%) | Mortality (%) * |
|---|---|---|---|---|---|---|
| 1954 | USS Bennington (CVA 20) | Rhode Island | 2600 | Catapult malfunction and explosion | 201 (7.7) | 103 (51.2) |
| 1966 | USS Oriskany (CVA 34) | Vietnam War | 3400 | Forward Hangar Deck, flare | 200 (5.9) | 44 (22) |
| 1967 | USS Forrestal (CVA 59) | Vietnam War | 5500 | Flight Deck, ordinance related | 295 (5.4) | 134 (45.4) |
| 1969 | USS Enterprise (CVN 65) | Hawaii | 5162 | Flight Deck, ordinance related | 343 (6.6) | 28 (8.2) |
| Ship Type | # Ships | Standard Crew Complement | Casualties per Ship | Injured Survivors | Burn Injuries in Survivors | Medical Capabilities |
|---|---|---|---|---|---|---|
| Aircraft Carrier (CVN) | 2 | 5500 Total: 11,000 | 2718; 62% Fatal Total: 5436 | 1030 Total: 2060 | 309 Total 618 | Physicians ………………………5 Nurses……………………………1 Corpsman………………………30 Ward Beds………………………52 Intensive Care Unit Beds………3 Operating Room Beds…………..1 Battle Dressing Stations………..6 |
| Destroyer (DDG) | 8 | 314 Total: 2512 | 136; 39% Fatal Total: 1088 | 83 Total: 664 | 25 Total: 200 | Independent Duty Corpsman….1 Corpsman………………………..3 Ward Beds………………………..2 Battle Dressing Stations…………2 |
| Cruiser (CG) | 3 | 376 Total: 1128 | 162; 39% Fatal Total: 486 | 99 Total: 297 | 30 Total: 90 | Independent Duty Corpsman….1 Corpsman………………………..3 Ward Beds……………………….2 Battle Dressing Stations………..2 |
| Totals (%) | 13 | 14,640 | 7010; 57% Fatal | 3021 | 908 (30%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tadlock, M.D.; Edson, T.D.; Cancio, J.M.; Flieger, D.M.; Wickard, A.S.; Grimsley, B.; Gustafson, C.G.; Yelon, J.A.; Jeng, J.C.; Gurney, J.M. War at Sea: Burn Care Challenges—Past, Present and Future. Eur. Burn J. 2023, 4, 605-630. https://doi.org/10.3390/ebj4040041
Tadlock MD, Edson TD, Cancio JM, Flieger DM, Wickard AS, Grimsley B, Gustafson CG, Yelon JA, Jeng JC, Gurney JM. War at Sea: Burn Care Challenges—Past, Present and Future. European Burn Journal. 2023; 4(4):605-630. https://doi.org/10.3390/ebj4040041
Chicago/Turabian StyleTadlock, Matthew D., Theodore D. Edson, Jill M. Cancio, Dana M. Flieger, Aaron S. Wickard, Bailey Grimsley, Corey G. Gustafson, Jay A. Yelon, James C. Jeng, and Jennifer M. Gurney. 2023. "War at Sea: Burn Care Challenges—Past, Present and Future" European Burn Journal 4, no. 4: 605-630. https://doi.org/10.3390/ebj4040041