
Efficacy and Complications Associated with Acellular Dermal Substitute Use in the Treatment of Acute Burns: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
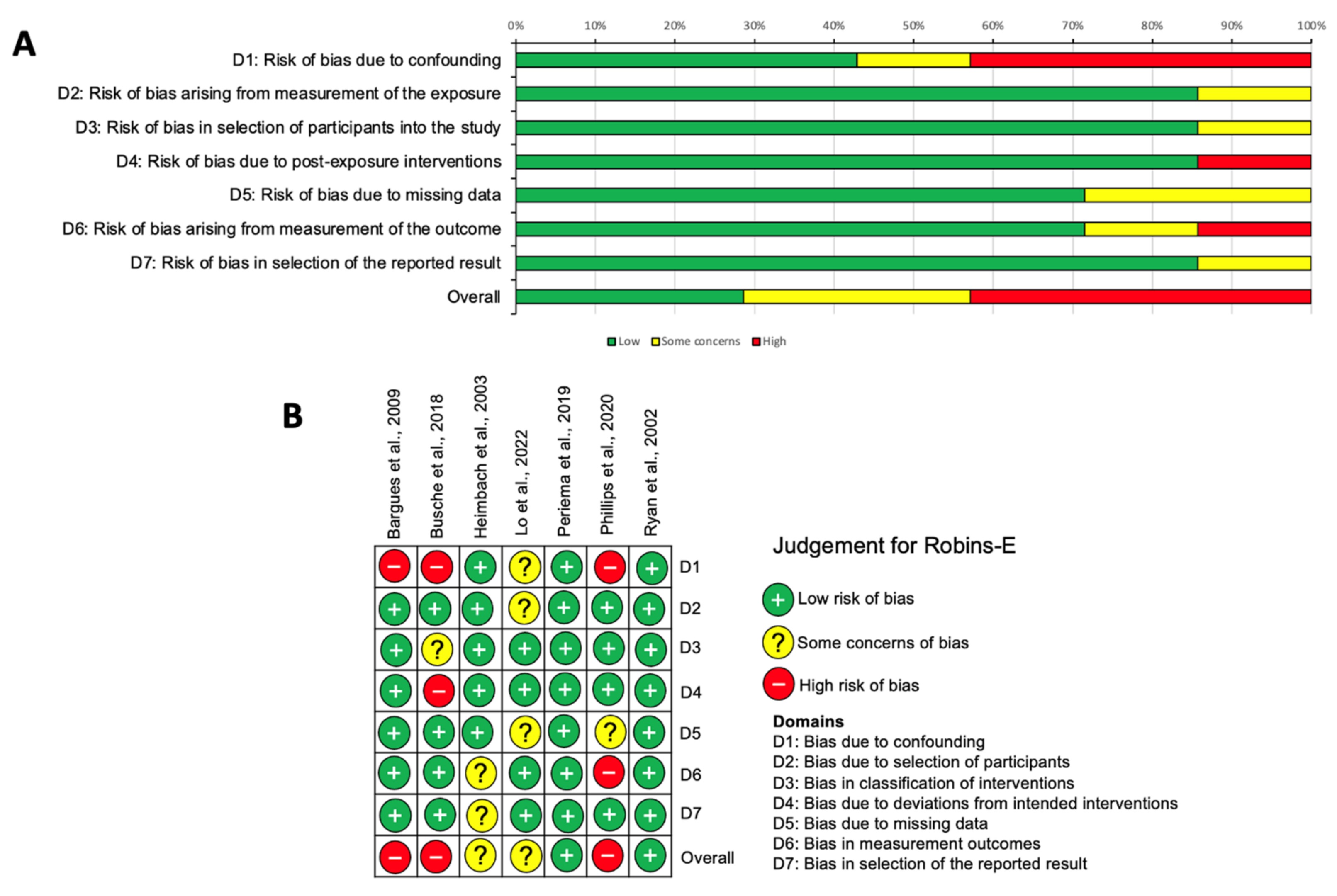
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
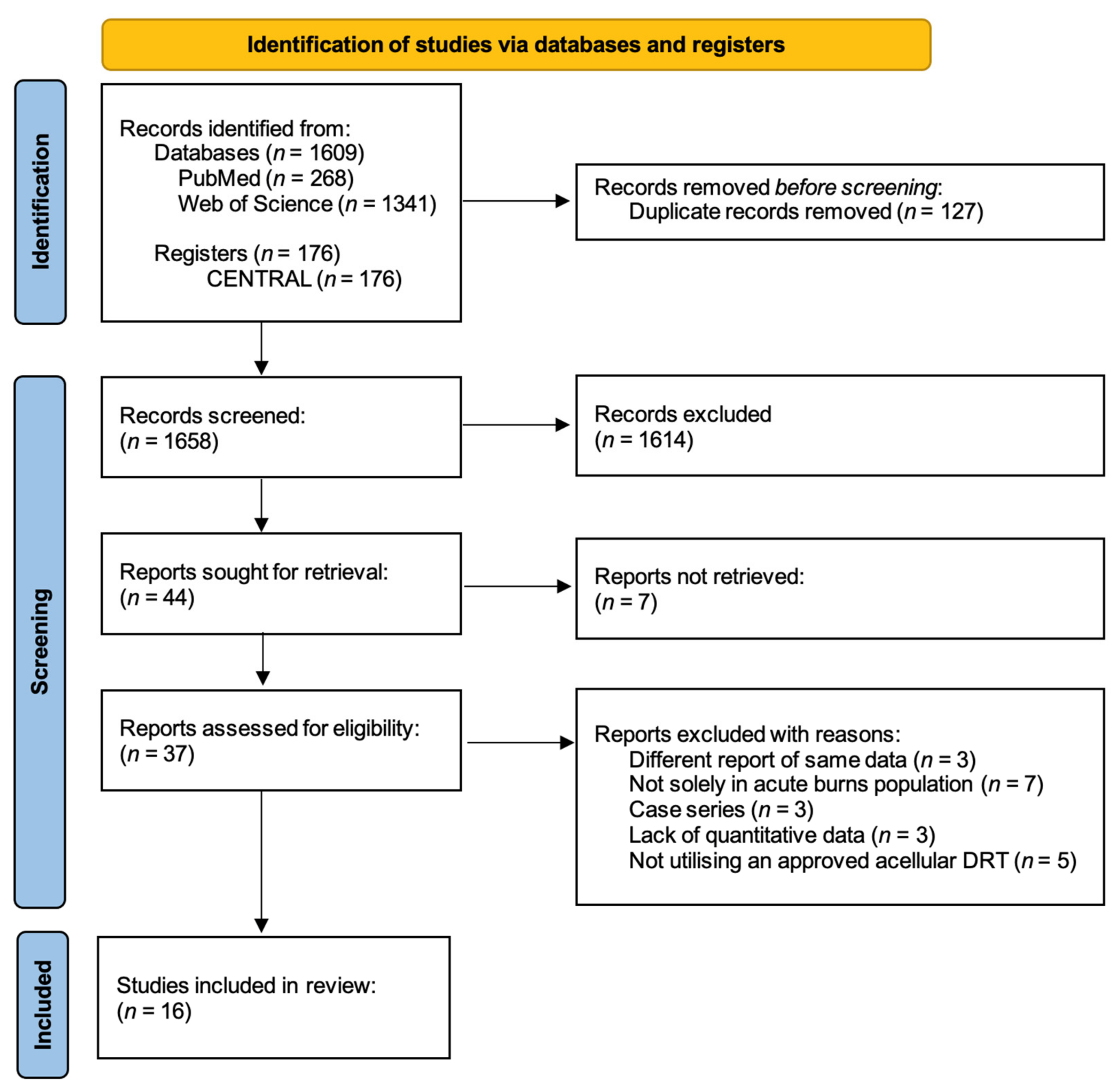
3.1. Study Selection
3.2. Study Characteristics
3.3. Primary Outcomes
3.3.1. Take Rate
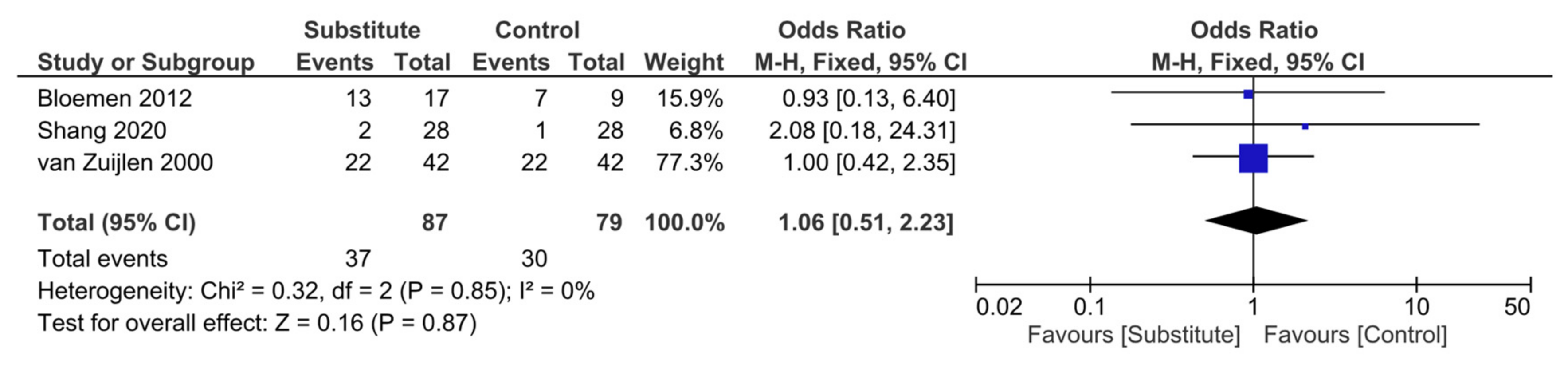
3.3.2. Incidence of Infection
3.4. Secondary Outcomes
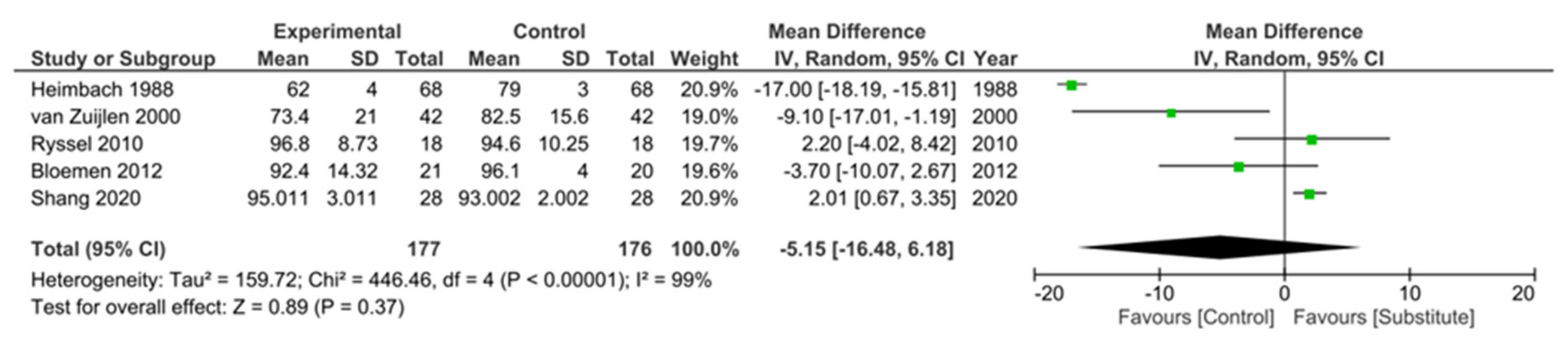
3.4.1. Scar Quality
3.4.2. Graft Loss
3.4.3. Length of Stay
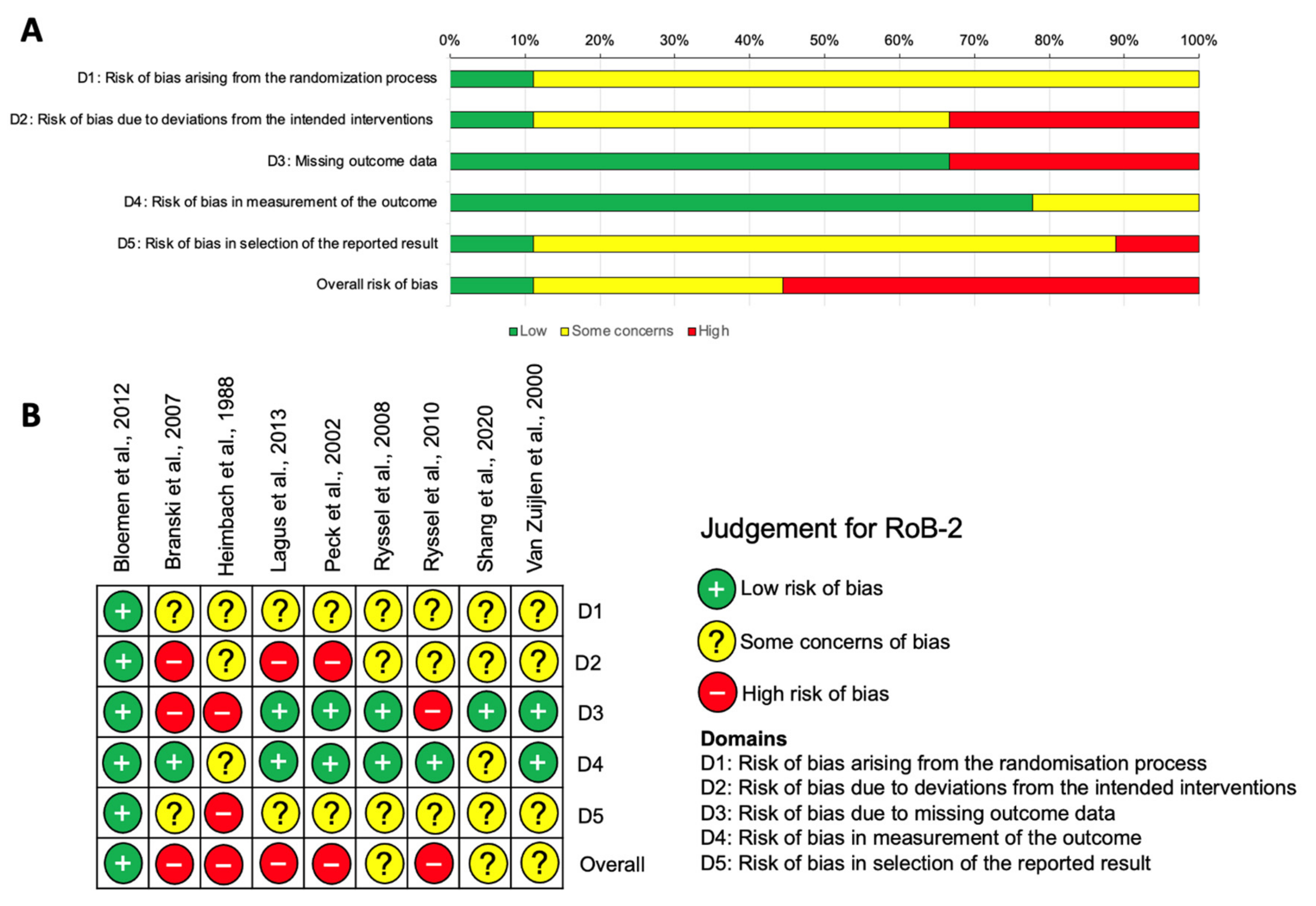
3.5. Risk of Bias Assessment
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yannas, I.V.; Burke, J.F. Design of an artificial skin. I. Basic design principles. J. Biomed. Mater. Res. 1980, 14, 65–81. [Google Scholar] [CrossRef] [PubMed]
- Shahrokhi, S.; Arno, A.; Jeschke, M.G. The use of dermal substitutes in burn surgery: Acute phase. Wound Repair Regen. 2014, 22, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Brusselaers, N.; Pirayesh, A.; Hoeksema, H.; Richters, C.D.; Verbelen, J.; Beele, H.; Blot, S.I.; Monstrey, S. Skin Replacement in Burn Wounds. J. Trauma Acute Care Surg. 2010, 68, 490–501. [Google Scholar] [CrossRef] [PubMed]
- Bay, C.; Chizmar, Z.; Reece, E.M.; Yu, J.Z.; Winocour, J.; Vorstenbosch, J.; Winocour, S. Comparison of Skin Substitutes for Acute and Chronic Wound Management. Semin. Plast. Surg. 2021, 35, 171–180. [Google Scholar] [CrossRef]
- Pruitt, B.A.; Levine, N.S. Characteristics and Uses of Biologic Dressings and Skin Substitutes. Arch. Surg. 1984, 119, 312–322. [Google Scholar] [CrossRef]
- Wainwright, D.J.; Bury, S.B. Acellular Dermal Matrix in the Management of the Burn Patient. Aesthetic Surg. J. 2011, 31, 13S–23S. [Google Scholar] [CrossRef]
- Ryssel, H.; Radu, C.A.; Germann, G.; Otte, M.; Gazyakan, E. Single-stage Matriderm® and skin grafting as an alternative reconstruction in high-voltage injuries. Int. Wound J. 2010, 7, 385–392. [Google Scholar] [CrossRef]
- Rudnicki, P.A.; Purt, B.D.; True, D.D.; Siordia, H.D.; Lohmeier, S.D.; Chan, R.K. Single-stage Composite Skin Reconstruction Using a Dermal Regeneration Template. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2622. [Google Scholar] [CrossRef]
- Integra LifeSciences. Integra Dermal Regeneration Template Brochure. 2012. Available online: https://www.integralife.com/file/general/1453795605-1.pdf (accessed on 3 October 2023).
- MedSkin Solutions Dr Suwelack AG. Matriderm. 2021. Available online: https://matriderm.com/en (accessed on 3 October 2023).
- PolyNovo®. NovoSorb® BTM. 2021. Available online: https://polynovo.com/novosorb-btm/ (accessed on 3 October 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Helbach, J.; Pieper, D.; Mathes, T.; Rombey, T.; Zeeb, H.; Allers, K.; Hoffmann, F. Restrictions and their reporting in systematic reviews of effectiveness: An observational study. BMC Med. Res. Methodol. 2022, 22, 230. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- ROBINS-E Development Group. Risk Of Bias In Non-randomized Studies—Of Exposure (ROBINS-E). 2023. Available online: https://www.riskofbias.info/welcome/robins-e-tool (accessed on 1 July 2023).
- Bloemen, M.C.T.; van der Wal, M.B.A.; Verhaegen, P.D.H.M.; Nieuwenhuis, M.K.; van Baar, M.E.; van Zuijlen, P.P.M.; Middelkoop, E. Clinical effectiveness of dermal substitution in burns by topical negative pressure: A multicenter randomized controlled trial. Wound Repair Regen. 2012, 20, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Branski, L.K.; Herndon, D.N.; Pereira, C.; Mlcak, R.P.; Celis, M.M.; Lee, J.O.; Sanford, A.P.; Norbury, W.B.; Zhang, X.-J.; Jeschke, M.G. Longitudinal assessment of Integra in primary burn management: A randomized pediatric clinical trial*. Crit. Care Med. 2007, 35, 2615–2623. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, D.; Luterman, A.; Burke, J.; Cram, A.; Herndon, D.; Hunt, J.; Jordan, M.; McMANUS, W.; Solem, L.; Warden, G.; et al. Artificial Dermis for Major Burns A Multi-Center Randomized Clinical Trial. Ann. Surg. 1988, 208, 313–320. [Google Scholar] [CrossRef]
- Lagus, H.; Sarlomo-Rikala, M.; Böhling, T.; Vuola, J. Prospective study on burns treated with Integra®, a cellulose sponge and split thickness skin graft: Comparative clinical and histological study—Randomized controlled trial. Burns 2013, 39, 1577–1587. [Google Scholar] [CrossRef]
- Peck, M.D.; Kessler, M.; Meyer, A.A.; Morris, P.A.B. A Trial of the Effectiveness of Artificial Dermis in the Treatment of Patients with Burns Greater Than 45% Total Body Surface Area. J. Trauma Inj. Infect. Crit. Care 2002, 52, 971–978. [Google Scholar] [CrossRef]
- Ryssel, H.; Gazyakan, E.; Germann, G.; Öhlbauer, M. The use of MatriDerm® in early excision and simultaneous autologous skin grafting in burns—A pilot study. Burns 2008, 34, 93–97. [Google Scholar] [CrossRef]
- Ryssel, H.; Germann, G.; Kloeters, O.; Gazyakan, E.; Radu, C. Dermal substitution with Matriderm® in burns on the dorsum of the hand. Burns 2010, 36, 1248–1253. [Google Scholar] [CrossRef]
- Shang, F.; Lu, Y.; Gao, J.; Hou, Q. Comparison of therapeutic effects between artificial dermis combined with autologous split-thickness skin grafting and autologous intermediate-thickness skin grafting alone in severely burned patients: A prospective randomised study. Int. Wound J. 2021, 18, 24–31. [Google Scholar] [CrossRef]
- Van Zuijlen, P.P.M.; van Trier, A.J.M.; Vloemans, J.F.P.M.; Groenevelt, F.; Kreis, R.W.; Middelkoop, E. Graft Survival and Effectiveness of Dermal Substitution in Burns and Reconstructive Surgery in a One-Stage Grafting Model. Plast. Reconstr. Surg. 2000, 106, 615–623. [Google Scholar] [CrossRef]
- Bargues, L.; Boyer, S.; Leclerc, T.; Duhamel, P.; Bey, E. Incidence and microbiology of infectious complications with the use of artificial skin Integra® in burns. Ann. Chir. Plast. Esthétique 2009, 54, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Busche, M.N.; Thraen, A.-C.J.; Gohritz, A.; Rennekampff, H.-O.; Vogt, P.M. Burn Scar Evaluation Using the Cutometer® MPA 580 in Comparison to “Patient and Observer Scar Assessment Scale” and “Vancouver Scar Scale”. J. Burn. Care Res. 2018, 39, 516–526. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, D.M.; Warden, G.D.; Luterman, A.; Jordan, M.H.; Ozobia, N.; Ryan, C.M.; Voigt, D.W.; Hickerson, W.L.; Saffle, J.R.; DeClement, F.A.; et al. Multicenter Postapproval Clinical Trial of Integra® Dermal Regeneration Template for Burn Treatment. J. Burn. Care Rehabil. 2003, 24, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.H.; Brown, J.N.; Dantzer, E.J.; Maitz, P.K.; Vandervord, J.G.; Wagstaff, M.J.; Barker, T.M.; Cleland, H. Wound healing and dermal regeneration in severe burn patients treated with NovoSorb® Biodegradable Temporising Matrix: A prospective clinical study. Burns 2022, 48, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Pereima, M.J.L.; Feijó, R.; da Gama, F.O.; Boccardi, R.d.O. Treatment of burned children using dermal regeneration template with or without negative pressure. Burns 2019, 45, 1075–1080. [Google Scholar] [CrossRef] [PubMed]
- Phillips, G.S.A.; Nizamoglu, M.; Wakure, A.; Barnes, D.; El-Muttardi, N.; Dziewulski, P. The Use of Dermal Regeneration Templates for Primary Burns Surgery in a UK Regional Burns Centre. Ann. Burn. Fire Disasters 2020, 3, 245–252. [Google Scholar]
- Ryan, C.M.; Schoenfeld, D.A.; Malloy, M.; Schulz, J.T.; Sheridan, R.L.; Tompkins, R.G. Use of Integra® Artificial Skin Is Associated With Decreased Length of Stay for Severely Injured Adult Burn Survivors. J. Burn. Care Rehabil. 2002, 23, 311–317. [Google Scholar] [CrossRef]
- Kohlhauser, M.; Luze, H.; Nischwitz, S.P.; Kamolz, L.P. Historical Evolution of Skin Grafting—A Journey through Time. Medicina 2021, 57, 348. [Google Scholar] [CrossRef]
- Cutometer® Dual MPA 580. Courage + Khazaka electronic GmbH. Available online: https://www.courage-khazaka.de/en/?view=article&id=178&catid=16 (accessed on 30 July 2023).
- Posluszny, J.A.; Conrad, P.; Halerz, M.; Shankar, R.; Gamelli, R.L. Surgical Burn Wound Infections and Their Clinical Implications. J. Burn. Care Res. 2011, 32, 324–333. [Google Scholar] [CrossRef]
- Greenhalgh, D.G.; Saffle, J.R.; Holmes, J.H.; Gamelli, R.L.; Palmieri, T.L.; Horton, J.W.; Tompkins, R.G.; Traber, D.L.; Mozingo, D.W.; Deitch, E.A.; et al. American Burn Association Consensus Conference to Define Sepsis and Infection in Burns. J. Burn. Care Res. 2007, 28, 776–790. [Google Scholar] [CrossRef]
- Brusselaers, N.; Pirayesh, A.; Hoeksema, H.; Verbelen, J.; Blot, S.; Monstrey, S. Burn Scar Assessment: A Systematic Review of Different Scar Scales. J. Surg. Res. 2010, 164, e115–e123. [Google Scholar] [CrossRef] [PubMed]
- Klimitz, F.J.; Neubauer, H.; Stolle, A.; Ripper, S.; Daeschler, S.C.; Aman, M.; Boecker, A.; Thomas, B.; Kneser, U.; Harhaus, L. Objective Burn Scar Assessment in Clinical Practice Using the Cutometer©: Introduction and Validation of a Standardized Measurement Protocol. J. Burn. Care Res. 2023, 44, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.L.; Sen, S.; Greenhalgh, D.G.; Lawless, M.; Curri, T.; Palmieri, T.L. Real-Time Prediction for Burn Length of Stay Via Median Residual Hospital Length of Stay Methodology. J. Burn. Care Res. 2016, 37, e476–e482. [Google Scholar] [CrossRef] [PubMed]
- Schultz, L.; Walker, S.A.; Elligsen, M.; Walker, S.E.; Simor, A.; Mubareka, S.; Daneman, N. Identification of predictors of early infection in acute burn patients. Burns 2013, 39, 1355–1366. [Google Scholar] [CrossRef]
- Lamme, E.N.; de Vries, H.J.; van Veen, H.; Gabbiani, G.; Westerhof, W.; Middelkoop, E. Extracellular matrix characterization during healing of full-thickness wounds treated with a collagen/elastin dermal substitute shows improved skin regeneration in pigs. J. Histochem. Cytochem. 1996, 44, 1311–1322. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Integra® Dermal Regeneration Template [9] | Matriderm® [10] | NovoSorb® Biodegradable Temporizing Matrix (BTM) [11] | |
|---|---|---|---|
| Manufacturer | Integra Life Science Corporation, Plainsboro, NJ, USA | MedSkin Solutions Dr. Suwelack AG, Billerbeck, Germany | PolyNovo®, Melbourne, Australia |
| First regulatory approval | 1996 | 2005 | 2019 |
| Number of layers | Bilaminar | Single layer | Bilaminar |
| Composition | Outer silicone layer, inner matrix of bovine tendon collagen, and shark chondroitin-6-sulfate | Type I, III, and V collagen and elastin scaffold | Outer sealing membrane bonded to porous matrix, both of synthetic polyurethane |
| Application procedure | 2 stages: attached to debrided burn, then top silicone layer replaced with STSG 2–4 weeks later | Single stage: Matriderm® and overlying STSG are placed on debrided wound simultaneously due to lack of upper epidermal layer in the template. | 2 stages: attached to debrided wound, then outer layer replaced with STSG once capillary refill is observed in ~2–4 weeks |
| Study | Location | Sample Size | Substitute (Number of Sites) | Control Used (Number of Sites) | Target Population | Mean Age in Years, ±Standard Deviation (If Available) | Male: Female | Burn Characteristics | Mean %TBSA Burn, ±Standard Deviation If Available | Outcome Measures |
|---|---|---|---|---|---|---|---|---|---|---|
| Bloemen et al. (2012) [16] | The Netherlands 1 | 86 | 4 arms: Matriderm®, STSG and topical negative pressure therapy = DS-TNP (21), Matriderm® and STSG = DS (23); STSG and TNP (22); STSG alone (20) | Adult | 44 ± 17 (DS-TNP), 48 ± 19.4 (DS), 49 ± 13.3 (STSG and TNP), 53 ± 18.3 (STSG alone) | 49:37 | Deep dermal or full-thickness burns | Deep dermal or full-thickness burns needing skin transplant, TBSA ≤15% | Take rate, incidence of infection, pain scores, graft loss, occurrence of hematoma, need for regrafting, scar quality, and scar elasticity. | |
| Branski et al. (2007) [17] | USA | 20 | Integra® (10) | STSG (10) | Pediatric | 7.4 (Integra®) and 6.2 (Control) | 4:1 | Burn size ≥50% TBSA and ≥40% TBSA full-thickness burn | Integra® = 70 ± 5%, control = 74 ± 4% | Body composition, serum proteins, sepsis, wound infection, scar quality, and length of stay. |
| Heimbach et al. (1988) [18] | USA 1 | 106 | Integra® (68) | STSG (68) | Adult and pediatric | No data | 3:1 | Life-threatening deep partial- and full-thickness burns | 46% ± 19% | Graft take, donor site morbidity, time to wound closure, surgeons’ assessment of substitute, mortality, and long-term assessment. |
| Lagus et al. (2013) [19] | Finland | 10 | Integra® (10) | STSG (10) and Cellonex® cellulose sponge (10) | Adult | 36.8 2 | 9:1 | Full-thickness burn >20% TBSA on anterior side of body | 35.8 ± 7.17 | Mortality, scar quality, and histological analysis. |
| Peck et al. (2002) [20] | USA | 9 | Integra® (9) | STSG allograft and Biobrane® (9) | Adult and pediatrics | 35.2 2 | No data | Deep partial- or full-thickness burns totaling >45% TBSA due to thermal injury | 66.1 ± 13.86 | Mortality, graft loss, wound or systemic infection, and length of stay. |
| Ryssel et al. (2008) [21] | Germany | 10 | Matriderm® (28) | STSG (28) | Adult | 49.5 ± 16.2 | 7:3 | Full-thickness burns | 45.6 ± 14.5 | Substitute/graft take rate, need to regraft, and scar quality (using VSS). |
| Ryssel et al. (2010) [22] | Germany | 18 | Matriderm® (18) | STSG (18) | Adult | 45.1 ± 17.4 | 13:5 | Full-thickness acute burns on the dorsum of both hands | 43.3 ± 11.8 | Substitute/graft take rate, need to regraft, scar quality (via VSS), range of motion (Finger-Tip-Palmar Crease-Distance (FPD) and Finger-Nail-Table-Distance (FNTD)). |
| Shang et al. (2020) [23] | China | 56 | Unspecified artificial dermis (28) | Intermediate thickness skin graft (ITSG) (28) | Adult | 36.48 ± 3.47 (artificial dermis), 36.38 ± 3.51 (control) | 31:25 2 | Total burn area >85% TBSA with deep partial-thickness burn area >50% TBSA and scar area >50% TBSA | No data | Healing time, scar quality (via VSS), graft take, infection rates, psychological status (self-rating anxiety and depression scales), and active recovery of function. |
| van Zuijlen et al. (2000) [24] | Netherlands | 31 | Matriderm® (42) | STSG (42) | Adult | 32.9 ± 19.3 | 18:13 | Deep partial- and full-thickness acute burns | 19.8 ± 14.5 | Take rate, infection, need for reconstruction, and scar quality. |
| Study | Location | Study Design | Sample Size | Substitute (Number of Sites) | Control Used (Number of Sites) | Target Population | Mean Age in Years, ±Standard Deviation If Available | Male: Female | Burn Characteristics | Mean %TBSA Burn ±Standard Deviation If Available | Main Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bargues et al. (2009) [25] | France | Retrospective | 50 | Integra® (71) | None | Adult and pediatric | 40 ± 15 | 35:15 | Deep partial-thickness acute burns | 45 ± 21 | Incidence of infection, microbiology of infections, and length of stay. |
| Busche et al. (2018) [26] | Germany | Prospective | 45 | Matriderm® (6) | STSG (49) | Adult | 45 | 65:35 | Scars from deep partial- and full-thickness burns treated acutely >2 years previously | No data | Burn scar evaluation with Cutometer, POSAS, and VSS. |
| Heimbach et al. (2003) [27] | USA 1 | Prospective | 216 | Integra® (841) | None | Adult and pediatric | 34.74 ± 23.85 | 70:30 | Life-threatening deep partial- to full-thickness burn | 36.5 ± 24.7 | Incidence of Integra infection, mortality, Integra, and autograft take rate. |
| Lo et al. (2022) [28] | Australia and France 1 | Prospective | 26 | NovoSorb® BTM (100) | None | Adult | 45.2 ± 16.5 | 22:4 | Deep partial- or full-thickness thermal burn 10–70% TBSA | 47.5 ± 14.2 | Substitute and STSG take, incidence of infection, adverse events, and scar quality (VSS at 12 months). |
| Pereima et al. (2019) [29] | Brazil | Retrospective | 44 | Integra® (22) | Integra® and negative pressure wound therapy (22) | Pediatric | No data | 25:19 | Deep partial- and full-thickness burns | No data | DRT and STSG take rates and time to maturation. |
| Phillips et al. (2020) [30] | UK | Retrospective | 94 | Matriderm® (35) and Integra® (59) | Adult and pediatric | 28 ± 20.3 (Matriderm), 17 ± 17.7 (Integra) | No data | Deep partial- and full-thickness burns | Integra = 36.8 ± 23.3, Matriderm = 15.7 ± 20.9 | DRT take, time to healing, complication rates, and graft loss. | |
| Ryan et al. (2002) [31] | US | Retrospective | 270 | Integra® (43) | STSG (227) | Adult | 50 ± 21 (Integra), 46 ± 20 (control) | No data | Full-thickness burn ≥20% | Integra = 55 ± 19, Control = 59 ± 21 | Mortality, LOS, and time to closure. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Press, I.; Moiemen, N.; Ahmed, Z. Efficacy and Complications Associated with Acellular Dermal Substitute Use in the Treatment of Acute Burns: A Systematic Review and Meta-Analysis. Eur. Burn J. 2023, 4, 548-562. https://doi.org/10.3390/ebj4040036
Press I, Moiemen N, Ahmed Z. Efficacy and Complications Associated with Acellular Dermal Substitute Use in the Treatment of Acute Burns: A Systematic Review and Meta-Analysis. European Burn Journal. 2023; 4(4):548-562. https://doi.org/10.3390/ebj4040036
Chicago/Turabian StylePress, Isobel, Naiem Moiemen, and Zubair Ahmed. 2023. "Efficacy and Complications Associated with Acellular Dermal Substitute Use in the Treatment of Acute Burns: A Systematic Review and Meta-Analysis" European Burn Journal 4, no. 4: 548-562. https://doi.org/10.3390/ebj4040036