
Frailty Screening Practice in Specialized Burn Care—A Retrospective Multicentre Cohort Study
 , , , ,
, , , ,
Abstract
:1. Background
2. Methods
2.1. Study Design and Participants
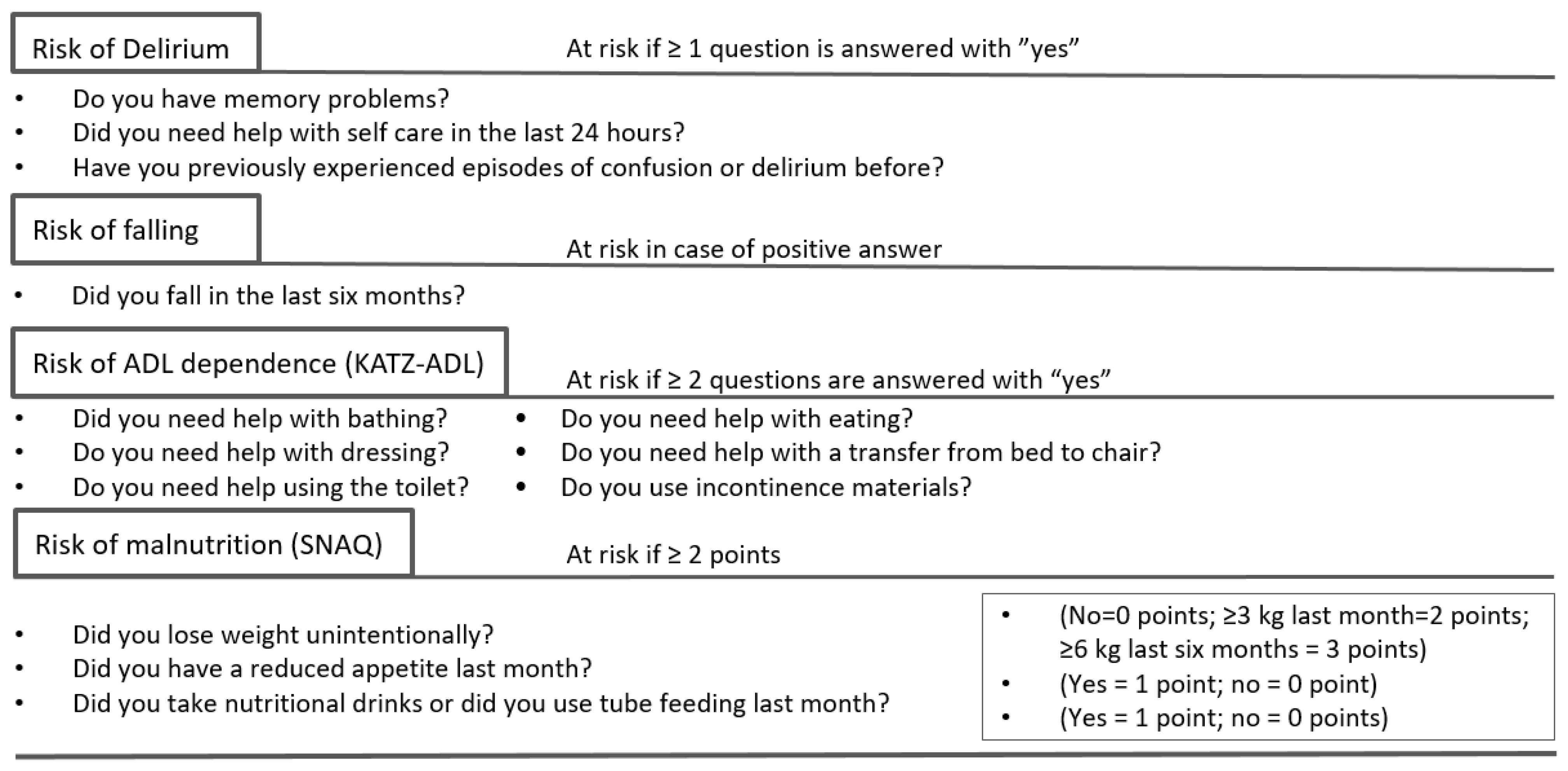
2.2. Frailty Assessment
2.3. Data Collection
2.4. Data Analysis and Statistical Analysis
3. Results Inclusion
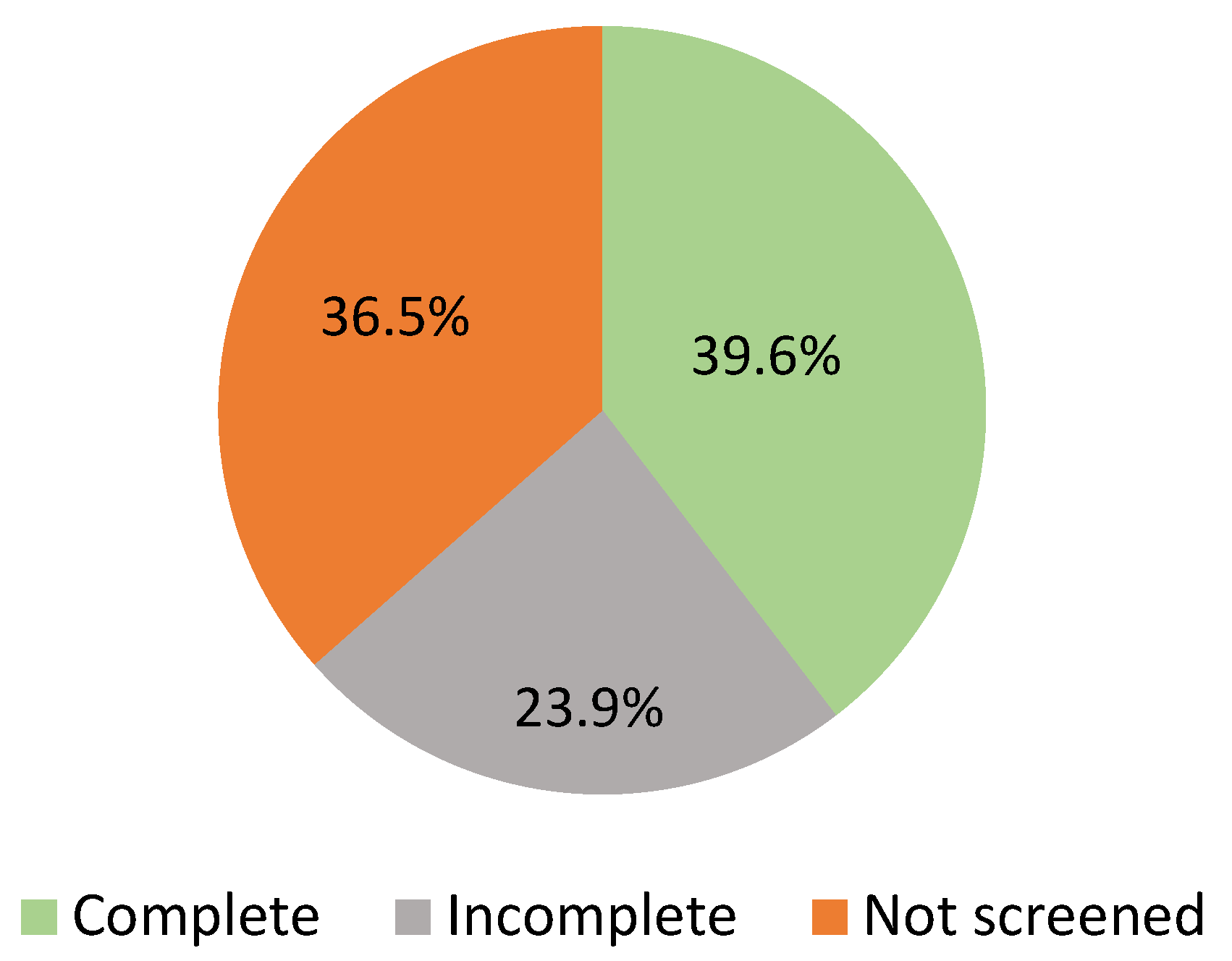
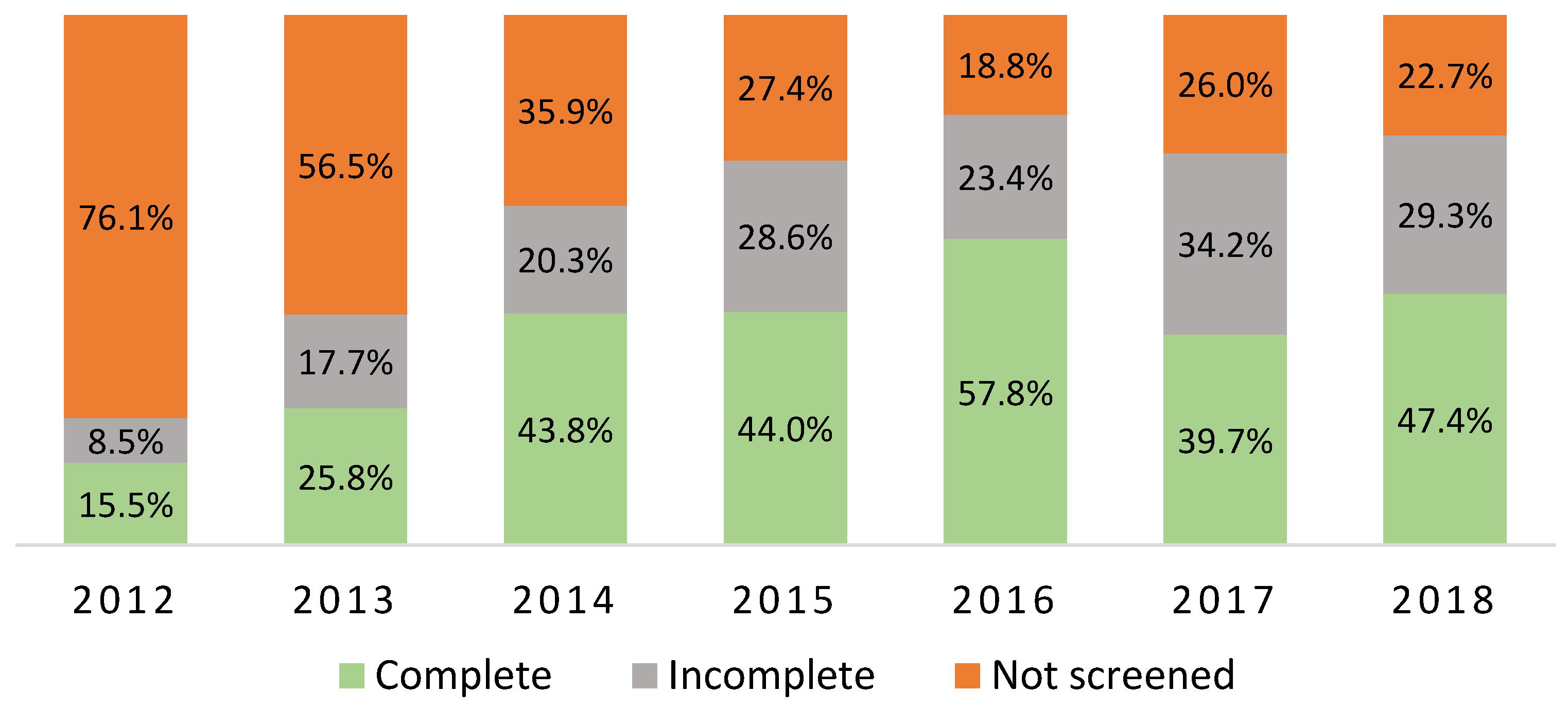
3.1. Feasibility of the DSMS Frailty Screening
3.2. Determinants of Complete Frailty Screening
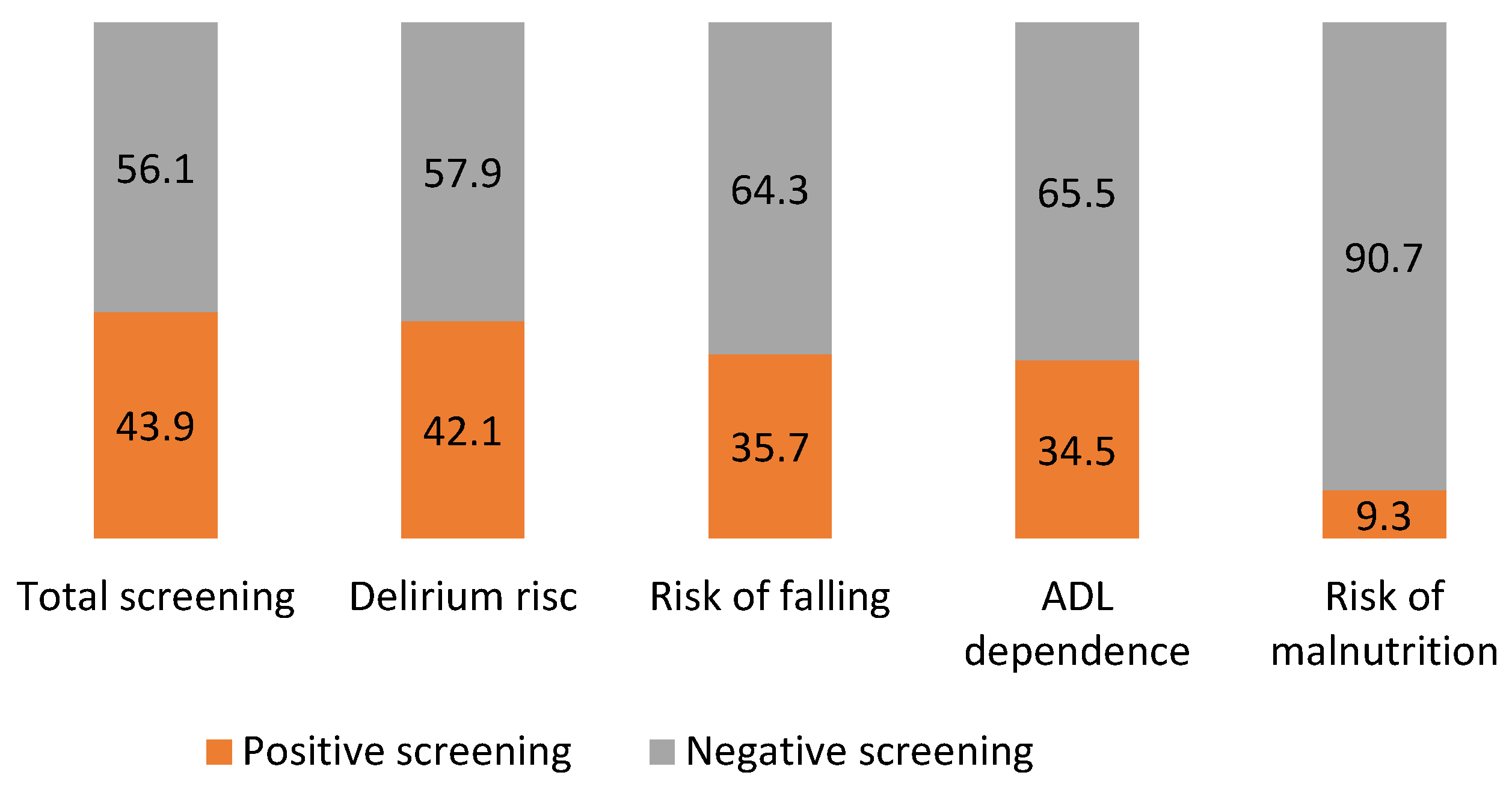
3.3. Risk of Frailty
3.4. Validity of the DSMS Frailty Screening: Known Group Validity and Predictive Validity
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | Patients with Burn Injury Only | |
|---|---|---|
| Logistic Regression (Univariable) | Logistic Regression (Univariable) | |
| OR (95% CI) | OR (95% CI) | |
| Age (years) | ||
| <75 | 1 | 1 |
| ≥75 | 2.85 (1.58–5.12) 1 | 3.48 (1.80–6.74) 1 |
| ASA Score | ||
| 1–2 | 1 | 1 |
| ≥3 | 3.91 (2.24–6.82) 1 | 3.73 (2.04–6.83) 1 |
| All Patients | Patients with Burn Injury Only | |
|---|---|---|
| Logistic Regression (Adjusted 3) | Logistic Regression (Adjusted 3) | |
| OR (95% CI) | OR (95% CI) | |
| Length of stay (days) | ||
| ≤7 | 1 | 1 |
| >7 | 1.97 (1.05–3.70) 2 | 2.45 (1.20–4.98) 2 |
| Discharge location | ||
| Home | 1 | 1 |
| Non-home 1 | 3.20 (1.69–6.12) 2 | 3.16 (1.53–6.55) 2 |
| In-hospital mortality | ||
| No | 1 | 1 |
| Yes | 3.66 (0.68–19.86) | 10.38 (1.08–99.27) |
References
- Oud, F.M.M.; de Rooij, E.J.A.; Schuurman, T.; Duijvelaar, K.M.; van Munster, B.C. Predictive value of the VMS theme ‘Frail elderly’: Delirium, falling and mortality in elderly hospital patients. Ned. Tijdschr. Geneeskd. 2015, 159, A8491. [Google Scholar] [PubMed]
- Duke, J.M.; Boyd, J.H.; Rea, S.; Randall, S.M.; Wood, F.M. Long-term mortality among older adults with burn injury: A population-based study in Australia. Bull. World Health Organ. 2015, 93, 400–406. [Google Scholar] [CrossRef]
- Warnier, R.M.; van Rossum, E.; van Velthuijsen, E.; Mulder, W.J.; Schols, J.M.; Kempen, G.I. Validity, Reliability and Feasibility of Tools to Identify Frail Older Patients in Inpatient Hospital Care: A Systematic Review. J. Nutr. Health Aging 2016, 20, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef] [PubMed]
- Snijders, B.M.G.; Emmelot-Vonk, M.H.; Souwer, E.T.D.; Kaasjager, H.A.H.; van den Bos, F. Prognostic value of screening instrument based on the Dutch national VMS guidelines for older patients in the emergency department. Eur. Geriatr. Med. 2021, 12, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Oud, F.M.M.; Schut, M.C.; Spies, P.E.; van der Zaag-Loonen, H.J.; de Rooij, S.E.; Abu-Hanna, A.; van Munster, B.C. Interaction between geriatric syndromes in predicting three months mortality risk. Arch. Gerontol. Geriatr. 2022, 103, 104774. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Heim, N.; van Fenema, E.M.; Weverling-Rijnsburger, A.W.; Tuijl, J.P.; Jue, P.; Oleksik, A.M.; Verschuur, M.J.; Haverkamp, J.S.; Blauw, G.J.; van der Mast, R.C.; et al. Optimal screening for increased risk for adverse outcomes in hospitalised older adults. Age Ageing 2015, 44, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Romanowski, K.; Curtis, E.; Barsun, A.; Palmieri, T.; Greenhalgh, D.; Sen, S. The frailty tipping point: Determining which patients are targets for intervention in a burn population. Burns 2019, 45, 1051–1056. [Google Scholar] [CrossRef] [PubMed]
- Romanowski, K.S.; Barsun, A.; Pamlieri, T.L.; Greenhalgh, D.G.; Sen, S. Frailty score on admission predicts outcomes in elderly burn injury. J. Burn Care Res. 2015, 36, 1–6. [Google Scholar] [CrossRef]
- Romanowski, K.S.; Curtis, E.; Palmieri, T.L.; Greenhalgh, D.G.; Sen, S. Frailty Is Associated with Mortality in Patients Aged 50 Years and Older. J. Burn Care Res. 2018, 39, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.; Phillips, G.; Radotra, I.; Smailes, S.; Dziewulski, P.; Zhang, J.; Martin, N. Frailty: An independent predictor of burns mortality following in-patient admission. Burns 2018, 44, 1895–1902. [Google Scholar] [CrossRef] [PubMed]
- Warnier, R.M.J.; van Rossum, E.; van Kuijk, S.M.J.; Magdelijns, F.; Schols, J.; Kempen, G. Frailty screening in hospitalised older adults: How does the brief Dutch National Safety Management Program perform compared to a more extensive approach? J. Clin. Nurs. 2020, 29, 1064–1073. [Google Scholar] [CrossRef] [PubMed]
- Ambagtsheer, R.C.; Archibald, M.M.; Lawless, M.; Kitson, A.; Beilby, J. Feasibility and acceptability of commonly used screening instruments to identify frailty among community-dwelling older people: A mixed methods study. BMC Geriatr. 2020, 20, 152. [Google Scholar] [CrossRef]
- Schuijt, H.J.; Oud, F.M.M.; Bruns, E.J.R.; van Duijvendijk, P.; Van der Zaag-Loonen, H.J.; Spies, P.E.; van Munster, B.C. Does the Dutch Safety Management Program predict adverse outcomes for older patients in the emergency department? Neth. J. Med. 2020, 78, 244–250. [Google Scholar] [PubMed]
- Oen, I.M.; van der Vlies, C.H.; Roeleveld, Y.W.; Dokter, J.; Hop, M.J.; van Baar, M.E. Epidemiology and costs of patients with toxic epidermal necrolysis: A 27-year retrospective study. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 2444–2450. [Google Scholar] [CrossRef] [PubMed]
- Cords, C.I.; Spronk, I.; Mattace-Raso, F.U.S.; Verhofstad, M.H.J.; van der Vlies, C.H.; van Baar, M.E. The feasibility and reliability of frailty assessment tools applicable in acute in-hospital trauma patients: A systematic review. J. Trauma Acute Care Surg. 2022, 92, 615–626. [Google Scholar] [CrossRef] [PubMed]
- Dutch Safety Management System DSMS, Frail Elderly Guideline (Veiligheids Management Systeem, Kwetsbare Ouderen Richtlijn). Available online: https://www.vmszorg.nl/vms-veiligheidsprogramma/10-themas/kwetsbare-ouderen/ (accessed on 2 October 2021).
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged. The Index of Adl: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Kruizenga, H.M.; Seidell, J.C.; de Vet, H.C.; Wierdsma, N.J.; van Bokhorst-de van der Schueren, M.A. Development and validation of a hospital screening tool for malnutrition: The short nutritional assessment questionnaire (SNAQ). Clin. Nutr. 2005, 24, 75–82. [Google Scholar] [CrossRef] [PubMed]
- van Loon, I.N.; Goto, N.A.; Boereboom, F.T.J.; Bots, M.L.; Verhaar, M.C.; Hamaker, M.E. Frailty Screening Tools for Elderly Patients Incident to Dialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 1480–1488. [Google Scholar] [CrossRef] [PubMed]
- van der Zanden, V.; Paarlberg, K.M.; van der Zaag-Loonen, H.J.; Meijer, W.J.; Mourits, M.J.E.; van Munster, B.C. Risk assessment for postoperative outcomes in a mixed hospitalized gynecological population by the Dutch safety management system (Veiligheidsmanagementsysteem, VMS) screening tool ‘frail elderly’. Arch. Gynecol. Obstet. 2021, 304, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Winters, A.M.; Hartog, L.C.; Roijen, H.; Brohet, R.M.; Kamper, A.M. Relationship between clinical outcomes and Dutch frailty score among elderly patients who underwent surgery for hip fracture. Clin. Interv. Aging 2018, 13, 2481–2486. [Google Scholar] [CrossRef] [PubMed]
- Karlekar, M.B.; Maxwell, C.A.; Dietrich, M.S.; Miller, R.S. Creating New Opportunities to Educate Families on the Impact of Frailty and Cognitive Impairment in a Trauma Intensive Care Unit: Results of a Quality Improvement Project. J. Palliat. Med. 2017, 20, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Bryant, E.A.; Tulebaev, S.; Castillo-Angeles, M.; Moberg, E.; Senglaub, S.S.; O’Mara, L.; McDonald, M.; Salim, A.; Cooper, Z. Frailty Identification and Care Pathway: An Interdisciplinary Approach to Care for Older Trauma Patients. J. Am. Coll. Surg. 2019, 228, 852–859.e851. [Google Scholar] [CrossRef] [PubMed]
- Joosten, E.; Demuynck, M.; Detroyer, E.; Milisen, K. Prevalence of frailty and its ability to predict in hospital delirium, falls, and 6-month mortality in hospitalized older patients. BMC Geriatr. 2014, 14, 1. [Google Scholar] [CrossRef]
- Tipping, C.; Chan, T.; Harrold, M.; Holland, A.; Hodgson, C. Using frailty to predict mortality in Australian ICU patients following trauma: A prospective observational study comparing two frailty measures. Aust. Crit. Care 2018, 31, 113. [Google Scholar] [CrossRef]
- Kistler, E.A.; Nicholas, J.A.; Kates, S.L.; Friedman, S.M. Frailty and Short-Term Outcomes in Patients with Hip Fracture. Geriatr. Orthop. Surg. Rehabit. 2015, 6, 209–214. [Google Scholar] [CrossRef]
- Gleason, L.J.; Benton, E.A.; Alvarez-Nebreda, M.L.; Weaver, M.J.; Harris, M.B.; Javedan, H. FRAIL Questionnaire Screening Tool and Short-Term Outcomes in Geriatric Fracture Patients. J. Am. Med. Dir. Assoc. 2017, 18, 1082–1086. [Google Scholar] [CrossRef]
- Hubbard, R.E.; Peel, N.M.; Samanta, M.; Gray, L.C.; Mitnitski, A.; Rockwood, K. Frailty status at admission to hospital predicts multiple adverse outcomes. Age Ageing 2017, 46, 801–806. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, D.; Rhee, P.; Drake, M.; Hodge, J.; Ingram, W.; Williams, R. Development of the Burn Frailty Index: A prognostication index for elderly patients sustaining burn injuries. Am. J. Surg. 2019, 218, 87–94. [Google Scholar] [CrossRef]
- Rockwood, K.; Theou, O. Using the Clinical Frailty Scale in Allocating Scarce Health Care Resources. Can. Geriatr. J. 2020, 23, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Flaatten, H.; De Lange, D.W.; Morandi, A.; Andersen, F.H.; Artigas, A.; Bertolini, G.; Boumendil, A.; Cecconi, M.; Christensen, S.; Faraldi, L.; et al. The impact of frailty on ICU and 30-day mortality and the level of care in very elderly patients (>/= 80 years). Intensive Care Med. 2017, 43, 1820–1828. [Google Scholar] [CrossRef]
- Flaatten, H.; Guidet, B.; Andersen, F.H.; Artigas, A.; Cecconi, M.; Boumendil, A.; Elhadi, M.; Fjølner, J.; Joannidis, M.; Jung, C.; et al. Reliability of the Clinical Frailty Scale in very elderly ICU patients: A prospective European study. Ann. Intensive Care 2021, 11, 22. [Google Scholar] [CrossRef]
- van Yperen, D.T.; Raats, J.W.; Dokter, J.; Ziere, G.; Roukema, G.R.; van Baar, M.E.; van der Vlies, C.H. Prevalence and Risk Factors for Delirium in Elderly Patients with Severe Burns: A Retrospective Cohort Study. J. Burn Care Res. 2020, 41, 371–376. [Google Scholar] [CrossRef]
- Persico, I.; Cesari, M.; Morandi, A.; Haas, J.; Mazzola, P.; Zambon, A.; Annoni, G.; Bellelli, G. Frailty and Delirium in Older Adults: A Systematic Review and Meta-Analysis of the Literature. J. Am. Geriatr. Soc. 2018, 66, 2022–2030. [Google Scholar] [CrossRef] [PubMed]
- Chróinín, D.N.; Francis, N.; Wong, P.; Kim, Y.D.; Nham, S.; D’Amours, S. Older trauma patients are at high risk of delirium, especially those with underlying dementia or baseline frailty. Trauma Surg. Acute Care Open 2021, 6, e000639. [Google Scholar] [CrossRef] [PubMed]
- Coutris, N.; Gawaziuk, J.P.; Magnusson, S.; Logsetty, S. Malnutrition in Burns: A prospective, single center study. J. Burn Care Res. 2021, 43, 592–595. [Google Scholar] [CrossRef] [PubMed]




| Characteristics | All, n = 515 |
|---|---|
| Sex: woman (%) | 260 (50.5) |
| Age, years (%) | |
| 70–74 | 179 (34.8) |
| 75–84 | 223 (43.3) |
| ≥85 | 113 (21.9) |
| Year of admission (%) | |
| 2012–2015 | 281 (54.6) |
| 2016–2018 | 234 (45.4) |
| ASA score 1 (%) | |
| 1–2 | 266 (54.0) |
| ≥3 | 227 (46.0) |
| Aetiology 1 (%) | |
| Flame | 192 (38.5) |
| Scald | 106 (21.2) |
| Other thermal injury 2 | 122 (24.4) |
| Other skin-related diseases 3 | 79 (15.8) |
| TBSA (%) | |
| <5 | 285 (55.3) |
| 5–19 | 168 (32.6) |
| ≥20 | 62 (12.0) |
| ICU (%) | 147 (28.5) |
| Revised Baux Score (median (P25–P75)) 4 | 88.0 (78.0–93.0) |
| Frailty Screening | Logistic Regression | |||
|---|---|---|---|---|
| Characteristics | Complete (n = 204) | None/Incomplete (n = 311) | Univariable | Multivariable |
| n (%) | n (%) | OR (95% CI) | OR (95% CI) | |
| Sex (%) | ||||
| Man | 106 (52.0) | 149 (47.9) | 1 | - |
| Woman | 98 (48.0) | 162 (52.1) | 0.85 (0.60–1.21) | - |
| Age, years (%) | ||||
| 70–74 | 67 (32.8) | 112 (36.0) | 1 | - |
| 75–84 | 91 (44.6) | 132 (42.4) | 1.15 (0.77–1.73) | - |
| ≥85 | 46 (22.5) | 67 (21.5) | 1.15 (0.71–1.86) | - |
| Year of admission (%) | ||||
| 2012–2015 | 92 (45.1) | 189 (60.8) | 1 | 1 |
| 2016–2018 | 112 (54.9) | 122 (39.2) | 1.89 (1.32–2.70) 1 | 2.15 (1.42–3.25) 1 |
| Day of the week (%) | ||||
| Week | 149 (73.0) | 225 (72.3) | 1 | - |
| Weekend | 55 (27.0) | 86 (27.7) | 0.97 (0.65–1.44) | - |
| ASA score 2 (%) | ||||
| 1–2 | 115 (56.9) | 151 (51.9) | 1 | - |
| ≥3 | 87 (43.1) | 140 (48.1) | 0.82 (0.57–1.71) | - |
| TSBA (%) | ||||
| <5 | 124 (60.8) | 161 (51.8) | 1 | 1 |
| 5–20 | 72 (35.3) | 96 (30.9) | 0.97 (0.66–1.43) | 0.90 (0.58–1.40) |
| >20 | 8 (3.9) | 54 (17.4) | 0.19 (0.09–0.42) 1 | 0.12 (0.05–0.29) 1 |
| Revised Baux Score (median (P25–P75)) | 82.5(77.5–89.0) | 85.5 (78.7–95.0) | 0.97 (0.96–0.98) 1 | - |
| ICU (%) | ||||
| No | 165 (80.9) | 203 (65.3) | 1 | - |
| Yes | 39 (19.1) | 108 (34.7) | 0.44 (0.29–0.68) 1 | - |
| Positive Frailty Screening 1 (n = 100) | Negative Frailty Screening (n = 128) | Logistic Regression (Univariable) | |
|---|---|---|---|
| n (%) | n (%) | OR (95% CI) | |
| Age (years) | |||
| <75 | 22 (22.0) | 57 (44.5) | 1 |
| ≥75 | 78 (78.0) | 71 (55.5) | 2.85 (1.58–5.12) 2 |
| ASA Score | |||
| 1–2 | 38 (38.4) | 90 (70.9) | 1 |
| ≥3 | 61 (61.6) | 37 (29.1) | 3.91 (2.24–6.82) 2 |
| DSMS Frailty Screening | Logistic Regression (Unadjusted) | Logistic Regression (Adjusted 3) | ||
|---|---|---|---|---|
| Positive Score (n = 100) | Negative Score (n = 128) | OR (95% CI) | OR (95% CI) | |
| Length of stay (days) | ||||
| ≤7 | 23 (23.0) | 47 (36.7) | 1 | 1 |
| >7 | 77 (77.0) | 81 (63.3) | 1.94 (1.08–3.50) 2 | 1.97 (1.05–3.70) 2 |
| Discharge location | ||||
| Home | 53 (53.0) | 104 (81.3) | 1 | 1 |
| Non-home 1 | 47 (47.0) | 24 (18.8) | 3.84 (2.13–6.95) 2 | 3.20 (1.69–6.12) 2 |
| In-hospital mortality | ||||
| No | 91 (91.0) | 126 (98.4) | 1 | 1 |
| Yes | 9 (9.0) | 2 (1.6) | 6.23 (1.32–29.52) 2 | 3.66 (0.68–19.86) |
| Logistic Regression (Univariable) | |
|---|---|
| OR (95% CI) | |
| Demographic and injury characteristics | |
| Age (years) | 1.11 (1.06–1.17) 1 |
| Sex (female) | 1.12 (0.67–1.90) |
| Burn size (TBSA%) | 1.01 (0.98–1.04) |
| Inhalation injury | 5.29 (0.58–48.00) |
| ASA score > 2 | 3.91 (2.24–6.82) 1 |
| Adverse outcomes | |
| Length of stay (days) | 1.94 (1.08–3.50) 1 |
| Discharge location | 3.84 (2.13–6.95) 1 |
| In-hospital mortality | 6.23 (1.32–29.52) 1 |
| Length of Stay (>7 Days) | Non-Home Discharge Location | In-Hospital Mortality | |
|---|---|---|---|
| Log Regression (Multivariable) OR (95% CI) | Log Regression (Multivariable) OR (95% CI) | Log Regression (Multivariable) OR (95% CI) | |
| Age (years) | 0.97 (0.92–1.02) | 1.05 (1.00–1.10) 3 | 1.13 (1.00–1.27) 1 |
| Sex (female) | 2.87 (1.53–5.39) 1 | 1.68 (0.88–3.18) | 0.89 (0.23–3.44) |
| Burn size (TBSA%) | 1.05 (1.00–1.10) 2 | 1.08 (1.03–1.13) 2 | 1.06 (1.01–1.10) 1 |
| Inhalation injury | 1.09 (0.11 (11.15) | 1.23 (0.19–7.84) | 2.50 (0.21–29.48) |
| ASA (>2) | 1.01 (0.53–1.91) | 2.03 (1.06–3.90) 2 | 3.45 (0.66–17.99) |
| DSMS score (≥2) | 2.09 (1.06–4.14) 1 | 2.80 (1.43–5.49) 2 | 2.71 (0.48–15.47) |
| DSMS Domain | Complete, n (%) | Incomplete, n (%) | Not Screened, n (%) |
|---|---|---|---|
| Risk of delirium | 258 (50.1) | 34 (6.6) | 223 (43.3) |
| Risk of falling | 255 (49.5) | 260 (50.5) | |
| Risk of ADL dependence | 276 (53.6) | 27 (5.2) | 212 (41.2) |
| Risk of malnutrition | 286 (55.5) | 14 (2.7) | 215 (41.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cords, C.I.; van der Vlies, C.H.; Stoop, M.; Nieuwenhuis, M.K.; Boudestein, K.; Mattace-Raso, F.U.S.; van Baar, M.E.; FRAIL Group; Dutch Burn Repository Group. Frailty Screening Practice in Specialized Burn Care—A Retrospective Multicentre Cohort Study. Eur. Burn J. 2023, 4, 87-100. https://doi.org/10.3390/ebj4010009
Cords CI, van der Vlies CH, Stoop M, Nieuwenhuis MK, Boudestein K, Mattace-Raso FUS, van Baar ME, FRAIL Group, Dutch Burn Repository Group. Frailty Screening Practice in Specialized Burn Care—A Retrospective Multicentre Cohort Study. European Burn Journal. 2023; 4(1):87-100. https://doi.org/10.3390/ebj4010009
Chicago/Turabian StyleCords, Charlotte I., Cornelis H. van der Vlies, Matthea Stoop, Marianne K. Nieuwenhuis, Kris Boudestein, Francesco U. S. Mattace-Raso, Margriet E. van Baar, FRAIL Group, and Dutch Burn Repository Group. 2023. "Frailty Screening Practice in Specialized Burn Care—A Retrospective Multicentre Cohort Study" European Burn Journal 4, no. 1: 87-100. https://doi.org/10.3390/ebj4010009