
Methoxyflurane for Relief of Procedural Pain in Burn Patients: A Prospective Single-Centre Evaluation Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statement of Ethics
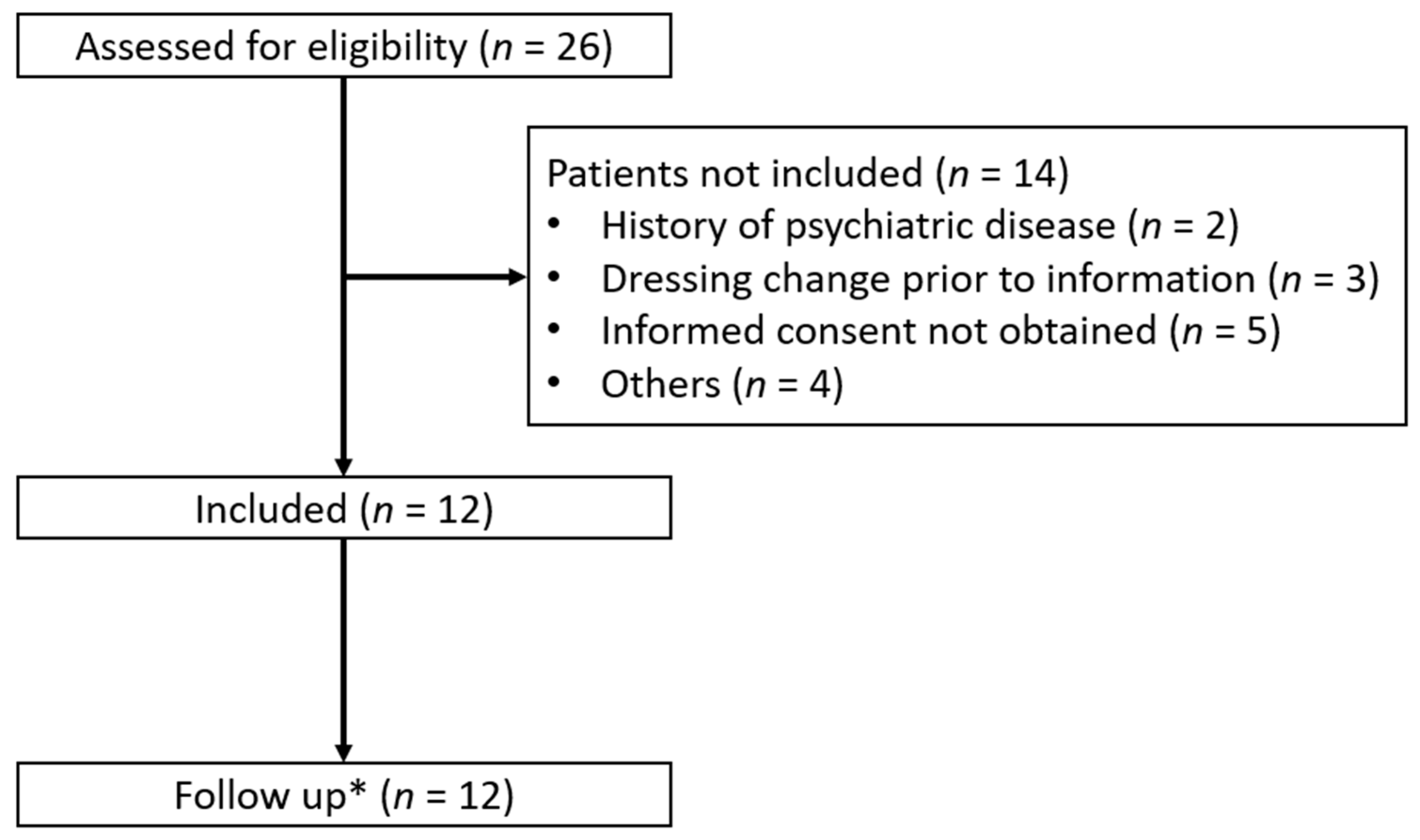
2.3. Eligibility Criteria
2.4. Study Site
2.5. Intervention
2.6. Data Collection
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Diamond, A.W. Analgesia for Burns Dressings. Lancet 1959, 274, 710–713. [Google Scholar]
- Laird, S.M.; Gray, B.M. Intermittent inhalation of methoxyflurane and trichloroethylene as analgesics in burns dressings procedures. Br. J. Anaesth. 1971, 43, 149–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verdier, J.; Leduc, A.; Duteille, F.; Bertrand-Vasseur, A.; Perrot, P. Utilisation du méthoxyflurane sur la douleur aiguë lors du pansement des brûlés [Usage of methoxyflurane for pain control for dressing change in burn patients]. Ann. Chir. Plast. Esthet. 2020, 65, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.; Mustard, L. The management of pain in the burns unit. Burns 2009, 35, 921–936. [Google Scholar] [CrossRef] [PubMed]
- Wasiak, J.; Mahar, P.D.; Paul, E.; Menezes, H.; Spinks, A.B.; Cleland, H. Inhaled methoxyflurane for pain and anxiety relief during burn wound care procedures: An Australian case series. Int. Wound J. 2014, 11, 74–78. [Google Scholar] [CrossRef]
- Wall, S.L.; Clarke, D.L.; Allorto, N.L. Analgesia Protocols for Burns Dressings: Challenges with Implementation. Burns 2019, 176, 139–148. [Google Scholar] [CrossRef]
- Wasiak, J.; Spinks, A.; Costello, V.; Ferraro, F.; Paul, E.; Konstantatos, A.; Cleland, H. Adjuvant use of intravenous lidocaine for procedural burn pain relief: A randomized double-blind, placebo-controlled, cross-over trial. Burns 2011, 37, 951–957. [Google Scholar] [CrossRef]
- Griggs, C.; Goverman, J.; Bittner, E.A.; Levi, B. Sedation and Pain Management in Burn Patients. Clin. Plast. Surg. 2017, 44, 535–540. [Google Scholar] [CrossRef]
- Packer, K.J.; Titel, J.H. Methoxyflurane analgesia for burns dressings: Experience with the analgizer. Br. J. Anaesth. 1969, 41, 1080–1085. [Google Scholar] [CrossRef] [Green Version]
- Jephcott, C.; Grummet, J.; Nguyen, N.; Spruyt, O. A review of the safety and efficacy of inhaled methoxyflurane as an analgesic for outpatient procedures. Br. J. Anaesth. 2018, 120, 1040–1048. [Google Scholar] [CrossRef] [Green Version]
- Davenport, H.T.; Quan, P. Methoxyflurane Anesthesia in Pediatrics: A Clinical Report. Can. Med. Assoc. J. 1964, 91, 1291–1294. [Google Scholar] [CrossRef]
- Grindlay, J.; Babl, F.E. Review article: Efficacy and safety of methoxyflurane analgesia in the emergency department and prehospital setting: Review Article. EMA Emerg. Med. Australas. 2009, 21, 4–11. [Google Scholar] [CrossRef]
- Prescribing Information and Adverse Event Reporting [Internet]. Available online: https://penthrox.co.uk/healthcare/prescribing-information-and-adverse-event-reporting/ (accessed on 1 August 2022).
- Kingon, A.; Yap, T.; Bonanno, C.; Sambrook, P.; Mccullough, M. Methoxyflurane: A review with emphasis on its role in dental practice. Aust. Dent. J. 2016, 61, 157–162. [Google Scholar] [CrossRef] [Green Version]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- R: Getting Help with R [Internet]. Available online: https://www.r-project.org/help.html (accessed on 10 April 2022).
- Studio–RStudio [Internet]. Available online: https://www.rstudio.com/products/rstudio/ (accessed on 9 July 2022).
- Borobia, A.M.; Collado, S.G.; Cardona, C.C.; Pueyo, R.C.; Alonso, C.F.; Torres, I.P.; González, M.C.; Casal Codesido, J.R.; Betegón, M.A.; Barcela, L.A.; et al. Inhaled Methoxyflurane Provides Greater Analgesia and Faster Onset of Action Versus Standard Analgesia in Patients with Trauma Pain: InMEDIATE: A Randomized Controlled Trial in Emergency Departments. Ann. Emerg. Med. 2020, 75, 315–328. [Google Scholar] [CrossRef] [Green Version]
- Gaskell, A.L.; Jephcott, C.G.; Smithells, J.R.; Sleigh, J.W. Self-administered methoxyflurane for procedural analgesia: Experience in a tertiary Australasian centre. Anaesthesia 2016, 71, 417–423. [Google Scholar] [CrossRef] [Green Version]
- Firn, S. Methoxyflurane analgesia for burns dressings and other painful ward procedures in children. Br. J. Anaesth. 1972, 44, 517–522. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, N.; Toscano, L.; Lawrence, M.; Phan, V.-A.; Singh, R.; Bampton, P.; Fraser, R.; Holloway, R.; Schoeman, M. Portable inhaled methoxyflurane is feasible and safe for colonoscopy in subjects with morbid obesity and/or obstructive sleep apnea. Endosc. Int. Open 2015, 3, E487–E493. [Google Scholar] [CrossRef] [Green Version]
- Ozainne, F.; Cottet, P.; Rial, C.L.; Von Düring, S.; Fehlmann, C.A. Methoxyflurane in Non-Life-Threatening Traumatic Pain—A Retrospective Observational Study. Healthcare 2021, 9, 1360. [Google Scholar] [CrossRef] [PubMed]
- Babl, F.E.; Jamison, S.R.; Spicer, M.; Bernard, S. Inhaled methoxyflurane as a prehospital analgesic in children. EMA Emerg. Med. Australas. 2006, 18, 404–410. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n = 12 | |
| Patient characteristics | |
| Age, years | 56 (50–68) |
| Sex, male | 8 (67%) |
| BMI #, kg/m2 | 26.5 (22.8–28.2) |
| ASA classification | |
| ASA II | 7 (58%) |
| ASA III | 5 (42%) |
| Burn related characteristics | |
| Percentage of total burn surface area, % | 10.5 (4.5–19.2) |
| Days since burn injury, days | 22 (17–34) |
| Days since last operation, days | 6 (5–7) |
| Pain level before procedure % | 35 (18–50) |
| Procedure duration, minutes | 44 (34–56) |
| Ongoing pain treatment | |
| Oral analgesics | |
| Paracetamol, 1 g × 2–4 | 12 (100%) |
| Gabapentin, 300–600 mg × 2–3 | 10 (83%) |
| Ibuprofen, 400 mg × 2–3 | 4 (33%) |
| Morphine ¤ | 8 (67%) |
| Others ¥ | 4 (33%) |
| Intravenous | |
| Morphine ¤ | 2 (17) |
| 95% CI | |||
| Primary outcome | |||
| Maximal pain during the procedure % | 60 (37–80) | ||
| Secondary outcomes | |||
| Procedure related outcomes | |||
| Patient satisfaction % | 96 (69–100) | ||
| Nurse-assessed pain level % | 57 (2–6]) | ||
| Patient movement | 1 (8%) | ||
| Serious adverse events and reactions | 0 (0%) | 0–24% | |
| Adverse events | |||
| During the procedure ¤ | 1 (8%) | 1–35% | |
| 1 week after the procedure $ | 1 (8%) | 1–35% | |
| Before | After | ||
| Physiologic changes | |||
| Oxygen saturation, % | 98 (97–99) | 99 (98–100) | |
| Pulse, beats/min | 92 (72–99) | 89 (73–96) | |
| MAP §, mmHg | 106 (96–112) | 97 (87–109) | |
| Lowest saturation during procedure, % | 96 (94–98) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Creutzburg, A.; Vestergaard, M.R.; Pape, P.; Hjelmdal, C.; Rangatchew, F.; Holmgaard, R.; Rasmussen, L.S. Methoxyflurane for Relief of Procedural Pain in Burn Patients: A Prospective Single-Centre Evaluation Study. Eur. Burn J. 2022, 3, 780-787. https://doi.org/10.3390/ebj3040047
Creutzburg A, Vestergaard MR, Pape P, Hjelmdal C, Rangatchew F, Holmgaard R, Rasmussen LS. Methoxyflurane for Relief of Procedural Pain in Burn Patients: A Prospective Single-Centre Evaluation Study. European Burn Journal. 2022; 3(4):780-787. https://doi.org/10.3390/ebj3040047
Chicago/Turabian StyleCreutzburg, Andreas, Martin R. Vestergaard, Pernille Pape, Caroline Hjelmdal, Filip Rangatchew, Rikke Holmgaard, and Lars S. Rasmussen. 2022. "Methoxyflurane for Relief of Procedural Pain in Burn Patients: A Prospective Single-Centre Evaluation Study" European Burn Journal 3, no. 4: 780-787. https://doi.org/10.3390/ebj3040047