

Comparison of the Airway Anatomy between Infants and Three Pediatric Simulators: A Radiological Study on Premature Anne, Infant AM Trainer and Simbaby Manikins

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
- Premature Anne (female baby born at 25 weeks—low fidelity);
- Infant Airway Management Trainer (three-month-old infant—low fidelity);
- SimBaby (9-month-old pediatric patient—high fidelity).
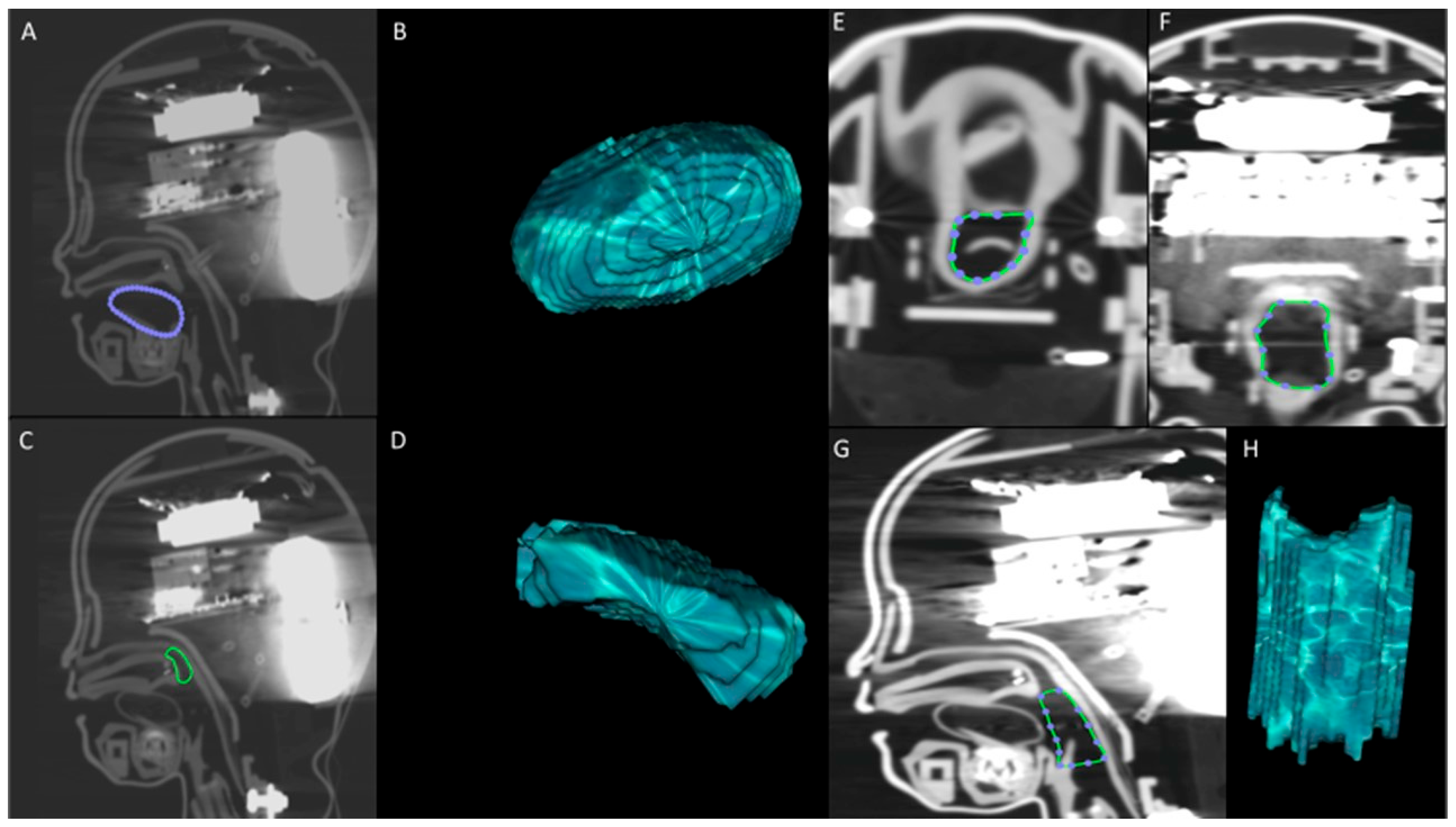
2.1. Radiological Measurements
- Sagittal T2 weighted TSE sequence (turbo spin echo; slice thickness: 4 mm, interspace: 1 mm, matrix: 512 × 512).
- Sagittal T1 weighted SPGR sequence (spoiled gradient recalled echo; slice thickness: 3.5, interspace: 1 mm, matrix: 512 × 512).
- 3D FIESTA sequence (fast imaging employing steady-state acquisition; slice thickness: 1 mm, interspace: 0, matrix: 512 × 512)
2.2. Primary Outcome and Statistical Analysis
- Adequate reproduction of airway, if the mean value was included between ±1 SD of the mean of the population;
- Partially adequate reproduction of airway, if the mean value of the simulator was over ±1 SD but comprised ± 1.96 SD of the mean of the population;
- Inadequate reproduction of airway, if the mean value of the simulator was <−1.96 or >1.96 SD from the mean of the population.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Je, S.; Cho, Y.; Choi, H.J.; Kang, B.; Lim, T.; Kang, H. An application of the learning curve-cumulative summation test to evaluate training for endotracheal intubation in emergency medicine. Emerg. Med. J. 2015, 32, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Garza, A.G.; Gratton, M.C.; Coontz, D.; Noble, E.; Ma, O.J. Effect of paramedic experience on orotracheal intubation success rates. J. Emerg. Med. 2003, 25, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.; van Wageningen, B.; Hendriks, I.; Eijk, R.; Edwards, M.; Hoogerwerf, N.; Biert, J. First-pass intubation success rate during rapid sequence induction of prehospital anaesthesia by physicians versus paramedics. Eur. J. Emerg. Med. 2015, 22, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Sagarin, M.J.; Barton, E.D.; Chng, Y.M.; Walls, R.M.; National Emergency Airway Registry Investigators. Airway management by US and Canadian emergency medicine residents: A multicenter analysis of more than 6000 endotracheal intubation attempts. Ann. Emerg. Med. 2005, 46, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Sayre, M.R.; Sakles, J.C.; Mistler, A.F.; Evans, J.L.; Kramer, A.T.; Pancioli, A.M. Field trial of endotracheal intubation by basic EMTs. Ann. Emerg. Med. 1998, 31, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.D.; Paris, P.M.; Pelton, G.H.; Garretson, D. Effect of varied training techniques on field endotracheal intubation success rates. Ann. Emerg. Med. 1984, 13, 1032–1036. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.B.; Taqueti, V.R. A brief history of the development of mannequin simulators for clinical education and training. Postgrad. Med. J. 2008, 84, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, M.B.; Wang, S.C.; Ross, B.E.; Holcombe, S.A.; Kempski, K.M.; Blackburn, A.N.; DeLorenzo, R.A.; Ryan, K.L. Anatomic accuracy of airway training manikins compared with humans. Anaesthesia 2021, 76, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Schalk, R.; Eichler, K.; Bergold, M.N.; Weber, C.F.; Zacharowski, K.; Meininger, D.; Byhahn, C.; Mutlak, H. A radiographic comparison of human airway anatomy and airway manikins--Implications for manikin-based testing of artificial airways. Resuscitation 2015, 92, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Schebesta, K.; Hupfl, M.; Rossler, B.; Ringl, H.; Muller, M.P.; Kimberger, O. Degrees of reality: Airway anatomy of high-fidelity human patient simulators and airway trainers. Anesthesiology 2012, 116, 1204–1209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schebesta, K.; Hupfl, M.; Ringl, H.; Machata, A.M.; Chiari, A.; Kimberger, O. A comparison of paediatric airway anatomy with the SimBaby high-fidelity patient simulator. Resuscitation 2011, 82, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Schebesta, K.; Spreitzgrabner, G.; Hörner, E.; Hüpfl, M.; Kimberger, O.; Rössler, B. Validity and fidelity of the upper airway in two high-fidelity patient simulators. Minerva Anestesiol. 2015, 81, 12–18. [Google Scholar] [PubMed]
- Kennedy, C.C.; Cannon, E.K.; Warner, D.O.; Cook, D.A. Advanced airway management simulation training in medical education: A systematic review and meta-analysis. BMC Anesthesiol. 2014, 42, 169–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doleman, B.; Blackwell, J.; Karangizi, A.; Butt, W.; Bhalla, A.; Lund, J.N.; Williams, J.P. Anaesthetists stress is induced by patient ASA grade and may impair non-technical skills during intubation. Acta Anaesthesiol. Scand. 2016, 60, 910–916. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| DISTANCES |
| A. Horizontal distance from the outermost portion of lower lip to the posterior pharyngeal wall |
| B. Horizontal distance from the lower alveolar process to the posterior pharyngeal wall |
| C. Oblique diameter of the tongue |
| D. Horizontal distance from the center of the tongue to posterior pharyngeal wall |
| E. Horizontal distance from the edge of the tongue to posterior pharyngeal wall |
| F. Horizontal distance from the canter of the soft palate to posterior pharyngeal wall |
| G. Horizontal distance from the vallecula to posterior pharyngeal wall |
| H. Horizontal distance from the tip of the epiglottis to the posterior pharyngeal wall |
| I. Curved length of the soft palate |
| J. Distance from the vallecula to the tip of the epiglottis |
| K. Distance from the posterior base of the epiglottis to the tip of the epiglottis |
| L. Height of the soft palate |
| M. Vertical distance from the base of the hard palate to the tip of the epiglottis |
| N. Vertical distance from the base of the hard palate to the vallecula |
| VOLUMES |
| O. Tongue |
| P. Retropalatal airspace |
| Q. Retroglossal airspace |
| Variable (Distances or Volumes) | Infants Mean ± SD | Manikins Mean ± SD | p Value | SimBaby | Premature Anne | Infant AM Trainer |
|---|---|---|---|---|---|---|
| A. Outermost portion of lower lip to posterior pharyngeal wall (cm) | 4.54 ± 0.31 | 6.44 ± 0.36 | <0.001 | 6.40 ↑ | 6.86 ↑ | 6.05 ↑ |
| B. Lower alveolar process to posterior pharyngeal wall (cm) | 3.46 ± 0.26 | 4.96 ± 0.35 | <0.001 | 5.15 ↑ | 5.23 ↑ | 4.50 ↑ |
| C. Oblique diameter of the tongue (cm) | 2.12 ± 0.28 | 2.46 ± 0.70 | 0.19 | 2.92 ↑ | 1.53 ↓ | 2.92 ↑ |
| D. Centre of the tongue to posterior pharyngeal wall (cm) | 2.07 ± 0.21 | 2.83 ± 0.30 | <0.001 | 2.85↑ | 3.16 ↑ | 2.48 ↑ |
| E. Edge of the tongue to posterior pharyngeal wall (cm) | 1.36 ± 0.26 | 1.60 ± 0.36 | 0.08 | 1.66 ↑ | 1.97 ↑ | 1.16 |
| F. Canter of the soft palate to posterior pharyngeal wall (cm) | 0.91 ± 0.13 | 1.26 ± 0.39 | 0.03 | 0.80 | 1.69 ↑ | 1.29 ↑ |
| G. Vallecula to posterior pharyngeal wall (cm) | 0.74 ± 0.18 | 1.48 ± 0.27 | <0.001 | 1.34 ↑ | 1.84 ↑ | 1.27 ↑ |
| H. Tip of the epiglottis to posterior pharyngeal wall (cm) | 0.39 ± 0.10 | 1.11 ± 0.45 | 0.001 | 0.64 ↑ | 1.66 ↑ | 1.01 ↑ |
| I. Curved length of the soft palate (cm) | 2.04 ± 0.28 | 1.26 ± 0.32 | <0.001 | 1.43 ↓ | 0.84 ↓ | 1.52 ↓ |
| J. Vallecula to tip of the epiglottis (cm) | 0.70 ± 0.15 | 1.03 ± 0.37 | 0.03 | 1.41 ↑ | 0.57 | 1.12 ↑ |
| K. Posterior base of the epiglottis to tip of the epiglottis (cm) | 0.68 ± 0.13 | 1.13 ± 0.38 | 0.007 | 1.58 ↑ | 1.09 ↑ | 0.71 |
| L. Height of the soft palate (cm) | 1.23 ± 0.32 | 1.44 ± 0.31 | 0.09 | 1.48 | 1.08 | 1.78 |
| M. Base of the soft palate to tip of the epiglottis (cm) | 1.78 ± 0.46 | 2.55 ± 0.48 | 0.001 | 2.45 ↑ | 2.06 | 3.13 ↑ |
| N. Base of the soft palate to vallecula (cm) | 2.26 ± 0.51 | 3.35 ± 0.76 | 0.002 | 3.41 ↑ | 2.47 | 4.18 ↑ |
| O. Tongue Volume (cm3) | 5.79 ± 1.21 | 6.08 ± 0.94 | 0.46 | 7.10 ↑ | 4.94 | 6.22 |
| P. Retropalatal airspace Volume (cm3) | 1.10 ± 0.30 | 1.14 ± 0.32 | 0.74 | 1.38 | 0.72 ↓ | 1.33 |
| Q. Retroglossal airspace Volume (cm3) | 0.97 ± 0.26 | 5.79 ± 1.59 | <0.001 | 6.52 ↑ | 7.15 ↑ | 3.69 ↑ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Via, L.; Falsaperla, D.; Merola, F.; Messina, S.; Lanzafame, B.; Borzì, S.R.; Basile, A.; Sanfilippo, F. Comparison of the Airway Anatomy between Infants and Three Pediatric Simulators: A Radiological Study on Premature Anne, Infant AM Trainer and Simbaby Manikins. Prosthesis 2023, 5, 602-609. https://doi.org/10.3390/prosthesis5030042
La Via L, Falsaperla D, Merola F, Messina S, Lanzafame B, Borzì SR, Basile A, Sanfilippo F. Comparison of the Airway Anatomy between Infants and Three Pediatric Simulators: A Radiological Study on Premature Anne, Infant AM Trainer and Simbaby Manikins. Prosthesis. 2023; 5(3):602-609. https://doi.org/10.3390/prosthesis5030042
Chicago/Turabian StyleLa Via, Luigi, Daniele Falsaperla, Federica Merola, Simone Messina, Bruno Lanzafame, Santo Riccardo Borzì, Antonio Basile, and Filippo Sanfilippo. 2023. "Comparison of the Airway Anatomy between Infants and Three Pediatric Simulators: A Radiological Study on Premature Anne, Infant AM Trainer and Simbaby Manikins" Prosthesis 5, no. 3: 602-609. https://doi.org/10.3390/prosthesis5030042