
Quantification of the Influence of Prosthetic Ankle Stiffness on Static Balance Using Lower Limb Prosthetic Simulators

Abstract
:1. Introduction
2. Methods
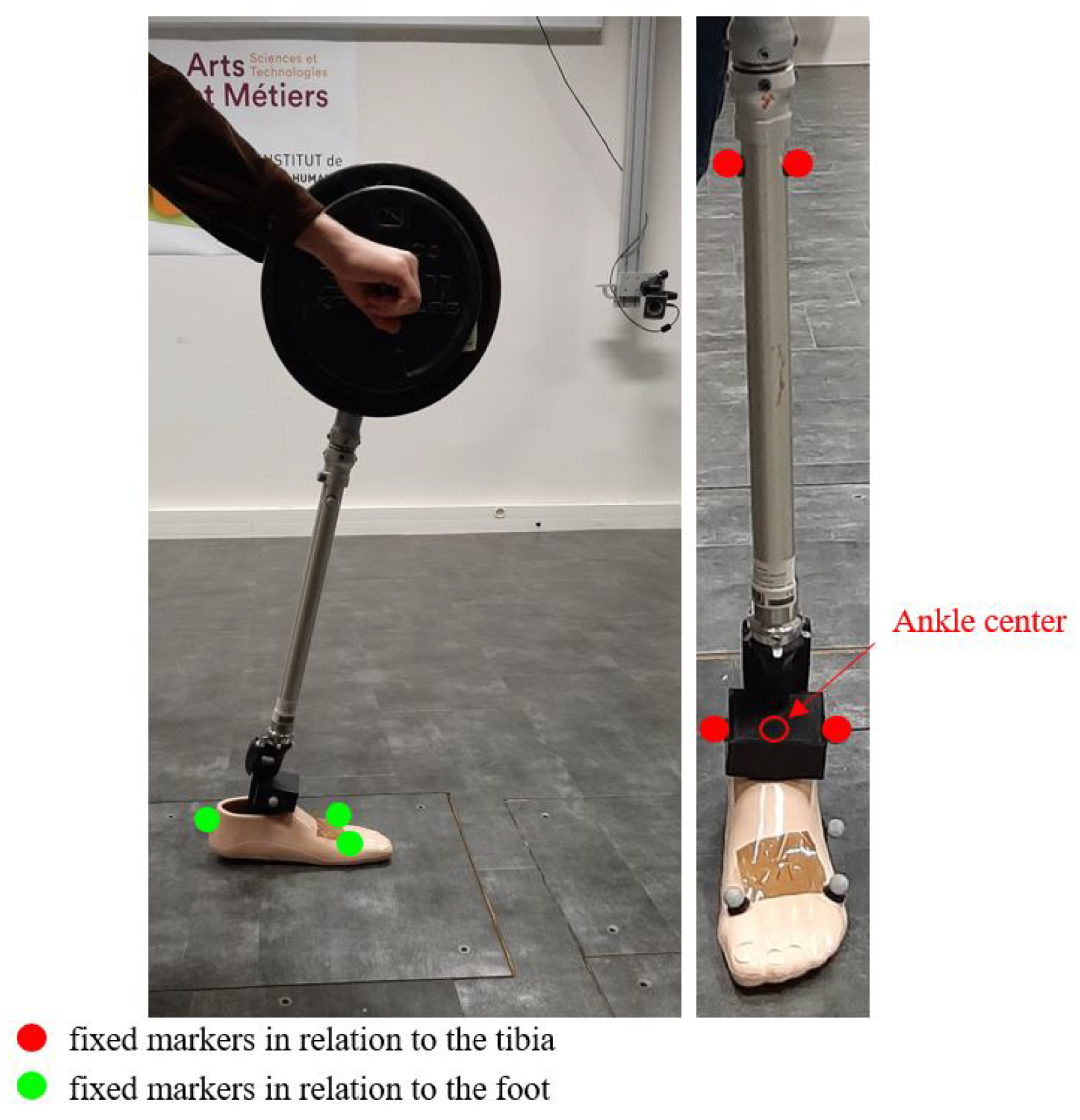
2.1. Stiffness Characterization
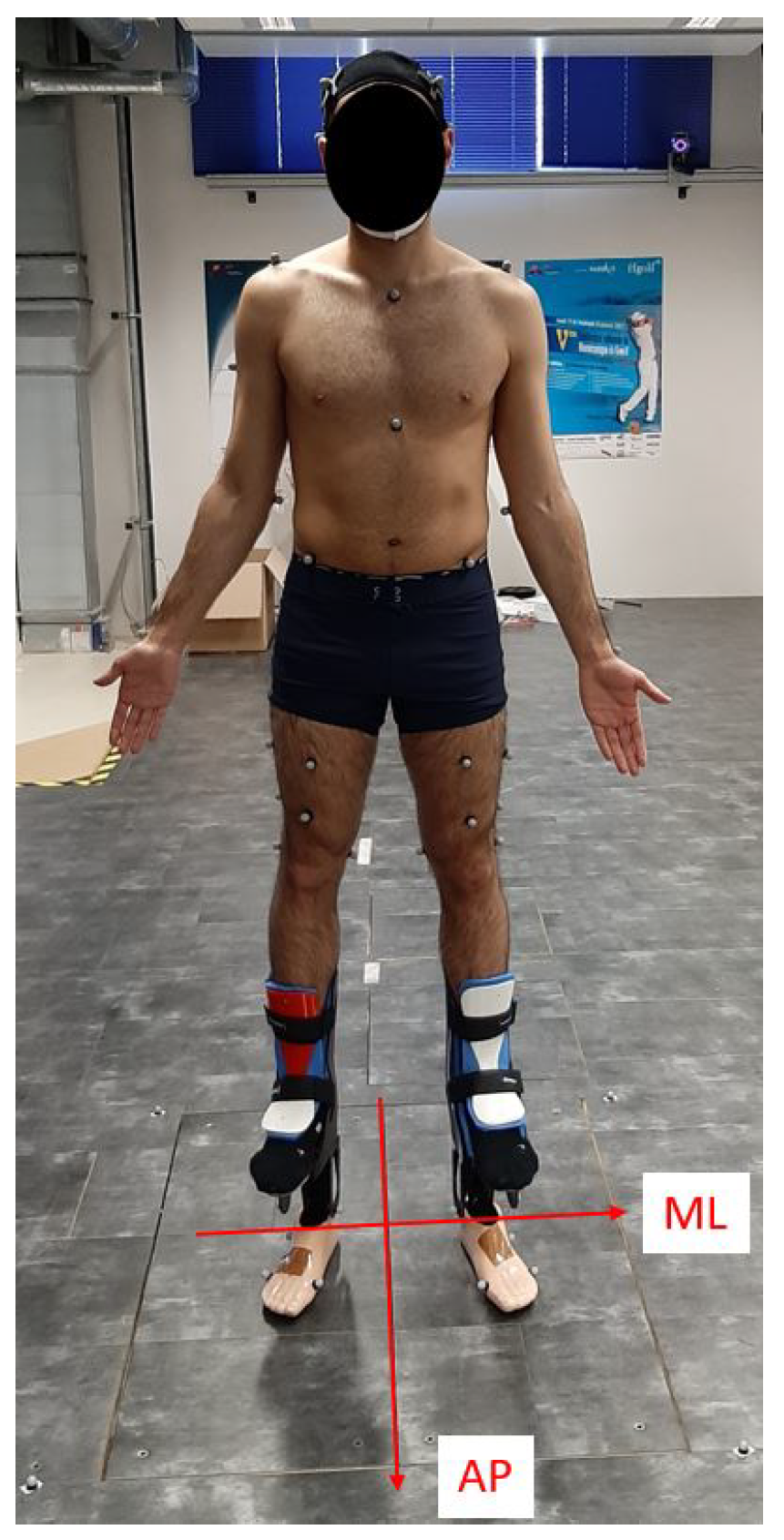
2.2. Subjects and Protocol
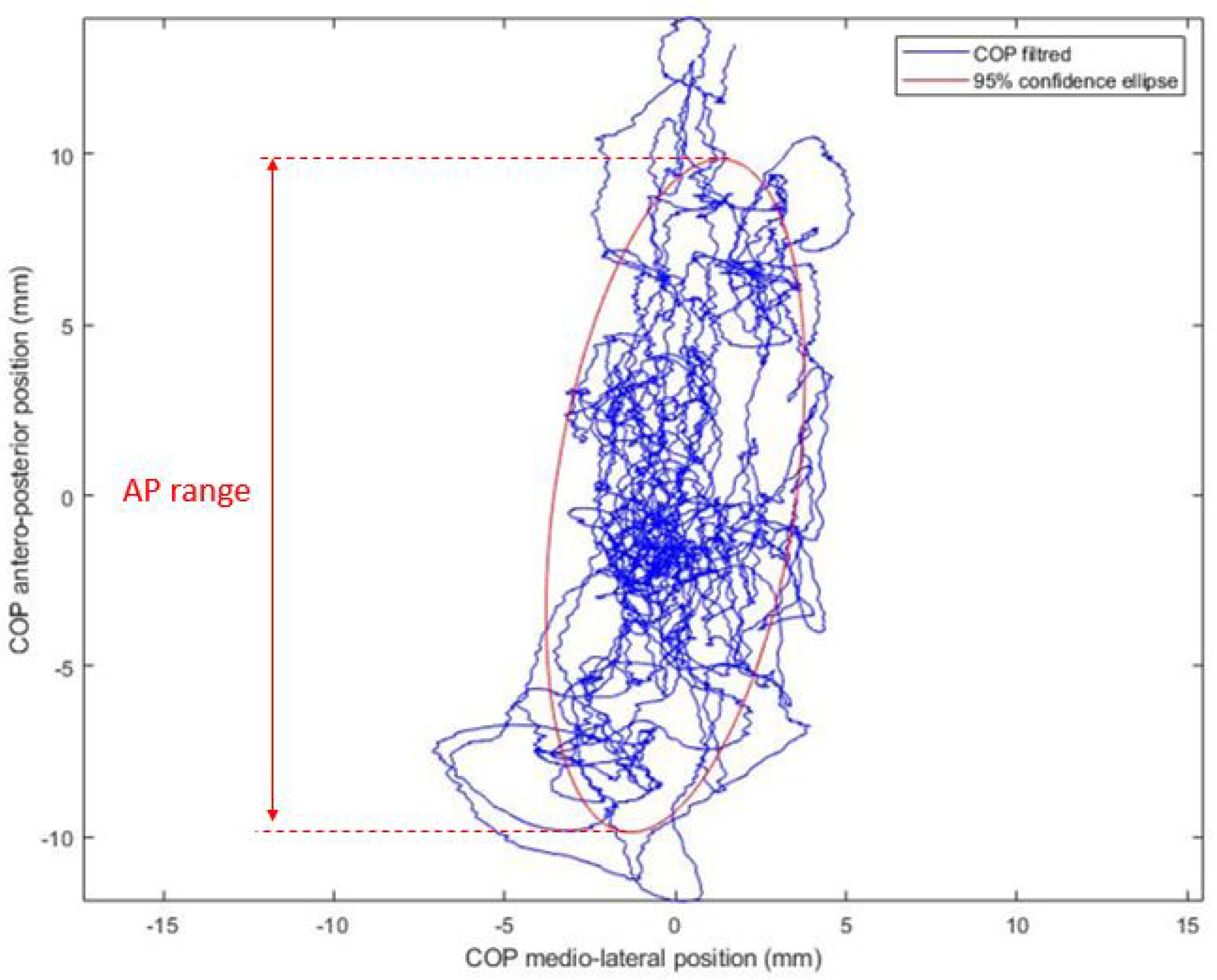
2.3. Data Processing
3. Results
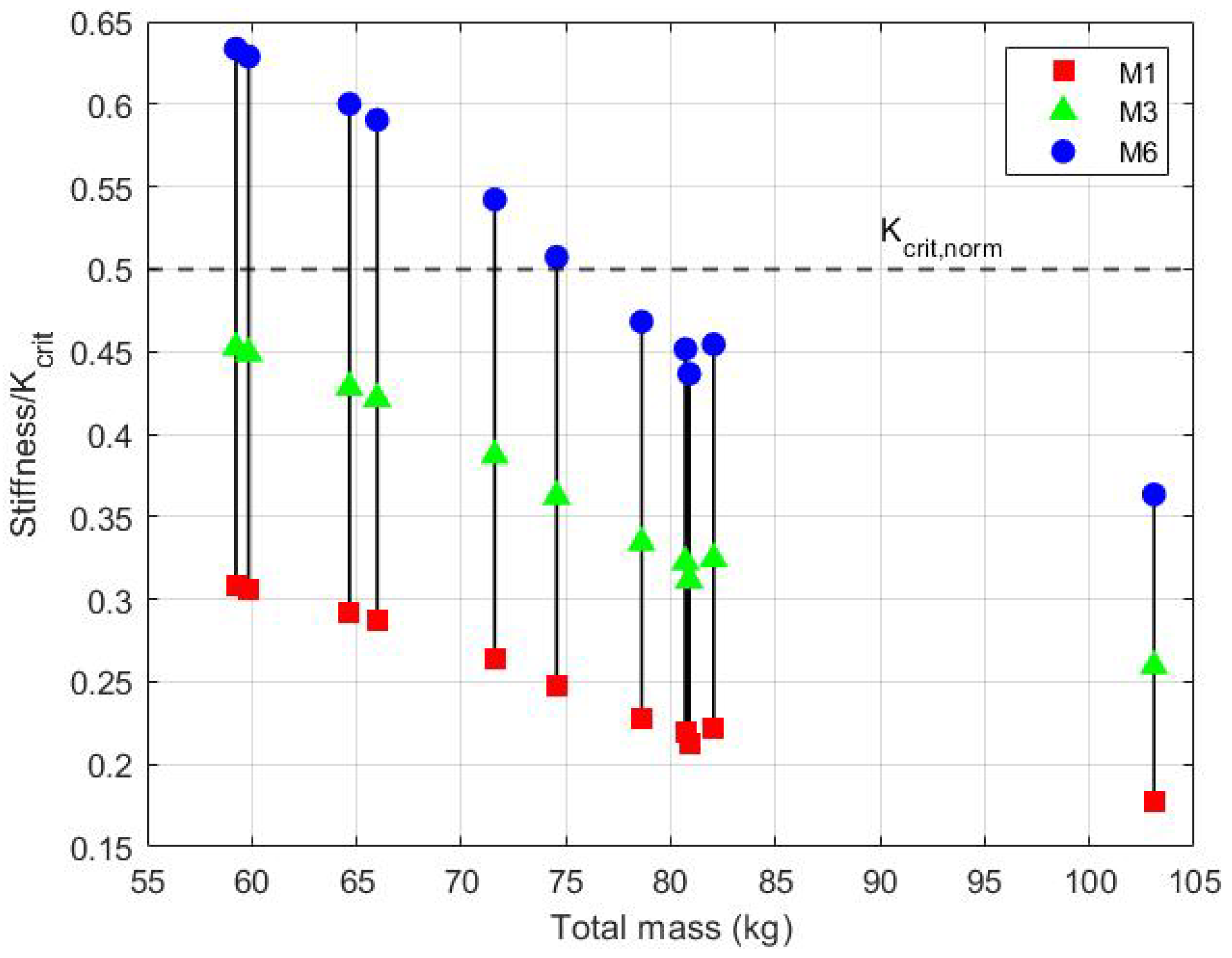
3.1. Ankle Stiffness
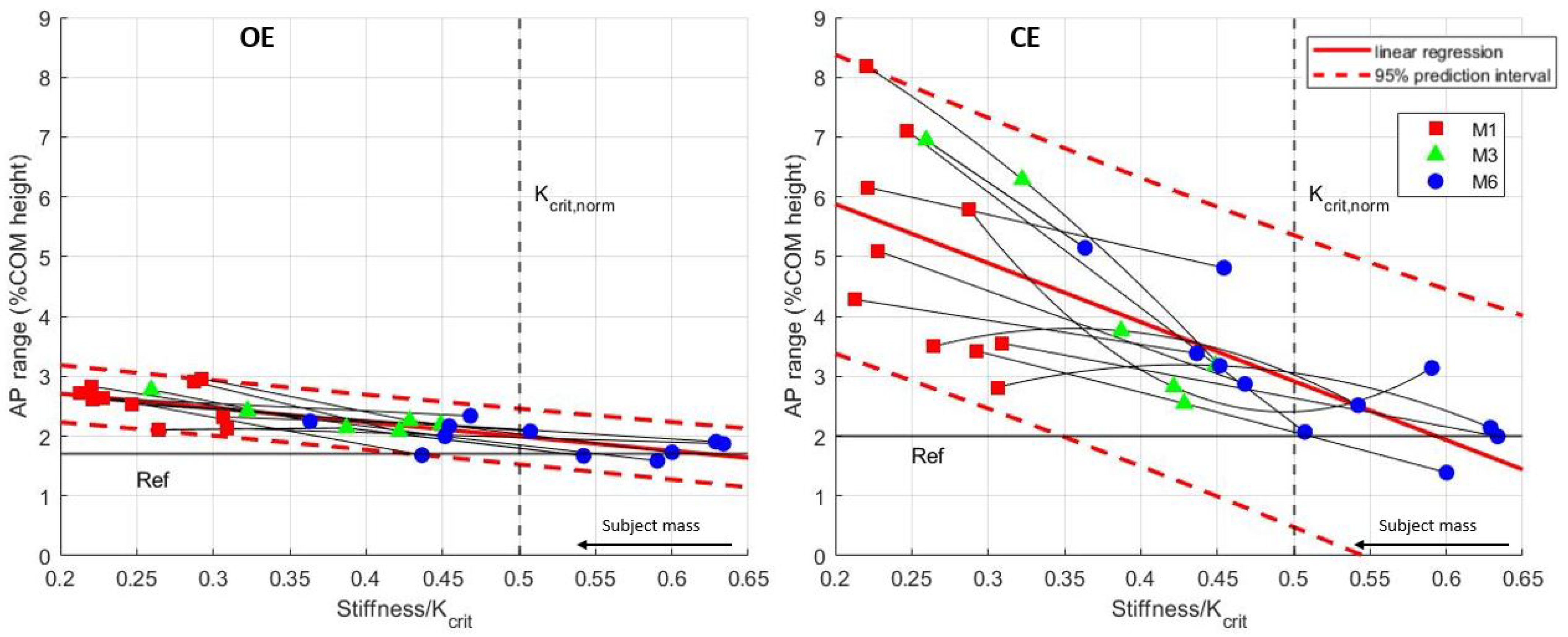
3.2. Static Balance Depending on the Prosthetic Ankle Stiffness
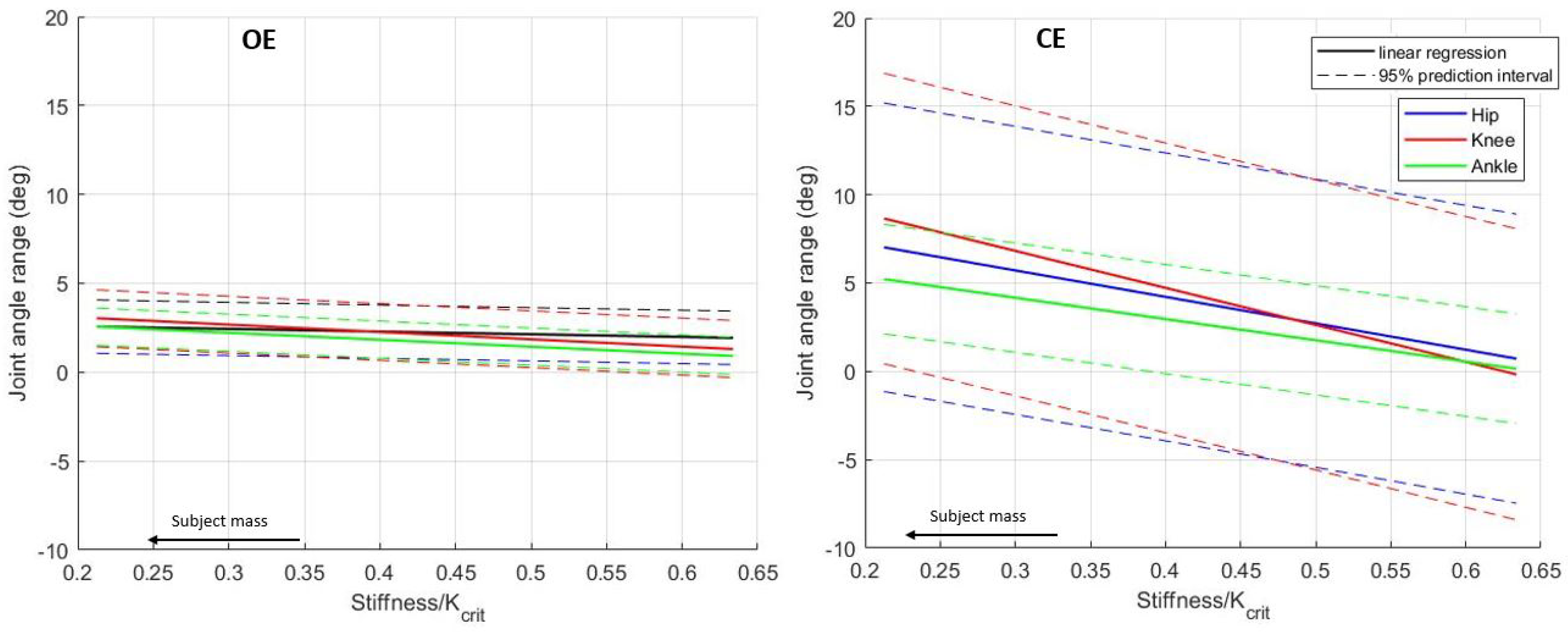
3.3. Joint Angles
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANOVA | Analyse Of Variance |
| AP | Antero-Posterior |
| CE | Closed Eyes |
| CI | Confidence Intervals |
| COM | Center Of Mass |
| COP | Center Of Pressure |
| ESAR | Energy Storage And Release |
| ML | Medio-Lateral |
| OE | Open Eyes |
| ROM | Range Of Motion |
| sd | standard deviation |
References
- Ziegler-Graham, K.; MacKenzie, E.J.; Ephraim, P.L.; Travison, T.G.; Brookmeyer, R. Estimating the Prevalence of Limb Loss in the United States: 2005 to 2050. Arch. Phys. Med. Rehabil. 2008, 89, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Kamali, M.; Karimi, M.; Eshraghi, A.; Omar, H. Influential factors in stability of lower-limb amputees. Am. J. Phys. Med. Rehabil. 2013, 92, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Quai, T.M.; Brauer, S.G.; Nitz, J.C. Somatosensation, circulation and stance balance in elderly dysvascular transtibial amputees. Clin. Rehab. 2005, 19, 668–676. [Google Scholar]
- Nadollek, H.; Brauer, S.; Isles, R. Outcomes after trans-tibial amputation: The relationship between quiet stance ability, strength of hip abductor muscles and gait. Physiother. Res. Int. 2002, 7, 203–214. [Google Scholar]
- Pedrinelli, A.; Saito, M.; Coelho, R.F.; Fontes, R.B.V.; Guarniero, R. Comparative study of the strength of the flexor and extensor muscles of the knee through isokinetic evaluation in normal subjects and patients subjected to trans-tibial amputation. Prosthet. Orthot. Int. 2002, 26, 195–205. [Google Scholar] [CrossRef] [Green Version]
- Butowicz, C.; Yoder, A.; Farrokhi, S.; Mazzone, B.; Hendershot, B. Lower limb joint-specific contributions to standing postural sway in persons with unilateral lower limb loss. Gait Posture 2021, 89, 109–114. [Google Scholar]
- Hermodsson, Y.; Ekdahl, C.; Persson, B.; Roxendal, G. Standing balance in trans-tibia1 amputees following vascular disease or trauma: A comparative study with healthy subjects. Prosthet. Orthot. Int. 1994, 18, 150–158. [Google Scholar] [CrossRef] [Green Version]
- Winter, D. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar]
- Hof, A.L. The equations of motion for a standing human reveal three mechanisms for balance. J. Biomech. 2007, 40, 451–457. [Google Scholar] [CrossRef]
- Winter, D.A.; Patla, A.E.; Prince, F.; Ishac, M.; Gielo-Perczak, K. Stiffness Control of Balance in Quiet Standing. J. Neurophysiol. 1998, 80, 1211–1221. [Google Scholar] [CrossRef] [Green Version]
- Hansen, A.H.; Wang, C.C. Effective rocker shapes used by able-bodied persons for walking and fore-aft swaying: Implications for design of ankle–foot prostheses. Gait Posture 2010, 32, 181–184. [Google Scholar] [PubMed] [Green Version]
- Fey, N.; Klute, G.; Neptune, R. The influence of energy storage and return foot stiffness on walking mechanics and muscle activity in below-knee amputees. Clin. Biomech. 2011, 26, 1025–1032. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.; Meier, M.; Sessoms, P.; Childress, D. The effects of prosthetic foot roll-over shape arc length on the gait of trans-tibial prosthesis users. Prosthet. Orthot. Int. 2006, 30, 286–299. [Google Scholar] [CrossRef]
- Kerkum, Y.; Philippart, W.; Houdijk, H. The effects of footplate stiffness on push-off power when walking with posterior leaf spring ankle-foot orthoses. Clin. Biomech. 2021, 88, 105422. [Google Scholar] [CrossRef]
- Klodd, E.; Hansen, A.; Fatone, S.; Edwards, M. Effects of prosthetic foot forefoot flexibility on gait of unilateral transtibial prosthesis users. J. Rehabil. Res. Dev. 2010, 47, 899. [Google Scholar]
- Major, M.; Twiste, M.; Kenney, L.; Howard, D. The effects of prosthetic ankle stiffness on ankle and knee kinematics, prosthetic limb loading, and net metabolic cost of trans-tibial amputee gait. Clin. Biomech. 2014, 29, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Major, M.; Twiste, M.; Kenney, L.; Howard, D. The effects of prosthetic ankle stiffness on stability of gait in people with transtibial amputation. J. Rehabil. Res. Dev. 2016, 53, 839–852. [Google Scholar] [CrossRef]
- Shepherd, M.; Azocar, A.; Major, M.; Rouse, E. Amputee perception of prosthetic ankle stiffness during locomotion. J. Neuroeng. Rehabil. 2018, 15, 99. [Google Scholar]
- Ku, P.X.; Abu Osman, N.A.; Wan Abas, W.A.B. Balance control in lower extremity amputees during quiet standing: A systematic review. Gait Posture 2014, 39, 672–682. [Google Scholar]
- Koehler-McNicholas, S.R.; SavvasSlater, B.C.; Koester, K.; Nickel, E.A.; Ferguson, J.E.; Hansen, A.H. Bimodal ankle-foot prosthesis for enhanced standing stability. PLoS ONE 2018, 13, e0204512. [Google Scholar] [CrossRef] [Green Version]
- Kolarova, B.; Janura, M.; Svoboda, Z.; Elfmark, M. Limits of stability in persons with transtibial amputation with respect to prosthetic alignment alterations. Arch. Phys. Med. Rehabil. 2013, 94, 2234–2240. [Google Scholar] [CrossRef] [PubMed]
- Molina-Rueda, F.; Molero-Sánchez, A.; Carratalá-Tejada, M.; Cuesta-Gómez, A.; Miangolarra-Page, J.; Alguacil-Diego, I. Limits of stability in patients with vascular (due to diabetes) and nonvascular unilateral transtibial amputation: A cross-sectional study. Int. J. Rehabil. Res. 2017, 40, 227–231. [Google Scholar]
- Pickerill, M.; Harter, R. Validity and reliability of limits-of-stability testing: A comparison of 2 postural stability evaluation devices. J. Athl. Train. 2011, 46, 600–606. [Google Scholar] [CrossRef] [Green Version]
- Inkol, K.A.; Vallis, L.A. Modelling the dynamic margins of stability for use in evaluations of balance following a support-surface perturbation. J. Biomech. 2019, 95, 109302. [Google Scholar] [CrossRef] [PubMed]
- Chiari, L.; Rocchi, L.; Cappello, A. Stabilometric parameters are affected by anthropometry and foot placement. Clin. Biomech. 2002, 17, 666–677. [Google Scholar] [CrossRef]
- Shepherd, M.; Simon, A.; Zisk, J.; Hargrove, L. Patient-preferred prosthetic ankle-foot alignment for ramps and level-ground walking. Trans. Neural Syst. Rehabil. Eng. 2021, 29, 52–59. [Google Scholar]
- Hansen, A.; Childress, D. Investigations of roll-over shape: Implications for design, alignment, and evaluation of ankle-foot prostheses and orthoses. Disabil. Rehabil. 2010, 32, 2201–2209. [Google Scholar] [CrossRef]
- Nederhand, M.J.; Van Asseldonk, E.H.; van der Kooij, H.; Rietman, H.S. Dynamic Balance Control (DBC) in lower leg amputee subjects; contribution of the regulatory activity of the prosthesis side. Clin. Biomech. 2012, 27, 40–45. [Google Scholar] [CrossRef]
- Arifin, N.; Abu Osman, N.A.; Ali, S.; Wan Abas, W.A. The effects of prosthetic foot type and visual alteration on postural steadiness in below-knee amputees. Biomed. Eng. Online 2014, 13, 23. [Google Scholar] [CrossRef]
- Groothuis, A.; Houdijk, H. The effect of prosthetic alignment on prosthetic and total leg stiffness while running with simulated running-specific prostheses. Front. Sports Act. Living 2019, 1, 16. [Google Scholar] [CrossRef] [Green Version]
- Curtze, C.; Hof, A.; van Keeken, H.; Halbertsma, J.; Postema, K.; Otten, B. Comparative roll-over analysis of prosthetic feet. J. Biomech. 2009, 42, 1746–1753. [Google Scholar] [CrossRef]
- Pillet, H.; Drevelle, X.; Bonnet, X.; Villa, C.; Martinet, N.; Sauret, C.; Bascou, J.; Loiret, I.; Djian, F.; Rapin, N.; et al. Apsic: Training and fitting amputees during situations of daily living. Intermed.-Range Ballist. Missile 2014, 35, 60–65. [Google Scholar] [CrossRef]
- Pillet, H.; Bonnet, X.; Lavaste, F.; Skalli, W. Evaluation of force plate-less estimation of the trajectory of the centre of pressure during gait. Gait Posture 2010, 31, 147–152. [Google Scholar] [PubMed]
- Dichgans, J.; Mauritz, K.H.; Allum, J.H.; Brandt, T. Postural sway in normals and atactic patients: Analysis of the stabilising and destabilizing effects of vision. Agressologie 1976, 17, 15–24. [Google Scholar] [PubMed]
- Popovic, R.; Pappas, I.P.I.; Nakazawa, K.; Keller, T.; Morari, M.; Dietz, V. Stability criterion for controlling standing in able-bodied subjects. J. Biomech. 2000, 10, 710–716. [Google Scholar] [CrossRef]
- Oliveira, L.F.; Simpson, D.M.; Nadal, J. Calculation of area of stabilometric signals using principal component analysis. Physiol. Meas. 1996, 17, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Clavel, L.; Attali, V.; Jacq, O.; Nierat, M.; Similowski, T.; Rouch, P.; Sandoz, B. Breathing through a spirometer perturbs balance. Comput. Methods Biomech. Biomed. Eng. 2017, 20, S41–S42. [Google Scholar] [CrossRef] [Green Version]
- Thomas-Pohl, M.; Villa, C.; Davot, J.; Bonnet, X.; Facione, J.; Lapeyre, E.; Bascou, J.; Pillet, H. Microprocessor prosthetic ankles: Comparative biomechanical evaluation of people with transtibial traumatic amputation during standing on level ground and slope. Disabil. Rehabil. Assist. Technol. 2019, 16, 17–26. [Google Scholar]
- Santos, B.R.; Delisle, A.; Larivière, C.; Plamondon, A.; Imbeau, D. Reliability of centre of pressure summary measures of postural steadiness in healthy young adults. Gait Posture 2008, 27, 408–415. [Google Scholar] [CrossRef]
- Albertsen, I.; Ghédira, M.; Gracies, J.; Hutin, E. Postural stability in young healthy subjects – impact of reduced base of support, visual deprivation, dual tasking. J. Electromyogr. Kinesiol. 2017, 33, 27–33. [Google Scholar]
- Sarroca, N.; Luesma, M.; Valero, J.; Del Caso, M.; Alonso, C.; Calleja, J.; Lorenzo, T.; Bayod, J.; Lahoz, M. Influence of insole material density in the stability of patients with prosthetic unilateral transtibial amputation. Sci. Rep. 2022, 12, 7854. [Google Scholar] [CrossRef] [PubMed]
- Toumi, A.; Simoneau-Buessinger, E.; Bassement, J.; Barbier, F.; Gillet, C.; Allard, P.; Leteneur, S. Standing posture and balance modalities in unilateral transfemoral and transtibial amputees. J. Bodyw. Mov. Ther. 2021, 27, 634–639. [Google Scholar] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Age | Sex | Mass | COM Height | Tested Prostheses | ||
|---|---|---|---|---|---|---|---|
| [kg] | [mm] | M1 | M3 | M6 | |||
| 1 | 22 | F | ✓ | ✓ | |||
| 2 | 25 | F | ✓ | ✓ | ✓ | ||
| 3 | 25 | F | ✓ | ✓ | ✓ | ||
| 4 | 28 | M | ✓ | ✓ | ✓ | ||
| 5 | 25 | M | ✓ | ✓ | ✓ | ||
| 6 | 24 | M | ✓ | ✓ | |||
| 7 | 24 | M | ✓ | ✓ | |||
| 8 | 24 | M | ✓ | ✓ | |||
| 9 | 40 | M | ✓ | ✓ | ✓ | ||
| 10 | 30 | M | ✓ | ✓ | |||
| 11 | 24 | M | ✓ | ✓ | |||
| Stiffness (Nm/rad) | |||
|---|---|---|---|
| M1 | M3 | M6 | |
| n cycles * | 7 | 7 | 10 |
| mean | |||
| sd | |||
| Configuration | Ref. | M6 | M3 | M1 | ||||
|---|---|---|---|---|---|---|---|---|
| Situation | OE | CE | OE | CE | OE | CE | OE | CE |
| AP range | ||||||||
| (% COM height) | ||||||||
| Ankle angle ROM | ||||||||
| (deg) | ||||||||
| Knee angle ROM | ||||||||
| (deg) | ||||||||
| Hip angle ROM | ||||||||
| (deg) | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Louessard, A.; Bonnet, X.; Catapano, A.; Pillet, H. Quantification of the Influence of Prosthetic Ankle Stiffness on Static Balance Using Lower Limb Prosthetic Simulators. Prosthesis 2022, 4, 636-647. https://doi.org/10.3390/prosthesis4040051
Louessard A, Bonnet X, Catapano A, Pillet H. Quantification of the Influence of Prosthetic Ankle Stiffness on Static Balance Using Lower Limb Prosthetic Simulators. Prosthesis. 2022; 4(4):636-647. https://doi.org/10.3390/prosthesis4040051
Chicago/Turabian StyleLouessard, Aude, Xavier Bonnet, Anita Catapano, and Helene Pillet. 2022. "Quantification of the Influence of Prosthetic Ankle Stiffness on Static Balance Using Lower Limb Prosthetic Simulators" Prosthesis 4, no. 4: 636-647. https://doi.org/10.3390/prosthesis4040051