
The Influence of Personality Traits on Specific Coping Styles and the Development of Posttraumatic Stress Symptoms following Acute Coronary Syndrome: A Cluster Analytic Approach

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
Procedure
2.2. Measures
2.3. 3-Month follow-up Measures
Personality Traits
Type-D (DS-14)
Alexithymia (TAS-20)
2.4. Resilience
2.5. Dependent Variables
2.6. Intervention
2.7. Data Analysis
3. Results
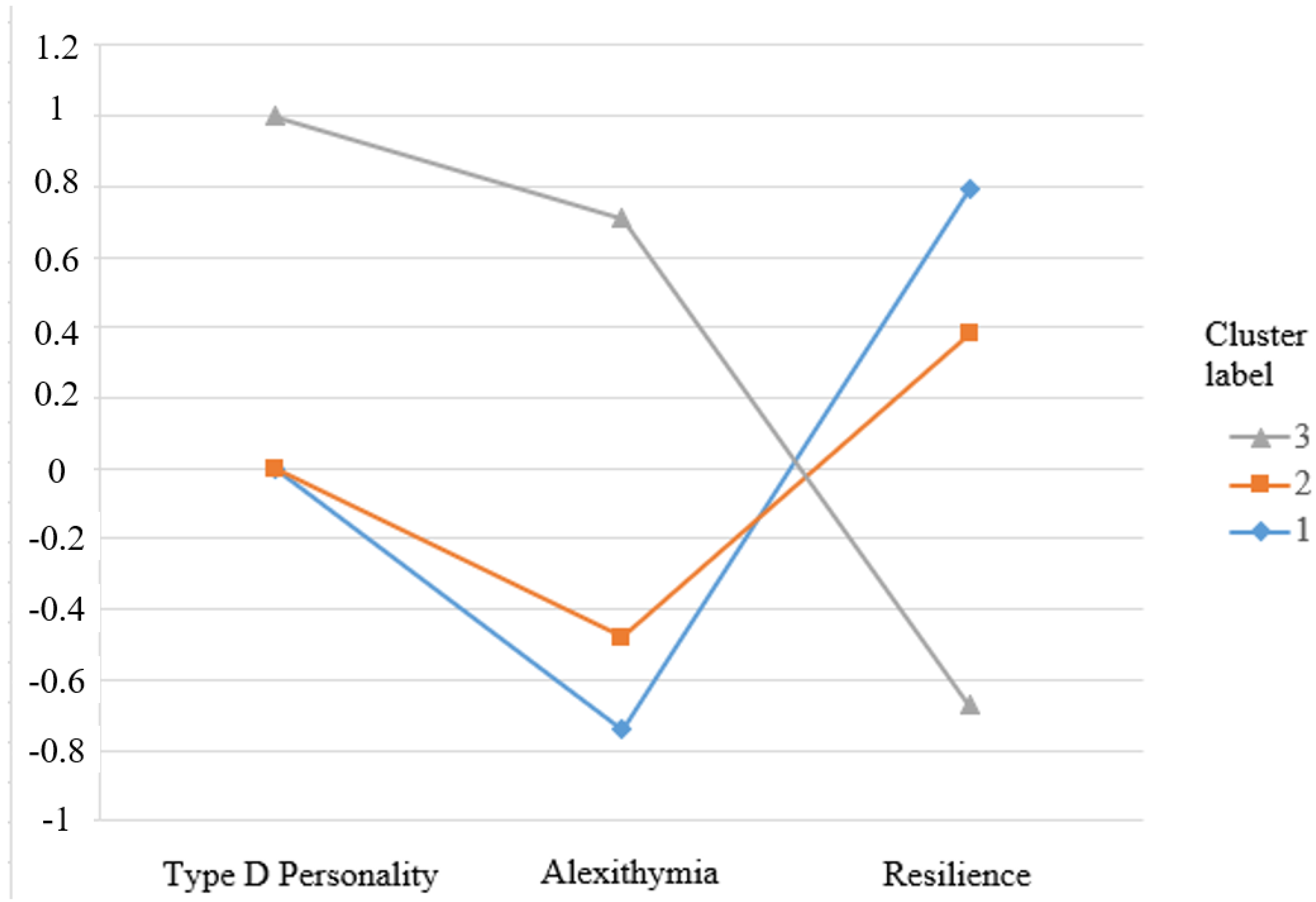
3.1. Cluster Analysis
3.2. Cluster Differences for Emotion Oriented Coping
3.3. Cluster Differences for Task Oriented Coping
3.4. Cluster Differences for Avoidant Coping
3.5. Cluster Differences for PTSD Symptoms
3.6. Secondary Analyses
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Edmondson, D.; Richardson, S.; Falzon, L.; Karina; Davidson, W.; Mills, M.A.; Neria, Y. Posttraumatic stress disorder prevalence and risk of recurrence in acute coronary syndrome patients: A meta-analytic review. PLoS ONE 2012, 7, e38915. [Google Scholar] [CrossRef] [Green Version]
- Jacquet-Smailovic, M.; Tarquinio, C.; Alla, F.; Denis, I.; Kirche, A.; Tarquinio, C.; Brennstuhl, M. Posttraumatic Stress Disorder Following Myocardial Infarction: A Systematic Review. J. Trauma. Stress 2021, 34, 190–199. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Edmondson, D.; Rieckmann, N.; Shaffer, J.A.; Schwartz, J.E.; Burg, M.M.; Davidson, K.W.; Clemow, L.; Shimbo, D.; Kronisha, I.M. Posttraumatic stress due to an acute coronary syndrome increases risk of 42-month major adverse cardiac events and all-cause mortality. J. Psychiatr. Res. 2011, 45, 1621–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilchinsky, N.; Ginzburg, K.; Fait, K.; Foa, E.B. Cardiac-disease-induced PTSD (CDI-PTSD): A systematic review. Clin. Psychol. Rev. 2017, 55, 92–106. [Google Scholar] [CrossRef]
- Chung, M.C.; Dennis, I.; Berger, Z.; Jones, R.; Rudd, H. Posttraumatic stress disorder following myocardial infarction: Personality, coping, and trauma exposure characteristics. Int. J. Psychiatry Med. 2011, 42, 393–419. [Google Scholar] [CrossRef]
- Chung, M.C.; Berger, Z.; Rudd, H. Comorbidity and personality traits in patients with different levels of posttraumatic stress disorder following myocardial infarction. Psychiatry Res. 2007, 152, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.S.; Denollet, J. Validity of the Type D personality construct in Danish post-MI patients and healthy controls. J. Psychosom. Res. 2004, 57, 265–272. [Google Scholar] [CrossRef] [Green Version]
- Kupper, N.; Denollet, J. Type D Personality as a Risk Factor in Coronary Heart Disease: A Review of Current Evidence. Curr. Cardiol. Rep. 2018, 20, 104. [Google Scholar] [CrossRef] [Green Version]
- Grande, G.; Romppel, M.; Barth, J. Association Between Type D Personality and Prognosis in Patients with Cardiovascular Diseases: A Systematic Review and Meta-analysis. Ann. Behav. Med. 2012, 43, 299–310. [Google Scholar] [CrossRef]
- Edwards, E.R.; Shivaji, S.; Micek, A.; Wupperman, P. Distinguishing alexithymia and emotion differentiation conceptualizations through linguistic analysis. Pers. Individ. Differ. 2020, 157, 109801. [Google Scholar] [CrossRef]
- Larsen, J.K.; Brand, N.; Bermond, B.; Hijman, R. Cognitive and emotional characteristics of alexithymia: A review of neurobiological studies. J. Psychosom. Res. 2003, 54, 533–541. [Google Scholar] [CrossRef]
- Frewen, P.A.; Dozois, D.J.A.; Neufeld, R.W.J.; Lanius, R.A. Meta-analysis of alexithymia in posttraumatic stress disorder. J. Trauma. Stress 2008, 21, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.; Zhao, J.; Li, Y.; Cao, F.-L. Post-traumatic stress disorder symptoms in first-time myocardial infarction patients: Roles of attachment and alexithymia. J. Adv. Nurs. 2015, 71, 2575–2584. [Google Scholar] [CrossRef]
- Schnyder, U.; Schmid, J.-P.; Znoj, H.J.; Wittmann, L.; Von Känel, R.; Barth, J.; Meister, R.E.; Princip, M. Association of Trait Resilience With Peritraumatic and Posttraumatic Stress in Patients With Myocardial Infarction. Psychosom. Med. 2016, 78, 327–334. [Google Scholar] [CrossRef]
- Southwick, S.M.; Bonanno, G.A.; Masten, A.S.; Panter-Brick, C.; Yehuda, R. Resilience definitions, theory, and challenges: Interdisciplinary perspectives. Eur. J. Psychotraumatol. 2014, 5, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agaibi, C.E.; Wilson, J.P. Trauma, PTSD, and resilience: A review of the literature. Trauma Violence Abus. 2005, 6, 195–216. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Keckeisen, M.E.; Nyamathi, A.M. Coping and adjustment to illness in the acute myocardial infarction patient. J. Cardiovasc. Nurs. 1990, 5, 25–33. [Google Scholar] [CrossRef]
- Gil, S. Coping style in predicting posttraumatic stress disorder among Israeli students. Anxiety, Stress Coping 2005, 18, 351–359. [Google Scholar] [CrossRef]
- von Känel, R.; Barth, J.; Princip, M.; Meister-Langraf, R.E.; Schmid, J.-P.; Znoj, H.; Herbert, C.; Schnyder, U. Early Psychological Counseling for the Prevention of Posttraumatic Stress Induced by Acute Coronary Syndrome: The MI-SPRINT Randomized Controlled Trial. Psychother. Psychosom. 2018, 87, 75–84. [Google Scholar] [CrossRef] [Green Version]
- Denollet, J. DS14: Standard Assessment of Negative Affectivity, Social Inhibition, and Type D Personality. Psychosom. Med. 2005, 67, 89–97. [Google Scholar] [CrossRef]
- Grande, G.; Jordan, J.; Kümmel, M.; Struwe, C.; Schubmann, R.; Schulze, F.; Unterberg, C.; von Känel, R.; Kudielka, B.M.; Fischer, J.; et al. Evaluation der deutschen Typ-D-Skala (DS14) und Prävalenz der Typ-D-Persönlichkeit bei kardiologischen und psychosomatischen Patienten sowie Gesunden [Evaluation of the German Type D Scale (DS14) and prevalence of the Type D personality pattern in cardiological and psychosomatic patients and healthy subjects]. Psychother. Psychosom. Med. Psychol. 2004, 54, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Emons, W.H.; Meijer, R.R.; Denollet, J. Negative affectivity and social inhibition in cardiovascular disease: Evaluating type-D personality and its assessment using item response theory. J. Psychosom. Res. 2007, 63, 27–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schafer, R.; Schneider, C.; Sitte, W.; Franz, M. Evidence of validity of the German version of the TAS-20. Contribution to the 52nd conference of the German board of psychosomatic medicine in bad honnef. Psychother. Psychosomaitk Med. Psychol. 2002, 52, 449–453. [Google Scholar]
- Bach, M.; Bach, D.; De Zwaan, M.; Serim, M.; Böhmer, F. [Validation of the German version of the 20-item Toronto Alexithymia Scale in normal persons and psychiatric patients]. PPmP—Psychother. Psychosom. Med. Psychol. 1996, 46, 23–28. [Google Scholar]
- Leppert, K.; Dye, L.; Strauß, B. RS—Resilienzskala. In Psychodiagnostische Verfahren in der Psychotherapie; Brähler, E., Schumacher, J., Strauß, B., Eds.; Hogrefe: Göttingen, Germany, 2002; pp. S295–S298. [Google Scholar]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- Schnyder, U.; Moergeli, H. German version of clinician-administered PTSD scale. J. Trauma. Stress 2002, 15, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Kälin, W. Deutsche 24-Item Kurzform des “Coping Inventory for Stressful Situations (CISS)”; von N.S. Endler & J.D.A. Parker basierend auf der Übersetzung von N. Semmer, F. Tschan & V. Schade Institut für Psychologie; Universität Bern: Bern, Switzerland, 1995; unveröffentlichter Fragebogen. [Google Scholar]
- Aguayo-Carreras, P.; Ruiz-Carrascosa, J.C.; Ruiz-Villaverde, R.; Molina-Leyva, A. Four years stability of type D personality in patients with moderate to severe psoriasis and its implications for psychological impairment. An. Bras. Dermatol. 2021, 96, 558–564. [Google Scholar] [CrossRef]
- de Bruin, P.M.; de Haan, H.A.; Kok, T. The prediction of alexithymia as a state or trait characteristic in patients with substance use disorders and PTSD. Psychiatry Res. 2019, 282, 112634. [Google Scholar] [CrossRef]
- Hemming, L.; Haddock, G.; Shaw, J.; Pratt, D. Alexithymia and Its Associations With Depression, Suicidality, and Aggression: An Overview of the Literature. Front. Psychiatry 2019, 10, 203. [Google Scholar] [CrossRef] [Green Version]
- Park, C.; Won, M.H.; Son, Y. Mediating effects of social support between Type D personality and self-care behaviours among heart failure patients. J. Adv. Nurs. 2021, 77, 1315–1324. [Google Scholar] [CrossRef]
- Barth, J.; Schneider, S.; von Känel, R. Lack of Social Support in the Etiology and the Prognosis of Coronary Heart Disease: A Systematic Review and Meta-Analysis. Psychosom. Med. 2010, 72, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Kupper, N.; Pedersen, S.; Höfer, S.; Saner, H.; Oldridge, N.; Denollet, J. Cross-cultural analysis of Type D (distressed) personality in 6222 patients with ischemic heart disease: A study from the International HeartQoL Project. Int. J. Cardiol. 2013, 166, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Taylor, G.J.; Bagby, R.M. The alexithymia personality dimension. In Oxford Library of Psychology. The Oxford Handbook of Personality Disorders; Widiger, T.A., Ed.; Oxford University Press: Oxford, UK, 2012; pp. 648–673. [Google Scholar]
- Ogłodek, E.A. Alexithymia and Emotional Deficits Related to Posttraumatic Stress Disorder: An Investigation of Content and Process Disturbances. Case Rep. Psychiatry 2022, 2022, 7760988. [Google Scholar] [CrossRef] [PubMed]
- Rutter, M. Resilience in the face of adversity. Protective factors and resistance to psychiatric disorder. Br. J. Psychiatry 1985, 147, 598–611. [Google Scholar]
- Stewart, D.E.; Yuen, T. A Systematic Review of Resilience in the Physically Ill. J. Psychosom. Res. 2011, 52, 199–209. [Google Scholar] [CrossRef]
- Marke, V.; Bennett, P. Predicting post-traumatic stress disorder following first onset acute coronary syndrome: Testing a theoretical model. Br. J. Clin. Psychol. 2013, 52, 70–81. [Google Scholar] [CrossRef]
- Nowakowski, K.; Wróbel, K. Psychopathic traits, psychological resilience and coping with stress in socially maladjusted youth. Psychiatr. Polska 2021, 55, 1157–1167. [Google Scholar] [CrossRef]
- Lee, S.; Kim, S.; Choi, J.Y. Coping and Resilience of Adolescents With Congenital Heart Disease. J. Cardiovasc. Nurs. 2014, 29, 340–346. [Google Scholar] [CrossRef]
- Roberts, N.P.; Kenardy, J.; Kitchiner, N.J.; Bisson, J.I. Systematic Review and Meta-Analysis of Multiple-Session Early Interventions Following Traumatic Events. Am. J. Psychiatry 2009, 166, 293–301. [Google Scholar] [CrossRef] [Green Version]
- Ginzburg, K.; Solomon, Z.; Bleich, A. Repressive Coping Style, Acute Stress Disorder, and Posttraumatic Stress Disorder After Myocardial Infarction. Psychosom. Med. 2002, 64, 748–757. [Google Scholar] [CrossRef]
- Alonzo, A.A.; Reynolds, N.R. The structure of emotions during acute myocardial infarction: A model of coping. Soc. Sci. Med. 1998, 46, 1099–1110. [Google Scholar] [CrossRef]
- Windgassen, S.; Moss-Morris, R.; Goldsmith, K.; Chalder, T. The importance of cluster analysis for enhancing clinical practice: An example from irritable bowel syndrome. J. Ment. Health 2018, 27, 94–96. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Mean (SD) or Percentages (N) | Observed Range | |
|---|---|---|
| Gender, male % | 84.4 (130) | |
| Age | 58.96 (9.99) | 33–84 |
| Type D personality, % | 16.2 (25) | |
| Alexithymia | 41.26 (10.45) | 21–68 |
| Resilience | 61.23 (11.11) | 20–77 |
| Emotion-oriented coping | 19.33 (5.86) | 8–35 |
| Task-oriented coping | 29.86 (5.62) | 8–40 |
| Avoidant coping | 22.36 (6.96) | 8–40 |
| Post-traumatic Stress Symptoms at 3-month follow-up | 10.64 (10.52) | 0–54 |
| Reexperiencing symptoms at 3-month follow-up | 2.73 (4.12) | 0–21 |
| Avoidance symptoms at 3-month follow-up | 2.94 (4.34) | 0–25 |
| Hyperarousal symptoms at 3-month follow-up | 4.94 (4.38) | 0–19 |
| Post-traumatic Stress Symptoms at 12-month follow-up | 9.50 (8.74) | 0–52 |
| Reexperiencing symptoms at 12-month follow-up | 2.07 (3.14) | 0–18 |
| Avoidance symptoms at 12-month follow-up | 2.96 (4.11) | 0–18 |
| Hyperarousal symptoms at 12-month follow-up | 4.38 (3.78) | 0–16 |
| Personality Cluster | N | Type D Personality | Alexithymia Mean (SD) | Resilience Mean (SD) |
|---|---|---|---|---|
| 1 | 61 | no | 33.50 (6.39) | 70.00 (4.41) |
| 2 | 60 | no | 43.96 (7.44) | 56.73 (9.92) |
| 3 | 25 | yes | 53.73 (9.43) | 49.61 (9.91) |
| Total | 146 | - | 41.26 (10.45) | 61.05 (11.33) |
| Mean differences (F values) | - | 72.88 (p < 0.001) | 71.05 (p < 0.001) | |
| Effect size | - | 0.71 | 0.70 | |
| Post hoc analysis | 3 > all All > 3 | 1 > all All > 3 |
| N | Mean (SD) | Lower than | Higher than | |
|---|---|---|---|---|
| Emotion-Oriented Coping | ||||
| 1. Low-Risk | 61 | 15.81 (5.12) | 2 *** 3 *** | |
| 2. Medium-Risk | 60 | 20.02 (4.67) | 3 *** | 1 *** |
| 3. High-Risk | 25 | 26.32 (3.65) | 1 *** 2 *** | |
| Task-Oriented Coping | ||||
| 1. Low-Risk | 61 | 32.31 (5.70) | 2 *** 3 *** | |
| 2. Medium-Risk | 60 | 28.24 (5.07) | 1 *** | |
| 3. High-Risk | 25 | 27.38 (5.74) | 1 *** | |
| Avoidant Coping | ||||
| 1. Low-Risk | 61 | 24.02 (8.19) | 2 * | |
| 2. Medium-Risk | 60 | 20.95 (5.85) | 1 * | |
| 3. High-Risk | 25 | 21.06 (5.79) | ||
| Post-traumatic Stress Symptoms at 3-month follow-up | ||||
| 1. Low-Risk | 61 | 6.90 (6.86) | 2 * 3 *** | |
| 2. Medium-Risk | 60 | 11.57 (10.81) | 3 ** | 1 * |
| 3. High-Risk | 25 | 19.20 (13.07) | 1 *** 2 * | |
| Re-experiencing at 3-month follow-up | ||||
| 1. Low-Risk | 61 | 1.80 (2.98) | 3 ** | |
| 2. Medium-Risk | 60 | 2.97 (4.64) | ||
| 3. High-Risk | 25 | 5.12 (4.82) | 1 ** | |
| Avoidance at 3-month follow-up | ||||
| 1. Low-Risk | 61 | 1.52 (2.95) | 3 *** | |
| 2. Medium-Risk | 60 | 3.18 (3.97) | ||
| 3. High-Risk | 25 | 6.44 (1.29) | 1 *** | |
| Hyperarousal at 3-month follow-up | ||||
| 1. Low-Risk | 61 | 3.54 (2.96) | 2 * 3 *** | |
| 2. Medium-Risk | 60 | 5.42 (4.62) | 3 * | 1 * |
| 3. High-Risk | 25 | 7.88 (5.39) | 1 *** 2 * | |
| Post-traumatic Stress Symptoms at 12-month follow-up | ||||
| 1. Low-Risk | 43 | 6.79 (7.30) | 2 (p = 0.06) 3 * | |
| 2. Medium-Risk | 39 | 11.15 (10.08) | 1 (p = 0.06) | |
| 3. High-Risk | 18 | 12.83 (6.93) | 1* | |
| Re-experiencing at 12-month follow-up | ||||
| 1. Low-Risk | 43 | 1.49 (2.58) | ||
| 2. Medium-Risk | 39 | 2.54 (3.69) | ||
| 3. High-Risk | 18 | 2.67 (3.16) | ||
| Avoidance at 12-month follow-up | ||||
| 1. Low-Risk | 43 | 2.23 (3.46) | ||
| 2. Medium-Risk | 39 | 4.00 (4.88) | ||
| 3. High-Risk | 18 | 2.44 (3.35) | ||
| Hyperarousal at 12-month follow-up | ||||
| 1. Low-Risk | 43 | 3.07 (2.81) | 3 *** | |
| 2. Medium-Risk | 39 | 4.62 (4.10) | 3 * | |
| 3. High-Risk | 18 | 7.17 (3.71) | 1 *** 2 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Princip, M.; von Känel, R.; Zuccarella-Hackl, C.; Meister-Langraf, R.E.; Znoj, H.; Schmid, J.-P.; Barth, J.; Schnyder, U.; Jimenez-Gonzalo, L.; Ledermann, K. The Influence of Personality Traits on Specific Coping Styles and the Development of Posttraumatic Stress Symptoms following Acute Coronary Syndrome: A Cluster Analytic Approach. Psych 2022, 4, 774-787. https://doi.org/10.3390/psych4040057
Princip M, von Känel R, Zuccarella-Hackl C, Meister-Langraf RE, Znoj H, Schmid J-P, Barth J, Schnyder U, Jimenez-Gonzalo L, Ledermann K. The Influence of Personality Traits on Specific Coping Styles and the Development of Posttraumatic Stress Symptoms following Acute Coronary Syndrome: A Cluster Analytic Approach. Psych. 2022; 4(4):774-787. https://doi.org/10.3390/psych4040057
Chicago/Turabian StylePrincip, Mary, Roland von Känel, Claudia Zuccarella-Hackl, Rebecca E. Meister-Langraf, Hansjörg Znoj, Jean-Paul Schmid, Jürgen Barth, Ulrich Schnyder, Lucia Jimenez-Gonzalo, and Katharina Ledermann. 2022. "The Influence of Personality Traits on Specific Coping Styles and the Development of Posttraumatic Stress Symptoms following Acute Coronary Syndrome: A Cluster Analytic Approach" Psych 4, no. 4: 774-787. https://doi.org/10.3390/psych4040057