
Risk Factors and Changes in Depression and Anxiety over Time in New Zealand during COVID-19: A Longitudinal Cohort Study
 , , , ,
, , , ,
Abstract
:Highlights
- The COVID-19 pandemic has caused substantial disruption to daily life.
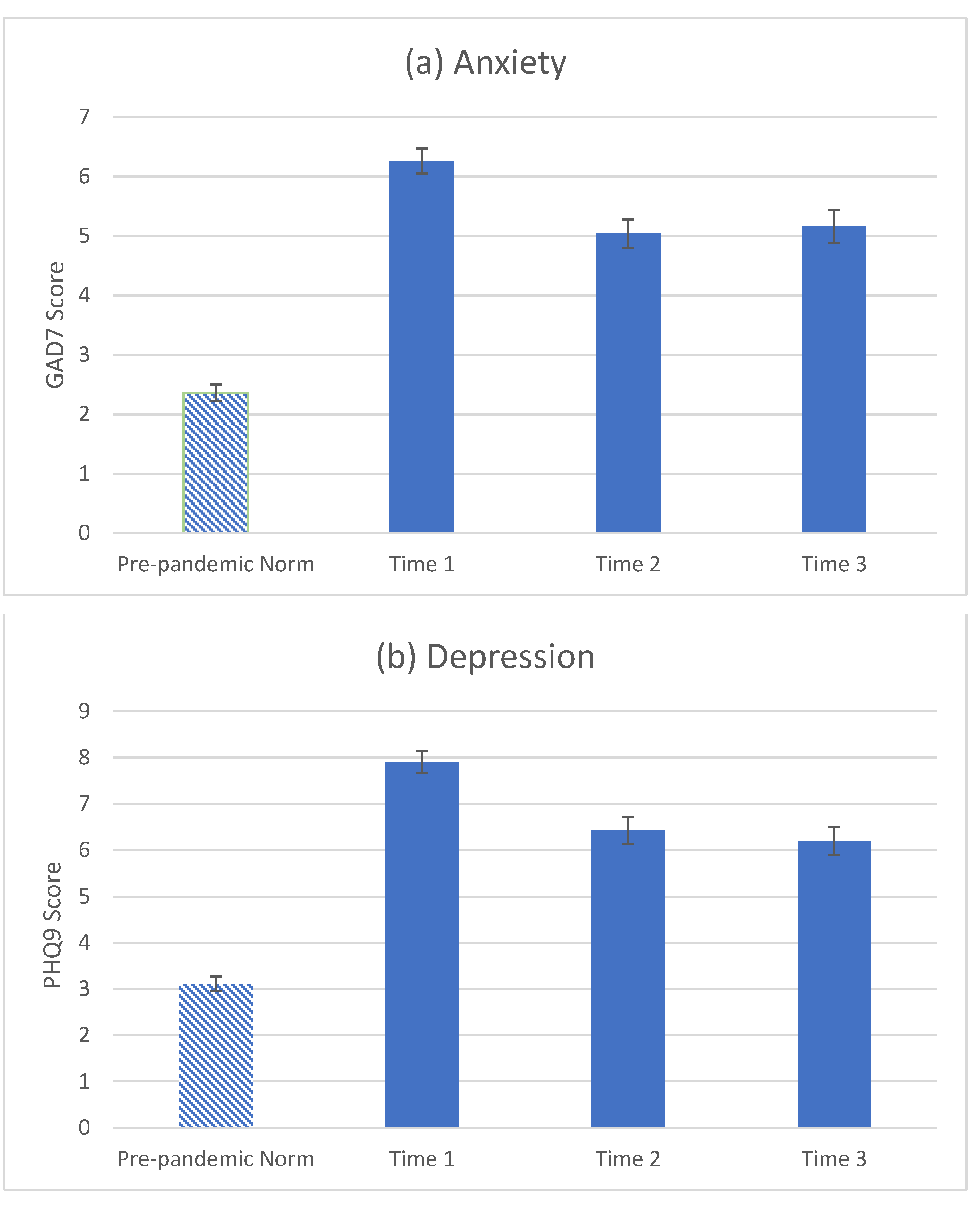
- The pandemic increased anxiety and depression in the general population of New Zealand in its first 3 months.
- This study found that depression and anxiety reduced over the first year of the pandemic in New Zealanders.
- However, even in a country with low transmission, anxiety and depression remained elevated compared to pre-pandemic norms.
- Younger age, being a pet owner, negative life events, and having mental health disorder increased the risk of anxiety and depression.
Abstract
1. Introduction
2. Aims of the Current Research
3. Methods
3.1. Participant Recruitment and Eligibility
3.2. Procedures and Measures
3.3. Statistical Analysis
4. Results
4.1. Sample Characteristics
4.2. Depression and Anxiety over Time
4.3. Risk Factors for Depression and Anxiety
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Daly, M.; Sutin, A.R.; Robinson, E. Longitudinal changes in mental health and the COVID-19 pandemic: Evidence from the UK Household Longitudinal Study. Psychol. Med. 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ettman, C.K.; Abdalla, S.M.; Cohen, G.H.; Sampson, L.; Vivier, P.M.; Galea, S. Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Netw. Open 2020, 3, e2019686. [Google Scholar] [CrossRef] [PubMed]
- Hyland, P.; Shevlin, M.; McBride, O.; Murphy, J.; Karatzias, T.; Bentall, R.P.; Martinez, A.; Vallières, F. Anxiety and depression in the Republic of Ireland during the COVID-19 pandemic. Acta Psychiatr. Scand. 2020, 142, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Płomecka, M.B.; Gobbi, S.; Neckels, R.; Radziński, P.; Skórko, B.; Lazzeri, S.; Jawaid, A.; Qureshi, S.U.; Haq, Z.; Barańczuk-Turska, Z.; et al. Mental health impact of COVID-19: A global study of risk and resilience factors. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Varma, P.; Junge, M.; Meaklim, H.; Jackson, M.L. Younger people are more vulnerable to stress, anxiety and depression during COVID-19 pandemic: A global cross-sectional survey. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 109, 110236. [Google Scholar] [CrossRef] [PubMed]
- Bueno-Notivol, J.; Gracia-García, P.; Olaya, B.; Lasheras, I.; López-Antón, R.; Santabárbara, J. Prevalence of depression during the COVID-19 outbreak: A meta-analysis of community-based studies. Int. J. Clin. Health Psychol. 2021, 21, 100196. [Google Scholar] [CrossRef] [PubMed]
- Santabárbara, J.; Lasheras, I.; Lipnicki, D.M.; Bueno-Notivol, J.; Pérez-Moreno, M.; López-Antón, R.; De la Cámara, C.; Lobo, A.; Gracia-García, P. Prevalence of anxiety in the COVID-19 pandemic: An updated meta-analysis of community-based studies. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 109, 110207. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Every-Palmer, S.; Jenkins, M.; Gendall, P.; Hoek, J.; Beaglehole, B.; Bell, C.; Williman, J.; Rapsey, C.; Stanley, J. Psychological distress, anxiety, family violence, suicidality, and wellbeing in New Zealand during the COVID-19 lockdown: A cross-sectional study. PLoS ONE 2020, 15, e0241658. [Google Scholar] [CrossRef]
- Gasteiger, N.; Vedhara, K.; Massey, A.; Jia, R.; Ayling, K.; Chalder, T.; Coupland, C.; Broadbent, E. Depression, anxiety and stress during the COVID-19 pandemic: Results from a New Zealand cohort study on mental well-being. BMJ Open 2021, 11, e045325. [Google Scholar] [CrossRef]
- Jia, R.; Ayling, K.; Chalder, T.; Massey, A.; Broadbent, E.; Coupland, C.; Vedhara, K. Mental health in the UK during the COVID-19 pandemic: Cross-sectional analyses from a community cohort study. BMJ Open 2020, 10, e040620. [Google Scholar] [CrossRef] [PubMed]
- Dawel, A.; Shou, Y.; Smithson, M.; Cherbuin, N.; Banfield, M.; Calear, A.L.; Farrer, L.M.; Gray, D.; Gulliver, A.; Housen, T.; et al. The effect of COVID-19 on mental health and wellbeing in a representative sample of Australian adults. Front. Psychiatry 2020, 11, 579985. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhao, J.; Ma, Z.; McReynolds, L.S.; Lin, D.; Chen, Z.; Wang, T.; Wang, D.; Zhang, Y.; Zhang, J.; et al. Mental health among college students during the COVID-19 pandemic in China: A 2-wave longitudinal survey. J. Affect. Disord. 2021, 281, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Jia, R.; Ayling, K.; Chalder, T.; Massey, A.; Gasteiger, N.; Broadbent, E.; Vedhara, K.; Coupland, C. The prevalence, incidence, prognosis and risk factors for depression and anxiety in a UK cohort during the COVID-19 pandemic. medRxiv 2021, preprint. [Google Scholar] [CrossRef]
- New Zealand Government. History of the COVID-19 Alert System. Available online: https://covid19.govt.nz/alert-levels-and-updates/history-of-the-COVID-19-alert-system/ (accessed on 15 September 2022).
- Bell, C.; Williman, J.; Beaglehole, B.; Stanley, J.; Jenkins, M.; Gendall, P.; Rapsey, C.; Every-Palmer, S. Psychological distress, loneliness, alcohol use and suicidality in New Zealanders with mental illness during a strict COVID-19 lockdown. Aust. N. Z. J. Psychiatry 2021, 56, 800–810. [Google Scholar] [CrossRef]
- Palgi, Y.; Shrira, A.; Ring, L.; Bodner, E.; Avidor, S.; Bergman, Y.; Cohen-Fridel, S.; Keisari, S.; Hoffman, Y. The loneliness pandemic: Loneliness and other concomitants of depression, anxiety and their comorbidity during the COVID-19 outbreak. J. Affect. Disord. 2020, 275, 109. [Google Scholar] [CrossRef]
- Tang, F.; Liang, J.; Zhang, H.; Kelifa, M.M.; He, Q.; Wang, P. COVID-19 related depression and anxiety among quarantined respondents. Psychol. Health 2021, 36, 164–178. [Google Scholar] [CrossRef]
- Ratschen, E.; Shoesmith, E.; Shahab, L.; Silva, K.; Kale, D.; Toner, P.; Reeve, C.; Mills, D.S. Human-animal relationships and interactions during the COVID-19 lockdown phase in the UK: Investigating links with mental health and loneliness. PLoS ONE 2020, 15, e0239397. [Google Scholar] [CrossRef]
- Te Hiringa Hauora/Health Promotion Agency. Results from the 2018 New Zealand Mental Health Monitor; Te Hiringa Hauora/Health Promotion Agency Insights and Evaluation Unit: Wellington, New Zealand, 2022. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Löwe, B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Wirtz, D.; Tov, W.; Kim-Prieto, C.; Choi, D.-w.; Oishi, S.; Biswas-Diener, R. New well-being measures: Short scales to assess flourishing and positive and negative feelings. Soc. Indic. Res. 2010, 97, 143–156. [Google Scholar] [CrossRef]
- Robinson, E.; Sutin, A.R.; Daly, M.; Jones, A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic. J. Affect. Disord. 2022, 296, 567–576. [Google Scholar] [CrossRef]
- Cohen, S. Psychosocial vulnerabilities to upper respiratory infectious illness: Implications for susceptibility to coronavirus disease 2019 (COVID-19). Perspect. Psychol. Sci. 2021, 16, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Madison, A.A.; Shrout, M.R.; Renna, M.E.; Kiecolt-Glaser, J.K. Psychological and behavioral predictors of vaccine efficacy: Considerations for COVID-19. Perspect. Psychol. Sci. 2021, 16, 191–203. [Google Scholar] [CrossRef] [PubMed]
- Duan, L.; Zhu, G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef]
- Hatch, S.L.; Dohrenwend, B.P. Distribution of traumatic and other stressful life events by race/ethnicity, gender, SES and age: A review of the research. Am. J. Community Psychol. 2007, 40, 313–332. [Google Scholar] [CrossRef]
- Esam, F.; Forrest, R.; Waran, N. Locking down the impact of New Zealand’s COVID-19 alert level changes on pets. Animals 2021, 11, 758. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristic | Completers | Non-Completers | p-Value |
|---|---|---|---|
| Gender, n (%) | 0.017 b,* | ||
| Male | 17 (7%) | 55 (12%) | |
| Female | 243 (93%) | 398 (88%) | |
| Age (years), M (SD) | 43.87 (16.62) | 40.26 (15.70) | 0.004 a,* |
| Ethnicity, n (%) | 0.075 b | ||
| White-NZ European, European | 224 (86%) | 369 (81%) | |
| BAME background | 37 (14%) | 89 (19%) | |
| Relationship status, n (%) | 0.073 b | ||
| Single, never married | 49 (19%) | 120 (26%) | |
| Single, divorced or widowed | 27 (10%) | 41 (9%) | |
| In a relationship/married, but living apart | 20 (8%) | 28 (6%) | |
| In a relationship/married, and cohabiting | 165 (63%) | 264 (58%) | |
| Education level, n (%) | <0.001 b,** | ||
| NCEA or lower (high school) | 52 (20%) | 101 (22%) | |
| Level 5 and 6 diploma or other | 28 (11%) | 41 (9%) | |
| Bachelor’s degree | 38 (15%) | 136 (30%) | |
| Postgraduate degree | 143 (55%) | 180 (39%) | |
| Keyworker status, n (%) | 0.705 b | ||
| Keyworker | 117 (45%) | 212 (46%) | |
| Not a keyworker | 144 (55%) | 246 (54%) | |
| Living alone, n (%) | 0.641 b | ||
| Living alone | 26 (10%) | 49 (11%) | |
| Living with others | 235 (90%) | 393 (89%) | |
| COVID-19 risk group, n (%) | 0.985 b | ||
| Most at risk | 21 (8%) | 36 (8%) | |
| At increased risk | 34 (13%) | 58 (13%) | |
| Not at risk | 206 (79%) | 364 (79%) | |
| Perceived risk of COVID-19, M (SD) | 2.42 (1.74) | 2.22 (1.52) | 0.170 a |
| PHQ-9, M (SD) | 7.92 (6.65) | 7.89 (.17) | 0.950 a |
| GAD-7, M (SD) | 6.27 (5.54) | 6.26 (5.30) | 0.975 a |
| SPANE-P, M (SD) | 19.90 (5.21) | 20.01 (4.91) | 0.790 a |
| Perceived loneliness, M (SD) | 3.91 (2.70) | 3.91 (2.85) | 0.991 a |
| COVID-19 worry, n (%) | 0.937 b | ||
| No worry | 94 (36%) | 163 (39%) | |
| Occasional worry | 144 (55%) | 227 (54%) | |
| Much worry | 18 (7%) | 27 (6%) | |
| Most worry | 4 (2%) | 6 (1%) | |
| Pet ownership, n (%) | 0.432 b | ||
| Pet owner | 153 (59%) | 244 (56%) | |
| Non-pet owner | 108 (41%) | 195 (44%) | |
| Smoking status, n (%) | 0.843 b | ||
| Smoker | 14 (5%) | 25 (6%) | |
| Non-smoker | 247 (95%) | 412 (94%) | |
| Exercise frequency, n (%) | 0.125 b | ||
| Almost every day | 129 (49%) | 172 (39%) | |
| 2–3 times a week | 70 (27%) | 148 (34%) | |
| Once a week | 25 (10%) | 49 (11%) | |
| Less than once a week | 24 (9%) | 46 (10%) | |
| Never | 13 (5%) | 24 (5%) | |
| Alcohol consumption, n (%) | 0.047 b,* | ||
| Daily | 24 (9%) | 43 (10%) | |
| 4–6 times a week | 43 (16%) | 49 (11%) | |
| 1–3 times a week | 93 (37%) | 133 (30%) | |
| Less than once a week | 29 (11%) | 75 (17%) | |
| Never | 72 (28%) | 137 (31%) |
| PHQ-9 a | GAD-7 a | |||||||
|---|---|---|---|---|---|---|---|---|
| Predictor | B | 95% CI | Standardised Beta | p-Value | B | 95% CI | Standardised Beta | p-Value |
| Age (per year) | −0.01 | [−0.02, −0.00] | −0.17 | 0.023 * | −0.02 | [−0.03, −0.01] | −0.27 | <0.001 ** |
| Female (yes/no) | 0.20 | [−0.35, 0.74] | 0.04 | 0.476 | 0.27 | [−0.31, 0.84] | 0.06 | 0.359 |
| BAME background (yes/no) | −0.22 | [−0.66, 0.21] | −0.06 | 0.316 | −0.11 | [−0.57, 0.35] | −0.03 | 0.632 |
| Keyworker (yes/no) | 0.10 | [−0.19, 0.40] | 0.04 | 0.498 | −0.01 | [−0.32, 0.30] | −0.01 | 0.953 |
| Prior mental health disorder (yes/no) | 0.53 | [0.23, 0.84] | 0.22 | <0.001 ** | 0.56 | [0.24, 0.89] | 0.23 | <0.001 ** |
| Living alone (yes/no) | −0.04 | [−0.48, 0.41] | −0.01 | 0.875 | 0.14 | [−0.33, 0.61] | 0.04 | 0.550 |
| COVID-19 risk groupb | ||||||||
| Most at risk | 0.26 | [−0.24, 0.75] | 0.06 | 0.308 | 0.11 | [−0.41, 0.64] | 0.03 | 0.668 |
| Increased risk | 0.02 | [−0.43, 0.46] | 0.05 | 0.943 | 0.25 | [−0.22, 0.73] | 0.07 | 0.288 |
| Positive life events (per unit) | −0.19 | [−0.46, 0.07] | −0.09 | 0.146 | −0.23 | [−0.51, 0.05] | −0.10 | 0.104 |
| Negative life events (per unit) | 0.31 | [0.13, 0.50] | 0.21 | <0.001 ** | 0.29 | [0.09, 0.48] | 0.19 | 0.004 * |
| Perceived loneliness (per unit) | 0.06 | [−0.01, 0.12] | 0.12 | 0.104 | 0.03 | [−0.04, 0.10] | 0.06 | 0.431 |
| SPANE-P (per unit) | −0.05 | [−0.09, −0.02] | −0.23 | 0.004 * | −0.05 | [−0.09, −0.02] | −0.23 | 0.005 * |
| Perceived risk of COVID-19 (per unit) | 0.03 | [−0.06, 0.12] | 0.04 | 0.502 | −0.01 | [−0.10, 0.08] | −0.01 | 0.836 |
| COVID-19 worryc | ||||||||
| No worry | 0.04 | [−0.26, 0.34] | 0.02 | 0.792 | −0.14 | [−0.46, 0.17] | −0.06 | 0.374 |
| Much worry | −0.33 | [−0.93, 0.27] | −0.07 | 0.279 | −0.15 | [−0.78, 0.49] | −0.03 | 0.649 |
| Most worry | 0.33 | [−0.71, 1.37] | 0.04 | 0.527 | 0.36 | [−0.74, 1.46] | 0.04 | 0.520 |
| Pet ownership (yes/no) | 0.43 | [0.15, 0.71] | 0.18 | 0.003 * | 0.39 | [0.10, 0.69] | 0.16 | 0.009 * |
| Smoker (yes/no) | −0.02 | [−0.66, 0.62] | −0.01 | 0.947 | 0.31 | [−0.37, 0.99] | 0.06 | 0.365 |
| Exercise frequencyd | ||||||||
| Almost every day | −0.29 | [−1.01, 0.43] | −0.12 | 0.430 | 0.30 | [−0.47, 1.06] | 0.12 | 0.447 |
| 2–3 times a week | −0.14 | [−0.87, 0.59] | −0.05 | 0.711 | 0.24 | [−0.54, 1.01] | 0.09 | 0.545 |
| Once a week | −0.39 | [−1.22, 0.44] | −0.09 | 0.354 | 0.16 | [−0.72, 1.04] | 0.04 | 0.715 |
| Less than once a week | −0.12 | [−0.91, 0.67] | −0.03 | 0.766 | 0.17 | [−0.67, 1.01] | 0.04 | 0.692 |
| Alcohol consumptione | ||||||||
| Daily | −0.21 | [−0.78, 0.36] | −0.05 | 0.468 | −0.16 | [−0.76, 0.45] | −0.03 | 0.614 |
| 4–6 times a week | −0.19 | [−0.63, 0.24] | −0.06 | 0.387 | 0.06 | [−0.40, 0.52] | 0.02 | 0.803 |
| 1–3 times a week | −0.18 | [−0.53, 0.17] | −0.07 | 0.325 | −0.14 | [−0.51, 0.23] | −0.06 | 0.451 |
| Less than once a week | −0.03 | [−0.52, 0.45] | −0.01 | 0.900 | −0.24 | [−0.75, 0.28] | −0.06 | 0.366 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Law, M.; Gasteiger, N.; Vedhara, K.; Massey, A.; Jia, R.; Ayling, K.; Chalder, T.; Coupland, C.; Broadbent, E. Risk Factors and Changes in Depression and Anxiety over Time in New Zealand during COVID-19: A Longitudinal Cohort Study. Psych 2022, 4, 706-716. https://doi.org/10.3390/psych4040052
Law M, Gasteiger N, Vedhara K, Massey A, Jia R, Ayling K, Chalder T, Coupland C, Broadbent E. Risk Factors and Changes in Depression and Anxiety over Time in New Zealand during COVID-19: A Longitudinal Cohort Study. Psych. 2022; 4(4):706-716. https://doi.org/10.3390/psych4040052
Chicago/Turabian StyleLaw, Mikaela, Norina Gasteiger, Kavita Vedhara, Adam Massey, Ru Jia, Kieran Ayling, Trudie Chalder, Carol Coupland, and Elizabeth Broadbent. 2022. "Risk Factors and Changes in Depression and Anxiety over Time in New Zealand during COVID-19: A Longitudinal Cohort Study" Psych 4, no. 4: 706-716. https://doi.org/10.3390/psych4040052