
Examining the Experiences of US Dentists during the First Wave of the COVID-19 Pandemic: Implications for Policy and Practice



Abstract
:1. Introduction
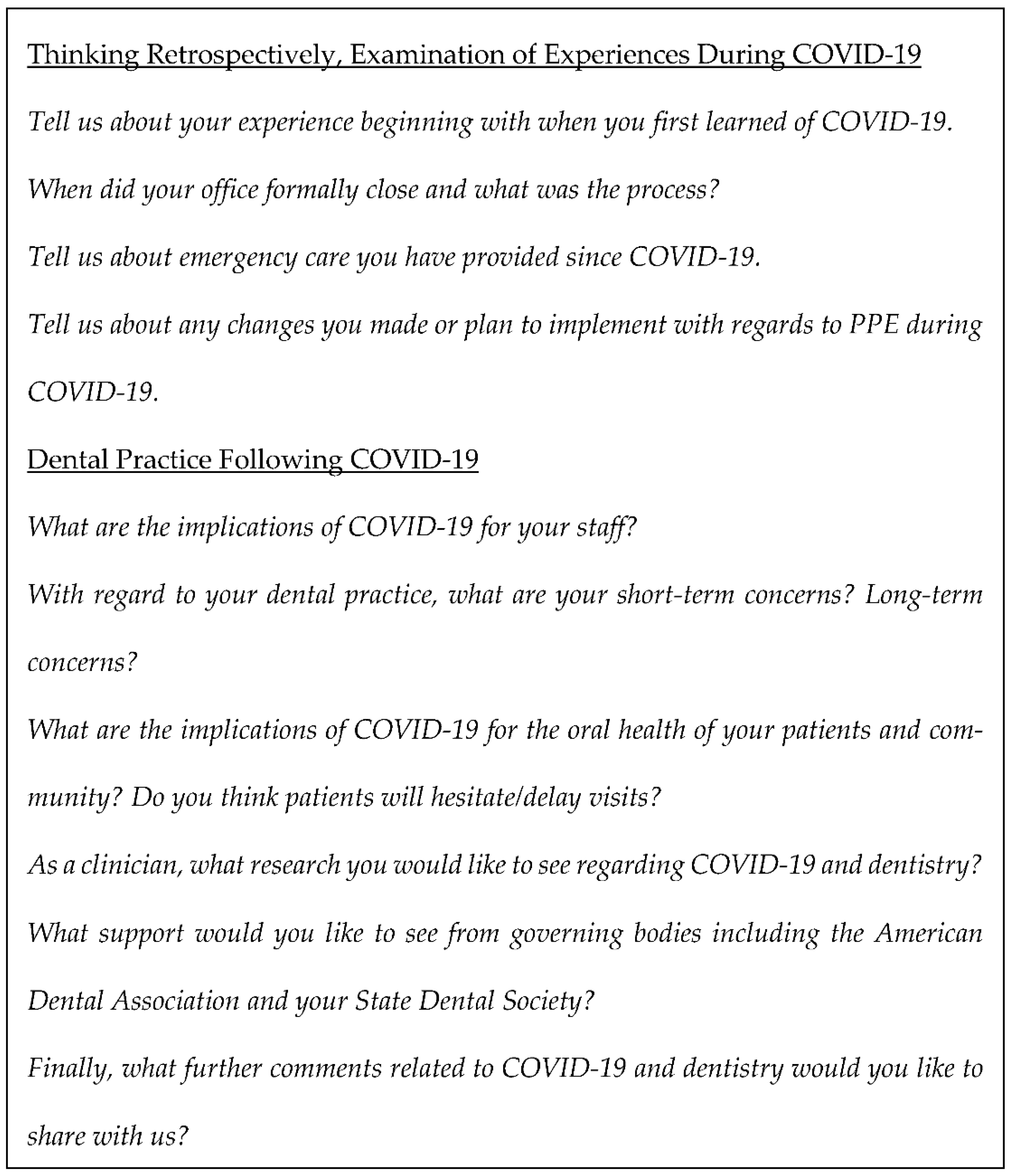
2. Materials and Methods
3. Results
3.1. Theme 1: Dentistry during COVID-19: Experiences to during the First Wave
3.1.1. Office Closures
3.1.2. Emergency Care Provided
3.1.3. PPE
3.1.4. Impact of COVID-19 on Staff
“They are very…concerned that we have adequate PPE, making sure we can implement social distancing and…change the flow of our days when we get back.”
3.1.5. Short-Term Concerns
3.2. Theme 2: Long-Term Concerns Regarding COVID-19
3.2.1. COVID-19’s Impact on Oral Health Disparities
3.2.2. Practice Viability and Financial Concerns
“Long-term concerns for me is just dentistry in general. Is it going to be the same as what it was, what we planned for when we…went into the dental field? With a lot of people losing their jobs or being furloughed, [everyone’s] disposable income is dwindling or... nonexistent. When we do open up are people going to see dentistry as something that they need? We can open back up, but if nobody has the money or interested in getting work done, we’re still highly effected by the [aftermath] of [COVID-19]”.
“I’m not sure what that’s going to do as far as effecting my specialty and this practice that I’ve been investing in for the last six and a half years… the student debt load that we all carry…the financial plans that [we] have… That’s [my] biggest long-term concern”.
3.2.3. COVID-19 as a Precedent
“If [infectious disease outbreaks] become more of a regular issue...what [they may] do is force everyone to close their doors. That’s my long-term concern. What kind of precedent [does COVID-19] set moving forward? What is deemed a [nationwide] emergency? It sets a precedent business-wise in the future [that dental offices could] close... you could possibly go out of business”.
3.3. Theme 3: COVID-19 Professional Communication and Dental Research
3.3.1. Governing Bodies Communication and Guidelines
3.3.2. Direction for Future Research
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 5 July 2022).
- ISDS Issues Recommendations for Dental Offices Regarding COVID-19. Illinois State Dental Society. Available online: https://www.isds.org/news-details/2020/03/16/isds-issues-recommendations-for-dental-offices-regarding-covid-19 (accessed on 8 April 2020).
- CDC Releases Interim Reopening Guidance for Dental Settings. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/oralhealth/infectioncontrol/statement-COVID.html (accessed on 31 July 2020).
- Checchi, V.; Montevecchi, M.; Checchi, L. Variation of Efficacy of Filtering Face Pieces Respirators over Time in a Dental Setting: A Pilot Study. Dent. J. 2021, 9, 36. [Google Scholar] [CrossRef] [PubMed]
- ADA Urges Dentists to Heed April 30 Interim Postponement Recommendation, Maintain Focus on Urgent and Emergency Dental Care Only. American Dental Association. Available online: https://www.ada.org/en/press-room/news-releases/2020-archives/april/summary-of-ada-guidance-during-the-covid-19-crisis?utm_source=adaorg&utm_medium=adahomerotator&utm_content=interim-statement&utm_campaign=covid-19 (accessed on 8 April 2020).
- Gorter, R.C.; Storm, M.K.; Te Brake, J.H.; Kersten, H.W.; Eijkman, M.A. Outcome of career expectancies and early professional burnout among newly qualified dentists. Int. Dent. J. 2007, 57, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. (Eds.) Sampling in Qualitative Research. In Nursing Research: Generating and Assessing Evidence for Nursing Practice, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2017. [Google Scholar]
- Consolo, U.; Bellini, P.; Bencivenni, D.; Iani, C.; Checchi, V. Epidemiological Aspects and Psychological Reactions to COVID-19 of Dental Practitioners in the Northern Italy Districts of Modena and Reggio Emilia. Int. J. Environ. Res. Public Health 2020, 17, 3459. [Google Scholar] [CrossRef] [PubMed]
- Bellini, P.; Checchi, V.; Iani, C.; Bencivenni, D.; Consolo, U. Psychological reactions to COVID-19 and epidemiological aspects of dental practitioners during lockdown in Italy. Minerva Dent. Oral Sci. 2021, 70, 32–43. [Google Scholar] [CrossRef]
- Abrar, E.; Abduljabbar, A.S.; Naseem, M.; Panhwar, M.; Vohra, F.; Abduljabbar, T. Evaluating the Influence of COVID-19 Among Dental Practitioners After Lockdown. Inquiry 2021, 58, 469580211060753. [Google Scholar] [CrossRef]
- Sotomayor-Castillo, C.; Li, C.; Kaufman-Francis, K.; Nahidi, S.; Walsh, L.J.; Liberali, S.A.; Irving, E.; Holden, A.C.; Shaban, R.Z. Australian dentists’ knowledge, preparedness, and experiences during the COVID-19 pandemic. Infect. Dis. Health 2022, 27, 49–57. [Google Scholar] [CrossRef]
- Salehiniya, H.; Hatamian, S.; Abbaszadeh, H. Mental health status of dentists during COVID-19 pandemic: A systematic review and meta-analysis. Health Sci. Rep. 2022, 5, e617. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.Z.; Gallo, G.N.; Babikow, E.; Wiesen, C.; Jackson, T.H.; Mitchell, K.; Jacox, L.A. Effects of the COVID-19 pandemic on dentists’ workforce confidence and workflow. J. Am. Dent. Assoc. 2022, 153, 610–624.e8. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Participant Characteristic | No. (%) | |
|---|---|---|
| Sex | ||
| Male | 8 (67%) | |
| Female | 4 (33%) | |
| Age | ||
| Mean | 32 | |
| Range | 7; 30–37 | |
| Years of Experience | ||
| Mean | 6 | |
| Range | 5, 5–10 | |
| Area of Practice | ||
| General Practitioner | 9 (75%) | |
| Specialist | 3 (25%) | |
| Position | ||
| Owner | 7 (58%) | |
| Associate | 5 (42%) | |
| Size of Practice | ||
| Mean number of Operatories | 7 | |
| Range | 10; 4–14 | |
| Office Closures | |
| “Well, it kind of felt like the rug was pulled out from underneath us to be honest, there was very little time to prepare. I remember I got the [closure] email...at 5:30 in the morning when I was getting ready for work. [We had to] get our first patients who were already on their way out the door home and then cancel everyone from there [forward].” | |
| “Every hygienist and assistant was on a phone calling patients, from either their operatories or a desk phone to get all the patients rescheduled or canceled at that time and [there was] uncertainty of how everyone was going to get paid. It was chaotic that first day, very chaotic, but they managed to go through the plan that each person was responsible for their own schedule and calling those patients to move them out to after April 8th, so that was chaotic.” | |
| “On Friday we talked about it and then implemented it over the weekend. So, it was... abrupt.” | |
| Emergency Care Provided | |
| “As a practice...we saw a number of patients the first two weeks via teledentistry. But then as [it] got pushed to a longer stay-at-home order, I have not felt comfortable letting patients go that long without being seen if they’re in pain. So I’ve been going in on an as-needed basis, that could mean [a few] patients a week, it could mean 12 patients a week and working with one assistant, the same assistant every time and triaging the needs there and providing whatever definitive care I can at that time.” | |
| “I have just done phone triage. I’ve had number of patients call. They express their symptoms [and I] talk it through with them. A couple have sent pictures, things like that…” | |
| “Lots of phone conversations, [I] have called in some antibiotics... gone in to see people for exam and X-rays. I have good endodontists in town who are seeing people who are swollen and are in severe pain. For extractions, our local oral surgeon is seeing [a]… few people, so I have done a few of those when necessary. But as far as temporary crowns [coming] off, I have urged people to get their own temporary cement, when possible, and if that has failed and they’re in pain, I have gone in.” | |
| “We’ve handled emergencies mainly over the phone. I have a front desk employee go into the office every day, checking any voicemail. With emergencies, we will see patients either in office or, depending on their emergency, refer them to a specialist for immediate care.” | |
| PPE | |
| “When we get going again, if we can get N95 masks we’re going to use [them] with disposable class one masks over those...We’ll change out the class one masks between patients, but we will use the N95 throughout the day just because there is a significant shortage, and they are a lot more costly. The assistants and the hygienists will [also] be using face shields, which they’re all for.” | |
| “We talked with our hygiene coordinator and [asked] what she thought. So, it wasn’t just a ‘This is how we’re doing it from now on.’ We wanted all levels of our staff to [be involved with PPE decision-making].” | |
| “If the new standard PPE are these hair nets, face shields, N95 super masks, gloved up. Are the patients going to be afraid and not trusting that it’s safe to go back? You know, if you’re looking like you’re coming out of a hazmat environment.” | |
| “We’ve obtained some N95 masks...we have not made any plans for a long-term change on PPE. I’m concerned about the adequacy of any PPE and cross-contamination in a dental office, whether it would be sufficient at this point or not. I can protect myself and my staff, but if there’s two patients in the office and we’re doing cleanings on [them], I’m not sure we can protect those patients from each other.” | |
| “It seems like we’re going to have to have a really good supply of level three surgical masks, face shields, [and] gowns available for people. Eye protection will be a must.” | |
| Impact of COVID-19 on Staff | |
| “It’s going to be hard to get [staff] over the fear of getting sick to get them back to work. Even though we’re doing all of these things PPE-wise, are they going to be able to get past that fear of getting sick and come back to work? I don’t know.” | |
| “They are very much concerned that we have the adequate PPE, making sure we can implement social distancing and how are we going to change the flow of our days when we get back...there’s a lot of potential for cross contamination with the dentist moving from room to room so frequently.” | |
| “The only ones concerned are the hygienists...because a lot of the research has them at the top of the list [to] be the first ones to get the virus. We’ll probably put in a protocol of no ultrasonic scalers, try to cut down on the aerosols, hopefully mostly hand-scaling, and go from there.” | |
| “My staff seems to be willing to go back when we are deemed essential and when our practice thinks it’s safe for us to go back.” | |
| “Everyone seems to be coping well. I think it’s a varying degree. Some very worried, others not so much, more concerned about when we’ll get back to work. Others worried about their safety and wellbeing [when we do get back to work].” | |
| Short-Term Concerns | |
| “So I think there will be a lot of changes as far as staying with a patient, which cuts down on your efficiency and your ability to see many patients in a day...even spreading out patients between chairs as opposed to being stacked right next to each other might be an issue that we see in the near future.” | |
| “I think the biggest short-term concern would be the wave of orthodontic emergencies we’ll have... breakages and losing progress due to things moving in an uncontrolled manner. Also, dealing with the heavy [patient] load in a bottleneck fashion...we’ve got to get everybody back in and that’s piled up and compounded.” | |
| “One of the biggest short-term concerns [with reopening] is getting PPE, not getting priced gouged on it and having enough for everybody. I think my biggest concern this week is even if we say, ‘Okay, the offices can open on [specific future date]’, I don’t know that we will be able to, because I don’t know if we’ll have the PPE.” | |
| “Short term concerns would be... how apprehensive patients will be to come in and if we’ll be able to fill our schedules like [we] once were.” | |
| “I believe there’ll be some hesitation. I don’t think that our overall office flow will be, hopefully, greatly impacted, due to the backlog of patients that has been rescheduled, but I do anticipate there being some fear and pushback from patients and possibly delaying appointments to later in the year.” | |
| I mean, I guess the biggest thing is just the delay in care. I mean, we can’t tell people that you are 100% safe here and there’s no way you’re going to potentially get it or spread it or whatever by being here. You can’t ever eliminate 100% of risk. | |
| COVID-19’s Impact on Oral Health Disparities | |
| “[I’m] mindful of patients who would be considered high risk like the elderly or patients that we know have hypertension or uncontrolled diabetes.” | |
| “Lower socioeconomic status [patients are] definitely going to be hit the hardest [and] they’re most likely the people that are still working [outside of the home].” | |
| “I do think that this will affect [our patients] dental health, which will affect their overall health. [As] dental disease progresses, we know it doesn’t get better without intervention. There will definitely be some implications... particularly when I think of perio. There’s a huge oral systemic connection with periodontal disease and we have all of these patients who aren’t getting medical care or oral healthcare. I think there’s going to be a lot of very unhealthy people when we come out of this.” | |
| “People with hypertension, diabetes, elderly, older populations, they would be the ones that I’d be most concerned with. Do we delay their treatment depending on what their needs are? Do we delay their treatment as long as we can until they have access to a vaccination, or they’ve had the disease themselves and have the antibodies? That would be the group that I worry about the most.” | |
| “So far, the people who haven’t wanted to come in [for emergency care] are the elderly, which I understand because the mortality rates are so much higher for them…They’re scared to come in.” | |
| “I think when we get back to work, I think we’re going to see a big increase in caries and obviously tooth pain and things like that because I think oral health is going to be minimized during this time. Everybody’s so focused on the coronavirus that their [oral health has been] pushed back...A lot of people, they have a normal routine. They get up, shower, brush their teeth. Go to work, come home, eat dinner, brush their teeth, go to bed. Being out of a routine, is everybody brushing their teeth every day anymore?” | |
| “I’m expecting the elderly population to be most apprehensive about coming back.” | |
| Practice Viability and Financial Concerns | |
| “I think this will definitely slow down the growth of the office...being closed for a month and a half. I’m also concerned with how [COVID-19] is going to impact the economy. And when we do return [to work], if people are still going to be scheduling new patient exams quite at the same level.” | |
| “Predicting a downturn in money spent on dental care because everyone right now is facing hardship.” | |
| “Obviously with a recession or downturn in the economy, more elective procedures will decrease, so I believe there will be a year to two to three lag on production just because instead of crowns, people will be doing large fillings and trying to get by a little bit more.” | |
| “Keeping my staff employed… [in] the long term we have a large practice and keeping it viable for the next five years [is a concern]. Cashflow.” | |
| “I think there’s going to be just a huge economic impact and I’m a little scared for that.” | |
| “Patients are fearful for their health, but they’re also fearful of the economic impact. People aren’t spending money and when it comes to healthcare costs, it seems dentistry is generally one of those things that [gets] put towards the bottom of the list for a lot of people, so I think we’re going to see a recession.” | |
| “Is [re-opening] going to be worth it money-wise? …Are you going to be able to stay open?” | |
| “Is the practice still going to be around when it’s all over? That’s really the major long-term concern.” | |
| “Long-term concerns for me is just dentistry in general. Is it going to be the same as what it was, what we planned for when we graduated or went into the dental field? With a lot of people losing their jobs or being furloughed and [everyone’s] disposable income is dwindling or... nonexistent. When we do open up are people going to see dentistry as something that they need, that they’re going to get the work done? We can open back up, but if nobody has the money or is interested in getting the work done, we’re still highly effected by what the virus did.” | |
| “[If] we lose enough patients [and] end up having to let some staff go, how does that affect our cash flow long-term?” | |
| “Obviously, the economy is going to take a downturn and I think with orthodontics being somewhat considered elective, I’m not sure what that’s going to do as far as effecting my specialty and this practice that I’ve been investing in and buying into for the last six and a half years. You know, the student debt load that we all carry and just the financial plans that you have. I think that’s the biggest long-term concern.” | |
| COVID-19 as a Precedent | |
| “If [infectious disease outbreaks] become more of a regular issue...what [they may] do is force everyone to close their doors… That’s my long-term concern. What kind of precedent [does COVID-19] set moving forward? What is deemed a [nationwide] emergency? It just sets a precedent business-wise in the future [that dental offices could] close... you could possibly go out of business.” | |
| “How many of these PPE [changes for] infection control are going to become permanent changes versus temporary?” | |
| “Long term... looking to the end of the year, I think everyone is wondering if there will be another [COVID-19] outbreak. I think down the road... everyone is going to be a little more cognizant of the spread of this type of virus or any type of virus that could affect our office because this is something that I don’t think anyone expected, a shutdown of all dental offices. So, I think that’ll be something on our minds and something that the [governing bodies] should be paying attention to as well.” | |
| Governing Bodies Communication and Guidelines | |
| “We need some direction from our governing bodies to reassure us that this can be done in a safe manner, and then I think ultimately it will be on individual offices to use their discretion and figure out what works best and is appropriate for their office for personal protection and wellbeing of the patients.” | |
| “I think we need to advocate for access to PPE. We’ve been leaned on heavily by the medical world to donate our self-purchased PPE, which [I was] happy to do and proud to have helped with. However, we’re taking a double hit financial[ly]... [cash] flow has stopped and we’re going to have to try to start that back up, but on top of that we’re then trying to access PPE so that we can be open to the public and serve them in a safe manner. That’s a rarity right now as far as getting your hands on the right equipment. We donated so much of our equipment [that] we won’t be able to function at normal capacity and we can’t get the [PPE] we need to do the procedures we have to do.” | |
| “I’d really like to see regulations and recommendations for the [PPE] changes that need to take place as soon as possible so that we can get those things up and running because if say [we] can return to work within a couple of days, financially that might be tempting, but if you don’t have all the proper safeguards in place, then you can’t open anyway. I think that creates a stagger where some offices will be ready to go, others will have to make modifications and won’t be able to open their doors, which creates confusion for patients...some frustration or they switch their dental homes because of it. Why not be getting [prepared] while we can since there’s not much else we can do at this time?” | |
| “[The national dental society] have done a good job of really being on top of sending out alerts via text and email and trying to keep their members in the loop as much as they can...part of it is [COVID-19] is just an everchanging elusive thing. They don’t want to put out statements that they have to retract later.” | |
| “I would like [the State Dental Society] to show us what a dental office will look like six months from now, in terms of how they expect it to function. So what [should] a general practitioner’s office look like from appointment scheduling to patients [arriving] at the door, to patient at the [front] desk, to chair treatment and check out? What does that look like? what are the expectations? Practical implementation of [guidelines].” | |
| “What protocols should we have? How many people can I see in an hour? Continuing to reinforce the correct PPE.” | |
| “When we are clear to reopen, I would like to see specific guidelines [that the governing bodies] recommend. If they’re just going to open it back to elective procedures, if they still want to wait on hygiene checks, things like that...kind of the sheets they’ve been releasing recently about what’s acceptable and what’s not. It would be nice to have something to show patients right away if there’s ever any concerns about what can actually be done.” | |
| “Something more concrete. Because, they always say use your best clinical judgment...As a dentist, you feel you’re alone, if somebody tells you to just use your best clinical judgment, okay, fair enough, but my clinical judgment is not the same as yours in every scenario.” | |
| “But there are different scenarios [for urban versus rural locations]. Chicago’s different than a [small town]...different than New York... different than Florida, and so I can understand that it would be challenging, but that’s where I think at a state level, they could really start to dig in with some more practical things to help us get back to work.” | |
| “[The] new laws in [US] Congress had a direct effect on our offices as small businesses as employers of less than 50 people. It was a main concern on what we would be responsible for or whether we’d be exempt as healthcare providers. So I think the [governing bodies]...were working in our corner to get things clarified and dental offices exempt, but it’s still something that I’ve heard different opinions on, so [it’s] been a little confusing.” | |
| “The dental societies [need to] start advocating our importance as healthcare providers. I think the same thing goes for primary care physicians and all of the other physicians out there who are temporarily put out of work, it really minimizes the significance of [us] as health care providers.” | |
| Direction for Future Research | |
| “[Does] high volume evacuation affect the presence of the virus in aerosols or affect the presence of aerosols in general, does it make us safer having that being used at all times? How long can it live on organic or non-organic surfaces like our hair?” | |
| “I would like to see how long the virus can be in the air.” | |
| “[Does] high vacuum suction actually get rid of it or not? Probably not, but... [does it] at least cut back a significant amount?” | |
| “How exposed we really are to [COVID-19 as dentists]. Also, if there’s really any way to, with aerosols, to get those out of the air.” | |
| “What’s going to be the protocol to actively treat somebody with coronavirus? Most effective methods to keep everybody safe.” | |
| “Primarily, infection control. What can we do to prevent cross-contamination? [What can we do to prevent it] being passed around [the office environment], things of that nature.” | |
| “I’d like to see evidence on [aerosols], how long these last and what type of aerosols we’re spreading through the air with our hand pieces and ultrasonic units.” | |
| “[Research on] the [effectiveness] of the different masks that we have been wearing toward stopping this [COVID-19 transmission].” | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simonovich, J.R.; Simonovich, S.D. Examining the Experiences of US Dentists during the First Wave of the COVID-19 Pandemic: Implications for Policy and Practice. Psych 2022, 4, 375-386. https://doi.org/10.3390/psych4030031
Simonovich JR, Simonovich SD. Examining the Experiences of US Dentists during the First Wave of the COVID-19 Pandemic: Implications for Policy and Practice. Psych. 2022; 4(3):375-386. https://doi.org/10.3390/psych4030031
Chicago/Turabian StyleSimonovich, Jordan R., and Shannon D. Simonovich. 2022. "Examining the Experiences of US Dentists during the First Wave of the COVID-19 Pandemic: Implications for Policy and Practice" Psych 4, no. 3: 375-386. https://doi.org/10.3390/psych4030031